
Abstract
The five major types of ovarian tumors in females of different age groups are discussed here with respect to discordance between ultrasonography, clinical features and histopathology findings. The importance of clinical examination cannot be denied in such cases as total dependence on investigation modalities may lead to wrong diagnosis and treatment. Five such cases admitted in the year 2017-2018 at Era's Lucknow medical college and hospital were selected for this series. All the cases had varied presentation, and diagnosis in each case was difficult as the nature of the masses differed markedly from the radiological findings. Even in expert hands, a radiological conclusion must go hand in hand with a proper clinical correlation.
Introduction
Amongst women worldwide, ovarian cancer is the sixth most common cancer (age standardized incidence rate: 6.6/100,000) and the seventh leading cause of cancer deaths (age standardized mortality rate: 4.0/100,000). 1 According to most cancer registries in India, ovarian cancer follows cervical and breast cancer, but has a low five-year survival rate (45%) because 80% are diagnosed with advanced disease. 2 Age-adjusted incidence rates of ovarian cancer vary between 5.4 and 8.0 per 100,000 population in different parts of the country. 3
The number of comprehensive cancer centers in India that can offer appropriate multidisciplinary care is quite small. Many patients receive suboptimal management owing to socioeconomic constraints, usually because they belong to rural areas where access to specialized healthcare is poor. The prohibitive cost of anti-neoplastic drugs is a major deterrent for many patients to continue treatment. There is a need to assess these factors objectively in our context; thus we present a case series of five varied presentations of ovarian tumors in females of different age groups in which ultrasound findings differed remarkably from clinical and histopathological findings.
Case series
Case 1
A 45-year old perimenopausal female P2L2 of average build complained of dull aching abdominal pain for four months with a gradually increasing abdominal mass. On abdominal examination, the umbilicus was central and inverted, with no visible veins or scarring, and a mass of 16 weeks’ gestationary size palpated in the left hypogastrium, cystic in consistency, freely mobile, non-tender, with a smooth surface and well defined margins, whose lower pole was out of reach, dull to percussion, without ascites around it. Vaginal speculum examination showed the cervix and vagina to be healthy. On digital vaginal examination, the uterus was normal in size, was separate from a left adnexal mass 20 × 15 cm in size felt having cystic consistency, regular margins, a smooth surface, and with fullness present in all fornices. Cervical movement was not transmitted to the mass.
Laboratory levels of CA-125 was 43.8 u/ml (mildly raised) but other tumor markers were normal.
The ultrasound scan described a well-defined partially solid and cystic left adnexal lesion measuring (22 × 12 × 18 cm). Neither ovary was separately visualized distinct from the lesion. No septations were seen. Computerized tomography (CT) scan confirmed these findings with enhancing solid components and septae presumed to be an ovarian neoplasm. On the basis of above findings, the morphological index was calculated as 8 and risk of malignancy index (RMI) 131.
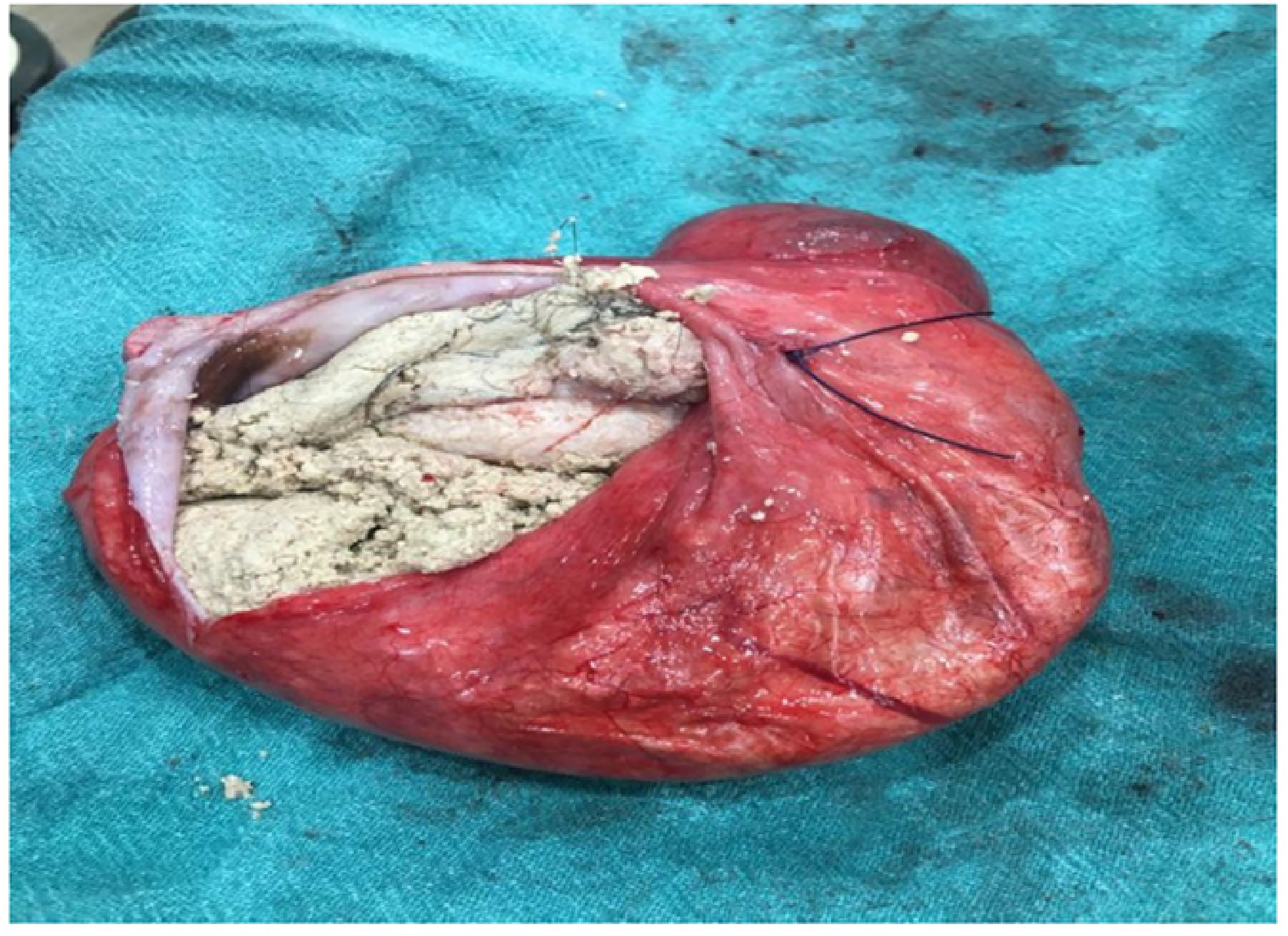
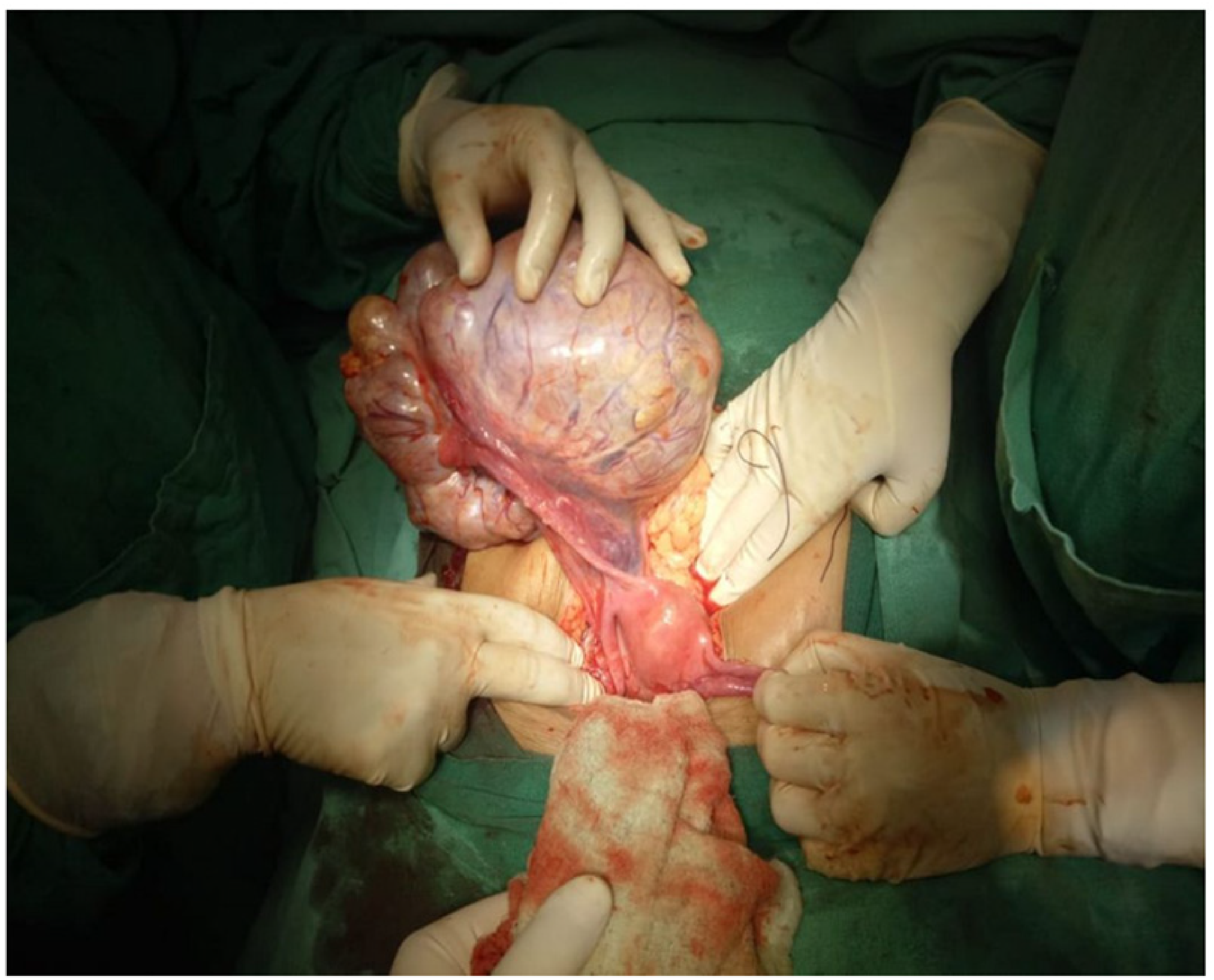
At laparotomy, a large multiloculated cyst of 26 × 27 cm in the left adnexa was found with no internal septations. The right tube and ovary were normal. No lymph nodes were involved and no ascites seen. Adhesions were present. Total abdominal hysterectomy with bilateral salpingo-oophorectomy was performed (Figure 1). Histopathology showed a mucinous cystadenoma of the left ovary (Figure 2)

Specimen of mucinous cyst adenoma.

Histopathological examination (HPE) of mucinous cyst adenoma in microscopic view.
Case 2
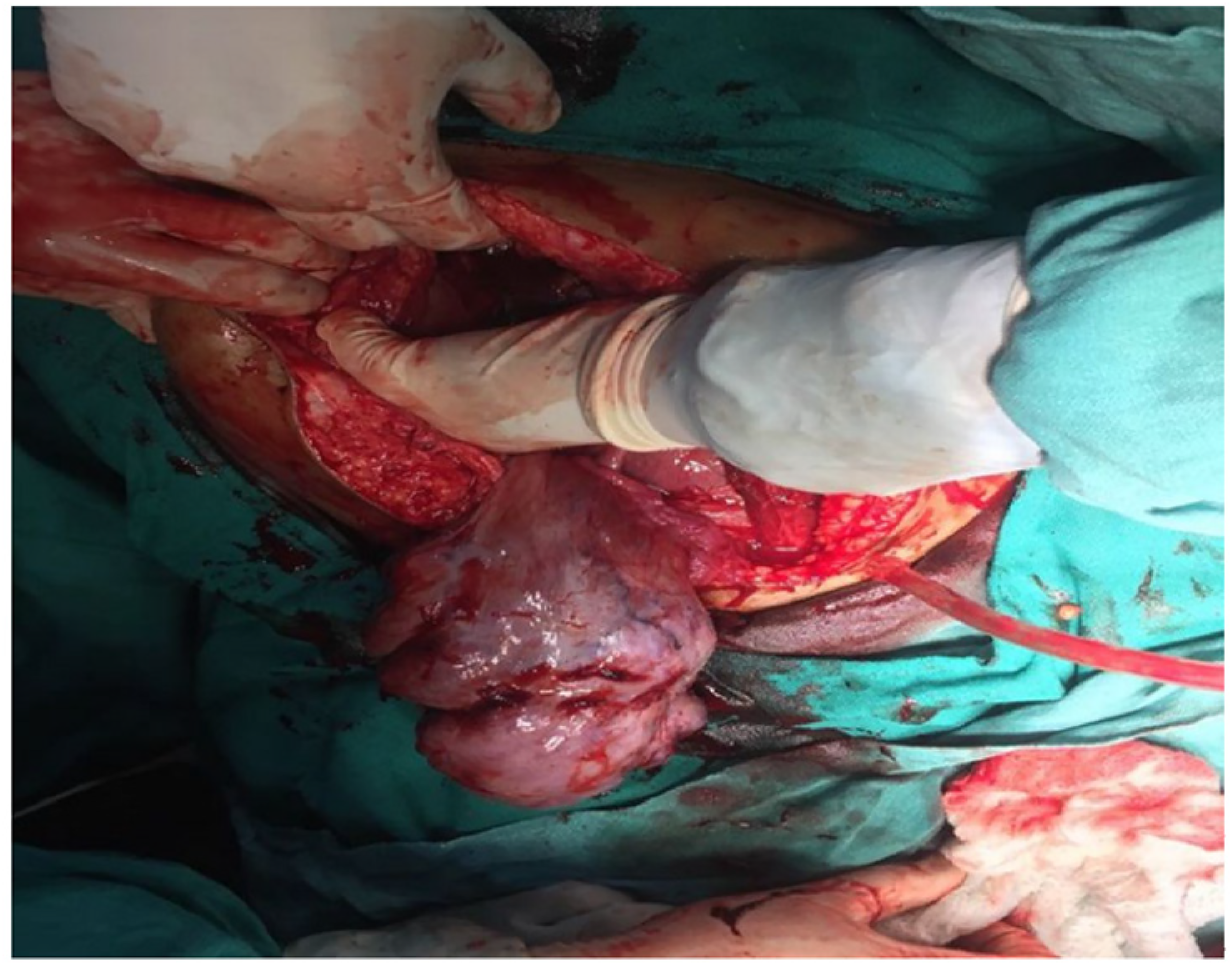
A 28-year old female nulligravida presented with dull aching abdominal pain for two years, with an abdominal mass gradually increasing in size over the last year. On examination, she was anemic and had a mass of 20 weeks’ gestationary size, firm in consistency, with a smooth surface and regular margin, arising from the pelvis more towards the right, freely mobile from side to side but otherwise restricted in mobility, non-tender with no fluid thrill, no shifting dullness and no lymphadenopathy. On vaginal speculum examination, an anterior vaginal wall cyst with bluish discoloration approximately of 1 × 1.5-cm was seen. On digital vaginal examination, the cervix was deviated to the right, and a mass of 18 × 20 cm, firm in consistency was palpated through the posterior fornix separate from the uterus. Ultrasonography showed a hetero-echoic, ill defined cystic mass 18 × 7 cm with septations. Both the ovaries could not be distinguished from the mass. Liver and renal function tests were normal, CA125 was 175u/ml (raised) and remaining tumor markers were normal. Enhanced CT scan showed a large abdomino-pelvic lobulated thick walled multiseptate cystic lesion measuring 18 × 16 × 13 cm, with abdominal lymphadenopathy. This complex ovarian malignant mass deemed to be metastatic. Further magnetic resonance imaging suggested a well-defined multi-loculated cystic mass with altered signal intensity in the pelvic region likely to be endometriomas. The morphological index was 6 and RMI was 175. On exploratory laparotomy, a solid friable mass of 15 × 15 cm was seen,adherent posteriorly to bowel & omentum on the left lateral side. A small amount (50ml) of ascites was present and sent for cytology. A total abdominal hysterectomy with bilateral salpingo-oophorectomy was performed (Figure 3). Histopathology showed a serous cystadenoma of the ovary (Figure 4) with negative cytology for malignant cells.
Specimen of serous cyst adenoma of ovary.
HPE of serous cyst adenoma of ovary in microscopic view.
Case 3
A 23-year old female P1 + 1L1 was admitted eight days after full term normal delivery with abdominal pain since delivery. Abdominal examination revealed a mass of 32 weeks’ gestation, which was hard, non-tender, mobile, with irregular surface, but well defined margins, arising from pelvis. Vaginal speculum examination showed healthy lochia, cervix and vagina. On digital vaginal examination, the uterus could not be felt separately from the mass which was irregular, firm, and non-tender. Both fornices were full and non-tender.
An ultrasound scan showed a large multi-loculated hetero-echoic mass in the right adnexa measuring 21 × 15 × 13 cm with few hyper-echoic foci, irregular internal hypo-echoic areas and increased vascularity but the right ovary was not visualized separately. Ascites was present. Laboratory levels of CA125 was 41.3 u/ml (mildly raised), Lactate dehydrogenase (LDH) was 54.6 ukat/l (raised) but the remaining tumour markers were normal. The morphological index was 12 and RMI was 124.
At laparotomy, a solid friable mass 25 × 25 cm in size was seen with an intact capsule, but without extra-capsular growth, with ascites present. The left Fallopian tube and ovary were normal. The uterus was of 12 weeks’gestationary size. No lymphadenopathy was found. A stage IA ovarian carcinoma was suspected and a hysterectomy with right sided salpingo-oophorectomy was performed (Figure 5). Histopathology showed simple hyperplasia without atypia in the endometrium, koilocytic change with Nabothian follicular cyst was present in the cervix. In the right ovary an embryonal dysgerminoma was found (Figure 6). Cytology was negative for malignant cells. Three cycles of chemotherapy (bleomycin, etoposide, cisplatin) were administered.

Specimen of embryonal dysgerminoma.

HPE of embryonal dysgerminoma in microscopic view.
Case 4
A 23-year old female primigravida 17 weeks pregnant, complained of abdominal pain for 15 days. On examination, a tender abdominal mass of 26 weeks’ gestationary size with restricted mobility was palpated, which could not be well differentiated from the gravid uterus. The mass had a regular margin, smooth surface and variegated consistency. Its lower pole could not be reached. There was no ascites.
Vaginal examination added no further information.
Ultrasonography showed a single live intra-uterine fetus of 16 weeks’ gestation with a large heterogeneous polypoidal soft tissue mass 14 × 10.6 cm in size with an internal cystic component in the right adnexa.
The magnetic resonance imaging (MRI) scan confirmed the gravid uterus, with evidence of a well-defined, heterogeneous lesion, possibly arising from the uterine fundus, extending to the right liver lobe, thought to be a fibroid. The right ovary was not visualized.
Laboratory levels of CA-125 was 149.6 u/ml (raised), LDH was 13.5 μkat/l (raised), and α- fetoprotein 500 ng/ml(raised), β-HCG 15,000 iu/l (normal at her gestational age).
The morphological index was 6 and RMI was 150.
At laparotomy, a mass of 11 × 6 cm was seen arising from right ovary with an intact capsule, Hepatomegaly was present. The left ovary and tube appeared to be normal. A right salpingo-oophorectomy was performed, and an omental biopsy taken. (Figure 7).
Specimen of dysgerminoma of ovary.
Histopathology showed this to be an ovarian dysgerminoma (Figure 8). Cytology was negative for malignant cells. A termination of pregnancy was carried out followed by adjuvant chemotherapy, (bleomycin, etoposide, cisplatin) in three cycles in post-operative period.
HPE of dysgerminoma of ovary in microscopic view.
Case 5
A 35-year old woman P2L2 complained of gradual onset of lower abdominal pain for three months, with a concomitant mass. On examination, a mass of 28 weeks’ gestationary size was palpated in the abdomen, dull to percussion, variegated in consistency, freely mobile, non-tender with an irregular surface but well-defined margins, whose lower pole could not be reached. There was no ascites.
Vaginal speculum examination showed healthy cervix and vagina. On digital vaginal examination, the mass had a variegated consistency, being separate from the uterus which was normal in size.
Laboratory levels of CA125 was 125. μ/ml (raised), and CA19-9 was 663.2 u/ml (markedly raised)
Ultrasonography showed two adjacent mixed solid and cystic lesions measuring (117.5 × 75.2 × 123.3 mm) on the right and (114.4 × 62.4 × 98 mm) on the left in the suprapubic region extending from the pubis to umbilicus, the solid components having minimal vascularity on color Doppler.
A CT scan showed multiple well-defined and lobulated peripherally enhancing cystic lesions, the largest measuring 13.8 × 12.3 cm, noted in the abdominopelvic region. Neither of the ovary could be visualized separately. The Morphological index was 6 and RMI was 377.
At laparotomy, a multi-lobulated mixed solid cystic mass 20 × 14 cm was found adjacent to the right Fallopian tube, with some ascites present. Total abdominal hysterectomy with bilateral salpingo-oophorectomy was carried out along with infracolicomentectomy (Figure 9). Histopathology showed a right ovary with sero-mucinous cysadenocarcinoma (Figure 10). The left ovary was unremarkable. The omentum had no tumour in situ. Cytology was negative for malignant cells. The patient underwent six cycles of chemotherapy post-operatively.
Specimen of sero mucinous cystadenocarcinoma.
Showing HPE of sero mucinous cyst adenocarcinoma in microscopic view.
Discussion
Ovarian cancer is common and is often detected in advanced stages. Thus, work-up based on clinical findings, ultrasonography characteristics and serum tumor markers will help in planning and organizing management with respect to time, cost effectiveness and infrastructure. Differentiation between benign and malignant pathology on the basis of the above will help in deciding the correct plan of management. 4 The risk of malignancy index (RMI = Menopausal status score Xultrasonographic score × absolute value of serum CA 125) is still commonly used in many countries for categorizing ovarian pathology. Simple rules created by the International Ovarian Tumor Analysis (IOTA) group and other logistic regression models have better performance.5, 6
A multicentric study, to evaluate accuracy of ultrasonography by subjective assessment of the specific pathology of adnexal masses in the hands of examiners with varied training and experience, concluded that specificity of ultrasound is high (91–100%) irrespective of type of adnexal mass, but the sensitivity showed substantial variation. In the case of simple cysts, it is c. 100% (95% CI, 61–100%), for hydrosalpinx 100% (95% CI, 34–100%), mature teratomas 88% (95% CI, 74–96%), endometriomas 75% (95% CI, 61–85%), ovarian fibromas 88% (95% CI, 47–100%), tubo-ovarian abscesses 88% (95% CI, 47–100%) and serous cystadenocarcinomas 82% (95% CI, 66–93%). Serous cystadenomas were misdiagnosed most commonly (40.5%). 7
MRI provides a better tissue characterization than Doppler ultrasound or CT scan. Pelvic MRI should be added where a complex ovarian tumouris so diagnosed. 8
Positive peritoneal fluid cytology is an isolated indicator of poor prognosis, whose sensitivity of is 90% and specificity is 96.5%. 9
Intra-operative frozen section has low sensitivity and positive predictive value for borderline ovarian tumors. 10 This facility is not available at our hospital.
Conclusion
To improve the pre-operative diagnosis, correlation of thorough clinical assessment, relevant radiological investigation in expert hands and relevant blood investigations are important, but may not be entirely reliable. IOTA scores are preferable. Careful comparison of results at expert group discussions with radiologists and a gynecological oncologist is vital; optimal staging, debulking and careful follow up, including chemotherapy compliance is needed for optimum results.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical clearance
Patient's identifiers have been anonymised.
Informed consent
Informed written consents were taken from the patients.