
Abstract
This study aimed to examine the associations of both subjectively and objectively measured sleep with physical activity among older adults and to explore the possible moderating role of chronotype in these associations. We included baseline data of 116 community-dwelling older adults without dementia from three prior studies. Pittsburgh Sleep Quality Index and Actigraphy were used as subjective and objective sleep measures, respectively. Physical activity was assessed by the Physical Activity Scale for the Elderly. The Morningness–Eveningness Questionnaire was used to measure chronotype, which was further dichotomized into morning type and non-morning type. Multiple linear regressions were performed to examine the associations, controlling for demographic and health characteristics. We found that better subjective sleep quality, shorter actigraphy sleep duration, and higher actigraphy sleep efficiency were uniquely associated with greater physical activity. Being a morning type might alleviate the adverse association between poor subjective sleep quality and physical activity among older adults.
The health benefits of physical activity in older adults have been well documented (Nuzum et al., 2020; Piercy et al., 2018). Being physically active reduces the risks of all-cause mortality, chronic medical conditions, functional disabilities in older adults, and improves the quality of life and mental health outcomes (Cunningham et al., 2020). Although older adults benefit more from physical activity in preventing disability and promoting health, it is more difficult to engage older adults in physical activity than younger adults (Ussery et al., 2021; Zhao et al., 2020). A national survey has suggested that the prevalence of physical inactivity among older adults increased significantly from 1998 to 2018 (Whitfield et al., 2021). In 2018, only 11% of older adults in the United States fully met the physical activity guidelines of 150 min of moderate to vigorous activity weekly (Zhao et al., 2020).
Sleep is also a key determinant of health among older adults. Older people tend to have more difficulty falling asleep and maintaining sleep (Li et al., 2018a). As such, approximately half of older adults experience sleep difficulties (Neikrug & Ancoli-Israel, 2010). In older adults, poor sleep, such as insufficient sleep duration and more frequent awakenings, is associated with poorer quality of life; reduced cognitive health and mental health; and higher risks for frailty, cardiovascular diseases, and mortality (Guida et al., 2021; Stone & Xiao, 2018; Wang et al., 2017).
As both physical activity and sleep are lifestyle factors that play pivotal roles in the well-being of older adults, many studies have been conducted to understand their association (Kredlow et al., 2015; Li et al., 2018b). Most of the studies focused on the association of physical activity with sleep (e.g., Li et al., 2018). Clinical trials and systematic reviews have found that physical activity improves sleep (Kredlow et al., 2015; Vanderlinden et al., 2020). Conversely, sleep can also impact the level of physical activity, as better sleep can reduce daytime sleepiness and fatigue, facilitating a more active lifestyle (Kline, 2014). Several observational studies suggest that better sleep quality is associated with higher physical activity levels in older adults (Huang et al., 2021; Vaingankar et al., 2020). Best et al. (2019), however, found no significant association between sleep quality and physical activity (Best et al., 2019). Given the inconsistent findings, more evidence is required.
Furthermore, studies investigating the association between sleep and physical activity have mostly used subjective sleep measures only. Research has found discrepancies between subjectively and objectively measured sleep in older adults and suggests that both approaches provide unique information and complement each other in assessing sleep (Hughes et al., 2018; Landry et al., 2015). Objective sleep measures attempt to estimate sleep parameters unbiasedly, and subjective sleep measures capture an individual's self-perceived sleep quality. Therefore, a combination of subjective and objective sleep measures could assess sleep in older adults more comprehensively than a single measure alone.
Chronotype refers to an individual's time preference for daily sleeping, waking, and activity, and has been termed morningness–eveningness (Danielsson et al., 2019). Chronotype is often categorized as morning type, evening type, or intermediate type. Recent research found that chronotype is also associated with physical activity in older adults (Thapa et al., 2020). Morning type older people had significantly higher levels of physical activity than evening people (Thapa et al., 2020). As such, it is possible that chronotype plays a role in the relationship between sleep and physical activity among older adults, which has not been studied.
The aims of this study are to examine the cross-sectional association between sleep and physical activity among older adults using both subjective and objective sleep measures and to explore the moderating role of chronotype. Our hypotheses are: (1) both subjective and objective sleep parameters are associated with the self-reported physical activity of older adults; (2) the associations are moderated by chronotype. Findings from this study will deepen our understanding of how different aspects of sleep in association with physical activity, provide implications for future research and for clinicians, and thus promote physical activity in older adults through modifying sleep behaviors.
Method
Study Setting and Participants
This study is a secondary data analysis of combined baseline data from an ongoing randomized controlled trial (RCT; n = 87) and two completed pilot studies (Li et al., 2020 [n = 8]; Li et al., 2021 [n = 21]) examining the efficacy of a personalized behavioral intervention for improving the physical activity and sleep among sedentary older adults. Participants were recruited from geriatric clinics or local communities. The inclusion and exclusion criteria were similar across the three studies. Older adults were included if they met all of the following criteria: (1) 60–85 years of age; (2) had no diagnosis of dementia or a Montreal Cognitive Assessment (MoCA) score >18 (Nasreddine et al., 2005); (3) self-reported >5 h/day of sedentary activity; (4) able to do mild to moderate physical activity; (5) self-reported poor quality sleep; (6) not diagnosed with sleep apnea; and (7) understood English. Among the total 116 participants, only 87 had data on chronotype; therefore, the moderating effect of chronotype (hypothesis 2) was examined using these 87 samples. The parent studies obtained approvals from the institutional review boards at the University of Pennsylvania School of Medicine or Johns Hopkins Medicine.
Measures
Demographic and Health Characteristics
Demographic information was collected, including age, gender, and race. Health characteristics in terms of body mass index (BMI), cognitive function, and the number of chronic conditions were also included. BMI was calculated as weight (kg) divided by height (m2). Cognitive function was determined by the MoCA, a widely used cognitive screening tool that measures visuospatial/executive function, naming, episodic memory, attention, language, abstraction, and orientation (Nasreddine et al., 2005). If the MoCA score fell between 18 and 25, participants were categorized into mild cognitive impairment (MCI), and if the MoCA score was 26–30, they were categorized into normal cognitive function. The number of chronic conditions was assessed by the number of diagnoses of the following conditions: cancer, hypertension, hyperlipidemia, cardiovascular disease, depression, stroke, diabetes, chronic obstructive pulmonary disease, renal diseases, sleep disorders, and arthritis.
Objective Sleep
Data on objective sleep were recorded using Actiwatch 2 (Philips Respironics Inc., Murrysville, PA), downloaded onto Actigraphy analysis software, Actiware (Philips, v6.0), and analyzed using low sensitivity for wakefulness (20 counts/min) setting. Participants wore the wristwatch device on the nondominant hand for 7–9 days and completed sleep diaries to help verify the time in and out of bed. The objective sleep variables were averaged over the days of wearing to account for intrasubject variability, and a previous study has suggested that a 7-day aggregate or longer was reliable in older adults (Van Someren, 2007). The variables include nocturnal sleep duration, sleep onset latency, wake after sleep onset (WASO), and sleep efficiency. Nocturnal sleep duration is the total duration of sleep in minutes from initial sleep onset to the last minute of asleep through the night. Sleep onset latency is the number of minutes that one takes to fall asleep after lights off; the longer, the more difficult in initiating sleep. WASO refers to the number of minutes awake after initial sleep onset, which is an indicator of sleep fragmentation. Sleep efficiency is the proportion of time asleep compared to the total time in bed and is a core indicator of sleep quality (Reed & Sacco, 2016).
Subjective Sleep
The Pittsburgh Sleep Quality Index (PSQI) was used to measure subjective sleep over the past month (Buysse et al., 1989). It comprised 19 self-rated sleep questions, which were grouped into seven components: subjective sleep quality, sleep onset latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction. A global score ranging from 0 to 21 was obtained by summing these components; the higher score, the poorer the sleep quality.
Chronotype
The Morningness–Eveningness Questionnaire (MEQ) was used to assess chronotype. MEQ consists of 19 self-reported items regarding sleep and wake times, preferred times for physical and mental activities, and subjective alertness (Horne & Ostberg, 1976). The items were rated on 4- to 5-point Likert scales, with a total score ranging from 16 to 86. Cutoffs of 42 and 58 were usually applied to define evening, intermediate, and morning types (Horne & Ostberg, 1976; Taillard et al., 2004). Consistent with a prior study, MEQ scores were dichotomized into morning type (>58) and non-morning type (≤58) due to the few samples in evening type (Quante et al., 2019).
Physical Activity
Physical activity was assessed using the Physical Activity Scale for the Elderly (PASE), a validated and widely used self-reported physical activity measure for older adults (Washburn et al., 1993). It included 12 components in terms of three types of physical activity over the past seven days: leisure time activity (five components), household activity (six components), and work-related activity (one component). Leisure time activity included walking outside, light, moderate, and strenuous sports/recreational activities, and muscle strength/endurance exercises. The items of leisure time activity asked for both frequency (never, 2 days, 3–4 days, and 5–7 days) and duration (<1 h, 1–2 h, 2–4 h, and >4 h). Household activity included light or heavy housework, home repairs, lawn work or yard care, outdoor gardening, and caring for another person. Responses to these activities are dichotomous (yes or no). Work-related activity referred to jobs involving standing or walking, and the number of hours per week was reported. Multiplying the frequency of each activity by the item weight and summing all the activities yielded the total PASE score. Higher scores indicated higher levels of physical activity.
Statistical Analysis
Means and standard deviations (SDs) were used to describe continuous variables and frequencies; percentages were used to present categorical variables. Spearman's bivariate correlations were conducted to explore the correlations between variables and to detect multicollinearity. Multiple linear regression analyses were conducted to examine the associations between sleep measures and physical activity. To check the multicollinearity of the models, the variance inflation factor (VIF) statistic was used; VIFs lower than four are defined as absent evidence of multicollinearity (Miles & Shevlin, 2001). The objective sleep measures and PSQI scores were first examined individually as an independent variable in Models I–V, respectively, and then examined together in Model VI. Given the known associations with sleep and/or physical activity, all models controlled for the following demographic and health characteristics: age, sex, race, BMI, cognition, and number of chronic conditions. Lastly, we added chronotype into Model VI and yielded Model VII. Then, to examine the moderating effect of chronotype on the association between sleep and physical activity, the interaction terms of chronotype and each sleep variable were built and added to Model VII individually. Only significant interaction terms were kept and presented as Model VIII. All statistical analyses were performed using IBM SPSS V26.0 (IBM Inc., Armonk, NY, USA) and a p-value <.05 was set as statistically significant.
Results
Among the 116 participants, 63.8% were female, 48.3% were White, and 33.6% might have had MCI (18 ≤ MoCA ≤ 25). On average, participants were aged 71.93 years (SD = 6.26) and had approximately three chronic conditions. Table 1 displays the participants’ demographic characteristics, physical activity, and sleep at baseline.
Participant Characteristics.
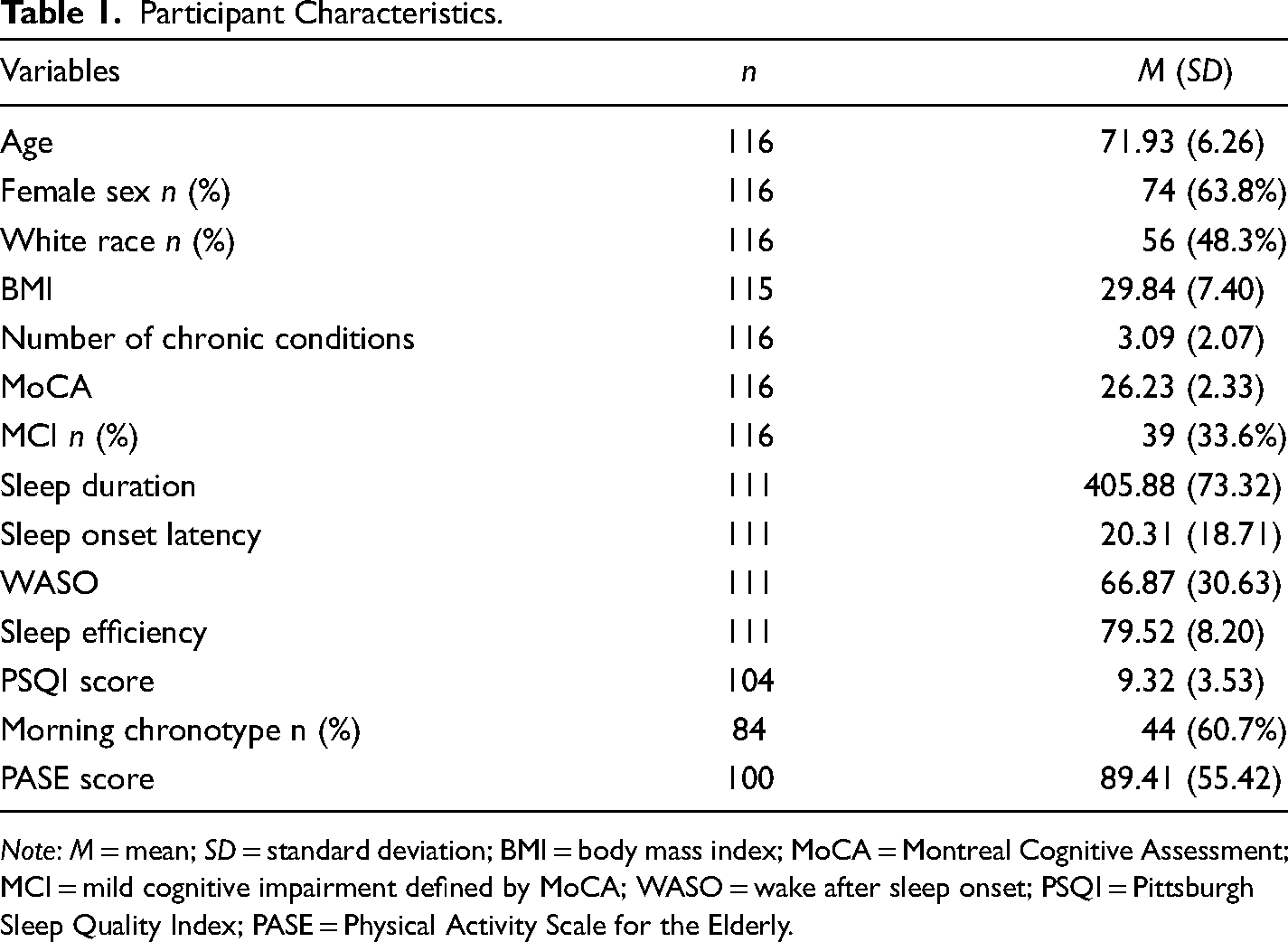
Note: M = mean; SD = standard deviation; BMI = body mass index; MoCA = Montreal Cognitive Assessment; MCI = mild cognitive impairment defined by MoCA; WASO = wake after sleep onset; PSQI = Pittsburgh Sleep Quality Index; PASE = Physical Activity Scale for the Elderly.
Table 2 displays the bivariate correlations across all variables. Between the objective sleep measures, WASO was positively correlated with sleep onset latency (r = 0.37, p < .01). Sleep efficiency was positively correlated with sleep duration (r = 0.45, p < .01), but was negatively correlated with sleep onset latency (r = −0.65, p < .01) and WASO (r = −0.83, p < .01). We found small but significant correlations between subjective and objective sleep measures. PSQI scores were correlated with WASO (r = 0.29, p < .01) and sleep efficiency (r = −0.21, p < .05).
Bivariate Correlations Across all the Variables.
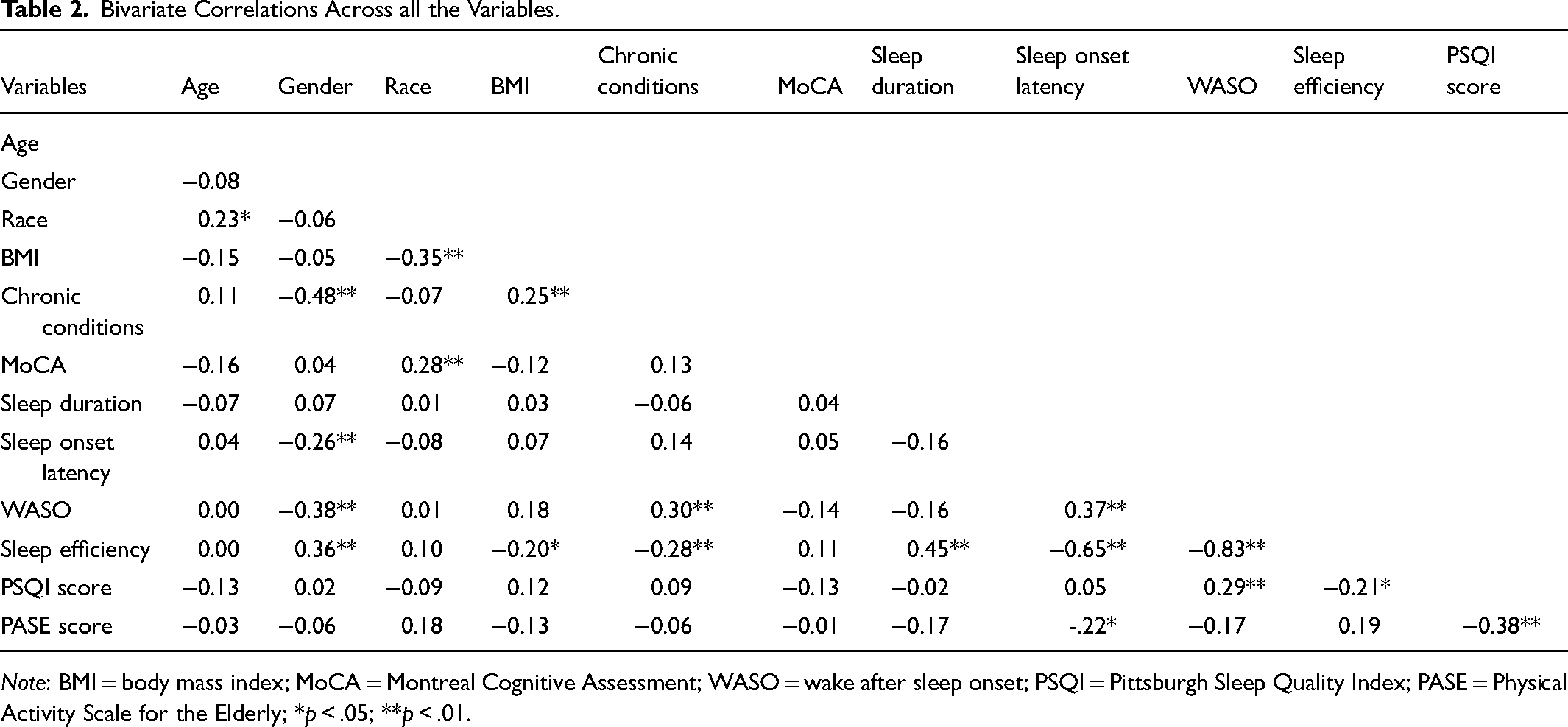
Note: BMI = body mass index; MoCA = Montreal Cognitive Assessment; WASO = wake after sleep onset; PSQI = Pittsburgh Sleep Quality Index; PASE = Physical Activity Scale for the Elderly; *p < .05; **p < .01.
The results of the multiple linear regressions are shown in Table 3. No evidence of multicollinearity was found, as the VIF values of all the independent variables were lower than 2 across the different models. According to Models I–V, all sleep variables, except for sleep duration, were individually associated with PASE scores, after adjusting for demographic and health characteristics. Specifically, shorter sleep onset latency (b = −0.75, 95% confidence interval [CI]: −1.47 to −0.03, p < .05), lower WASO (b = −0.41, 95% CI: −0.79 to −0.03, p < .05), better subjective sleep quality (b = −6.36, 95% CI: −9.44 to −3.29, p < .001), and higher sleep efficiency (b = 1.49, 95% CI: 0.01–2.96, p < .05) were significantly associated with higher levels of physical activity. Furthermore, as bivariate correlation results indicated that sleep efficiency was highly correlated with sleep onset latency and WASO, Model VI included sleep efficiency, sleep duration, and PSQI scores, but not sleep onset latency or WASO. The results showed that a lower PSQI score (better subjective sleep quality) (b = −5.94, 95% CI: −8.99 to −2.88, p < .001), shorter sleep duration (b = −0.24, 95% CI: −0.39 to −0.09, p < .01), and higher sleep efficiency were significantly related to an increased PASE score (b = 2.14, 95% CI: 0.61–3.68, p < .01).
The Association Between Sleep and Physical Activity Controlling for Demographic and Health Variables.

Note. b = unstandardized coefficient; CI = confidence interval; BMI = body mass index; MoCA = Montreal Cognitive Assessment; WASO = wake after sleep onset; PSQI = Pittsburgh Sleep Quality Index; *p < .05; **p < .01; ***p < .001.
When testing the moderating effect of chronotype, we found that the interaction term of chronotype and PSQI score was significantly associated with PASE scores; all other interaction terms were nonsignificant. As shown in Table 4, chronotype was not significantly associated with physical activity when the interaction of a morning type and PSQI score was not adjusted for (Model VII), but it was significant after adding the interaction term (Model VIII). Being a morning type reduced the negative association between poor subjective sleep quality and physical activity (b = 11.44, 95% CI: 5.03–17.85, p < .01).
The Moderating Effect of Chronotype on the Association of Sleep and Physical Activity.
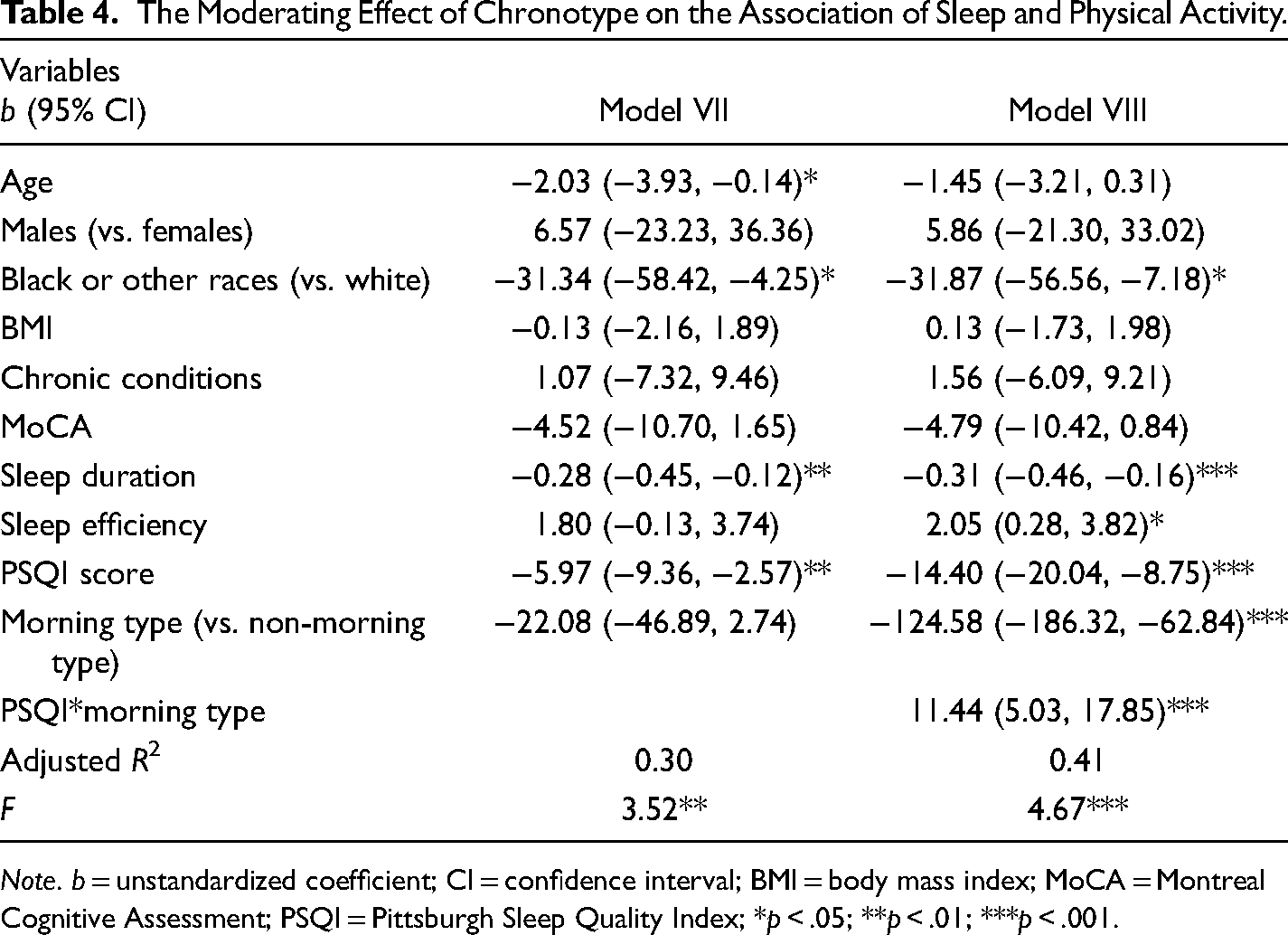
Note. b = unstandardized coefficient; CI = confidence interval; BMI = body mass index; MoCA = Montreal Cognitive Assessment; PSQI = Pittsburgh Sleep Quality Index; *p < .05; **p < .01; ***p < .001.
Discussion
We examined the associations of both objective and subjective sleep measures with the levels of physical activity among community-dwelling older adults and explored the moderating effect of chronotype on this association. The results supported our hypotheses. When examining the sleep indicators simultaneously, objective sleep duration, objective sleep efficiency, and subjective sleep quality were unique from each other in association with a participant's physical activity, controlling for demographic and health characteristics. We also found that chronotype moderated the association between subjective sleep quality and physical activity, with the morning type alleviating the negative relation of poor sleep quality to physical activity.
The findings strengthen the current evidence of the association between sleep and physical activity by including both subjective and actigraphy sleep measures. We found that longer sleep onset latency, greater WASO, poorer sleep efficiency, and worse subjective sleep quality were associated with a lower level of physical activity. This aligned with a cross-sectional study in older women (Lambiase et al., 2013), which used the same actigraph-measured sleep indicators. Two longitudinal studies (Holfeld & Ruthig, 2014; Huang et al., 2021) also demonstrated that greater subjective sleep quality at baseline was associated with a higher level of physical activity at follow-up among middle-aged and older adults.
The results regarding sleep duration and physical activity were inconsistent among the previous studies. Some studies found no association between sleep duration and physical activity (Kline et al., 2017; McClain et al., 2014); some found a positive association (Kredlow et al., 2015; Štefan et al., 2018). Consistent with Savin et al. (2021), we found that shorter sleep duration was associated with more physical activity. A possible explanation may be that time spent in physical activity and sleep might compete in a 24-h day and shorter sleep time might enable individuals to be more engaged in other activities (Savin et al., 2021). In particular, when the physical activity was measured by PASE, which takes leisure activity, household activity, and work-related activity into account, it is possible that people with shorter sleep were involved in more social or occupational activities. This is supported by the study of Hispanic/Latino adults aged 18–74 years, which found that shorter sleep was associated with more work-related physical activity (Tom et al., 2020). In addition, the association between sleep duration and physical activity was only significant when adjusting for sleep efficiency and subjective sleep quality, suggesting that future studies should control for sleep quality indicators when examining the association.
Furthermore, we found that—according to the guide for interpreting correlations in medical research—subjective PSQI score was correlated with only two objective indicators (WASO and sleep efficiency) and to a negligible extent (Mukaka, 2012). Both subjective and objective sleep measures provided unique information on the relationship of sleep to physical activity. This aligned with the findings of the previous studies that there were certain discrepancies between subjective and objective measures and that they might supplement each other by capturing different aspects of sleep among older adults (Landry et al., 2015; O’Donnell et al., 2009). The discrepancy might be contributed by the limitations of both objective and subjective measures (Hughes et al., 2018). The objective sleep measure (i.e., wrist actigraphy) was critiqued with some potential measurement errors, such as failing to discover participants’ waking up early and misinterpreting lying quietly before going to sleep as sleep (Kreutz et al., 2021). The subjective sleep measure (i.e., PSQI) was vulnerable to recall bias and relies on the cognitive function and personal perceptions of participants (O’Donnell et al., 2009). A third of our participants might have had MCI, which might have contributed to the discrepancy. Even though PSQI was found to have satisfactory reliability in older people with MCI (Bademli et al., 2019), inaccuracy in their self-reported sleep is possible. But the present study places more emphasis on the self-perception of sleep, rather than accuracy. Older adults tend to perceive their sleep quality differently from objective reality, although there is no consensus yet. While O’Donnell et al. (2009) found that older adults were likely to perceive their sleep quality positively, Landry et al. (2015) found that older adults were more likely to underestimate their sleep quality.
Moreover, the mechanisms of the association between sleep and physical activity remain unclear (Kredlow et al., 2015). Our finding of the moderating effect of chronotype may shed some light on further understanding of the association. Being a morning type might protect against the relation of poor subjective sleep quality to physical activity among older adults. Glavin et al. (2021) found that chronotype moderated the relationship between exercise timing and bedtime. A meta-analysis found that the time of day of exercise moderated the effect of physical activity on sleep (Kredlow et al., 2015). Even though these studies did not examine the moderation of chronotype directly, they have indicated that the time preference of activities might influence the association between sleep and physical activity. The protective effect of a morning type was expected as several previous studies have found that older adults with the morning type were more physically active (Chaput et al., 2020; Thapa et al., 2020).
The findings of the present study highlight the importance of sleep assessment and provide implications for clinical practices and future research to promote active aging through addressing sleep problems in older adults. Patient's sleep was not routinely assessed or documented in clinical practice (Sun et al., 2021), and sleep disturbances among older adults were often underestimated (Bloom et al., 2009). Therefore, it is essential to pay more attention to sleep health in older adults to promote their health (Guida et al., 2021; Stone & Xiao, 2018), including but not limited to the physical activity that was found in our study. Given the important roles of both sleep and physical activity in the overall health of older adults and the fact that they are modifiable, sleep practices/interventions are encouraged, such as sleep hygiene education, stimulus control therapy, and relaxation techniques (Holfeld & Ruthig, 2014).
Our findings extend the current knowledge by indicating the unique insights of both objective and subjective sleep on the association with physical activity. Future studies should consider incorporating both objective and subjective measures when investigating the association between sleep and physical activity. Also, the present study focuses on the relation of sleep to physical activity, as the relation of physical activity to sleep is well-established (Kredlow et al., 2015). Further RCTs are needed to better understand the potentially reciprocal relationship and to explore whether interventions that target one (either physical activity or sleep) can benefit both. Moreover, studies need to further test whether the impact of sleep on physical activity differs between morning type older adults and non-morning type older adults.
A strength of the present study is that sleep was comprehensively assessed using a combination of both subjective and objective sleep measures. In addition, to the best of our knowledge, our study is the first attempt to examine the moderating effect of chronotype on the association of sleep and physical activity. Nevertheless, the results should be interpreted in the context of several limitations. First, the data we used were from three clinical trials in which differences might have existed even with the same sample eligibility criteria used across the trials. In the analysis, we added study difference as a covariate, no significant difference was shown across the studies in terms of the association between sleep and physical activity. Second, the clinical trials attempted to recruit older adults with self-reported sleep problems. Given the evidence that older adults with worse sleep may be less physically active, the association of sleep and physical activity found in this study might be different from the general older adult population. Third, the sample size was small, but we conducted a power analysis and confirmed the models of our major findings (i.e., Model VI, Model VII, and Model VIII) had a statistical power >0.85. Fourth, as secondary data analysis, there might be unmeasured confounders that were not adjusted for; for example, depressive symptoms (Garfield et al., 2016). Fifth, physical activity was assessed subjectively with PASE. Even though it is a validated tool, objective measures of physical activity may provide additional information to supplement the findings in the present study. Last, the cross-sectional design did not allow for any causal inferences. Future larger-scale studies with longitudinal designs or RCTs are needed to further investigate sleep's impact on physical activity in older adults.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Nursing Research (grant numbers K23NR018487, P30NR018093, and R00NR016484).