
Abstract
Diversion programs were developed to decrease the number of incarcerated mentally ill individuals. The number of diversion programs and mental health courts is rapidly growing, and an increased number of diversion programs are willing to accept defendants charged with violent felonies, stressing the need for thorough risk assessments as part of diversion eligibility evaluations. This study was designed to examine the utility of the Historical–Clinical–Risk Management–20 (HCR-20) and Psychopathy Checklist Screening Version (PCL:SV) in predicting diversion noncompliance and reincarceration in a sample of 131 defendants participating in different diversion programs in New York. Results provided support for the use of the HCR-20 and PCL:SV in the context of diversion, although the HCR-20 proved to be superior to the PCL:SV in predicting diversion noncompliance and reincarceration.
The main goal of diversion programs is to decrease the number of individuals with psychiatric disorders in the criminal justice system by offering treatment in the community in lieu of a jail sentence. The establishment of such programs was a major recommendation of the National Coalition for Jail Reform as early as the 1970s, and over the past 40 years significant progress has been made in the creation and implementation of these programs. Steadman, Cocozza, and Veysey (1999) defined jail diversion as programs that screen detainees for the presence of mental illness and employ mental health professionals to evaluate the detainees and to collaborate with attorneys, community treatment providers, and the courts to link mentally ill defendants with community-based mental health services. In 1992, a national survey estimated that 52 jail diversion programs existed in the country (Steadman, Morris, & Dennis, 1995). Today, there are more than 300 diversion programs operating nationally (Steadman & Naples, 2005). When first developed, diversion programs were decentralized in that referrals could be made from unspecialized courts. However, as part of a larger movement of therapeutic jurisprudence (Wexler, 2001), centralized diversion was developed through mental health courts, a type of special jurisdiction courts where all defendants are handled in a single court docket (Steadman, Davidson, & Brown, 2001). There has also been a rapid increase in the number of mental health courts from 1 in 1997 to more than 100 today (National GAINS Center, 2002).
Although diversion programs around the nation vary in a number of ways, regardless of whether the diversion takes place through mental health courts or is decentralized, most courts require defendants to take a guilty plea prior to being released to treatment in the community. Diversion programs employ a collaborative team, which includes clinicians who develop treatment plans and make linkages to treatment. Availability of appropriate clinical placement is ensured prior to the judge making a ruling regarding diversion, and the court requires specialized monitoring of participants with possible sanctions for noncompliance, including reincarceration (Steadman et al., 2001). In addition to compliance with the treatment plan, other requirements usually include regular court review hearings, meetings with case managers, and repeated random toxicology exams (Redlich, 2005). Incentives to participate include the dismissal or reduction of charges on completion of a predetermined period of treatment and court supervision. Alternatively, if defendants do not comply with the conditions set forth by the diversion program, they are sentenced to a prison term that is negotiated before entering the guilty plea.
A review of the available program evaluation research suggests that individuals diverted and monitored by diversion programs receive better linkages to the community, receive more treatment services, and show a reduction in reincarceration rates (Cosden, Ellens, Schnell, Yamini-Diouf, & Wolfe, 2003; Steadman, Cocozza, et al., 1999; Steadman, Deane, et al., 1999). However, despite the fact that a key component of diversion is the evaluation of defendants by mental health professionals for eligibility for diversion (Steadman, Cocozza, et al., 1999), to our knowledge no national survey has been conducted to identify diversion assessment practices. Anecdotal observations suggest that very few programs utilize any standardized psychological assessment instruments or risk assessment tools as part of diversion evaluations. Decision makers are continuously called to assess whether mentally ill incarcerated individuals are “safe enough” to be released from jails and prisons or whether they pose a danger to the community (Douglas, Yeomans, & Boer, 2005, p. 479). It is now widely accepted that clinical judgment of future risk of violence is greatly improved by the addition of structured risk assessment tools (Grey et al., 2004; Litwack, 2001). However, no published study was found that assessed the utility of any psychological assessment tool to predict compliance or reincarceration in the context of criminal justice diversion.
Although diversion programs were initially developed to target a population of nonviolent offenders, a movement toward a second generation of mental health courts that accept more felonies has been identified (Redlich, Steadman, Monahan, Petrila, & Griffin, 2005). An increased number of diversion programs are more willing to accept individuals with violent offenses applying a “totality of the circumstances approach” (Redlich et al., 2005, p. 534). For instance, it is not rare for the district attorney’s offices in New York City to consider individuals charged with attempted murder for participation in diversion. As diversion programs accept more felonies, they also tend to use jail as a sanction for noncompliance more frequently (Redlich, 2005). In addition, individuals charged with felonies face longer prison sentences if noncompliant than do individuals charged with misdemeanors. Inclusion of risk assessment tools in the diversion evaluation process is important because the goal of diverting the mentally ill from the criminal justice system should not be attained at the expense of public safety. The fact that an increased number of potential diversion participants may be charged with violent offenses, may have been convicted of violent crimes in the past, and may face longer prison sentences if noncompliant underlies the importance of using risk assessment tools to maximize success and minimize the chances of recidivism in the community.
The lack of comprehensive risk assessments likely prevents mentally ill individuals from being appropriately matched with treatment and intensity of court supervision. Even though diversion programs are growing in number, community-based services are limited. Typically, once an individual has been accepted for diversion, linkage with the appropriate treatment program can be delayed several months. Thus, a considerable number of those accepted for diversion wait in jail for long periods of time. A follow-up study of more than 1,000 individuals diverted through a mental health court found that about one fifth were later rediverted through the same program at least once because of a new arrest that led to reincarceration (Boccaccini, Christy, & Poythress, 2005). A thorough risk assessment could help determine whether the level of risk can be managed in the community and could also allow diversion programs to identify the risk factors that should be a target both for treatment providers and case managers providing judicial supervision. Therefore, appropriate risk assessments could potentially reduce the number of reincarcerations and rediversion.
Some diversion programs continue to accept only persons charged with nonviolent misdemeanors. It has been argued that these programs are likely to continue to restrict access to nonviolent offenders because accepting riskier cases can jeopardize the continuation of mental health courts (Wolff, 2002). However, the only study comparing violent and nonviolent diverted offenders showed no difference in treatment compliance or rate of recidivism. These results did not support the exclusion of individuals solely based on their intake offense (Naples & Steadman, 2003). It is arguable that a more comprehensive risk assessment would be more informative when determining individuals’ eligibility for diversion, as opposed to eliminating individuals based solely on the severity of the current charge.
Both the Psychopathy Checklist Screening Version (PCL:SV; Hart, Cox, & Hare, 1995) and the Historical–Clinical–Risk Management–20 (HCR-20) violence risk assessment scheme (Webster, Douglas, Eaves, & Hart, 1997) have been widely used and validated and are reliable measures for predicting future violence and recidivism among adult mentally ill individuals. The HCR-20 (Webster et al., 1997) is a structured professional judgment (SPJ) tool in which the instrument is used to guide the clinician’s evaluation to include risk factors that research has shown to have predictive value for future violence. The HCR-20 was developed using a logical guide intended to structure decisions made by professionals about future violence by encouraging the consideration of 20 key violence risk factors. This scale includes Historical (H), Clinical (C), and Risk Management (R) factors and avoids using cutoffs for classification of risk to allow for professional judgment (Grey et al., 2004). Several published studies have found a relationship between HCR-20 scores (both total and subscale scores) and violence with moderate to large effect sizes (see Douglas, Guy, & Weir, 2005, for a review of studies on the HCR-20).
An area of debate within the risk assessment literature is whether specific assessment of defendants’ personality traits that are believed to correlate with recidivism should be used over general risk assessment tools that were specifically designed for the identification of high-risk offenders. (Wormith, Stevenson, Olver, & Girard, 2004). The PCL and its variants (e.g., Psychopathy Checklist–Revised [PCL-R]—Hare, 1991; PCL:SV—Hart et al., 1995) have dominated the area of personality evaluation within the field of risk assessment (Grey et al., 2004). The PCL:SV is a shorter version of the PCL-R and consists of 12 items. When first developed, the PCL was thought of not as a risk assessment tool but as a psychometric measure of psychopathy (Porter & Woodworth, 2006). Research has consistently shown that Hare’s measures of psychopathy, although not intended as risk assessment measures per se, predict violence and recidivism, particularly violent recidivism, among released offenders (Porter, Birt, & Boer, 2001; Salekin, Rogers, & Sewell, 1996; Walters, 2003a). Most studies have found that PCL’s Factor 2 (socially deviant–impulsive lifestyle component) is more predictive of general and violent recidivism than PCL’s Factor 1 (affective–interpersonal component; Douglas, Yeomans, & Boer, 2005; Hemphill, Hare, & Wong, 1998; Walters, 2003b). These results provide support for the theory that the behavioral features of psychopathy tend to be better predictors of violence and recidivism than the core personality features of psychopathy (Douglas, Yeomans, & Boer 2005; Skeem & Mulvey, 2001).
Recent studies have suggested that the PCL and other risk assessment tools lack instrument-outcome specificity (Coid et al., 2011). For example, although the HCR-20 was developed to predict risk for violence, it also predicts general offending (Coid et al., 2009). Even though the PCL:SV was developed to assess psychopathy, there is some evidence suggesting that individuals who score high on the PCL do poorly in therapeutic community treatment, show less motivation, and are discharged earlier from treatment (Rice, Harris, & Cormier, 1992). In the context of diversion, these outcomes could translate to noncompliance with the conditions of release and subsequent reincarceration. In addition, individuals with psychopathic traits are more likely to recidivate, particularly engaging in new violent offenses (Salekin et al., 1996), an important outcome in diversion programs.
The HCR-20 was thought to be a suitable risk assessment tool in the context of diversion because of the unique contribution of clinical factors that are correlated not only with violence and recidivism but also with treatment response. Particularly, characteristics such as lack of insight, impulsivity, and prior treatment failure (evaluated by the C scale) have been identified as important dynamic variables in making predictions of treatment success (Morey, 1996). In addition, violence is also a perilous outcome in diversion as it may carry significant consequences for the offender, the public, and the court.
The aim of this study was to examine the utility of the HCR-20 and PCL:SV in predicting key outcomes in a sample of defendants released from jail to participate in court-mandated treatment through diversion programs in New York City. Both the HCR-20 and the PCL have been validated in forensic, civil, and correctional samples, yet the predictive utility of these instruments in the context of court-mandated treatment through diversion has not been examined.
A challenge when designing this investigation was to define the outcome variables of interest. In fact, one of the main shortcomings of the research to date is that studies evaluating the effectiveness of diversion programs use different criteria for evaluating program effectiveness. The most common outcome indicators of program success used by the existing studies include reductions in rearrest rates, jail time, and hospitalizations (Hoff et al., 1999; Lamb Weinberger, & Reston-Parham, 1996; Steadman, Cocozza, et al., 1999; Weisman, Lamberti, & Price, 2004). Other outcome measures have included treatment retention, public safety, access to housing, use of behavioral health services, development of independent living skills, reduction of drug difficulties, and improvement in quality of life (Boothroyd, Mercado, & Poythress, 2005; Broner, Lattimore, Cowell, & Schlenger, 2004; Steadman, Cocozza, et al., 1999). Number of rehospitalizations has been used by some studies as a poor outcome indicator (Lamb et al., 1996), whereas others have viewed it as a sign of program effectiveness (Steadman, Cocozza, et al., 1999).
Because the main goal of diversion is to alleviate the overrepresentation of individuals with mental illness from the criminal justice system, reincarceration was considered a key outcome for the purpose of this study. Defendants receiving treatment in the community under court supervision can be reincarcerated for two reasons: engaging in a severe violation of the conditions of the diversion programs or being rearrested on a new charge. However, different judges, district attorneys, and diversion programs vary in what they consider to be a severe violation of the conditions that warrant reincarceration as well as in the number of opportunities offered to defendants before jail is used as a sanction. Therefore, the definition of successful completion can be inconsistent across diversion programs. As a result, this study operationalized the diversion noncompliance variable based on the authors’ observation, after years of clinical practice in diversion programs, of what most courts tend to consider a violation of the conditions of the plea, even if for some courts this does not result in a remand to jail. In the present study, diversion noncompliance broadly encompasses treatment nonadherence, noncompliance with case management supervision, drug and alcohol relapses, and violent behavior (see the method section for a fuller description of operationalization).
Criterion measures for this study included reincarceration and diversion noncompliance. The utility of the HCR-20 and PCL:SV in predicting these outcome variables was tested using logistic regression analyses (LRA) and receiver operating characteristic (ROC) curves for the instruments’ total scores and subscales. It was hypothesized that individuals who earned higher scores on the HCR-20 and PCL:SV would be significantly more likely to be noncompliant and reincarcerated relative to individuals who earned lower scores.
Because of the limited financial resources usually available in diversion programs and mental health courts, the use of multiple risk assessment instruments is usually not feasible. Therefore, the selection of the most appropriate risk assessment instrument in the context of diversion is a desirable goal. In particular, the scoring of the HCR-20 currently requires the use of the PCL-R or PCL:SV, which demands more resources and time (Cooke, 2010). Some studies have demonstrated that the HCR-20 without the psychopathy item adds incremental validity to the PCL-R in predicting violence and antisocial behavior (Guy, Douglas, & Henry, 2010). As a result, this study also explored whether the HCR-20 added any incremental validity to the PCL:SV, even if H7 (the psychopathy item) is removed. Incremental validity of the HCR-20 minus Item 7 (HCR-20-7) was evaluated using sequential LRAs.
Items included in the C scale of the HCR-20, such as lack of insight, negative attitudes, active symptoms of major mental illness, impulsivity, and unresponsiveness to treatment, appear to be important not only for the prediction of violence and recidivism but also for the prediction of treatment adherence, which is a main component of diversion compliance. Another contribution of the HCR-20 over the PCL is that of the R scale. In the context of diversion, defendants are released to the community with specific treatment plans and levels of supervision. Levels of personal support, exposure to destabilizers, and feasibility of treatment postrelease (all items included in the R scale) are well known to clinicians prior to diversion. Because of the important contribution of the C and R scales of the HCR-20, it was hypothesized that in the context of criminal justice diversion, the HCR-20-7 would add incremental validity to the PCL:SV, specifically in predicting diversion noncompliance.
Method
Participants
The sample for this study consisted of 131 criminal defendants arrested for misdemeanor or felony charges who chose a mental health diversion option as opposed to incarceration. This study was part of a larger study for which 71 participants were administered a battery of tests that included the HCR-20 and PCL:SV. To increase the sample size for this study, 60 additional files were randomly selected and the HCR-20 and PCL:SV were scored via file review only. All participants were recruited from three mental health courts and three diversion programs in New York City: the Brooklyn Mental Health Court, the Brooklyn Forensic LINK Program of the Education and Assistance Corporation (EAC), EAC-Bronx Treatment Alternative to Safer Communities (TASC) and Mental Health Court, and EAC-Queens TASC (this program also diverts defendants from the Queens Mental Health Court). These programs are nonprofit agencies that offer an alternative to incarceration for mentally ill offenders coming out of the Brooklyn, Staten Island, Queens, and Bronx court systems. Defendants are provided with court advocacy, linkage from incarceration to the community, design of an individualized treatment plan by professional mental health program staff, and intensive transitional case management for a period of 1 to 2 years. Every individual incarcerated in Rikers Island (New York City’s jail) who receives mental health services and has an open court case is considered for referral to these programs.
For defendants to be eligible for diversion by any of these programs, they must have an Axis I diagnosis from the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 1994). Eligible clients must agree to a guilty plea and are then released on their own recognizance to enter treatment in the community under the diversion program’s supervision. The courts are given updates on the individuals’ progress at regular intervals until they have completed their treatment, at which time they are sentenced to a reduced charge. For example, felony charges are generally dropped to a misdemeanor with probation. Misdemeanor charges are dropped to minor-level misdemeanors or are dismissed. If, however, a client fails to complete treatment or violates the terms of his or her plea in another manner, he or she is sentenced to serve a prearranged prison term. The diversion programs included in the current study accept defendants charged with misdemeanor and felony charges. Although most of the defendants have been charged with nonviolent crimes, those charged with violent crimes are not excluded if treatment is offered.
Approximately 90 defendants who were identified as eligible for any of the aforementioned programs and who agreed to participate in the diversion alternative were referred for participation in this study. However, 14 defendants were not included because no research assistants were available to conduct interviews within the 3-week window, defendants did not complete the interviews, or they refused to participate. In addition, 60 files were randomly selected from Brooklyn Forensic LINK, Queens TASC, and Bronx TASC and Mental Health Court (20 from each program). This resulted in a sample composed of 63 (48.1%) of defendants from the Brooklyn Forensic LINK Program, 33 (25.2%) from the Bronx TASC and Mental Health Court, 26 (19.8%) from the Queens TASC, and 9 (6.9%) from the Brooklyn Mental Health Court. All of these programs generally enroll from 100 to 200 participants in a 1-year period. As a result, a sample size of 131 is considered to be representative of diversion programs in New York City.
Participants in this sample had a mean age of 37.32 years (SD = 10.63, range = 18–59). The sample consisted of 90 (68.7%) males and 41 (31.3%) females. Most participants were African American (47.3%) or Hispanic (30.5%), with others being Caucasian (14.5%) or listing their ethnicity as Other (7.6%). The mean years of education in this sample was 10.63 (SD = 2.99, range = 0–18). In terms of clinical variables, 93.1% reported a history of mental health treatment and 92.4% reported a history of substance abuse; 29.8% of participants were diagnosed with major depressive disorder, 26.0% with bipolar disorder, 19.1% with schizophrenia, 8.4% with an anxiety-related disorder, 8.0% with delusional disorder, 6.1% with schizoaffective disorder, and 2.5% with other diagnoses.
Of the participants, 82.0% had been arrested at least once prior to the index offense (M = 11.47, SD = 17.3). In all, 99 (75.6%) participants were charged with a felony and 32 (24.4%) with a misdemeanor as the index offense. Most of the participants were charged with drug-related offenses. For example, 52.7% were charged with criminal sale or criminal possession of a controlled substance, 15.5% with robbery, 12.2% with assault, 6.1% with petit larceny, 4.6% with burglary, 4.6% with criminal contempt, and 4.3% with other types of offenses.
Measures
HCR-20 Violence Risk Assessment Scheme
The HCR-20 (Webster et al., 1997) is an SPJ instrument designed to assess the risk of future violence in adult offenders with a violent history and/or a major mental disorder or personality disorder. The HCR-20 consists of 20 historical, clinical, and risk management variables that its authors determined had support in the research literature as indicators of violence risk. The HCR-20 has been validated in clinical and forensic settings in different countries. The Pearson correlation between two raters in a sample of 72 federal inmates was found to be +.80. In addition, the H scale of the HCR-20 has been found to have a correlation of +.52 with number of previous violent charges (Douglas, Webster, Eaves, Wintrup & Hart, 1996). The validity of the HCR-20 has been assessed by correlating it with scores from the PCL-R (Hare, 1991) and the Violence Risk Appraisal Guide (VRAG; Rice & Harris, 1995). The correlation between the total HCR-20 score and the PCL-R was found to be +.64, and it was +.54 with the VRAG. The correlation between the H scale and the PCL-R was found to be +.61, and that with the VRAG was +.54. Results of other studies indicate that the HCR-20 has good interrater reliability and predictive validity (de Vogel & Ruiter, 2006; see Douglas, Guy, et al., 2005, for a review of studies on the HCR-20).
Hare PCL:SV
The PCL:SV (Hart et al., 1995) is a 12-item scale based on a subset of PCL-R items that can be completed in civic and forensic settings in less than 1.5 hr (Hart et al., 1995). The PCL:SV was developed as a “relatively quick and inexpensive way of assessing psychopathic traits in offender and forensic patients” (Hart et al., 1995, p. 1). The PCL:SV approaches the construct of psychopathy equivalently to its first developed counterpart, the PCL-R (Guy & Douglas, 2006). Both instruments divide psychopathy into two components: an affective–interpersonal component and a socially deviant–impulsive lifestyle component. These two components are termed Part 1 and Part 2 in the PCL:SV. Validation studies reveal that there is a high correspondence between the two instruments, with rs of .80, .68, and .81 between Total, Part 1, and Part 2 scores, respectively, across five samples (Hart et al., 1995, as cited in Guy & Douglas, 2006). Interrater reliabilities of the 12 items of the PCL:SV were calculated on seven different samples, and the weighted mean reliabilities ranged from .50 to .79. Cronbach’s alphas were calculated across 11 samples, averaging about .84 (Hart et al., 1995). Other studies have also shown the PCL:SV to have adequate validity and reliability (Cooke, Michie, Hart, & Hare, 1999; Hart, Hare, & Forth, 1994; Salekin et al., 1996).
Interrater Reliability
Interrater reliability of the HCR-20 and PCL:SV was examined on a subsample of approximately 40% of participants (n = 48). These cases were chosen randomly from the larger data set. A measure of chance-corrected agreement intraclass correlation coefficient (ICC) was used as the index of reliability because it corrects for additive and multiplicative biases, whereas measures of association such as Pearson’s r do not (Douglas, Yeomans, & Boer, 2005). A two-way random effect variance model using the absolute agreement definition type (McGraw & Wong, 1996) was used. The reliability of a single rater or the single measure, ICC1, was considered the primary index of reliability. Generally, values of ICC greater than .75 are considered excellent, values between .74 and .60 are considered good, and values between .59 and .40 are considered fair (Cicchetti & Sparrow, 1981). Item-level interrater reliability was calculated for each measure. For the HCR-20, the reliability of a single rater (ICC1) was .90. Item 6 (major mental illness) had the lowest reliability (.55), and Items 2 (young age at first violent incident) and 18 (lack of personal support) had the highest reliability, both reaching a value of .89. ICCs for the H, C, and R scales were .93, .80, and .61, respectively. The mean PCL:SV item interrater reliability was .93; Item 3 (deceitful) had the lowest reliability (.59), and Item 2 (grandiose) had the highest reliability (.84). ICCs for PCL:SV Parts 1 and 2 were .84 and .88, respectively.
Operational Definition of Criterion Variables
Criterion measures were coded from charts where all recidivism data as well as any incidents of diversion noncompliance are documented by participants’ case managers. Compliance with diversion was dichotomized into one category: diversion compliance versus diversion noncompliance. Any of the following was classified as diversion noncompliance: absconding from residential treatment program, failure to attend more than 2 days of outpatient program and/or weekly meetings with case manager, more than two incidents of drug or alcohol relapse, and violent behavior. Although the choice of three as the number of missing meetings or relapse incidents is somewhat random, anecdotal observations of the ways in which diversion programs operate suggest that it is usually after three episodes when case managers tend to bring these incidents to the attention of the judge, which may result in a violation of the conditions of release.
Violence was included within diversion noncompliance because acts of violence are usually considered a violation of the plea agreement. Violence was defined consistently with the operational definitions used by McNiel and Binder (1987, 1994) and the description of violence provided by the HCR-20’s manual (Webster et al., 1997). Threatening behavior was defined as “clear and unambiguous threats of harm” (Webster et al., 1997, p. 24) and behavior likely to cause intimidation or fear, such as stalking. Physical violence was defined as bodily acts of aggression against others such as pushing or punching and “behavior which obviously is likely to cause harm to another person” (Webster et al., 1997, p. 24). Reincarceration was classified as any criminal activity after diversion leading to a new charge and incarceration, or any violation of the conditions of the plea agreement that led to issuance of a bench warrant or a remand to jail.
Procedure
Data for this study were collected from October 2006 to February 2010. Participants who were interviewed were informed of the nature of the study as well as the risks and benefits associated with participation. All participants provided written consent for participation and were screened via an interview conducted in the diversion program or mental health courts offices or in the residential treatment programs where individuals receive treatment services. Participants were interviewed within 3 weeks of their release from jail or the date of their guilty plea. The 3-week window was chosen based on the time that it usually takes for defendants to start receiving full services. The first 2 weeks after release are usually spent meeting with case managers and attending several appointments (e.g., medical and social security appointments). Semistructured interviews took from 1 hr to 2 hr and included the administration of the HCR-20 and PCL:SV, among other measures that were part of a larger study. In addition, researchers had access to file-based collateral information containing initial intake interviews conducted by the diversion program, background psychiatric and mental health reports, psychosocial summaries, and complete criminal records. Demographic data were also collected from files.
The files of 60 additional individuals who were currently participating in or had recently completed diversion were randomly selected and reviewed for the scoring of the instruments. The scoring of the HCR-20 and PCL:SV for these additional 60 participants was based on file review only, as these participants were not interviewed. Information available in the files included participants’ psychosocial histories, intake evaluation, psychiatric evaluations, and information from other institutions (e.g., Rikers Island’s records, hospital records). For all participants, researchers were also able to ask questions of the case managers assigned to the cases if considered necessary for the scoring of any of the items. Prior studies have demonstrated that file data provide a reliable means of collecting HCR-20 (Douglas et al., 1999) and PCL (Grann, Langstrom, Tengstrom, & Stalenheim, 1998) ratings for research purposes.
All interviews and file reviews were conducted by John Jay College of Criminal Justice doctoral and master’s students, who were trained in the administration of all the instruments. Two master’s students conducted 20 interviews together before scoring the instruments independently. Other students conducted at least 10 interviews with another student before scoring the instruments independently. Regular meetings were held to discuss cases and scoring.
Outcome data were cumulatively recorded at 3, 6, and 12 months from diversion placement. An individual was considered to be noncompliant at 12 months if he or she had been noncompliant at 3 or 6 months. Outcomes were recorded through a review of the files that contained the case manager’s progress notes, treatment update letters from treatment providers, weekly toxicology exam results, monthly progress letters for the courts, and legal documents including violation or bench warrant order forms. Researchers collecting outcome data were blind to the scores on the predictors.
Institutional review board (IRB) approval was obtained by the review committee of John Jay College of Criminal Justice. In addition, to recruit participants from the Brooklyn Mental Health Court, IRB approval was obtained by the review committee of the Center for Court Innovation, which oversees research in the Brooklyn Mental Health Court.
Results
Classification Criteria
Using the aforesaid criteria, 43 (32.8%) participants were classified as noncompliant at 3 months, 55 (42.0%) at 6 months, and 62 (47.3%) at 12 months. Regarding reincarcerations, 27 (20.6%) were reincarcerated or out on a warrant at 3 months, 41 (31.3%) at 6 months, and 51 (38.9%) at 12 months.
Data Checks
A series of LRAs was conducted to check for possible differences between the group of participants who were interviewed (n = 71) and the group of participants who were not interviewed (n = 60) using the two outcome variables (noncompliance and reincarceration) cumulatively recorded at 12 months as predictor variables. No significant differences were found, χ2(2, 131) = 1.44, p > .05. The two groups were also found to be homogeneous in terms of demographic variables. However, inspection of the predictor variables revealed that the groups differed significantly on PCL:SV Part 1 score (B = 0.414, SE = 0.120, Wald χ2 = 11.22, p < .05; odds ratio = 1.51, 95% CI = 1.18–1.92). The mean score for the interviewed group was 2.92 (SD = 2.52) versus a mean of 1.63 (SD = 1.97) for the noninterviewed group. An inspection of the six items of the PCL:SV Part 1 scale revealed significant differences only on Item 4 (lacks remorse) and Item 6 (doesn’t accept responsibility). Although researchers had access to thorough files that included psychosocial and psychological evaluations, these two personality characteristics might be more difficult to assess without interviewing the defendants, which may explain the significant differences between the two groups on these items.
Descriptive Statistics
Table 1 lists descriptive statistics and t tests for the predictor variables. The mean for the HCR-20 was generally consistent with that found in other samples of mentally ill offenders (Grey et al., 2004; Grey, Taylor, & Snowden, 2008). However, the mean score for the PCL:SV was below values generally found in forensic psychiatric populations where scores tend to range between 12.97 and 16.56 (Hart et al., 1995). Specifically, the mean score for Part 1, which encompasses the affective–interpersonal features, was particularly low when compared to other forensic psychiatric samples (Hart et al., 1995), whereas Part 2, which encompasses the behavioral features, was closer to values found in other studies. In addition, t tests revealed that participants in the diversion noncompliance and reincarceration groups earned significantly higher scores on all measures and subscales.
Mean, Standard Deviations, and t Tests for HCR-20 and PCL:SV Scores on Diversion Noncompliance and Reincarceration Status

Note. DC = diversion compliance; DNC = diversion noncompliance; NR = non-reincarceration; R = reincarceration; T = Total score; H = Historical; C = Clinical; R = Risk Management; d = Cohen’s d; CI = confidence interval. All t tests had 129 degrees of freedom
Correlational Analyses
Table 2 lists intercorrelations for the predictor variables. Most of the intercorrelations were high because the instruments contain similar risk factors. However, none of the correlations between the two instruments were greater than .80. As expected, the H scale of the HCR-20 correlated stronger with Part 2 of the PCL:SV than with Part 1.
Correlations Among the Scores on the HCR-20 and PCL:SV
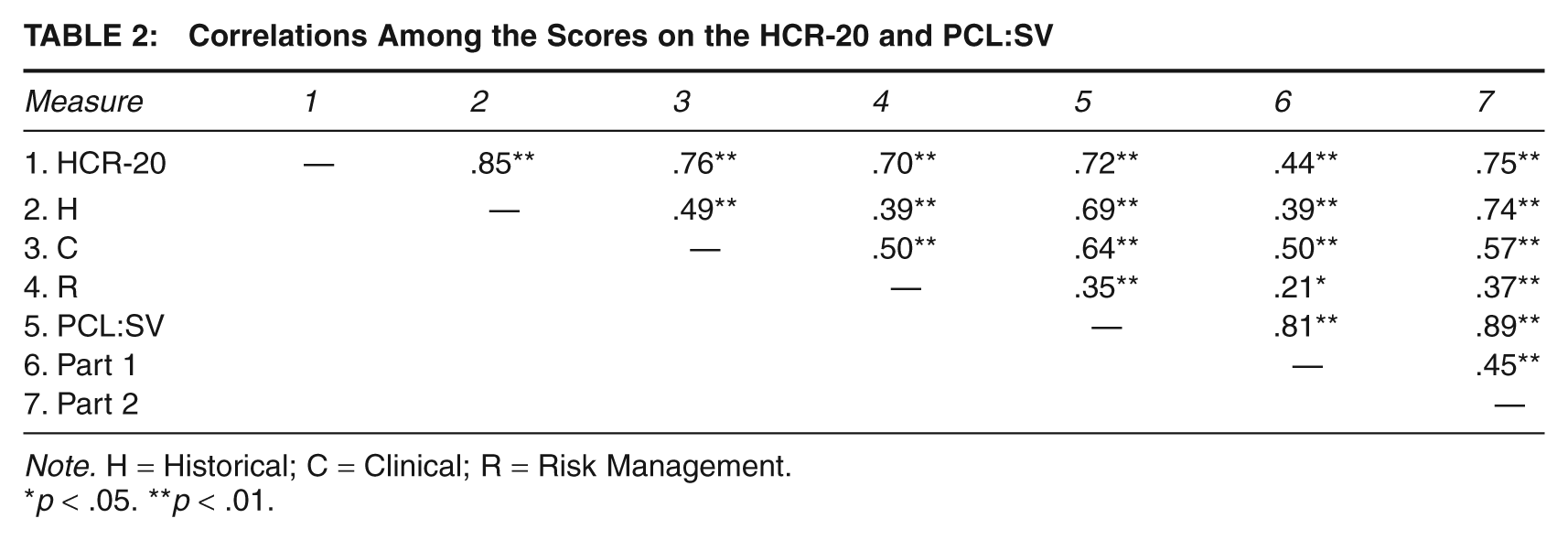
Note. H = Historical; C = Clinical; R = Risk Management.
p < .05. **p < .01.
Predictive Validity
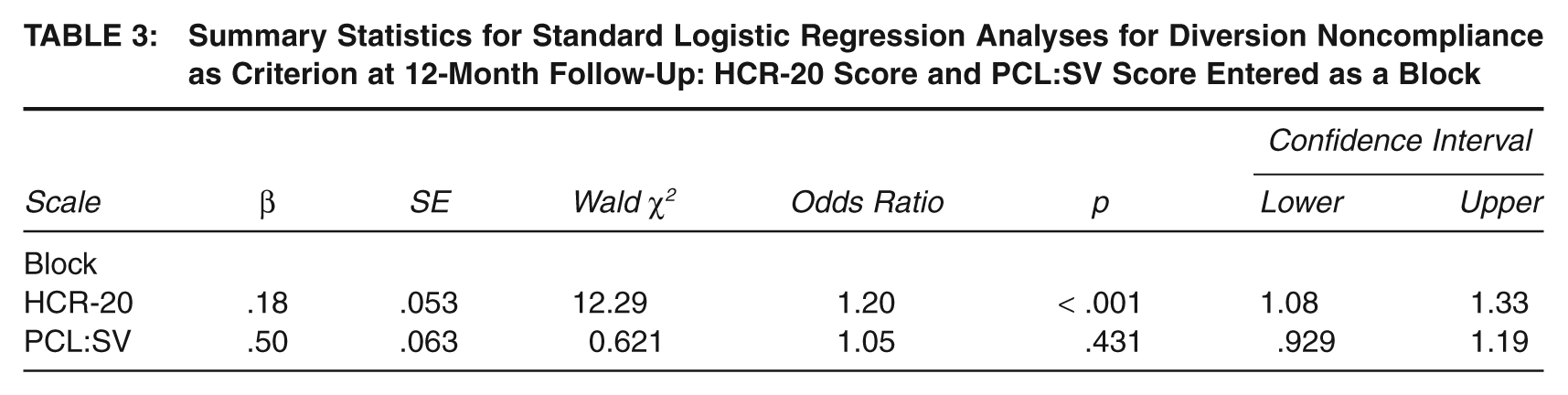
To determine if the diversion noncompliance group could be classified by the HCR-20 and PCL:SV, an LRA was conducted with cumulative diversion noncompliance as the criterion and the total scores of the HCR-20 and PCL:SV as predictors. The model was significant, χ2(2, 131) = 36.04, p < .001, indicating that both the HCR-20 and the PCL:SV as a group distinguished individuals who complied with diversion from those who did not comply. However, inspection of individual predictors revealed that only the HCR-20 significantly predicted the outcome when the other indices were controlled. The same results were found at 3- and 6-month follow-up periods. Table 3 shows regression coefficients, Wald statistics, odds ratios, and confidence intervals for both scales together at the 12-month follow-up period.
Summary Statistics for Standard Logistic Regression Analyses for Diversion Noncompliance as Criterion at 12-Month Follow-Up: HCR-20 Score and PCL:SV Score Entered as a Block
The same analyses were conducted for reincarceration as a criterion. The model was significant, χ2(2, 131) = 18.06, p < .001, indicating that both the HCR-20 and the PCL:SV subscales as a group distinguished individuals who were reincarcerated from those who were not. However, examination of individual predictors revealed that no individual scale significantly predicted the outcome when contributions of the remaining indices were controlled for.
To examine what subscales of the HCR-20 showed better predictive validity, an LRA was conducted with the three subscales of the HCR-20 entered as a block and diversion noncompliance as criterion. The R scale was the only significant predictor at 6 and 12 months, B = 0.360, SE = 0.135, Wald χ2(1, N = 131) = 7.15, p = .007; odds ratio = 1.433, 95% CI = 1.101–1.866, whereas both the C and R scales showed significance at the 3-month follow-up period. When reincarceration was used as a criterion at 12 months, the H scale was the only significant predictor, B = 0.166, SE = 0.065, Wald χ2(1, N = 131) = 6.49, p = .011; odds ratio = 1.180, 95% CI = 1.039–1.340. The H scale also performed better than the C and R scales at 3- and 6-month follow-ups.
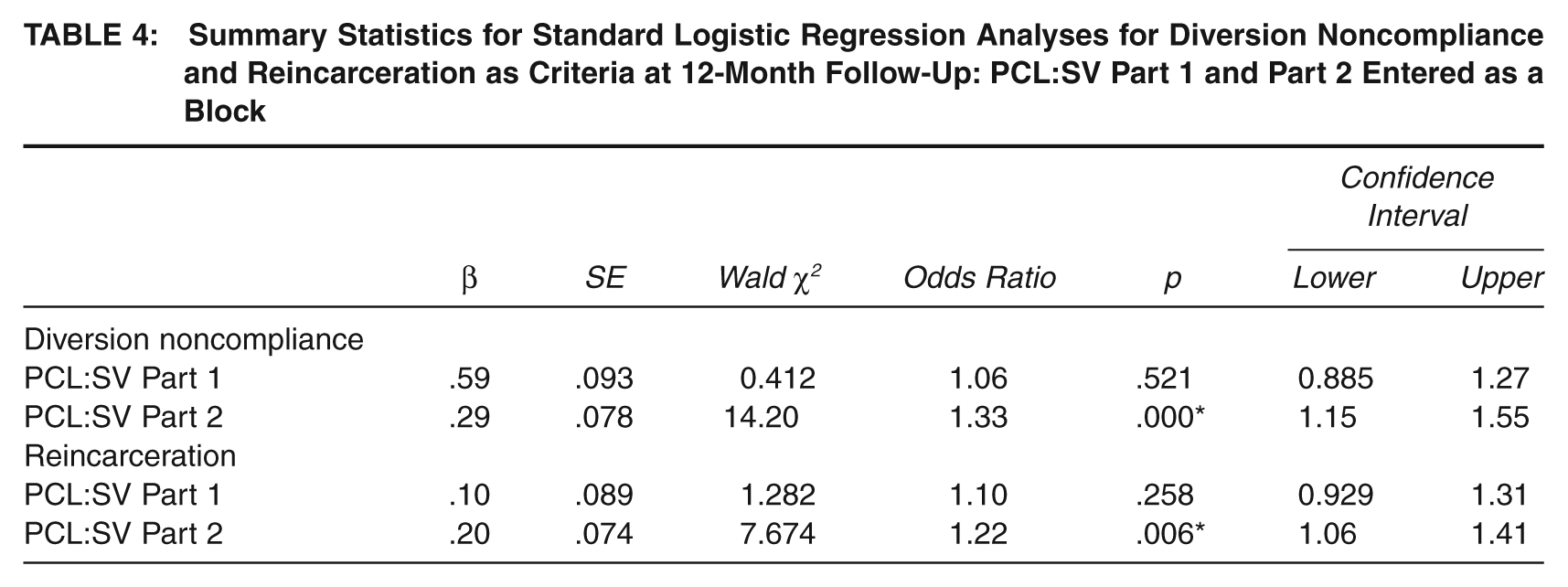
When both Part 1 and Part 2 of the PCL:SV were entered as a block in an LRA, Part 2 was the only one to show significance for both diversion noncompliance and reincarceration as criteria. Table 4 shows regression coefficients, Wald statistics, odds ratios, and confidence intervals for both subscales of the PCL:SV together at the 12-month follow-up period with diversion compliance and reincarceration as criterion variables.
Summary Statistics for Standard Logistic Regression Analyses for Diversion Noncompliance and Reincarceration as Criteria at 12-Month Follow-Up: PCL:SV Part 1 and Part 2 Entered as a Block
LRAs were also conducted to explore whether the HCR-20 and PCL:SV predicted violence or recidivism (new charge) at 12 months. However, no significant results were found. The low base rate for violence (9.9%) and recidivism (19.1%) likely contributed to these nonsignificant results. Finally, hierarchical LRAs were conducted to test whether the administration method (interview plus file review vs. file review only) moderated the predictive validity of the HCR-20 or the PCL:SV at the 12-month follow-up. The interaction term was not found to be significant for any of the criterion variables, showing no moderation effect of administration procedure.
Receiving Operating Characteristic Analyses
ROC curves for the predictors were generated. The area under the curve (AUC) refers to the probability that a randomly selected individual from the noncompliance or recidivism group will have scored higher on the predictor variables than a randomly selected individual from the compliance or nonrecidivism groups. The AUC ranges from .0, perfect negative prediction, to 1.0, perfect positive prediction. The HCR-20 showed the largest AUC for both diversion noncompliance and reincarceration. Consistent with the regression analyses, the H scale of the HCR-20 performed better when predicting reincarcerations, whereas the R scale performed better when predicting diversion noncompliance. Part 2 of the PCL:SV obtained larger AUCs than Part 1 with both predictors. Table 5 lists the values for the AUCs for all predictors and criteria.
Areas Under the Curves (AUCs) of Receiver Operating Characteristic Analyses for Diversion Noncompliance and Reincarceration at 12-Month Follow-Up
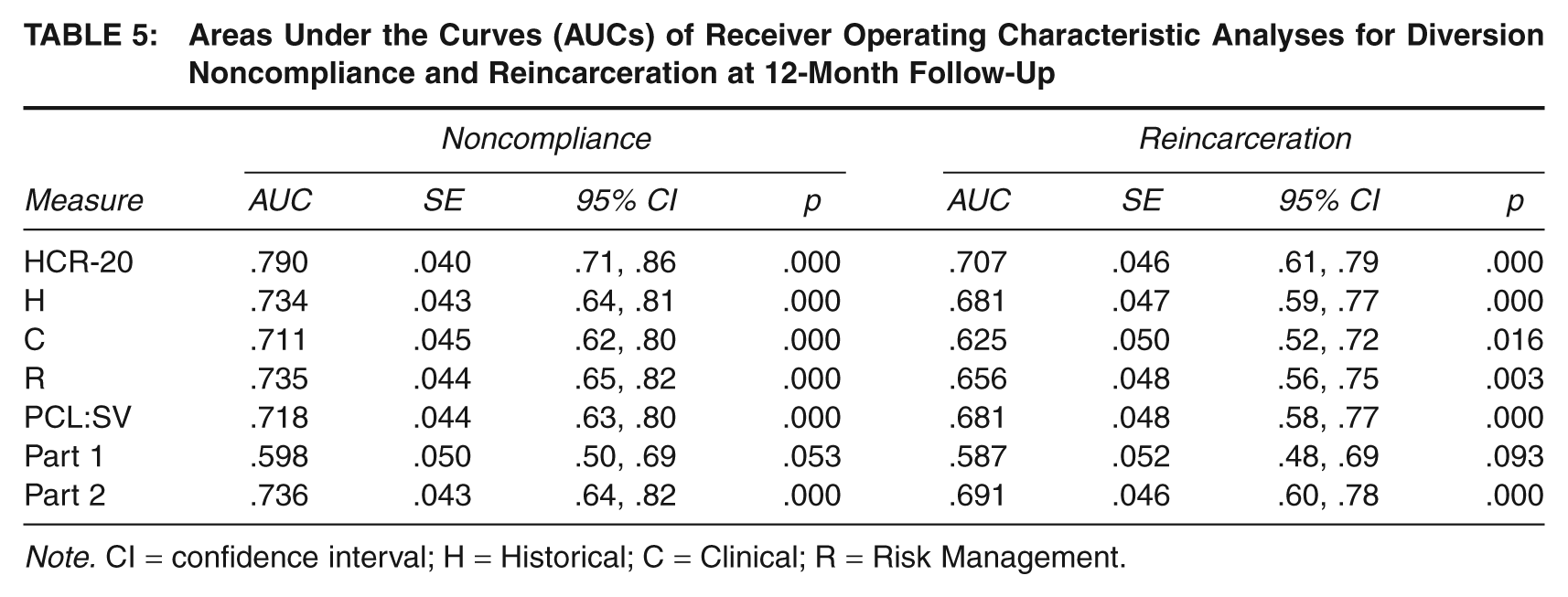
Note. CI = confidence interval; H = Historical; C = Clinical; R = Risk Management.
Incremental Validity
To determine if the results would remain the same for the HCR-20 with the psychopathy item removed, a sequential LRA with diversion noncompliance as the criterion variable was conducted with the PCL:SV total score entered first, followed by the HCR-20-7. The PCL:SV significantly differentiated the groups, Wald χ2(1, N = 131) = 17.37, p < .001. Comparison of log likelihood ratios of models with and without the addition of HCR-20-7 showed significant improvement when HCR-20-7 was added to the equation, Δχ2(1, N = 131) = 13.68, p < .001, with HCR-20-7 being the only variable that contributed significantly to the prediction, HCR-20-7 Wald χ2(1, N = 131) = 11.87, p = .001; PCL:SV Wald χ2(1, N = 131) = 1.18, p > .05. When the order was reversed, the PCL:SV failed to contribute significantly to the predictive power of the HCR-20 alone.
Discussion
Diversion programs and mental health courts are growing in number, and increasing numbers of defendants, including felony and violent offenders, are being released from jails to enter community-based treatment. The relocation of these felony and violent offenders from jail into the community amplifies the importance of using risk assessment instruments as part of diversion evaluations to assist the courts’ eligibility decisions and minimize the risk of reincarceration. This study was designed to investigate the utility of the HCR-20 and PCL:SV in predicting reincarceration and diversion noncompliance in a sample of defendants released from jail to participate in diversion in New York City.
Descriptive statistics for the risk assessment instruments showed a mean HCR-20 score that is generally consistent with other samples of mentally ill offenders. However, participants of this study earned lower scores on the PCL:SV, particularly on Part 1, when compared to other forensic samples. These results suggest that this sample may consist of what has been described as antisocial offenders (high scores on Factor 2 and low scores on Factor 1; Patrick, 1994), as opposed to psychopathic offenders (high scores on Factor 1 and low scores on Factor 2). In fact, only five participants (3.8%) exceeded the cutoff score of 17 recommended by Hart et al. (1995) for strong evidence of psychopathy on the PCL:SV. The low base rate of psychopathy in this sample may be an artifact of the diversion programs’ selection criteria. Even though second-generation diversion programs are more likely to divert more felony than misdemeanor offenders (Redlich et al., 2005), most of the participants deemed eligible for diversion were charged with nonviolent offenses. In the current sample, 72.5% of participants were charged with nonviolent offenses versus 27.5% of participants charged with violent offenses. Research has found that high scores on the PCL are strong predictors of violent recidivism (Porter et al., 2001; Salekin et al., 1996; Walters, 2003a).
The finding that administration procedure (interview plus file review vs. file review only) did not moderate the predictive validity of the HCR-20 or PCL:SV is of practical significance to diversion programs with limited time and resources for additional evaluations. If diversion staff are provided with comprehensive records and trained in the scoring of these measures, our results suggest that additional interviews may not be necessary. It should, however, be noted, that the 60 participants who were not interviewed received significantly lower scores on Part 1 because some personality characteristics (such as acceptance of responsibility and remorse) may be more difficult to assess without meeting the defendants. This significant difference on the affective–interpersonal component of the PCL:SV between interviewed and noninterviewed participants may have also contributed to the lower base rate of psychopathy in this study compared to other forensic samples.
Results of a series of logistic regression and ROC analyses provided preliminary support for the use of the HCR-20 and PCL:SV in the context of diversion evaluations. The HCR-20 was found to be superior to the PCL:SV in the prediction of both diversion noncompliance and reincarceration. It is important to note that because of the generally low scores on Part 1 of the PCL:SV, PCL:SV total scores were restricted in range, which may have contributed to the superiority of the HCR-20 over the PCL:SV in this sample. In fact, Part 2 of the PCL:SV was the only significant predictor when compared to Part 1 for both diversion noncompliance and reincarcerations.
However, the low scores found on the PCL:SV were not totally unexpected. In fact, the HCR-20 had been hypothesized to be more useful in the context of diversion because of the inclusion of clinical (dynamic) variables in addition to antisocial historical (static) variables. Because of the nature of this population as primarily mentally ill, more variability was expected to be found on instruments that include clinical factors. In addition, the low base rate of psychopathy found in this sample is consistent with the low comorbidity between psychopathy and Axis I diagnoses reported by prior research (Hare, 2003; Hidebrand & de Ruiter, 2004; Stalenheim & Knorring, 1996). This study’s findings are consistent with the results of a recent meta-analytic study (Guy et al., 2010) that found that HCR-20 outperformed the PCL:SV in predicting antisocial behavior and violence. Nevertheless, replications of this study are needed to see if consistent base rates of psychopathy are obtained across diversion populations.
Sequential LRA showed that the HCR-20 added incremental validity to the PCL:SV when predicting diversion noncompliance, even when the psychopathy item was subtracted from the total score. Conversely, the PCL:SV failed to contribute significantly to the predictive power of the HCR-20. Examination of the subscales indicated that when predicting diversion noncompliance, the R scale proved to be the most useful, especially at 6- and 12-month follow-up periods. This result suggests that the consideration of the discharge and treatment plans and conditions of supervision on discharge play an important role in the risk assessment and management of compliance in the context of diversion. It is not surprising that the C scale was most useful in predicting noncompliance at 3 months. Some of the variables included in the C scale are theoretically related to treatment response, such as insight, impulsivity, and prior treatment failure. Furthermore, Item 3 of the clinical scale (active symptoms of major mental illness) is particularly significant given the short follow-up period. This is a positive finding considering that dynamic factors are changeable whereas static factors are not. Therefore, reducing severity of symptoms, improving insight, and fostering more positive attitudes may in fact improve the prognosis in terms of diversion compliance. As a result, identification and quick intervention of dynamic risk factors can likely decrease the incidents of noncompliance in the short term.
Participants in this study were quite homogeneous on historical factors given the high prevalence of substance abuse, mental illness, early victimization, and type of offenses (mostly nonviolent felonies). This characteristic of the sample, paired with the fact that the criterion variable was diversion noncompliance and not violence alone, may explain the superiority of the R and C scales over the H scale in predicting compliance. However, when the criterion variable was reincarceration, the H scale outperformed the C and R scales at the three follow-up periods. This result is consistent with the importance of historical factors, such as prior history of violence or prior supervision failure, in the prediction of future offending and severe violations of supervision.
Results of this study suggest that risk assessment instruments can be useful in the context of diversion programs to assess the risk of reincarceration and noncompliance and to adjust different levels of supervision or intensity of treatment according to the needs of the defendants. The HCR-20 was developed to help clinicians identify the factors that need to be considered when making predictions of risk. A final determination of low, moderate, or high risk is encouraged as opposed to using prescribed cutoff scores. Consistent with accepted practice in scoring the HCR-20, within the context of diversion, the authors of this study recommend that HCR-20 scores not be the sole basis for determining eligibility for diversion. Hence, cutoffs scores are not suggested in this study. Instead, the HCR-20 should be used to guide clinicians in considering important risk factors when making decisions about diversion. Because clinical factors have been shown to be more useful in predicting compliance in the short term, the HCR-20 could also be used as a way to guide treatment by pointing out areas that need to be addressed to improve prognoses about diversion.
Further research should be conducted with larger samples and longer follow-up periods. Following defendants for longer periods of time may result in increased incidents of violence and recidivism, allowing for further examination of the enduring accuracy of the HCR-20 and PCL:SV in predicting these two variables in the context of diversion. In addition, this study did not examine the predictive validity of the structured final risk judgments of the HCR-20, which have been found by prior research to be superior to the HCR-20 used actuarially (Pedersen, Rasmussen, & Elsass, 2010). Future studies should evaluate the validity of final risk judgments of the HCR-20 in the context of criminal justice diversion.
Footnotes
This article is part of a special issue titled “Diversion from Standard Prosecution”, edited by Kirk Heilbrun and David DeMatteo of Drexel University. Part of the data collection for this study was conducted for the first author’s dissertation while a doctoral student at the City University of New York’s doctoral program in psychology offered by John Jay College of Criminal Justice in conjunction with the CUNY Graduate Center. Preliminary findings from this research were presented at the Annual Meeting of the American Psychology-Law Society, in Vancouver, Canada, in March 2010. The authors would like to thank Michele Galietta and Keith Markus from John Jay College of Criminal Justice for their consultation and invaluable feedback as members of the first author’s dissertation committee. We also wish to thank the Brooklyn Mental Health Court, the Center for Court Innovation, and EAC-TASC Mental Health Diversion Programs. Particularly, we thank Judge D’Emic, Carol Fisler, Lucille Jackson, Ruth O’Sullivan, Lauren D’Isselt, Tania Chandler, and Merrill Rotter for allowing us complete access to their programs to collect data for this project. Finally, we are grateful to Charles Amrhein from EAC-Bronx TASC and Mental Health Court for his unconditional support and assistance; and Danielle Cassela, Meghan Ellis, and Katherine Click for their assistance interviewing participants.