
Abstract
In this article, we present the results of a preliminary evaluation of a comprehensive treatment program specifically designed to treat co-occurring issues of mental illness and criminal risk in persons with mental illness (PMI) that are criminal justice involved. Participants include 47 incarcerated male PMI in a secure psychiatric prison or a residential treatment facility. Of the 47 participants, 31 (66%) completed the program, attended 94% of all sessions, completed 83% of assigned homework, and actively participated in treatment sessions as evidenced by participation ratings. Change was examined using a four-tiered assessment strategy, including pre–post significance testing, magnitude of effect sizes, clinical cutoffs, and reliable change indices. Results showed evidence of strong therapeutic alliance and treatment program satisfaction, as well as symptom reduction and some evidence for reduced criminal thinking. Program modifications and implications for enhancing service delivery to justice involved PMI are discussed.
Persons with mental illness (PMI) are overrepresented in the criminal justice system (Steadman, Osher, Clark-Robbins, Case, & Samuels, 2009), and continue to be incarcerated at alarming rates (Hodgins, 1995; James & Glaze, 2006; Steadman, Morris, & Dennis, 1995; Torrey, 1995). Recent estimates suggest that between 15% (Steadman et al., 2009) and 24% (James & Glaze, 2006) of incarcerated offenders suffer from a severe mental illness; though most estimates underrepresent the number of mentally ill incarcerated offenders (Steadman et al., 1995). While incarcerated, PMI experience poor institutional adjustment (e.g., Feder, 1991) and victimization (Human Rights Watch, 2003; Torrey et al., 1992), as well as increased psychiatric symptomatology (Bauer, 2012). Furthermore, PMI released from prison encounter numerous transitional difficulties (Davidson, Hoge, Merrill, Rakfeldt, & Griffeth, 1995; Draine, Wolff, Jacoby, Hartwell, & Duclos, 2005; Haimowitz, 2004; Jacoby & Kozie-Peak, 1997), and are at increased risk for psychiatric rehospitalization or criminal recidivism (Feder, 1991). Thus, targeted interventions for PMI who are criminal justice involved (referred to from here forward as “offenders with mental illness” [OMI] for simplicity’s sake) need to meet public health goals in mental health policy as well as public safety goals in criminal justice policy.
Unfortunately, minimal progress in the treatment of OMI has been made in the last 30 years (Snyder, 2007). Historically, it was assumed that providing better mental health care would reduce the number of PMI in jails and prisons; however, this assumption proved incorrect as providing better mental health care improves psychiatric outcomes, but has no appreciable effect on criminal justice outcomes (Calsyn, Yonker, Lemming, Morse, & Klinkenberg, 2005; Morrissey, Meyer, & Cuddeback, 2007). To improve criminal justice outcomes, we must provide services that address the underlying causes of criminal behavior (e.g., Hodgins et al., 2007; Morgan, Fisher, Duan, Mandracchia, & Murray, 2010). Unfortunately, OMI have limited access to comprehensive treatments that target co-occurring issues of mental illness and “criminalness” (Bewley & Morgan, 2011; Morgan, Flora, et al., 2012). It should be noted that we use the phrase criminalness here as it was developed as a useful verbal tool for helping offenders quickly and efficiently refer to their antisocial and/or offending behavior. For purposes of this intervention, we define criminalness as behavior that breaks laws and social conventions and/or violates the rights and well-being of others, and may or may not lead to arrestable offenses such as abuse of sick leave, drug possession, person, property, and violent crime (Morgan, Flora, et al., 2012). In fact, “treatment outcome research on mentally ill offenders specifically is almost nonexistent” (Rice & Harris, 1997, p. 164), and
are as scarce now as they were 30 years ago . . . Too few programs are being developed and too few promising programs are being tested with the rigor that would yield the proof needed to label them as evidence based. (Snyder, 2007, p. 6)
The lack of effective interventions for OMI is a public health concern. Severe psychiatric disorders occur up to 4 times more frequently in incarcerated populations (Hodgins, 1995), as PMI are at increased risk of being arrested and incarcerated when compared with nonmentally ill individuals (Munetz, Grande, & Chambers, 2001; Teplin, 1984, 1990). Furthermore, with 3 times more PMI in criminal justice facilities than state hospitals (Abramsky & Fellner, 2003), the criminal justice system has become a primary public health service setting for individuals with mental disorders (Fagan & Ax, 2003; Holton, 2003). This has resulted in incongruence between the public safety mandate of the criminal justice system, which was not designed for the treatment and management of PMI, with the treatment and management needs of PMI. Furthermore, few resources are targeted toward the specific psychiatric, behavioral, and rehabilitative needs of OMI (Boothby & Clements, 2000) in spite of evidence that minimal discrepancy exists between psychiatric symptoms presented by PMI in the criminal justice system and PMI in mental health settings such as psychiatric hospitals (Morgan et al., 2010; Quinsey, Harris, Rice, & Cormier, 2006; Wolff, Morgan, Shi, Huening, & Fisher, 2011).
Although little is known about effective therapeutic strategies for OMI, it is often postulated that strategies that have proven beneficial for treating criminality in general population offenders may also prove beneficial with OMI whose criminal behavior has similar etiology (Morgan, Flora, et al., 2012); however, this is yet to be empirically investigated. Furthermore, it is impractical to suggest that merely applying correctional strategies that work for offenders without mental illness to OMI will result in similar treatment gains as these strategies do not target issues of mental illness that may impede therapeutic progress. Thus, although we know the use of intensive (Bourgon & Armstrong, 2005; Wormith & Olver, 2002) and empathic human services that rely on a therapeutic alliance (see Andrews & Bonta, 2010; Gendreau, 1996b) improve outcomes for offenders without mental illness, we have not examined whether these same principles hold true for OMI. Similarly, using cognitive-behavioral therapeutic strategies (e.g., cognitive and modeling strategies; Gendreau, 1996a, 1996b) that are grounded in social learning theory (see, for example, Andrews & Bonta, 2010), implement structure (Leak, 1980; Morgan & Flora, 2002), and integrate out of treatment homework exercises (Morgan & Flora, 2002; Morgan, Flora, et al., 2012) have proven to be effective practices for nonmentally ill offenders, but we do not know whether these practices prove equally effective with OMI. Similarly, Illness Management and Recovery (IMR; Mueser & MacKain, 2005) is an evidence-based practice for individuals suffering from severe and persistent mental illnesses; however, it has not been demonstrated that standard treatment approaches for severe mental illness alone are effective interventions for OMI because these approaches do not typically target issues which have been shown to be related to criminal behavior, such as criminal thinking styles and attitudes (see Andrews & Bonta, 2010). Thus, mental health professionals treating offenders need to address psychiatric symptoms and criminalness (Hodgins et al., 2007; Morgan et al., 2010; Morgan, Flora, et al., 2012). Simply treating the mental illness does not reduce criminal recidivism (Bonta, Law, & Hanson, 1998); however, correctional rehabilitative efforts must not ignore the mental health issues. The goal of correctional interventions for OMI must focus on the joint goals of reducing psychiatric hospitalization days and time spent incarcerated, as well as increasing the number of functional days. As noted by Senator Patrick Kennedy (2007), evidence-based practices need to “improve the lives of young people and make sure they do not commit further crimes” (p. 26).
To meet this need, we developed Changing Lives and Changing Outcomes: A Therapeutic Program for Justice Involved Persons With Mental Illness. The strength and innovation of this program is the integration of the best evidenced-based practices in the mental health and criminal justice fields. Changing Lives and Changing Outcomes provides a framework for intervening when mental illness and criminalness co-occur in keeping with recent advances in the treatment of co-occurring disorders that recommend unified treatment protocols (Allen, McHugh, & Barlow, 2008), or a combined/interdisciplinary approach (Nathan & Gorman, 2007). This program seeks to enhance quality of life, reflected through improved psychiatric status and reduced recidivism. This preliminary evaluation examines participant treatment engagement, treatment feasibility, treatment satisfaction, and effectiveness of a therapeutic program that addressed mental illness and criminalness simultaneously. Specifically, we examined treatment compliance and pre–post measures of symptomatology and antisocial attitudes in a sample of OMI incarcerated in a psychiatric prison or serving a probated sentence and admitted to a residential treatment facility.
Method
Intervention
Changing Lives and Changing Outcomes: A Therapeutic Program for Justice Involved Persons With Mental Illness (Morgan, Kroner, Mills, & Bauer, 2012) integrates issues of criminalness and mental illness into nine therapeutic modules: Preparing for Change, Mental Illness and Criminalness Awareness, Medication Adherence, Coping With Mental Illness and Criminalness, Antisocial Thoughts and Attitudes, Emotions Management, Antisocial Associates, Skill Development (i.e., problem-solving skills, social and recreational skills, and vocational/housing skill development), and Substance Abuse.
Changing Lives and Changing Outcomes includes a comprehensive and structured treatment manual that provides clinicians a guide for treating OMI. The manual includes a treatment plan for each session with specific structured exercises (for in-group and out-of-group work) designed to teach specified objectives each session. The program incorporates a psychosocial rehabilitation model, social learning paradigm, and a cognitive-behavioral model for change with cognitive-behavioral theory being more prevalent and apparent throughout the manual. Although the manual was designed for implementation with individual offenders or in a group setting, for purposes of this evaluation the program was offered in a group format.
Participants attended three treatment sessions per week (excluding holidays, facility lockdowns, or therapist unavailability). Each session, as outlined in the manual, lasted between 1.5 and 2 hr, with the target session length equaling 1 hr, 50 min. The nine therapeutic modules were delivered in 74 sessions over 24 weeks. Treatment providers were doctoral students, and all groups were led by one treatment provider. Treatment providers were provided the treatment manual and offender workbook and educated about the treatment program during initial weekly supervision sessions; as the treatment providers were doctoral students, they received weekly supervision (approximately 1-hr sessions) with the lead author for the life of the groups. Groups were closed such that dropouts or noncompleters were not replaced (i.e., closed admission policy).
Participants
Participants consisted of 47 incarcerated male PMI in a secure psychiatric prison (n = 8; one treatment group) or a residential treatment facility (n = 39; four treatment groups). Of these, 31 1 (65.9%) met the successful completion criteria defined as the completion of all sessions of the program or completed all sessions of the program that they were eligible to complete prior to their successful discharge from the facility.
Participants had a mean age of 31 years (SD = 10.8) and were predominantly Caucasian (n = 35, 79.5%), with 7 (15.9%) participants identifying as African American, and 2 (4.5%) as Native American. Three individuals did not self-identify their race. Six participants identified their ethnicity as Hispanic, but 22 participants did not provide this information. The majority of participants were single/nonpartnered (n = 26, 55.3%) or married/partnered (n = 14; 29.7%). The remainder were divorced (n = 2, 4.3%), separated (n = 4, 8.5%), or widowed (n = 1, 2.1%). The average years of education were 11 (SD = 2.07), with approximately one half (48.9%) of the sample reporting a General Equivalency Diploma (GED). Index offenses 2 varied: drug/alcohol related crime(s) such as possession or distribution (n = 30), robbery/burglary (n = 13), assault/battery (n = 6), aggravated assault/aggravated robbery (n = 4), sex offense (n = 1), and other types of offenses (n = 18). These numbers exceed the number of participants as several participants were convicted of multiple offenses. Thirty-one (67.4%) of the participants were receiving psychotropic medications for a variety of self-reported disorders, including thought disorder, bipolar disorder, or major depressive disorder (n = 31, 65.96%), as well as other diagnoses, including anxiety disorders (n = 2, 4.3%), substance use disorder (n = 2, 4.3%), attention deficit/hyperactivity disorder (n = 1, 2.1%), and “split personality disorder” (n = 1, 2.1%). Ten participants did not report their diagnosis. There were no significant demographic differences (i.e., race, ethnicity, relationship status, GED obtainment, index offense, psychotropic medication use) between program completers and noncompleters with the exception that noncompleters were significantly younger (M = 24.3, SD = 6.1) and less educated (M = 10.1, SD = 1.7) than completers (M = 33.7, SD = 11.3 and M = 11.4, SD = 2.1, respectively, p < .05).
Procedure
Changing Lives and Changing Outcomes was provided as a clinical service at two facilities: a special needs prison that houses felony offenders and a residential treatment facility. The special needs prison is a psychiatric and medical facility with 550 beds for inmates who, due to severe psychiatric illnesses, are unable to maintain stable mental health functioning in a general correctional population. The residential treatment facility was designed to treat offenders on probation with substance abuse and alcohol dependency, and is one of only two residential treatment centers in Texas accepting offenders with dual diagnosis (mental illness and substance abuse).
Participants at the psychiatric prison were identified by the treatment team as a person in need of this intervention. A list of potential participants was then provided to the treatment provider for review of eligibility and appropriateness for the program. Recruitment was based on the treatment team’s recommendation, diagnosis of severe mental illness, a potential release date of approximately 2 to 4 years, permission to leave his assigned housing unit for treatment, and an absence of sexual misconduct infractions for at least 1 month prior to initial recruitment. Two participants’ release dates exceeded 6 years; however, they were parole eligible within 2 years. When possible, prior to beginning the intervention, participants were moved to a specified housing wing for ease of movement throughout the prison while participating in the intervention. One participant remained in a separate housing wing reserved for elderly inmates and inmates in need of ongoing medical services. Recruitment of participants occurred in group format during which the treatment provider described the treatment program and behavioral requirements for participation. Participants were then afforded the opportunity to sign an informed consent and commit to participating in the program. All participants recruited at that time agreed to participate in the intervention.
Participants at the residential treatment facility were identified by facility staff at the time of admission as a dual diagnosed resident. A list of recently admitted dual diagnosed residents was provided to the treatment provider by the facility for potential recruitment. To best ensure participants would not be discharged prior to the completion of the intervention, only recently admitted residents were recruited to participate. These residents were approached in group format where they were educated about the treatment program and behavioral requirements for participation. These potential participants were then afforded the opportunity to sign an informed consent and commit to participating in the program. All participants recruited at that time agreed to participate in the intervention, with the exception of one newly admitted resident who was soon to be transferred to another facility.
Assessments were administered prior to commencement of the intervention followed by 2-month and 4-month follow-up assessments. A post-intervention assessment was conducted at the conclusion of the offender’s participation in the program (approximately 6 months after the initial assessment for participants that completed the entire program).
As this is a program evaluation of a new intervention requested to enhance clinical services, this preliminary evaluation did not utilize random assignment or a control group (e.g., an alternate treatment group, treatment as usual group) at either facility. Group therapists provided the intervention as outlined in the treatment manual. Weekly supervision monitored therapists’ adherence to the treatment manual. As the therapists in this study were psychologists-in-training, supervision was also required for case management and reviewing clinical skills development. Related readings (e.g., Andrews & Bonta, 2010; Andrews, Bonta, & Hoge, 1990; Yalom & Leszcz, 2005) were assigned as necessary.
Measures
Treatment Engagement
The Working Alliance Inventory (WAI; Horvath & Greenberg, 1989, 1994) is a 36-item questionnaire with three subscales used to assess different aspects of the working alliance. The three subscales assess (a) client and therapist agreement on the goals of therapy, (b) client and therapist agreement on how to reach the goals of therapy, and (c) the degree of confidence, trust, comfort, and acceptance between the therapist and client. The WAI has client and therapist versions; however, only the client version was utilized in this study. On the WAI the client is asked, using a 7-point Likert-type scale ranging from 1 (never) to 7 (always), to indicate which statements best describe their experience of the therapeutic alliance. Subscale scores range from 12 to 84, and can be summed to obtain a total score with a range of 36 to 252. The WAI has high internal consistency with Cronbach’s alpha ranging from .89 to .92 for the global measure and the three subscales (132). In addition, the WAI has “good” convergent validity (see Horvath & Greenberg, 1989; Safran & Wallner, 1991).
Treatment Satisfaction
The Client Satisfaction Questionnaire (CSQ-8; Larsen, Attkisson, Hargreaves, & Nguyen, 1979) is an eight-item self-report measure, utilizing a 4-point Likert-type response scale, to assess client satisfaction with mental health services. Initial measures of the CSQ-8 by Larsen et al. (1979) resulted in an alpha coefficient of .93 indicating good internal consistency. Furthermore, Larsen et al. found an alpha coefficient of .92, again indicating high internal consistency. In addition, only one factor has consistently been yielded during factor analysis of the CSQ-8 (Gaston & Sabourin, 1992).
Treatment Effectiveness
The Outcome Questionnaire (OQ-45; Lambert et al., 1996) is a 45-item questionnaire used to assess client progress in therapy and is designed to be administered repeatedly throughout treatment. Each item is scored on a 5-point scale with a total score range from 0 to 180, where a higher total score indicates elevated levels of client distress and pathology. The OQ-45 measures clients’ subjective discomfort/symptoms, problems in interpersonal relationships and problems in social role performance. The items also measure individual and social characteristics that affect the client’s quality of life pertaining to positive and negative functioning. Change in client distress and pathology levels is considered significant when the total score increases by 14 points or more and passes below 64 points. Internal consistency for the OQ-45 scales are moderate to high with coefficient alphas of .91 (Symptom Distress [SD]), .74 (Interpersonal Relations [IR]), .71 (Social Role), and .93 (Total Score; Walters, 2006). The OQ-45 test–retest reliability is .84 (Ellsworth, Lambert, & Johnson, 2006).
The Symptom Checklist-90–Revised (SCL-90-R; Derogatis, 1994) is a self-report instrument designed to assess a broad range of psychological problems and symptoms. Respondents are asked to rate how distressed they have felt during the past 7 days on a list of 90 symptoms. Each item is rated on a 5-point Likert-type scale, ranging from 0 (not at all distressed) to 4 (extremely distressed). The SCL-90-R is made up of nine symptom subscales: Somatization, Obsessive-Compulsive, Interpersonal Sensitivity, Depression, Anxiety, Hostility, Phobic Anxiety, Paranoid Ideation, and Psychoticism; as well as three global indices: the Global Severity Index (GSI), the Positive Symptom Distress Index (PSDI), and the Positive Symptom Total. The overall score for clinical distress, the GSI, which is reflective of the number and severity of all items endorsed, is the most commonly used scale in therapy outcome research (Elliot et al., 2006). Coefficient alphas to assess internal consistency for the SCL-90-R scales used in the present study were Depression, .90; Anxiety, .88; Hostility, .85; Paranoid Ideation, .79; and Psychoticism, .80 (Derogatis, Rickels, & Rock, 1976). Test–retest reliability coefficients were calculated at 1- and 10-week intervals and ranged from 0.78 to 0.90 (Derogatis, 1994; Horowitz, Rosenberg, Baer, Ureno, & Villasenor, 1988). In addition, the SCL-90-R has been reported to display acceptable levels of convergent validity (Derogatis et al., 1976; Dinning & Evans, 1977). Finally, the SCL-90-R is frequently used as a mental health outcome measure, and this instrument has shown to be sensitive to change in psychotherapy (Crits-Cristoph, 1992; Kopta, Howard, Lowrey, & Beutler, 1994).
The Psychological Inventory of Criminal Thinking Styles (PICTS; Walters, 1995a, 1995b) is an 80-item self-report measure designed to assess the cognitive thinking patterns associated with serious criminal behavior. Scores utilized in this study were calculated for two content scales (Current Criminal Thinking and Historical Criminal Thinking), and two composite scales (Proactive Criminal Thinking and Reactive Criminal Thinking), with higher scores being indicative of a higher degree of criminal thinking (Walters, 2001). The PICTS scales used in this study have high internal consistency with Coefficient alphas of Proactive, .83; Reactive, .91; Current, .88, and Historical, .83 (Walters, 2006). Scale test–retest reliability coefficients were also found to be adequate for male and female offenders, ranging from 0.68 to 0.85 after 2 weeks, and 0.57 to 0.72 after 12-weeks (Walters, 1995a; Walters, Elliott, & Miscoll, 1998). In terms of validity, the PICTS scales were found to correlate modestly to moderately with other measures of criminality, such as the number of prior arrests, the number of prior commitments, the age at first arrest, the age at first commitment, the Hare Psychopathy Checklist–Revised, and the Lifestyle Criminality Screening Form (see Walters, 2001, for a review). Thus, the psychometric properties of the PICTS appear to be adequate for the exploratory purposes of this study.
Data Analytic Plan
The focus of this preliminary evaluation was to examine fidelity, engagement, treatment satisfaction, and the preliminary effectiveness of Changing Lives and Changing Outcomes. Change in targeted symptoms was assessed using a pre–post test design. T tests were used to examine differences in pre-treatment and post-treatment test scores for mental health symptoms (from the SCL-90-R), criminal thinking (from the PICTS), and general treatment outcome functioning (from the OQ-45). Cohen’s effect sizes were included to examine the magnitude of treatment effects. To determine whether change was clinically meaningful, we examined pre–post changes in relation to the clinical cutoffs for the instrument being used. For example, did offenders in the clinically significant range at pre-intervention fall into the nonclinically significant range at post-intervention? Finally, given we are interested in not only statistically significant findings but reliable and practical change we calculated a reliable change index on the self-report measures. Using Jacobson and Truax’s (1991) strategy of incorporating reliabilities into pre- and post-testing change scores, each change score is transformed into a standardized score. Reported is the percent of the sample that had a reliable change score above a standard score of 1.96 (p < .05).
Results
Fidelity, Engagement, and Treatment Satisfaction
Treatment fidelity was measured by program attendance and treatment completion. Participants attended 94% of all sessions. Although participants at the residential treatment facility could refuse to attend sessions, there was institutional policy that staff could issue a disciplinary infraction for not attending scheduled programming. For purposes of this program, staff was discouraged from issuing disciplinary infractions for missed sessions and we are unaware of any participants being issued a disciplinary infraction for not attending a session. Nevertheless, it is possible that the mere possibility of receiving a disciplinary infraction for missed attendance influenced the attendance rate at that facility.
Of the 50 participants initially enrolled to complete the program, three were dismissed from the group almost immediately (within two sessions) due to not meeting group admission criteria (n = 1), elected to return to jail rather than participate in the residential treatment program (n = 1), and due to transfer to an alternate treatment program (n = 1). Of the remaining 47 participants, 31 (65.9%) completed the program or all sessions they were eligible to complete. Thus, 16 (34%) participants were unsuccessfully discharged from the program. Reasons for treatment noncompletion included institutional misconduct (n = 13), psychiatric relapse (i.e., hospitalization in an acute psychiatric unit; n = 1), criminal recidivism (i.e., charged with a new crime; n = 1), and interfering with treatment process (n = 1).
Treatment engagement was assessed by homework compliance, participation in group discussions, and responses to the WAI. Treatment completers completed 83.5% of assigned homework (homework is assigned in 66 of the 74 sessions). Group members’ participation for all sessions was rated on a 10-point Likert-type scale by the therapist facilitating the group. Anchors for these ratings were 1 = no participation in activities/discussion or generally disruptive to the session, 5 = participated in activities/discussion when prompted, and 10 = active participation in activities and contributed to session discussion. Completers received an average participation rating of 8.12 (SD = 1.03) across 333 sessions. Noncompleters received an average participation rating of 7.06 (SD = 1.91) across 149 sessions. Results suggest that participants evidenced commitment (i.e., were engaged) to participating in the treatment as measured by homework compliance and therapist ratings of session participation. Results of the WAI indicated completers (n = 19, 12 participants missing WAI scores) reported strong agreement between themselves and therapists on the behaviors that are the basis of treatment (M = 69.7, SD = 14.2), the therapeutic bond with the therapist (M = 70.6, SD = 14.2), and on the goals of therapy (M = 68.9, SD = 15.5).
Program completers treatment satisfaction was measured by the CSQ-8 on a 4-point Likert-type scale (4 = greater satisfaction, n = 17). Results indicated consistently positive results for participant ratings of quality of service (M = 3.53, SD = 0.41), received desired service (M = 3.35, SD = 0.79), program met the participants’ needs (M = 3.47, SD = 0.52), willingness to recommend the program (M = 3.53, SD = 0.51), satisfaction with quantity of service received (M = 3.59, SD = 0.51), ability of service to help with problems (M = 3.47, SD = 0.51), overall satisfaction with treatment program (M = 3.53, SD = 0.51), and willingness to seek help from this program in the future (M = 3.53, SD = 0.51).
Outcome Assessment
Table 1 presents descriptive statistics, t-tests results, Cohen’s d effect sizes, and reliability of change index for participants’ pre–post test scores on scales from the OQ-45, SCL-90-R, and PICTS.
Descriptive Statistics and Results of Outcome Evaluation Results for Measures of Mental Health Functioning and Criminal Thinking
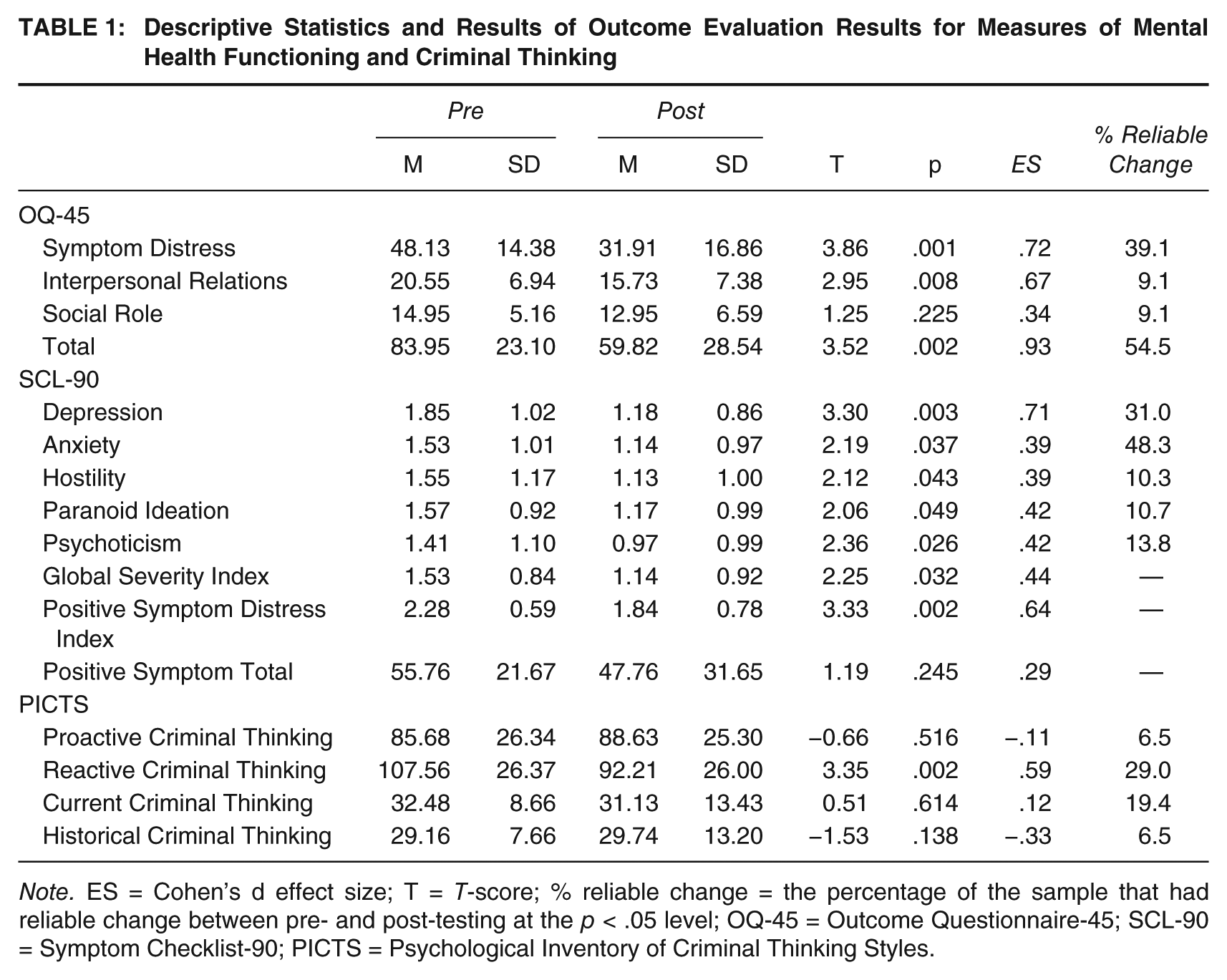
Note. ES = Cohen’s d effect size; T = T-score; % reliable change = the percentage of the sample that had reliable change between pre- and post-testing at the p < .05 level; OQ-45 = Outcome Questionnaire-45; SCL-90 = Symptom Checklist-90; PICTS = Psychological Inventory of Criminal Thinking Styles.
General Mental Health Treatment OQ-45
T tests performed on pre- and post-test OQ-45 scale scores indicated statistically significant (p < .05) reductions for SD, IR, and the OQ-45 total score. Cohen’s d effect sizes for these three scales were 0.72, 0.67, and 0.93, respectively, indicating medium–large treatment effects. For the OQ-45, a total score of 63 or more indicates clinically significant distress. It is noted that at pre-testing participants obtained a mean total score of 84 (clinically significant) and at post-testing participants obtained a mean total score of 60 (subclinical distress) indicating a clinically significant treatment effect. Similarly, a cut score of 36 or more on the SD scale is clinically significant (38) and results of this intervention produced a clinically significant reduction from 48 (pre-test) to 32 (post-test). Interpersonal functioning as measured by the IR scale went from clinically significant (M = 21; clinically significant cut score = 15) down to the clinical cut score threshold (16) at post-test. At a p < .05 level, 39.1% of the participants demonstrated reliable pre- and post-testing change on SD, 9.1% on Interpersonal Functioning, 9.1% on Social Role, and 54.5% on the OQ-45 Total Score.
Mental Health Symptoms
T tests performed on pre–post SCL-90-R scores indicated statistically significant (p < .05) treatment gains for Depression, Anxiety, Hostility, Paranoid Ideation, Psychoticism, symptom severity (GSI), and symptom intensity (PSDI) scales. Cohen’s effect sizes for these scales indicated medium treatment effects for Anxiety, Hostility, Paranoid Ideation, Psychoticism, and symptom severity scales (Cohen’s d range = 0.39-0.44) and moderately large treatment effects for Depression (Cohen’s d = 0.71) and symptom intensity (Cohen’s d = 0.64) scales. Examining the pre-treatment clinical profile of the SCL-90-R indicated that the mean scale scores did not reach the clinically significant threshold; however, all of the mean scale scores were above the mean scores for the inpatient psychiatric male normative sample and at post-treatment the Depression, Anxiety, and symptom intensity scales dropped below the mean scale scores when compared with the inpatient psychiatric male normative sample. At a p < .05 level, 31.0% of the participants demonstrated a reliable pre- and post-testing change on Depression, 48.3% on Anxiety, 10.3% on Hostility, 10.7% on Paranoid Ideation, and 13.8% on Psychoticism.
Criminal Thinking
Changes in criminal thinking were assessed by the Proactive and Reactive criminal thinking scales and the Current and Historical criminal thinking scales of the PICTS. Results of t tests indicated statistically significant (p < .05) reductions in Reactive criminal thinking; no significant differences were found for the remaining three scales. Cohen’s d for the Reactive criminal thinking scale was 0.59 indicating a moderate treatment effect. In addition to the intervention producing a statistically significant treatment effect of moderate size, the mean pre-test (M T-score = 63) to post-test (M T-score = 57) reflected a clinical reduction from high (pre) to average (post) T-scores according to Walters’s (2006) interpretation guidelines. At a p < .05 level, 6.5% of the participants demonstrated a reliable pre- and post-testing change on the Proactive scale, 29.0% on Reactive, 19.4% on Current, and 6.5% on the Historical scale.
Discussion
Changing Lives and Changing Outcomes is a comprehensive treatment program designed to meet the mental health and criminal justice needs of OMI. It is, to the best of our knowledge, the first intervention of its kind for intervening with this unique population. Results of this evaluation indicated that in spite of the intense nature of this program, participants were able to complete it at a satisfactory rate. Furthermore, participants engaged in the treatment process as measured by session participation and homework compliance. They were engaged with their therapists, agreed upon the goals and tasks of therapy, and were generally satisfied with the treatment program. Of greater significance though is the outcome assessment from this preliminary evaluation. We utilized a four-tiered evaluation process consisting of pre–post significance testing, calculation of effect sizes to measure the magnitude of effect, examination of clinical cutoffs to measure clinically significant change, and reliable change scores (see Jacobson & Truax, 1991) to identify the percentage of treated individuals that experienced meaningful and reliable change. Results of the outcome assessment indicated statistically and clinically significant reductions in mental health symptoms and distress, and modest reductions in reactive criminal thinking (reactive criminal thinking consists of a hostile attributional bias that is predictive of reactionary type crimes/violence, for example, assaults, domestic violence; Walters, Frederick, & Schlauch, 2007).
The strength and innovation in Changing Lives and Changing Outcomes is the integration of the best evidenced-based practices in the mental health and criminal justice fields. In keeping with recent advances in the treatment of co-occurring disorders that recommend unified treatment protocols (Allen et al., 2008), or an integrated therapeutic approach (Nathan & Gorman, 2007), Changing Lives and Changing Outcomes provides a framework for intervening when mental illness and criminalness co-occur. The goal of Changing Lives and Changing Outcomes is to enhance quality of life by increasing functional “good” days and reducing psychiatric and criminal recidivism, thereby extending beyond the goals of criminal justice diversion initiatives or behavioral health interventions aimed at managing or controlling offenders. Results of this preliminary evaluation suggest that we can, in fact, improve psychiatric status, and effect change in at least one variable, criminal thinking, that is strongly associated with criminal recidivism (see Andrews & Bonta, 2010, for a review of criminal prediction literature).
Based on the results of this preliminary evaluation, program modification is warranted. Specifically, the results regarding significant and reliable change in participants’ antisocial attitudes are encouraging, especially when considered in the context of criminal thinking and antisocial attitudes as strong predictors of criminal recidivism (see Andrews & Bonta, 2010); however, we desired even greater effects. Thus, to increase the potential effect, we are increasing the Problematic Thoughts and Attitudes module from 10 sessions to 13 (total program length now = 77 sessions) and we have made this the third module (after the Preparing for Change and Mental Illness and Criminal Awareness modules) in the sequence to allow for more observations and intervention points (i.e., treatment providers can address issues of criminal thinking and antisocial attitudes throughout the remaining modules). For example, in the Medication Adherence module, participants’ attitudes and dysfunctional thoughts that are supportive of a criminal lifestyle and interfere with prosocial decision making, such as medication compliance, can be challenged. It is anticipated that this increased focus will produce even greater and more reliable change in an area of functioning that is not only critical to offender success (see Andrews & Bonta, 2010) but one that is also difficult to change (see Reid & Gacono, 2000; Samenow, 2001).
Although the results of this preliminary evaluation are promising much work remains to be done. First, the sample size is insufficient to make global conclusions regarding the success of the intervention. As this evaluation was conducted with clinically obtained data, we were unable to implement a control group comparison or random assignment to treatment versus control group conditions. Future work must include comparisons to control groups including alternate treatments that are appropriate for OMI, and random assignment to therapeutic conditions is necessary. Randomized controlled clinical trials are the gold standard for treatment outcome work and should be the benchmark for evaluating Changing Lives and Changing Outcomes. In future studies, treatment providers will not be responsible for obtaining clinical data due to potential biasing (e.g., inflated working alliance scores) from such a methodology. This evaluation was also limited by the absence of clinical data (e.g., OQ-45, SCL-90, PICTS) at time of termination that would allow for comparisons between completers and noncompleters. Finally, future studies should include behavioral data (e.g., work performance, time to program graduation, disciplinary infractions) and not be limited to self-report measures.
Footnotes
Acknowledgements
The authors are thankful to Marshall Bewley and Chris Romani for facilitating treatment groups included in this program evaluation. We are thankful to Matthew Gutierrez, Angelea Bolanos, Tori Dean, and Katy White for assisting with data entry and scoring of measures.
This project was funded by the Center for Behavioral Health Services & Criminal Justice research.