
Abstract
This study examined the relationship between older adults’ subjective versus objective sleep and subjective cognitive decline (SCD), and explored the role of depression on this association. One hundred and four community-dwelling older adults underwent a week of actigraphic sleep monitoring, and completed a series of neuropsychological screeners. Older adults’SCD score was positively correlated with subjective insomnia, but not with objective sleep parameters. Further mediation modeling revealed that older adults’depression mediated the association between subjective insomnia and SCD. Subjective sleep, rather than objective sleep, may be a more sensitive indicator for older adults’ SCD, with depression symptoms appearing to account for most of the variance. These findings extend our perspective on the relationship between sleep disruption and cognitive decline, and highlight the necessity of early targeted interventions on sleep to reduce the risk of cognitive impairment in the elderly with SCD.
Introduction
Subjective cognitive decline (SCD), also known as subjective cognitive complaints (SCC) or subjective cognitive impairment (SCI), refers to a self-perceived worsening of cognitive functions while in the absence of objective impairments detected by neuropsychological assessments (Jessen et al., 2014). A growing body of evidence suggests that SCD increases the risk for developing mild cognitive impairment (MCI; van Harten et al., 2018) and Alzheimer’s disease (AD; Lin et al., 2019). The National Institute of Aging and Alzheimer’s Association (NIA-AA) posits that AD is a continuum that normally begins with asymptomatic, preclinical phase (preclinical AD), converts into symptomatic, pre-dementia phase (MCI due to AD), and culminates in clinical dementia (Sperling et al., 2011). Therefore, it is helpful in identifying those who should be screened for AD.
The relationship between AD and sleep is becoming apparent with accumulating evidence in recent years that AD pathology has been shown to be associated with sleep disruptions (Lucey, 2020; Osorio et al., 2011). However, sleep in SCD has been less assessed, and the existing findings are inconsistent. Over the last decade, 12 studies explored the relationship between SCD and sleep in older adults, with seven studies focusing on subjective sleep, two studies on objective sleep, and three studies involving both subjective and objective sleep (Table 1). For subjective sleep, the results showed that older adults’ SCD significantly correlated with the Pittsburgh Sleep Quality Index (PSQI; Chen et al., 2019; Kang et al., 2017; Leng et al., 2020), the Epworth Sleepiness Scale (ESS; Okamura et al., 2016; Tardy et al., 2015), and sleep satisfaction (Tardy et al., 2015). Nevertheless, non-significant correlations between subjective sleep and SCD have also been reported in previous studies, using various subjective sleep assessments including PSQI (Cavuoto et al., 2016; Chen et al., 2019; Gamaldo et al., 2019; Lauriola et al., 2017). For objective sleep, four studies used wrist actigraph (Bubbico et al., 2019; Cavuoto et al., 2016; Lauriola et al., 2017; Manousakis et al., 2018), and two studies used polysomnography (PSG) recording sleep electroencephalogram (EEG; Manousakis et al., 2018; Tardy et al., 2015). Similar with the findings of subjective sleep, inconsistent findings have also been observed in the relationship between objective sleep and SCD. For instance, Bubbico et al. (2019) using actigraph found that older adults with SCD showed a shorter total sleep time (TST) than non-SCD, but two other similar studies reported a null effect (Cavuoto et al., 2016; Lauriola et al., 2017).
Studies (N = 12) Investigating the Relationship Between SCD and Sleep in Older Adults

Note. a PSQI sub-dimensions; b single item or self-compiled scale; c actigraphic; d polysomnographic; NC, normal control; SCD, subjective cognitive decline; PSQI, the Pittsburgh Sleep Quality Index; ISI, the Insomnia Severity Index; ESS, the Epworth Sleepiness Scale; RBDSQ, the Rapid-eye-movement sleep Behavior Disorder Screening Questionnaire; S, significant; NS, non-significant.
In addition to the global sleep quality index (i.e., PSQI), insomnia index can also reflect the relationship between sleep and cognition in older adults (Bruce & Aloia, 2006; Cross et al., 2019; Yaffe et al., 2014). Insomnia is a common sleep disorder in older adults (Morin & Benca, 2012), with a prevalence ranging from 17% to 60% in studies that utilized the diagnostic criteria for insomnia and from 8.2% to 74.8% in studies that asked about insomnia symptoms (Nguyen et al., 2019). Accompanied by symptoms of insomnia, decreased cognitive functions across domains, for example, attention, working memory, verbal information processing, verbal memory, verbal fluency, and visual memory, were observed in older adults accordingly (Sexton et al., 2020). With respect to AD continuum-related diseases, in older adults with insomnia, sleep duration, sleep fragmentation, sleep efficiency, the percentage of non-rapid eye movement sleep stage I (i.e., N1) and non-rapid eye movement sleep stage III (i.e., N3) was found to be independently associated with the presence of amnesic MCI (Zhang et al., 2020). Moreover, in three longitudinal studies, older adults with insomnia were more likely than those without to have a diagnosis of AD or cognitive decline at follow-up (Cricco et al., 2001; Lobo et al., 2008; Osorio et al., 2011).
In addition to sleep, SCD has been found to be positively correlated with depression (Liew, 2019; Molinuevo et al., 2017; Zlatar et al., 2018). Furthermore, depression was also found to be associated with sleep disruptions in older adults, with sleep declines being both a symptom of and a possible cause of depression (Roberts et al., 2000). Recently, a path analysis study showed that both sleep and depression were linked with cognitive decline in MCI patients, with sleep disturbance appearing to predict depressive symptoms (McKinnon et al., 2019). However, the role of depression in the relationship between pre-MCI stage, that is, SCD, and insomnia is less understood.
In the present study, we intend to extend the understanding of the relationship between SCD and sleep by including both subjective and objective sleep measurements and exploring the role of depression in this relationship. Therefore, the aims of our study were: (1) to explore the correlation between SCD and subjective sleep, SCD and objective sleep, respectively, and (2) to investigate the role of depression in the relationship between sleep and SCD.
Methods
Participants
We used convenient sampling and contact older adults randomly from our participant database. One hundred and four community-dwelling older adults aged 55 and above were contacted and recruited for the study. The inclusion criteria for recruitment were: (1) age ≥55; (2) no historical or current neurological diseases or psychiatric conditions; (3) completion of the neuropsychological screeners. Participants were excluded if their scores of the Mini-Mental State Examination (MMSE) were less than 24 (n = 6), which reflected objective neuropsychological deficits (Folstein et al., 1975). This study was conducted in the laboratory. Each older adult was invited to the lab twice, with the first time to complete the neuropsychological screeners and delivered the actigraph, and with the second time to return the actigraph and submit the sleep log. Of 98 participations enrolled, 87 older adults had actigraph data. Participants were instructed to remain free of caffeine, drugs, and alcohol during the study period. Demographic, neuropsychological, and sleep characteristics of the sample are shown in Table 2.
Demographic, Neuropsychological, and Sleep Characteristics of the Sample

Note. a Correlation resultswith SCD-Q9; b Average sleep characteristics per day for 1 week. MMSE, the Mini-Mental State Examination; SCD-Q9, the Subjective Cognitive Decline Questionnaire 9; GDS, the Geriatric Depression Scale; ISI, the Insomnia Severity Index; PSQI, the Pittsburgh Sleep Quality Index; * p< .05, ** p< .01, *** p< .001.
In the present study, participants’ subjective cognitive declines were measured by the Subjective Cognitive Decline Questionnaire 9 (SCD-Q9; Gifford et al., 2015), but they were not classified as SCD and non-SCD older adults. Instead, in order to explore associations between the degree of SCD and subjective versus objective sleep, we quantitatively assess older adults’ subjective cognitive declines by the SCD-Q9 without making a definition of SCD or dichotomizing the sample between SCD and non-SCD group (Valech et al., 2019).
The study was reviewed and approved by the ethics committee of Faculty of Psychology, Southwest University (No. H20035) to be in accordance with the Declaration of Helsinki. All participants were fully informed of the purpose and procedure of the study, and they each provided a written informed consent.
Neuropsychological Assessments
Participants’ demographic data were collected, and then they were instructed to complete a series of neuropsychological screeners measuring their cognitive function, sleep, and depression. Specifically, the MMSE (Folstein et al., 1975) and SCD-Q9 (Gifford et al., 2015) assessed older adults’ objective and subjective cognitive decline respectively; the Insomnia Severity Index (ISI, Morin, 1993) assessed participants’ subjective insomnia; and the Geriatric Depression Scale (GDS) measured older adults’ depression (Yesavage et al., 1982). Additionally, a spatial associative memory task was administrated before and after 1 week interval, which is not within the scope of this study.
Subjective Cognitive Decline Assessment
The brief version of SCD-Q with 9 items (Gifford et al., 2015) was used to measure participants’ self-perceived cognitive decline. The SCD-Q9 is a useful tool for screening and quantifying SCD, which was developed based on the SCD criteria proposed by the Subjective Cognitive Decline Initiative (SCD-I). It has been found to be strongly and significantly correlated with the 21-item version (Gifford et al., 2015). Previous studies confirmed that the SCD-Q9 is applicable in Chinese, with a Cronbach’s α of 0.847 and a coefficient of validity of 0.871 (Hao et al., 2017). For this study, the questionnaire demonstrated a good internal reliability (Cronbach’s α = 0.91).
Subjective Insomnia
Subjective insomnia was assessed by the ISI (Morin, 1993), which evaluates self-perceived severity of insomnia over the past 2 weeks. Items are scored using a Likert scale with five response options (0 = not at all to 4 = very much). Total scores ranged from 0 to 28, and higher scores indicate greater perception of insomnia. For this study, the measurement showed a good internal reliability (Cronbach’s α = 0.91).
Depression Assessment
The GDS (Yesavage et al., 1982) was used to assess older adults’ depression over the past week. It is a self-assessment tool that consists of answering yes or no to short, clear questions. Individual answers are scored by 0 or 1, and the obtained values range from 0 to 30. Higher scores indicate greater depression. For this study, the scale showed a good internal reliability (Cronbach’s α =0.99).
Actigraphic Sleep
The Actigraph (Bluetooth® Smart wGT3X-BT) was used to monitor participants’ objective sleep. They were required to wear a small, wrist-worn monitor on the non-dominant wrist for 1 week, except for water activities (e.g., bath and swim). Offline analysis of actigraphic data used the ActiLife software (ActiLifev6.13.4, LLC, Pensacola, FL, USA). Actigraphs were measured in 60 s epochs. To prevent first day effect, we excluded the first 24 h period data of actigraph from the following analyses. We used the Choi algorithm to define the non-wearing time, which has been described in more details elsewhere (Choi et al., 2012). We calculated the TST (minutes scored as “asleep”), sleep efficiency (SE, sleep minutes divided by minutes in bed), wake after sleep onsettime (WASO, minutes awake after sleep onset occurred), and awakenings (the number of awakenings).
Data Analysis
First, we conducted a conservative version of Harman’s one factor test (Malhotra et al., 2006) to verify that the results are not from a common method bias (CMB). We performed a confirmatory factor analysis (CFA) loading all items on a single factor, and examined the fit indices. The fit for the single factor model is poor (χ2(1952) =5227.65,RMSEA = 0.13, NNFI = 0.61, CFI = 0.62, and standardized RMR = 0.14) and the chi-square change (∆χ2 = 1089.80, ∆df = 6, p < .001) from the hypothesized measurement model is highly significant. Thus, we consider the potential effect of CMB to be non-substantial. Second, we investigated the correlation between subjective sleep and SCD versus objective sleep and SCD. Third, we tested the hypothesized model with depression as a potential mediator for the relationship between the variable that significantly predicted SCD in correlation analysis, that is, subjective insomnia, and SCD by estimating the 95% confidence interval (CI) with 5000 sampled with repetition. Statistical analyses were performed using SPSS 26.0 (IBM Corporation, Armonk, NY, USA), and the mediation modeling was conducted with SPSS PROCESS macro 3.4 (Hayes, 2013, Hayes, 2016).
Results
The Correlations Between SCD and Subjective versus Objective Sleep
Individual analysis showed that older adults’ SCD was significantly correlated with their subjective insomnia (r = 0.27, p < .01) and that greater perceived insomnia predicted higher SCD, while the correlation with PSQI was not significant (r = 0.07, p = .48). However, the correlations between SCD and objective sleep parameters were not significant (Table 2).
Mediation Modeling
Mediation effect analysis was performed using model 4 in the PROCESS program developed by Hayes (Hayes, 2013). The results showed that the predictive effect of subjective insomnia on depression (β = 0.50, p < .001) and SCD (β = 0.27, p < .01) was significant. After adding depression as a mediator, the predictive effect of subjective insomnia on SCD was non-significant (β = 0.07, p = .49), indicating a mediation effect of depression on the association between subjective insomnia and SCD (Table 3).
the Mediation Effect of Depression on the Association Between Subjective Insomnia and SCD
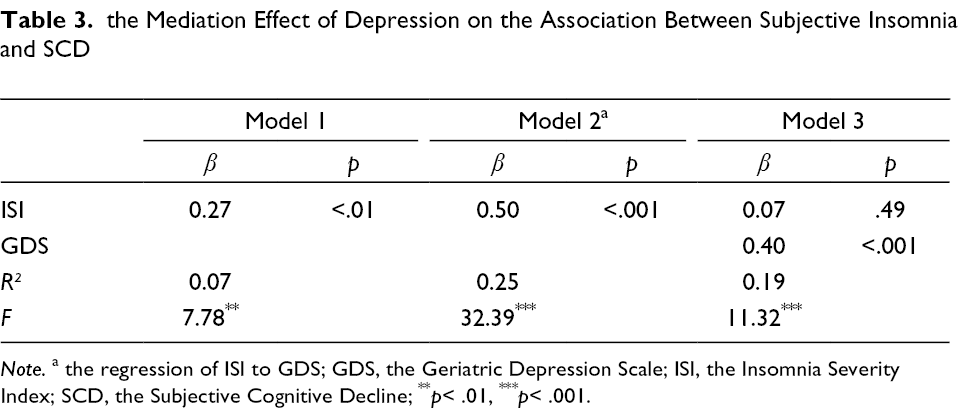
Note. a the regression of ISI to GDS; GDS, the Geriatric Depression Scale; ISI, the Insomnia Severity Index; SCD, the Subjective Cognitive Decline; ** p< .01, *** p< .001.
In addition, the percentile Bootstrap test indicated that the indirect effect of subjective sleep on SCD through depression severity was significant (95 % BootCI = [0.08, 0.36]). The direct effect (0.07) and indirect effect (0.20) accounted for 27.29% and 72.71% of the total effect respectively.
Discussion
To investigate the relationship between sleep and SCD in community-dwelling older adults, we found that SCD was correlated with subjective insomnia (i.e., ISI) rather than objective sleep (i.e., actigraphic data). Furthermore, this identified link between subjective insomnia and SCD was mediated by depression that both subjective insomnia and cognitive decline may be at least partially underpinned by depression symptoms. These findings indicate that subjective insomnia may explain SCD variations better than objective sleep and this study is the first to determine the mediator role of depression on the relationship between subjective insomnia and SCD.
Older adults’ SCD associated with their subjective insomnia rather than objective sleep, which is inconsistent with the results of other stages on the AD continuum (i.e., MCI and AD). With respect to AD, there was a salient dysregulation of sleep-wake cycle, featured by sleep fragmentation and irregular sleep-wake rhythm (Liguori et al., 2020). Moreover, these objective sleep disruptions have been found to be correlated with AD biomarkers, such as amyloid deposition, tau pathology, neuroinflammation, and oxidative damage (Liguori et al., 2020; Targa et al., 2020). Similar substantial objective sleep alterations were also observed in MCI patients (Basta et al., 2019; D'Rozario et al., 2020; Liu et al., 2020). For example, using ahome-based portable device WatchPAT (Itamar Medical Inc., Caesarea, Israel) that can simultaneously measure the peripheral arterial tone (PAT) signal, pulserate, oximetry, actigraphy, body position, snoring and chest motion, the study found that both AD and MCI patients showed a significantly reduced rapid eye movement (REM) sleep and increased light sleep as compared to normal controls, while the subjective PSQI and ESS scores generally showed no difference (Tadokoro et al., 2020). In contrast, the present study and one previous study (Tardy et al., 2015) found that SCD, unlike AD and MCI, was significantly associated with subjective sleep, but not associated with objective sleep (i.e., parameters from actigraph or a nocturnal ambulatory polygraphy). Combining these existing findings, it seems that subjective and subjective indices are related, and objective and objective indices are related, which is unsurprising. As a very early preclinical stage of AD, older adults with SCD only report a cognitive function decline on the subjective level, and this self-awareness of cognitive impairments may have common variability with the awareness of sleep disruptions. On the other hand, older adults with AD and MCI could have difficulties for the understanding of items from subjective sleep assessments, which may bring the inaccurate evaluation results and insensitivity of subjective measurements. However, we need to be cautious when inferring this finding, at least with the consideration of the following aspects. First, so far, there is no unified method for SCD assessment, including but not only with a single or multiple self-made items (e.g., “Do you feel as if your memory is worsening?”; Leng et al., 2020) and standardized scales (e.g., the subjective memory complaints questionnaire; Kang et al., 2017). Moreover, different scoring methods (e.g., categorically versus discretely) could also affect the results (Bubbico et al., 2019; Kang et al., 2017). Second, subjective sleep measurements are different. Other than the PSQI that assesses global sleep quality with seven dimensions, there are several standardized questionnaires measuring different characteristics of sleep, such as the ISI for insomnia, the RBDSQ for REM sleep disorders, and the ESS for sleepiness. In our study, we found that subjective insomnia was more sensitive than the PSQI in terms of the relationship with SCD. Third, in the process of cognitive aging, sleep changes may be non-linear, which requires in-depth analysis in further longitudinal research (Cavuoto et al., 2016).
Previous studies have shown that shorter and longer sleep duration, as compared with normal sleep duration, was significantly associated with an increased risk for depression (Zhai et al., 2015). In addition, this association between depression and sleep was distinctly shown with subjective sleep but not with objective sleep, implicating that subjective sleep may be a stronger trait marker for subthreshold depression symptoms (Gould et al., 2018). Our mediation model further suggests that there may be comorbidities among subjective insomnia, cognitive decline, and depression. In late-life neurodegenerative diseases, both sleep disturbance and depression may be at least partially underpinned by cerebrovascular changes. For instance, aggregation and accumulation of amyloid-β (Aβ), which contributes to the development of AD, has been found to be associated with sleep disruptions and worsening of mood (Steiger & Pawlowski, 2019). Through the deepening of subjective perception of insomnia, individuals may generate more negative emotions, especially depression, which could lead to subjective perception of cognitive decline.
The present study has some limitations that need to be considered. First, this study may be biased in its sampling (e.g., more than 67 % of participants were females, and all participants belonged to one ethnic group, that is, Chinese Han). Thus, acaution should be taken when generalizing the current findings to populations with different sociodemographic characteristics. Second, this study used a cross-sectional study design that we cannot formally test mediating relationships of longitudinal, causal associations between subjective sleep and SCD. Further longitudinal studies are needed to examine the potential longitudinal development of this association. Third, the use of actigraphy in this study allowed the noninvasive assessment of objective sleep. However, future polysomnographic studies are needed to characterize macro- and micro-sleep architecture in older adults with SCD and for objectively assessing the presence of other sleep pathologies.
Conclusion
The findings of our study suggest that the subjective measure of insomnia captures subtle differences in sleep better than objective sleep, and is an indicator for older adults’ SCD that is independent of objective sleep. At the same time, depression played a mediating role in this association. These findings extend our perspective on the relationship between sleep disruption and cognitive decline, and highlight the need for early and targeted intervention on sleep to reduce the risk of subsequent cognitive impairment progression.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship,and/or publication of this article: This work was supported by the National Natural Science Foundation of China (31971007, 31971028), the Ministry of Education of Humanities and Social Science project (17YJA190015), and the CAS Key Laboratory of Mental Health, Institute of Psychology (KLMH2019K02).
Author Biographies