
Abstract
Cystic lesions of the pancreas are being increasingly diagnosed incidentally in recent decades due to easy availability of abdominal imaging. They may be neoplastic or benign. Tuberculosis, the great masquerader, may rarely involve the pancreas mimicking pancreatic malignancy, cyst, or abscess. Identification of this rare entity is crucial to avoid potentially risky surgery as anti-tubercular pharmacotherapy is highly effective. We report a case of a 40-year old cirrhotic man who presented with a cystic hypodense lesion in the pancreatic tail and was subsequently diagnosed with pancreatic tuberculosis. Apart from the rarity of diagnosis, our case also highlights the utility of endoscopic ultrasound for minimally invasive assessment of pancreatic lesions.
Case Report
A 40-year old male, diagnosed with alcohol-related cirrhosis ten years previously, presented with anorexia and significant weight loss (10 kgs in the past six weeks). He denied any history of fever or altered bowel or bladder habits, and his last alcohol intake was 10 years back. His body mass index was 19 kg/m2. General and systemic examination was unremarkable except for mild pallor. His full blood count showed pancytopenia (Hb: 108 g/L, leucocytes: 3.8 × 109/L, platelets: 92 × 109/L). Liver and renal function tests were within normal limits. Tumor markers (AFP, CEA, and CA-19-9) were within normal limits. Computed tomography revealed a hypodense lesion measuring 3.8 × 1.9 × 2.4 cm in the pancreatic tail, along with mesenteric, retroperitoneal, and pelvic lymphadenopathy.
Considering the possibility of malignancy, endoscopic ultrasound with fine needle aspiration cytology was carried out, revealing an irregularly contoured, avascular, hypoechoic cystic lesion in the pancreatic tail (size: 3.3 × 2.4 cm) without septations nor nodules together with peripancreatic lymph nodes (Fig. 1A).
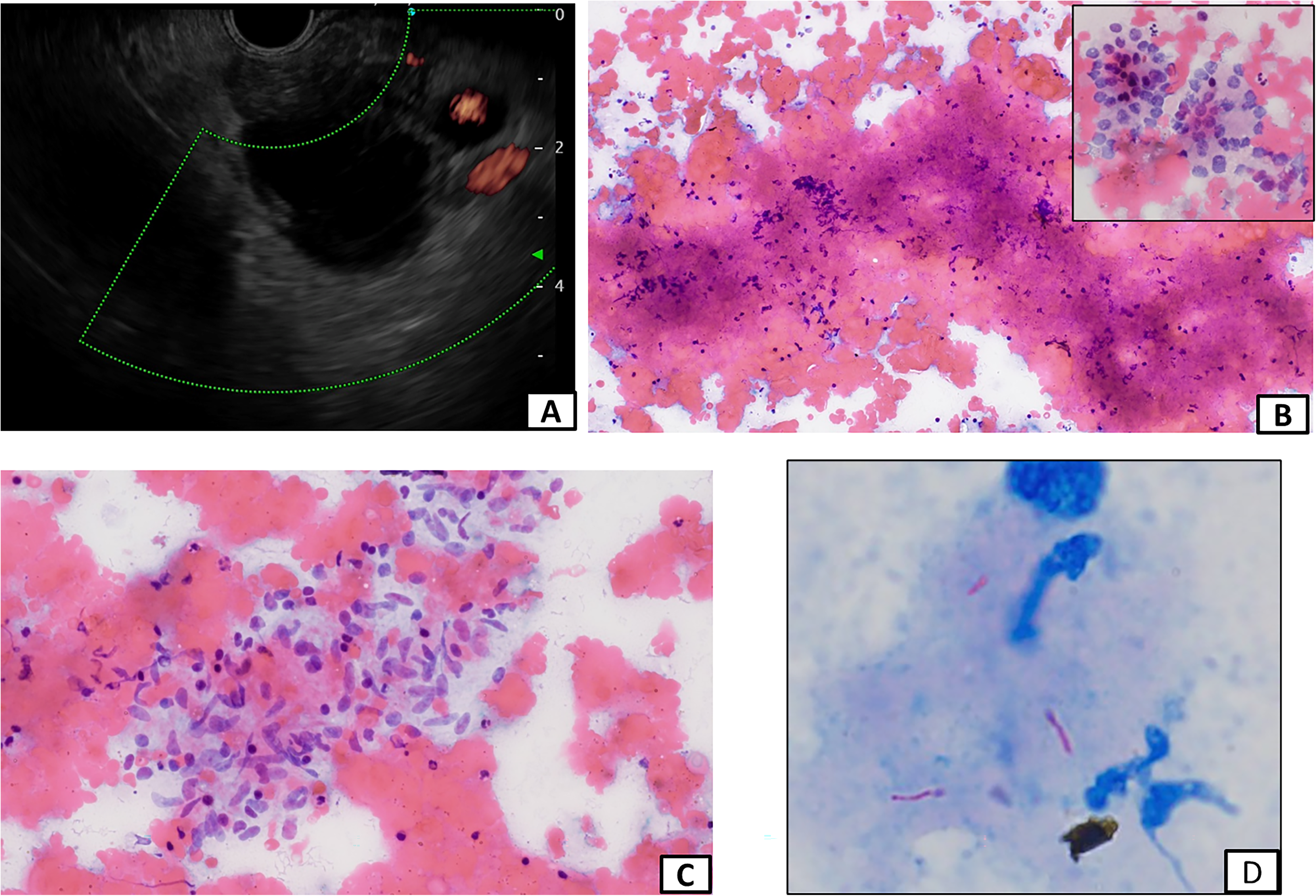
(A) Endoscopic ultrasound depicting an irregularly contoured, avascular, hypoechoic cystic lesion in the pancreatic tail without septations or nodules along with peripancreatic lymph nodes. (B) Caseation necrosis in cytology smear (inset: pancreatic acinar cells) (MGG ×20). (C) Epithelioid cell granuloma in cytology smear (H&E ×20). (D) Acid-fast bacilli (ZN stain ×100).
Purulent material was aspirated from the cyst using a 19G needle under ultrasound guidance, which was sterile but cytology revealed multiple epitheloid cell granulomas with acid-fast bacilli staining positive with Ziehl–Neelsen stain (Fig. 1B to D).
Modified anti-tubercular therapy without pyrazinamide on account of underlying cirrhosis (Child–Turcotte–Pugh Class-A) was commenced.
Discussion
Pancreatic tuberculosis is rare with most data confined to case reports and case series.1–5 The rarity of the entity is corroborated in large autopsy reviews where pancreatic involvement has been documented in only 0% to 2.1% of cases. 1 Not a single case of pancreatic tuberculosis was reported in a large series of 300 cases of abdominal tuberculosis from India, attributed to possible anti-mycobacterial effects of pancreatic lipases and deoxyribonucleases.1,4 Pancreatic involvement is usually isolated and lesions are rarely detected elsewhere in other organs. Owing to the frequent association with lymphadenopathy, the contiguous spread of bacilli to the pancreas from the affected lymph nodes appears to be the likely pathogenesis. However, hematogenous dissemination from occult pulmonary lesions may also occur.3,4 Up to a quarter of patients with pancreatic tuberculosis have predisposing immunosuppressive states such as HIV, although it has been reported in immunocompetent patients too.1,3,5
Tuberculosis is more frequent in immunosuppressed states including cirrhosis where it often presents atypically with more frequent extrapulmonary involvement. 6 Pancreatic tuberculosis usually presents non-specifically with fever, weight loss, abdominal pain, and jaundice. 1 Despite weight loss, fever was conspicuously absent in our patient possibly due to underlying cirrhosis. Radiologically it usually presents as a mass often mimicking malignancy. A cystic lesion, as seen in our patient, has been reported in <2% of cases. The head of the pancreas is the most commonly involved site and the tail is only involved in ∼10% of cases. 1
The absence of specific radiological features makes the diagnosis challenging. A high index of suspicion is required, particularly in countries such as India, endemic to tuberculosis. In addition, endoscopic ultrasound has emerged as an excellent modality for the diagnosis of pancreatic lesions. It allows detailed morphological characterization including septae, mural nodules, and communication with the pancreatic duct. Further, it permits sampling for cytological and histopathological confirmation. Indeed, the diagnosis was confirmed in our case specifically after guided assessment and cytological confirmation.
Pancreatic tuberculosis is uncommon but an eminently treatable condition. It should not be missed.
Footnotes
Author contributions
AS contributed to manuscript writing; BD contributed to data collection and manuscript writing; MUA contributed to data collection; RL contributed to data collection and cytology; NG contributed to cytology analysis; AD contributed to manuscript writing, data collection, and critical review.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Informed consent
Written informed consent for patient information and images to be published was taken from the patient.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.