
Abstract
Eosinophilic ascites, owing to serosal involvement, is a very rare manifestation of eosinophilic gastroenteritis in children, especially when it occurs with muscular involvement in the absence of mucosal disease, which may be confirmed by endoscopic ultrasonography. An 11-year-old girl, presenting with massive eosinophilic ascites and colicky abdominal pain with peripheral eosinophilia, raised IgE levels and positive skin prick test, had such investigation which confirmed the presence of muscle layer thickening of both stomach and small bowel. She responded well to steroids and montelukast.
Case report
A previously healthy 11-year-old girl presented with abdominal pain and recurrent vomiting of two months’ duration. The pain was initially a dull ache, mostly in the epigastrium, lasting up to 30 min at a time. Its intensity progressively increased, with added colicky pain. She also had recurrent bouts of bilious vomiting with partial relief of her pain. She had lost her appetite, but no weight loss was noted. There was neither diarrhoea, fever, oedema, nor a history of asthma or allergies. Seafood had been eaten one week before the onset of symptoms. She had no stigma of chronic illness, normal size and weight and massive ascites.
Investigations revealed a normal haemoglobin (149 g/L) with normal red cell indices, normal platelet count (3 × 109/L), raised leucocyte count (27,500/µL [normal range = 4000–11,000/µL]) and an absolute eosinophil count of 9000/µL (normal range < 500). IgE was elevated (2633 IU/mL [normal range <100 IU/mL]). Ascitic fluid analysis showed 8000/mm3 cells, 90% being eosinophils. The ascitic fluid concentration of glucose was 60.5 mmol/L, protein 41 g/L, adenosine deaminase was 10 IU/mL (excluded tuberculosis), with non-contributory gram stain, bacterial culture and malignant cytology. Repeated stool examinations were negative for parasites, as was serology for strongyloides, toxocara and trichinella. The skin prick test revealed a strong allergy to shellfish and other fish and a mild allergy to yeast and food additives. Abdominal sonography revealed massive ascites with thickening of the antro-pyloric region, duodenum, jejunum and proximal ileum (Figure 1a and b). Endoscopy revealed no visible mucosal abnormality in these areas nor in the oesophagus or colon. Multiple mucosal ‘bite on bite’ biopsies showed normal histology in the mucosal and submucosal layers.
(a) Computed tomography (CT) of the abdomen showing antro-pyloric thickening with significant gastric residue. (b) Abdominal CT scan showing thickened small bowel loops. (c) Endoscopic ultrasound showing a thickened antro-pyloric region. (d) Endoscopic ultrasound showing thickened small bowel loops.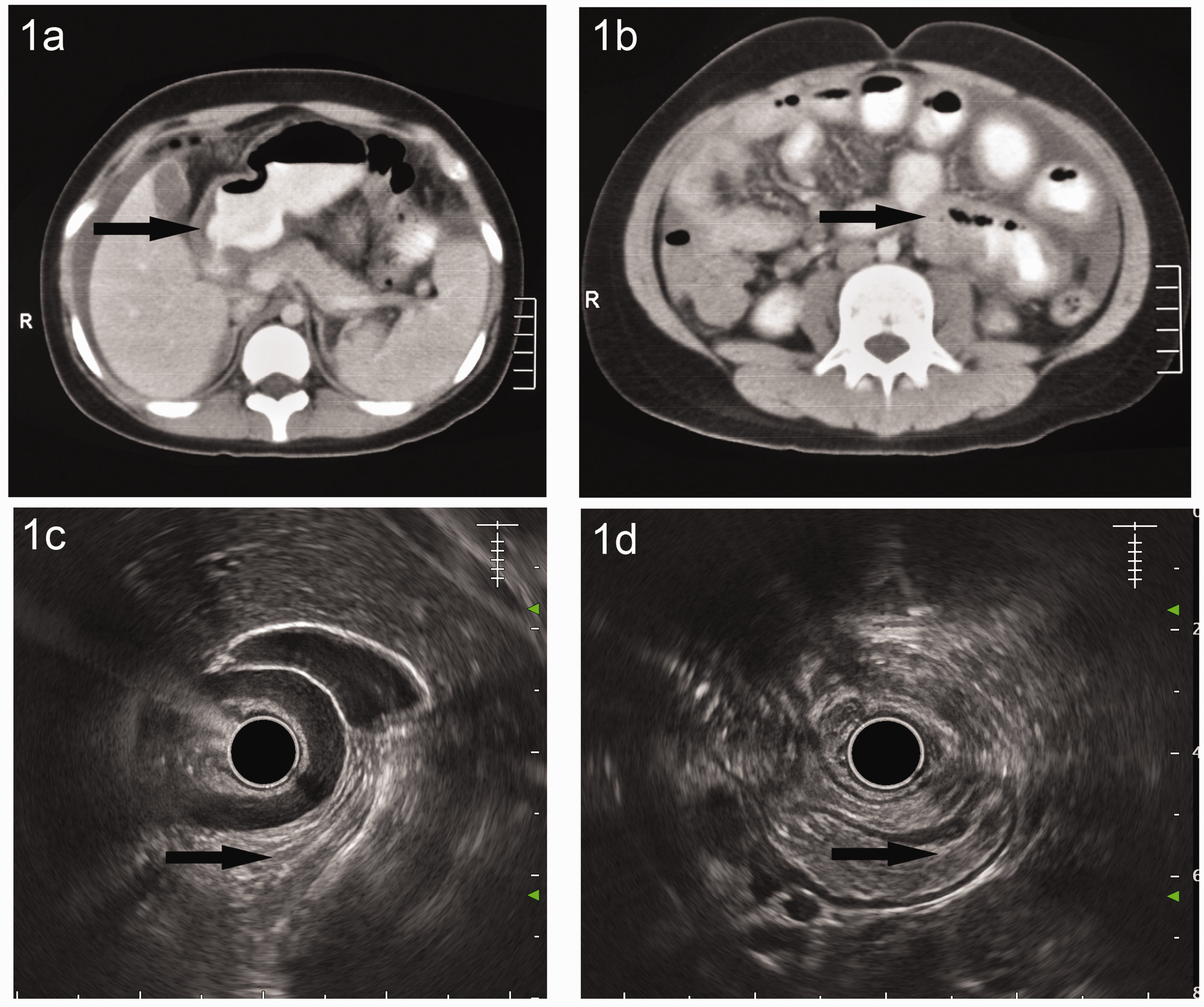
A dramatic response to prednisolone was seen, with a complete resolution of ascites within one week. Steroid treatment was tapered off and stopped over three months, after documenting normal sonography, eosinophil counts and IgE levels. She relapsed twice with identical symptoms, raised eosinophils and IgE, one and two years later, the possible triggers being seafood and yeast, respectively. Relapses were diagnosed by endoscopic ultrasound which confirmed muscle layer thickening in the antro-pyloric region, duodenum and jejunum (Figure 1c and d). The first relapse was treated with prednisolone, which was continued at a low dose for one year; the second relapse occurred one month after stopping steroids. As she had developed a Cushingoid habitus, montelukast in addition to lower doses of prednisolone (5 mg) were advised, with strict avoidance of the dietary triggers.
Endoscopic ultrasound showing thickened small bowel loops.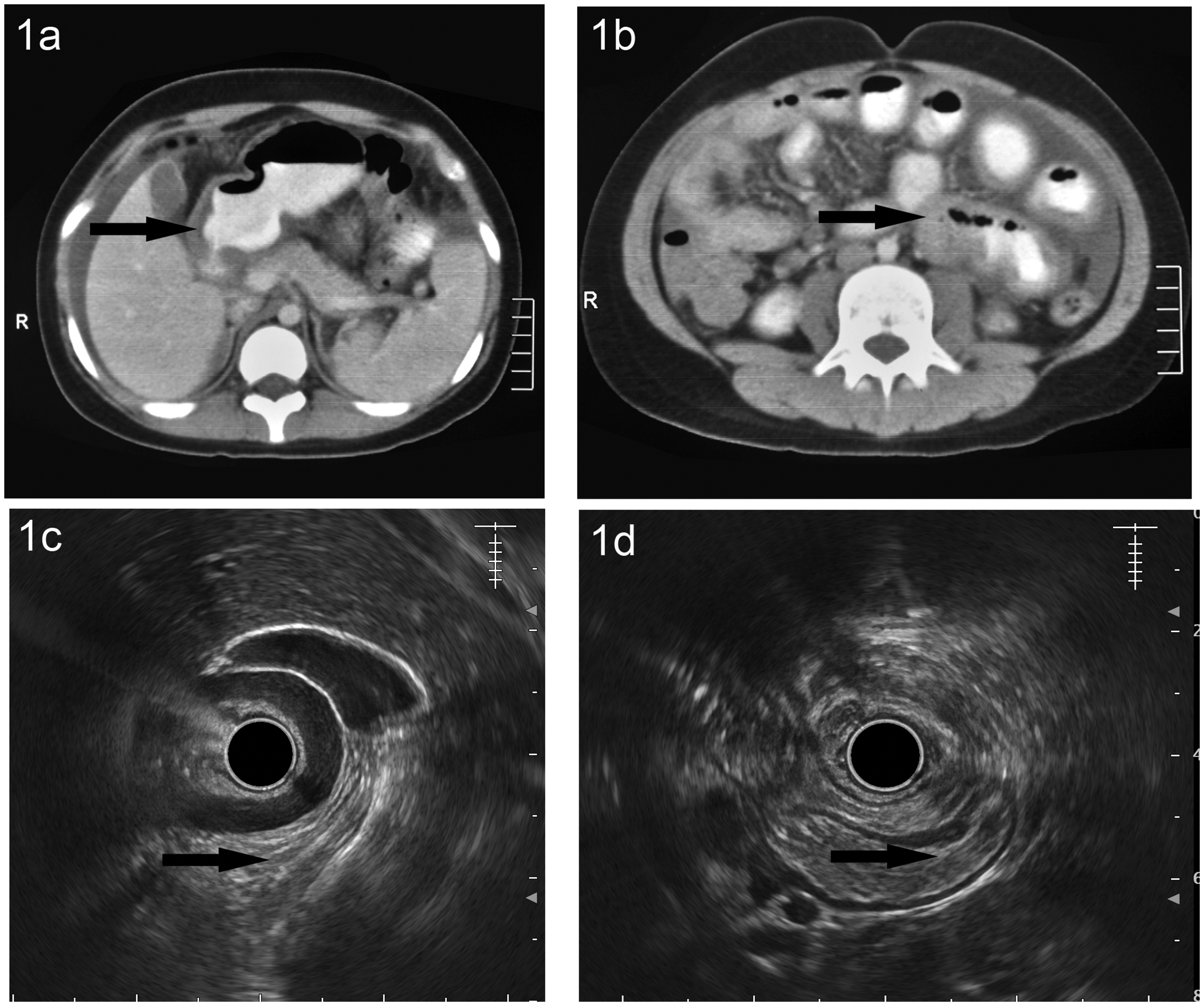
Discussion
EGE was first recognised by Kaijser in 1937 and classified by Klein into three overlapping subtypes: mucosal; muscular; or serosal.1,2 The mucosal form—characterised by diarrhoea, anaemia, protein-losing enteropathy or growth failure—is the commonest, alone or in combination with other subtypes; viz. a muscular form (features of intestinal obstruction) or serosal form, which is the rarest, presenting with bloating, abdominal pain and eosinophilic ascites. 2 The diagnostic criteria proposed by Telly et al. includes: the presence of gastrointestinal symptoms; eosinophilic infiltration of one or more areas of the gastrointestinal tract; absence of eosinophilic infiltration in extra-intestinal organs; and the exclusion of secondary causes of eosinophilia. 3 It is known that a fraction of patients with EGE has co-existing food allergies, which could be the possible trigger in them and can lead to peripheral eosinophilia. 3 Peripheral blood eosinophilia occurs in up to 80% of cases, with the highest levels seen in the serosal type. 4 Atopy or allergic disorders co-exist in 25%–75% of patients. 5
The serosal subtype presents with eosinophilia, pleural effusion or ileus. The mucosal subtype tends to be chronic; the muscle subtype has frequent relapses, but these are uncommon with pure serosal involvement. 6
Serosal EGE typically co-exists with the mucosal and muscular type; a combination of serosal with only muscular subtype without a mucosal involvement is extremely rare. A previously reported case has serosal involvement in the form of eosinophilic ascites along with positivity for antinuclear antibodies. 7
Endoscopic ultrasonography has been used in adults occasionally to confirm the diagnosis of EGE, 8 but has not been reported in children. It is an attractive modality in this population as it avoids both radiation and contrast.
The prompt response as well as multiple relapses in our patient is consistent with the 90% response rate to steroids and the 50% relapse rate described in literature, the relapses being more frequent in the muscular subtype. 5
Montelukast has been shown to have equivalent efficacy to steroids and may be used as a steroid-sparing agent. 6 Cyclophosphamide, azathioprine or biologicals such as mepolizumab have been used in non-responders. 9
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.