
Abstract
Little is known about the role of conflict management in explaining the victim–offender overlap. This article assesses the victim–offender overlap for adults (18-32) in intimate and nonintimate relationships, covering their relationship with their partner and with friends and acquaintances/strangers. Controlling for conceptually important variables, we explore whether different conflict management styles are associated with a respondent being in the victim-only, offender-only, both, or neither group (separately for verbal aggression, physical abuse for intimate and nonintimate relationships, and sexual abuse for intimate relationships). Data are from a nationally representative panel of U.S. households (N = 2,284 respondents of whom 871 women and 690 men report being in an intimate partnership). We observed a high degree of overlap between victimization and offending across our abuse measures. We found a range of modestly consistent set of risk factors, for example, conflict management styles and self-control, for the victim–offender overlap for partner and nonpartner abuse experiences.
While the field of criminology studies victims and offenders as mostly distinct groups, newer research suggests that they share a number of demographic and behavioral similarities (Muftić & Hunt, 2013). In fact, the “victim–offender overlap” is a consistent observation. Research showing a link between individuals reporting both violent offending and victimization exists across multiple conflicts, including delinquency, homicide, and other violent crime (Gottfredson, 1981). Recent studies (Schreck, Berg, Ousey, Stewart, & Miller, 2017) have also found that previous victimization has been a strong predictor of later perpetration among U.S. urban youth and young adults (Reingle & Maldonado-Molina, 2012; Zimmerman, Farrell, & Posick, 2017).
Our study focuses on assessing the victim–offender overlap among young adults in intimate relationships, an understudied area (Muftić, Finn, & Marsh, 2015; Tillyer & Wright, 2014). Furthermore, a novel approach is used, investigating offending and victimization within and outside of the intimate relationship. The victim–offender overlap is investigated by asking participants to report on aspects of their intimate relationship and aspects of their nonintimate relationships. While previously identified risk factors from the overlap literature are examined, the article also investigates a new construct, conflict management style (CMS), and assesses a wider variety of aggressive behaviors over a broader age range (18-32) than most of the prior research.
Verbal aggression, physical abuse, and sexual abuse are examined as separate categories rather than one overall intimate partner violence (IPV) category. By collapsing these acts into a single dependent variable, researchers risk combining separate behaviors and experiences that might have unique determinants and that might also differ importantly by gender (Tillyer & Wright, 2014). While there is a considerable overlap of victims and offenders, some crime victims share little resemblance to offenders (Maldonado-Molina, Jennings, Tobler, Piquero, & Canino, 2010; Muftić et al., 2015), but there appears to be more evidence of similarities than differences (Schreck, Stewart, & Osgood, 2008). The victim–offender overlap in this study is defined as an individual who self-identified as an offender in at least one verbal aggression (past 6 months) or physical and sexual abuse (past 12 months) incident and also self-reported as a victim in at least one verbal aggression or physical and sexual abuse incident over the same period. These incidents may have occurred within a single relationship or within different relationships.
Predictors of the Victim–Offender Overlap
Researchers have reported that the victim–offender overlap is associated with a number of person-level demographic factors (Sampson & Lauritsen, 1990), family factors (Zimmerman et al., 2017), substance use (Reingle & Maldonado-Molina, 2012), and relational attributes of the victim and the offender (Zimmerman et al., 2017). One of the most consistent predictors of the victim–offender overlap is low self-control (Schreck, 1999; Schreck et al., 2008), linked to both offending (Pratt & Cullen, 2000) and victimization (Holtfreter, Reisig, & Pratt, 2008). In a sample of young adults, low self-control predicted overlap between general violence victimization and offending (Flexon, Meldrum, & Piquero, 2016), consistent with adolescent research (Jennings, Higgins, Tewksbury, Gover, & Piquero, 2010). Our article draws on Gottfredson and Hirschi’s (1990) self-control theory which suggests that both victimization and offending are produced by similar processes and experiences emanating from individuals’ socialization and experiences with family (Schreck, 1999). Individuals who exhibit low self-control are more likely to place themselves in situations in which their risky behaviors connect them with offenders as co-offenders or victims (Holtfreter et al., 2008).
Limited attention has been paid in the overlap literature to CMS and predictions from psychological theories of aggression focused on the determinants and consequences of interpersonal conflict (Tedeschi & Felson, 1994). Originally, Blake and Mouton (1970) described approaches to managing organizational conflict that are reflective of the typical give and take in interpersonal conflict. These include conciliatory styles such as avoiding, integrating or ignoring problems, accommodating, compromising, and collaborating and more aggressive competing styles such as dominating or forcing (Blake & Mouton, 1970). This research has been incorporated into theories of aggression and interpersonal violence (Tedeschi & Felson, 1994). CMS is a potentially missing link in the study of understanding the victim–offender overlap (Felson, Berg, Rogers, & Krajewski, 2018). Knowing how people generally handle conflict in disputes may be key to understanding why the same people often rotate between the roles of victim and offender and how violence tends to develop from routine disputes (Felson, 1984). Furthermore, there is evidence of cross-situational consistency in CMS (Furman & Buhrmester, 1992). CMS thus appears to represent general interactional tendencies during hostile exchanges (P. M. Miller, Danaher, & Forbes, 1986) and may help explain the overlap.
IPV
Although a somewhat controversial topic within IPV, given the prominence of feminist-based approaches to IPV interventions that assume a male batterer and female victim, the overlap of victimization and offending has received some attention from IPV researchers. Based on the Centers for Disease Control and Prevention (CDC) definition, IPV refers to verbal aggression, physical abuse, and sexual abuse between a current or former intimate partner or spouse (Breiding, Basile, Smith, Black, & Mahendra, 2015). While there is strong evidence of the victim–offender overlap for general criminal behavior, studies examining the overlap for IPV are less common. As argued by researchers (Tillyer & Wright, 2014), given the ubiquity of IPV and evidence that at least some IPV has been characterized as “mutual” (M. P. Johnson & Ferraro, 2000; Steinmetz, 1980), the existence of the victim–offender overlap within IPV warrants further study. Building on typologies identified by M. P. Johnson (2011), a common form of IPV is gender-symmetric situational violence. Studies also find that the correlates of IPV are generally the same correlates of nonpartner violence, suggesting the two forms of violence are generated by a common or similar set of social causes (Moffitt & Caspi, 1999).
Within intimate partnerships, given the presumed regular interactions and close proximity of two persons, whatever the circumstances that produced the violence, if left unresolved, can lead to more conflicts and a switching of victim or offender roles (Tillyer & Wright, 2014). In one of the strongest studies assessing the overlap for IPV (using data from the National Longitudinal Study of Adolescent Health [Add Health] sample), Reingle and colleagues found evidence for the IPV “victim–offender” overlap (Reingle, Staras, Jennings, Branchini, & Maldonado-Molina, 2012). Tillyer and Wright’s (2014) analysis of Add Health data revealed that the victim–offender overlap exists for IPV (defined as physical abuse). About 80% of respondents reported no involvement in IPV in the past year; among those reporting any IPV, 9.7% identified as a victim only, 3.8% identified as a perpetrator only, and 6.7% reported both IPV victimization and perpetration in the prior year (Tillyer & Wright, 2014). Of the 697 IPV victims, 40.5% were also IPV perpetrators, demonstrating a high rate of 41% of victim–offender overlap (Tillyer & Wright, 2014). Also, those just perpetrators and those victims and perpetrators presented with similar characteristics distinct from the profiles of those who were just victims (Tillyer & Wright, 2014).
Muftic and colleagues (2015) also found an overlap in IPV using crime report/police data for all adults. From a sample of 1,256 cases of IPV from police reports, 37% were IPV victims only, 17.9% were persistent IPV offenders (individuals who perpetrated IPV in the original incident, but did not experience domestic violence [DV] victimization in the 18+-month follow-up period), 18% were desistent IPV offenders (individuals who engaged in IPV offending in the original incident but had no officially recorded record of IPV incident in the follow-up), and 27.1% were victim-offenders.
Offenders are known to consume alcohol and drugs (Riley, 1987), and research suggests that alcohol and drug consumption increases risks of victimization and offending for IPV (Nabors, 2010; Reingle et al., 2012). To account for the potential habitual routine activities formed over the course of longer partnerships, we control for the longevity/length of the relationship in our models. We also explore the variable of cohabitation, as living in the same place is likely to place the potential victim into more regular contact with their partner (i.e., more opportunity for conflicts to arise) for a longer period of time (Tillyer & Wright, 2014). Within the realm of IPV, some work has been done to assess the role of conflict management in IPV (Kurdek, 1994). An aggressive CMS seems to lead to conflict escalation (Siffert & Schwarz, 2011) and thus appears to be the least constructive in conflict resolution with partners (Rholes, Kohn, & Simpson, 2014).
The Current Study and Hypotheses
In this study, we apply psychological explanations to explore the role of CMS in explaining the overlap of victimization and offending among adult couples 18 to 32 years old using a national sample. We investigate verbal aggression, physical abuse, and sexual abuse exhibited within the couple’s relationship (“partners”) and similar behaviors experienced/perpetrated in relationships with friends and strangers (“nonpartners”) separately. We investigate risk factors for victims-only, offenders-only, and the victim–offender overlap group compared with the no abuse group. We assess the importance of CMS in intimate relationships (both interactions within and outside the relationship) while controlling for the respondents’ own internal capabilities of exerting self-control and basic elements of their routine activities. We include additional correlates suggested by research indicating that victims and offenders often have similar demographic characteristics. For example, an exploration of gender is important because IPV studies are often gender-specific (e.g., investigating male-only perpetrators or female-only victims; Tillyer & Wright, 2014). The literature on female offending continues to grow (S. Miller, 2005), and research suggests that the victim–offender overlap may be present, with female offending often occurring in the context of women being victimized by their male partners (Swan, Gambone, Caldwell, Sullivan, & Snow, 2008). Other research suggests the correlates of male offending are similar to the correlates of female offending (Moffitt, Caspi, Rutter, & Silva, 2001).
Our first hypothesis was that we would see an overlap of victimization and perpetration across verbal aggression, physical abuse, and sexual abuse measures of partner and nonpartner abuse. We expect that, among abuse victims, the victim-only group would represent a smaller percentage of cases than the overlap group. We held a similar expectation for those perpetrating abuse. Our second hypothesis was that how the respondent and their partners and nonpartners manage conflict and self-control would be the most consistent and strongest predictors of the victim–offender overlap. Our third hypothesis was we would observe similar sociodemographic and substance use risk factors for each of our comparison groups relative to the no abuse group.
Method
Participants
The sample was drawn from the online AmeriSpeak panel to participate in the Interpersonal Conflict and Resolution (iCOR) study. Participants were 1,562 (872 women and 690 men) general population young adults (mean age = 26) reporting that they were currently in an intimate relationship. The participants report on aspects of their intimate partner relationship (someone they are seeing, dating, living with, or married to) and aspects of their nonintimate relationships (friends and acquaintances/strangers). As seen in Table 1, participants described themselves as White (57.4%), Hispanic (20.9%), Black (12.1%), and Other (9.6%). Median household income was US$37,500. Participants reported that their intimate relationships had lasted 4.6 years at the time of the survey, with 67% currently cohabitating with their partner.
Sample Description
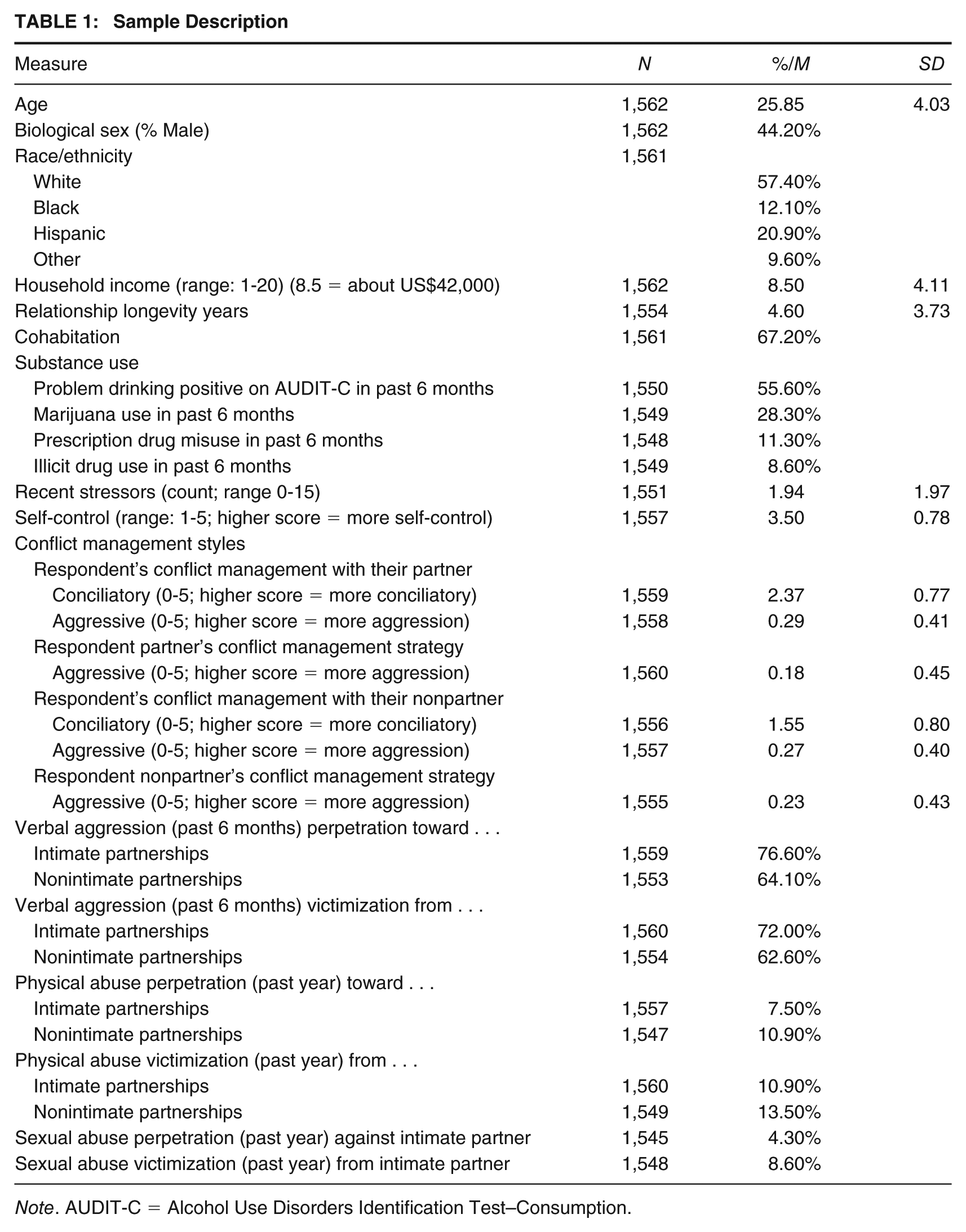
Note. AUDIT-C = Alcohol Use Disorders Identification Test–Consumption.
Measures
Dependent Variables
Abuse/aggression outcomes were assessed for two types of relationships: (a) The respondent’s current intimate partner or spouse, defined as seeing each other, dating, living together, or married. Those respondents involved in more than one romantic relationship were asked to pick the person with whom they spend the most time as the partner who would be referenced in the ensuing iCOR survey. (b) Nonintimate partners such as friends (defined as people whom the respondent knows well and feels very friendly toward and who feels friendly toward the respondent in return) and acquaintances/strangers (defined as people the respondent occasionally encounters but does not really know or people whom the respondent has never seen before). We developed five victim–offender overlap measures separately for intimate partner (a) verbal aggression, (b) physical abuse, (c) sexual abuse, and nonpartner (d) verbal aggression and (e) physical abuse. Each of these measures was coded as a categorical variable with four categories from 0 (no abuse/aggression), 1 (victimization only), 2 (offending only), and 3 (both).
Verbal aggression was measured by asking respondents to think about some unpleasant or hostile interactions they may have had. They were then asked to indicate how often in the past 6 months they had engaged in (and were the victim of) the following five behaviors in relationships with partners and nonpartners, separately: (a) shouting, name-calling, insults, and other confrontational behavior; (b) accusing the counterpart of wrong-doing (e.g., cheating, breaking rules, backing out on a commitment); (c) accusing the counterpart of disrespect or poor treatment; (d) attempts to get the counterpart to do something he or she did not want to do; and (e) put down or otherwise made counterpart feel worthless. Responses were based on a 5-point scale (never, less than once a month, 1-2 times a month, once a week, more than once a week). The average score across the five items had good reliability (Cronbach’s α =.86 for verbal aggression victimization and Cronbach’s α =.82 for verbal aggression offending) and was coded such that a higher score reflects more frequent perpetration of verbal aggression separately for victimization and perpetration (note all Cronbach’s alpha scores reported in this section are based on the current sample). These items were based on the work of multiple researchers (Felson, 1992; Straus, Hamby, Boney-McCoy, & Sugarman, 1996; Tedeschi, 1984).
Physical abuse was measured for relationships with partners and nonpartners (separately), with two global items (Centers for Disease Control and Prevention, 2018) covering the number of times in the past year the respondent recalled (a) striking a counterpart with an object or weapon and (b) punching, kicking, scratching, biting, slapping, or hitting counterpart with your fist. We also asked whether the respondent was a victim of the same items from the counterpart. A value of 1 was equivalent to any physical abuse in the past year and 0 was equivalent to no physical abuse in the past year for physical abuse victimization and perpetration measures separately. The alpha scores were over .8 for physical abuse victimization and offending scales.
Based on the Youth Risk Behavior Surveillance measure of sexual abuse, intimate partner sexual abuse was measured with single global item (Centers for Disease Control and Prevention, 2018), separately for perpetration and victimization, covering the number of times in the past year the respondent had “forced someone you were married to, dating or going out with to do sexual things that they did not want to do.” We also asked whether the respondent was a victim of their intimate partner forcing them to do sexual things that they did not want to do. The respondents were instructed to include but not limit in their count such things as kissing, touching, or physically forcing them to have sexual intercourse. We dichotomized both the victimization and the perpetration measures ranging from 0 (no sexual abuse) to 1 (any sexual abuse). We did not include measures of sexual abuse for nonintimate partners.
Independent Variables
CMS measures were based on work on interpersonal conflict (Felson, 1992; Phillips & Cooney, 2005; Steadman, 1982). For this article, exploratory followed by confirmatory factor analyses of the CMS measures yielded a two-factor solution (alpha reliability was all above .8 for both factor scales) which was consistent for our measures of the respondent’s CMS with partners and nonpartners. Factor 1—conciliatory CMS included the following items: apologize to, give in to, find a middle ground, walk away, try to explain, and get help from others. The scale response for all CMS items were 1 (never), 2 (rarely), 3 (sometimes), 4 (frequently), and 5 (always). Factor 2—aggressive CMS included the following items: argue with, physically threaten, verbally threaten, put the other person down verbally, strike the other person, and punch the other person. We further asked the respondent to report on their perception of the usual CMS of their partner and nonpartners, with similar items but worded to reflect the behavior of the respondent’s partner/nonpartner. Respondents were asked about their own aggressive CMS with their partners and nonpartners, but conciliatory styles were only asked of the respondent’s own behavior but not their partners’ or nonpartners’ conciliatory CMS. We did not measure the use of CMS by the respondent’s partner or nonpartner because we did not believe the respondent could accurately report on this issue (e.g., how would the respondent know whether their partner or nonpartner felt they were apologizing, giving in, finding a middle ground, or trying to explain themselves). Item averages were computed for each scale. We coded three continuous variables representing the respondents’ CMS first toward intimate partners where the (a) respondent uses a conciliatory CMS, (b) the respondent uses an aggressive CMS, or (c) the respondent’s partner uses aggressive CMS. Furthermore, we coded three variables representing the respondent’s CMS vis-à-vis nonpartners where (d) the respondent uses a conciliatory CMS, (e) the respondent uses an aggressive CMS, or (f) the respondent’s nonpartner uses an aggressive CMS. Higher values on each variable indicate greater frequency of implementing that specific CMS scale.
Recent life stressors were assessed through a checklist of exposure to 16 potential stressors or adverse life events in the past 6 months (e.g., serious injury, illness, or a death in the family; breakup of a romantic relationship or divorce; trouble with the law) using a modified scale (Ge, Conger, Lorenz, & Simons, 1994). Response options were 1 (yes) or 0 (no). A summary count of exposures was created, ranging from 0 to 16 recent stressors. The scale had a Cronbach’s alpha of .87, where higher values are interpreted as being more frequent stressful life events.
Self-control draws from the Brief Self-Control Scale (Tangney, Baumeister, & Boone, 2004). We fielded an eight-item version of this scale (Cronbach’s α = .82), including measures of restraint (e.g., have a hard time breaking bad habits) and impulsivity (e.g., often act without thinking through all the alternatives), based on modifications from other (Maloney, Grawitch, & Barber, 2012). Scale scores ranged from 1 (not at all like me) to 5 (very much like me), as an item average of the eight items. A higher score reflects greater levels of self-control.
Alcohol use and substance use were measured separately. An indicator of problem drinking over the past 6 months was assessed with the three-item Alcohol Use Disorders Identification Test–Consumption (AUDIT-C) scale, with a score range of 0 to 12. An indicator was coded 1 (for problem drinking) and 0 (for negative to alcohol screener), reflecting scores of 4 or more for males and 3 or more for females (Bradley et al., 2007). The scale had good reliability (Cronbach’s α =.81). Based on measures from the Add Health study (Harris, 2009), we explored marijuana use, prescription drug misuse, and illicit drug use over the past 6 months. Each drug use measure was coded on a five-point scale reflecting never, monthly or less, 2 to 4 times a month, 2 to 3 times a week, or 4 or more times a week. Each variable is coded 1 (for consuming the substance one or more times) or 0 (for no substance use; the reference category).
Nature of romantic relationship was covered with two measures. First, longevity of the current relationship was measured as the number of years the respondent has been with their partner (a continuous measure). Second, cohabitation was measured as a two-level variable with either a value of 0 (for respondents who have partners who maintain a separate residence; reference category) or a value of 1 (for respondents who share a residence with their partner).
Respondent demographics assessed in the iCOR survey instrument include biological sex assigned at birth coded from 0 (female) to 1 (male) and current age (continuous measure). Additional demographics come for the AmeriSpeak panelist survey administered annually to panelists; all iCOR prime respondents are AmeriSpeak panel members. These measures include ethnicity (White non-Hispanic, Black non-Hispanic, Hispanic, Other) and household income, an 18-level categorical measure ranging from less than US$5,000 to US$200,000 or more, treated as a continuous measure from 1 (less than US$5,000), 2 (US$5,000-US$9,999), 3 to 9 (represent US$4,999, increases up to US$49,999), 10 (US$50,000-US$59,999), 11 (US$60,000-US$74,999), 12 (US$75,000-US$84,999), 13 (US$85,000-US$99,999), 14 (US$100,000-US$124,999), 15 (US$125,000-US$149,999), 16 (US$150,000-US$174,999), 17 (US$175,000-US$199,999), and 18 (US$200,000 or more).
Procedures
This study makes use of data from the iCOR study. We drew a sample of 4,714 cases from the online AmeriSpeak panel. We achieved about a 50% participation rate in recruiting our 2,284 participants. AmeriSpeak is a probability-based, nationally representative panel of about 25,000 households covering over 99% of U.S. households. AmeriSpeak randomly selects households sampled with a known nonzero probability of selection from an extant established national frame. Households are then contacted by U.S. mail, telephone, express mailers, and interviewers (face-to-face) to capture harder to reach cases and recruit them to the panel.
Data collection (online web responses except for 71 respondents who opted for a telephone interview) took place from September 2016 through April 2017. From the iCOR sample of 2,284 cases, we selected 1,561 respondents who were in a current intimate partnership (final n = 1,541 after excluding cases with missing data; less than 1% of the sample is missing data on the outcome measures and most covariates). Staff sent a postal letter and email to eligible panel members describing the study and indicating that an invitation to participate in the survey would be forthcoming. The invitation let eligible panel members know about the survey and covered the informed consent procedures. The surveys were mostly completed in English (20 were in Spanish). A list of supportive resources was available at all times to respondents. The sample that did not respond to the initial invitation was contacted multiple times by postal mail, email, and phone. Participants received a US$15 incentive for responding to the survey.
Analysis Plan
First, poststratification weights were applied to ensure national representativeness for the project data. Following univariate analyses (Table 1), we conducted bivariate analyses on the overlap of three types of victimization and perpetration separately for abuse/aggression in relationships with intimate partners and nonpartners (Table 2). Next, we conducted multivariable analyses in Stata 14.0 with listwise deletion of missing data (less than 2% of the sample is missing data on the outcome measures and covariates), via a multinomial logistic regression model. Multinomial logistic regression model is an extension of the binary logistic regression model, where the dependent variable has more than two categories. It can be thought of as simultaneously estimating binary logistic regression for all possible comparisons among the outcome categories, but is recommended as a more parsimonious and efficient approach (Long, 1997). Multinomial regression modeling is also the approach used by other researchers studying the victim–offender overlap (Jennings et al., 2010). Analysis was conducted for each of the four categorical (i.e., no abuse/aggression, victimization only, offending only, and both victimization and offending) dependent variables, that is, partner (IPV) sexual, physical, and verbal abuse/aggression, and nonpartner physical and verbal abuse/aggression.
Overlap of Three Types of Victimization and Perpetration
Independent variables covered demographic characteristics, relationship variables, substance use, stressors, self-control, and CMS. For each independent variable, adjusted (i.e., controlling for other independent variables) odds ratios (aORs) are presented comparing the likelihood of being in the victimization-only, offender-only, and victimization and offending group compared with the reference group (no aggression/no abuse), with an aOR greater than 1 indicating increasing log odds of being in each of the three abuse/aggression categories compared with no abuse/no aggression.
Results
Descriptive results are presented in Table 1. Most participants exhibited a mid-frequency of conciliatory CMS with their partners (average score of 2.4) based on a scale of 1 (never), 2 (rarely), 3 (sometimes), 4 (frequently), and 5 (always). Participants reported slightly lower frequency of conciliatory CMS with nonintimate partners (average score of 1.6). Most of the participants and their partners (based on the respondent’s perceptions) were very low in their use of aggressive CMS in their intimate relationship (both scores on average were <.30, with 1 being the lowest level and 5 the highest level of aggressive conflict management behavior), and similar low levels of aggressive conflict management were observed within the respondents’ nonintimate relationships (both scores on average were also below .30).
Almost four in five respondents reported verbal aggression perpetrated against an intimate partner in the past 6 months (Table 1), and about two thirds reported these behaviors toward a nonintimate partner. We observed similar numbers for victimization. About 8% of the respondents reported physical abuse perpetrated against an intimate partner in the past year, and about 11% reported these behaviors toward a nonintimate partner. We observed somewhat higher rates for victimization. About 4% of the respondents reported sexual abuse perpetrated against an intimate partner in the past year, and 9% reported being a victim of sexual abuse by an intimate partner in the past year (no sexual abuse measures were available for nonintimate partners).
The basic distribution of overlap data across crime types for partners is the following (not shown in tables): 79% of the cases involve a participant who experienced IPV victimization (at least one or more of the following: sexual abuse, physical abuse, or verbal aggression) and perpetrated either one or more of the three forms of IPV abuse (with most of this overlap due to verbal aggression), 5% victimization only, 3% perpetration only, and 13% neither victimization nor perpetration. A similar distribution for overlap cases was also observed for nonpartners.
Rates of Verbal Aggression in Partner and Nonpartner Relationships
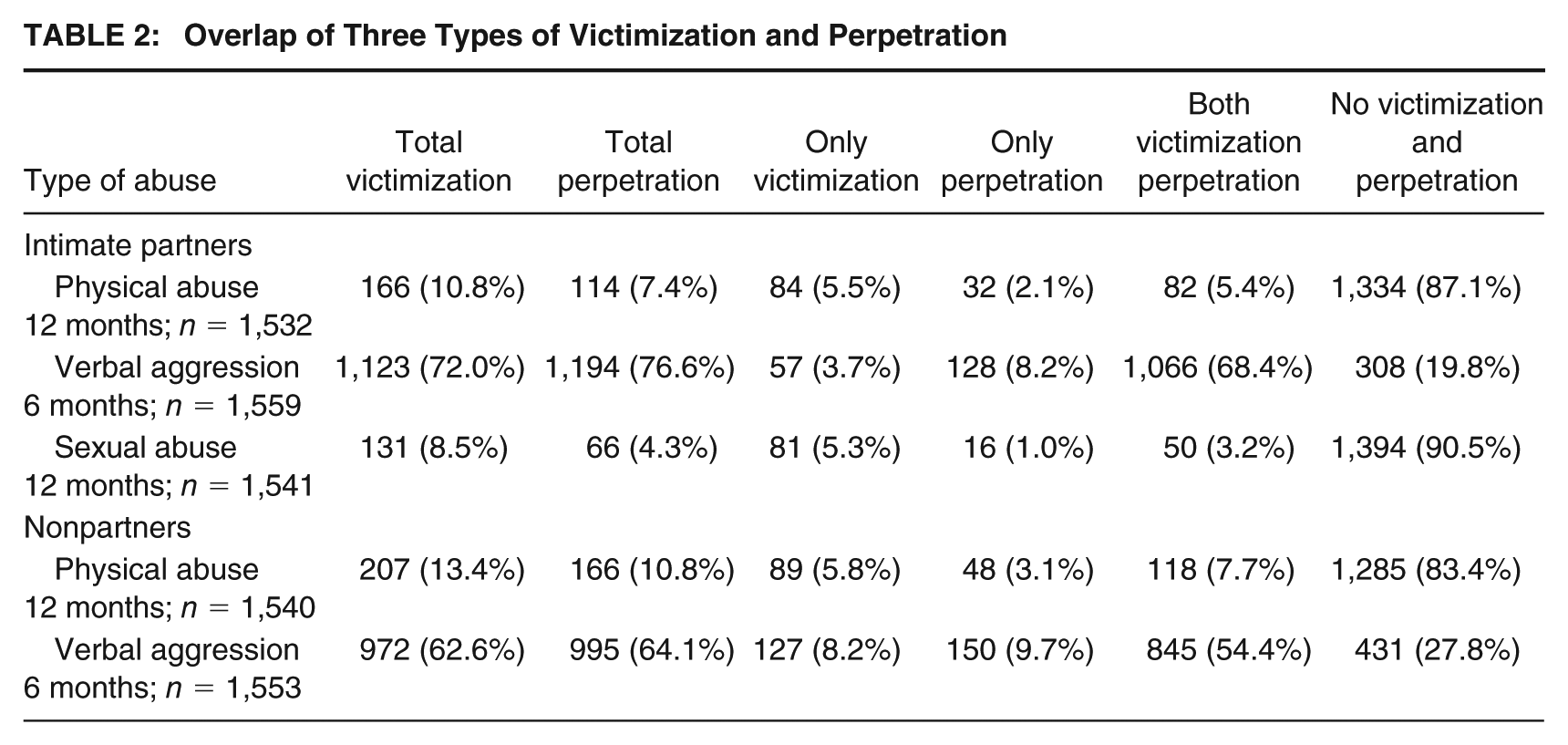
Table 2 presents additional descriptive data. As seen in Table 2, 68% of all respondents (1,066/1,559) were in the victim–offender overlap group for IPV verbal aggression (54% victim–offender overlap in nonpartner relationships for verbal aggression). Among the 1,123 victims of IPV verbal aggression, 95% (n = 1,066) were also perpetrating verbal aggression (data not shown in tables), with 87% reporting verbal aggression perpetration among victims of verbal aggression in nonpartner relationships (data not shown in tables). Among the 1,194 perpetrators of IPV verbal aggression, 89% (n = 1,066) were also victims of verbal aggression (85% of perpetrators reported verbal aggression victimization in nonpartner relationships; data not shown in tables).
Rates of Sexual Abuse in Partner Relationships
Sexual abuse among intimate partners had the least amount of overlap between victimization and perpetration. In Table 2, 3% of all respondents (50/1,541) were in the victim–offender overlap IPV sexual abuse group. Among the 131 victims of IPV sexual abuse, 38% (n = 50) were also perpetrating IPV sexual abuse (data not shown in tables). Among the 66 perpetrators of IPV sexual abuse, 76% (n = 50) reported that they were also victims of IPV sexual abuse.
Rates of Physical Abuse in Partner and Nonpartner Relationships
The overlap of IPV physical victimization and perpetration overall was about 5% (8% overlap for physical abuse with nonpartners). Among the 166 victims of IPV physical abuse, 49% (n = 82) also reported perpetrating IPV physical abuse (57% reported physical abuse in relationships with nonpartners; data not shown in tables). Among the 114 perpetrators of IPV physical abuse, 71.9% (n = 82) were also victims of IPV physical abuse (71.1% who reported perpetration of physical abuse with nonpartners also were physical abuse victims).
Multivariable Models of Verbal, Physical, and Sexual Abuse within Intimate Partnerships
Multinomial regression model results are presented in Tables 3 and 4. As detailed in the “Analysis Plan” section, aORs and significance levels were presented. Using Cohen’s guidance for interpreting odds ratios, a value of about 1.5 would be considered a small effect; 3.45, a medium effect size; and 9, a large effect size (Cohen, 1988). Chen, Cohen, and Chen (2010) have developed similar guidelines for interpreting odds ratios. Tables 3 and 4 reveal most of our significant odds ratios to be small effects, with a few medium effects. The aORs are presented for each of the outcome categories compared with the reference group (no aggression/no abuse).
Multinomial Logistic Regressions of Intimate Partner Sexual and Physical Abuse and Verbal Aggression Victimization and Offending in aORs
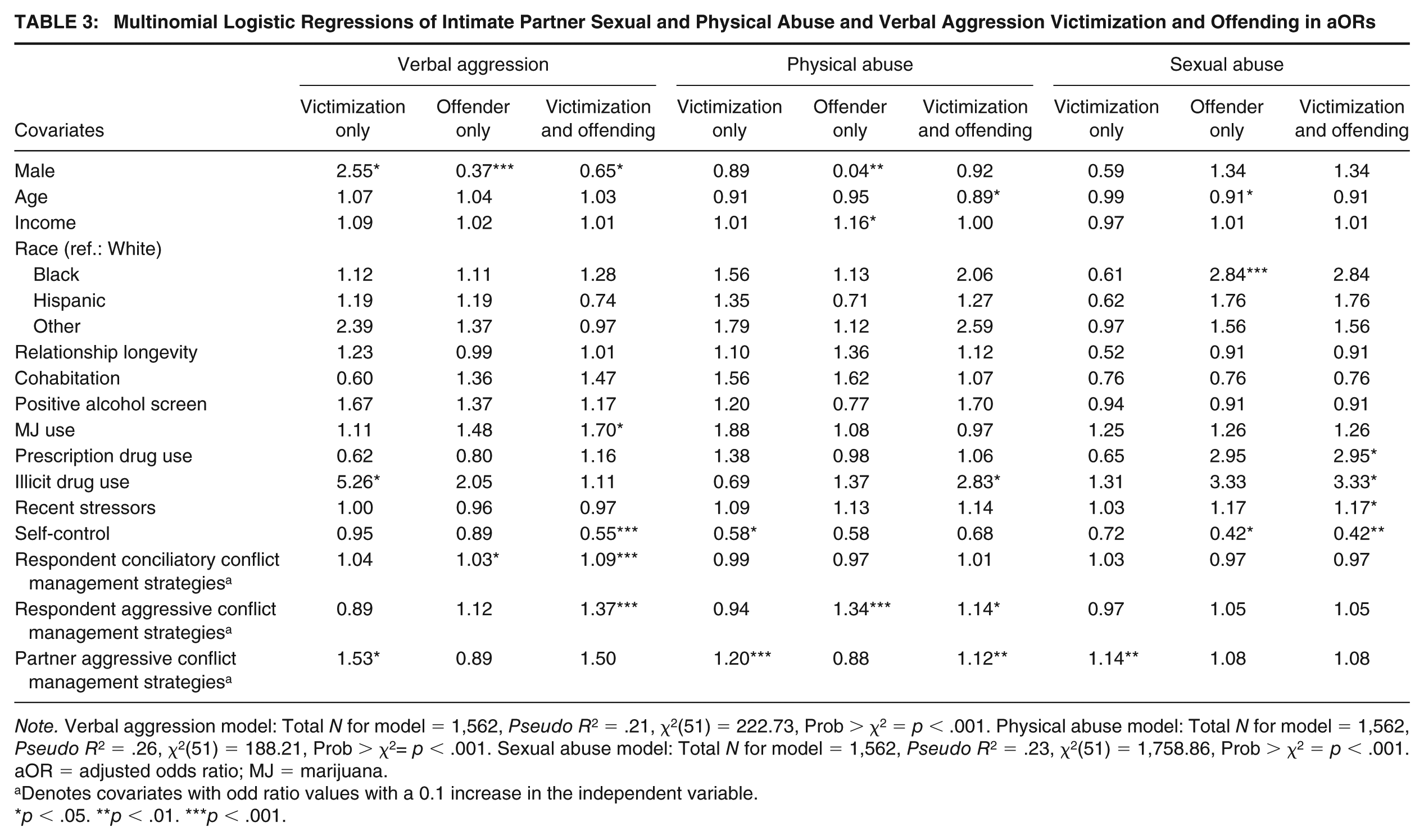
Note. Verbal aggression model: Total N for model = 1,562, Pseudo R2 = .21, χ2(51) = 222.73, Prob > χ2 = p < .001. Physical abuse model: Total N for model = 1,562, Pseudo R2 = .26, χ2(51) = 188.21, Prob > χ2= p < .001. Sexual abuse model: Total N for model = 1,562, Pseudo R2 = .23, χ2(51) = 1,758.86, Prob > χ2 = p < .001. aOR = adjusted odds ratio; MJ = marijuana.
Denotes covariates with odd ratio values with a 0.1 increase in the independent variable.
p < .05. **p < .01. ***p < .001.
Multinomial Logistic Regressions of Nonpartner Verbal Aggression and Physical Abuse Victimization and Offending
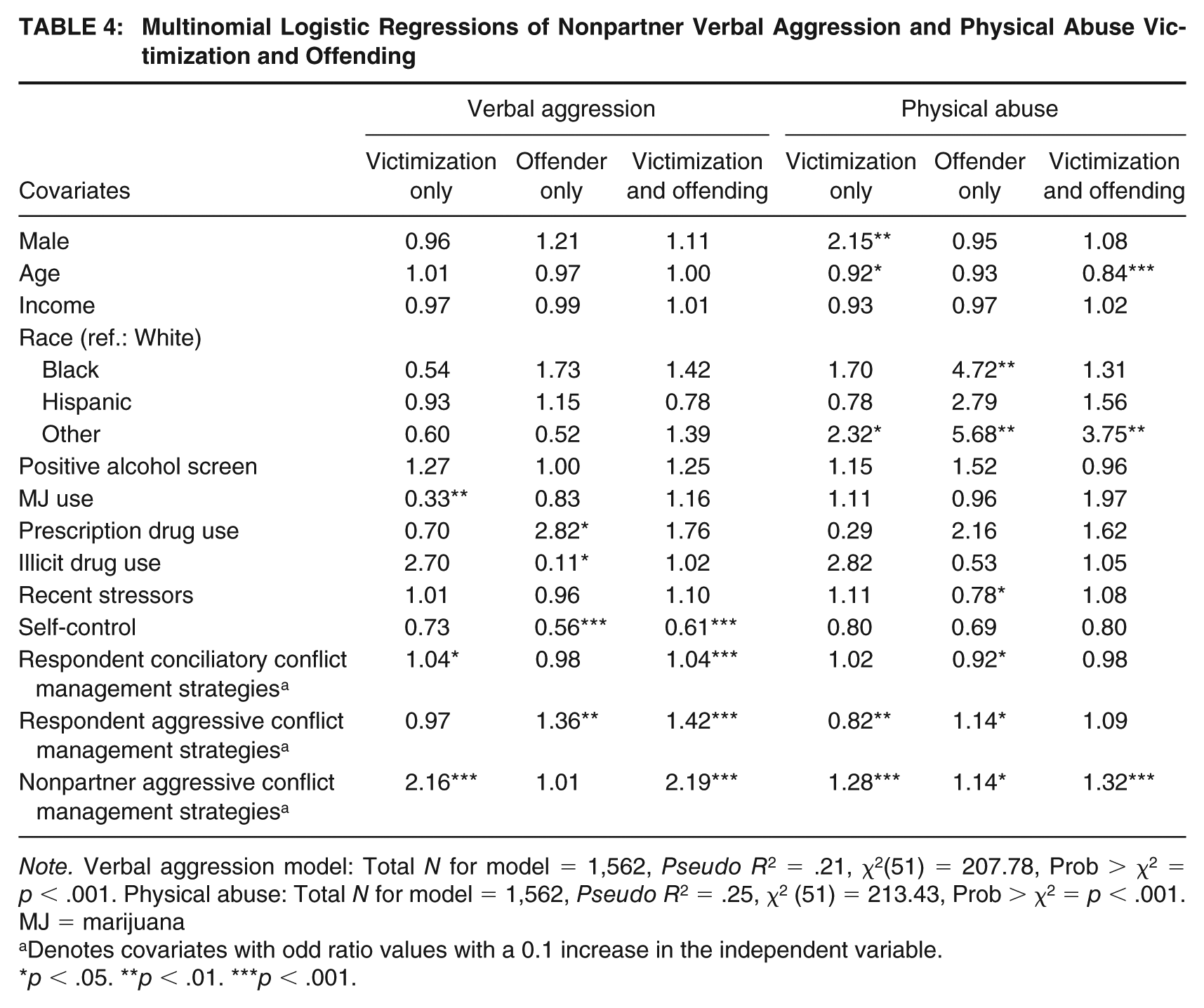
Note. Verbal aggression model: Total N for model = 1,562, Pseudo R2 = .21, χ2(51) = 207.78, Prob > χ2 = p < .001. Physical abuse: Total N for model = 1,562, Pseudo R2 = .25, χ2 (51) = 213.43, Prob > χ2 = p < .001. MJ = marijuana
Denotes covariates with odd ratio values with a 0.1 increase in the independent variable.
p < .05. **p < .01. ***p < .001.
For the IPV verbal aggression model (Table 3), those higher in self-control (for each one unit increase on self-control scale) were 0.45 times less likely to be in the verbal aggression victim–offender overlap group compared with the no aggression reference group. Those respondents who used conciliatory CMS with their partners were 1.03 times more likely to be in verbal aggression offending-only group compared with the no aggression reference group (and 1.09 times more likely to be in the victim–offender overlap group compared with the no aggression reference group). Those who used aggressive CMS with their partners had a 1.37 times greater likelihood of being in the verbal aggression victim–offender overlap group compared with the no aggression reference group. Those respondents’ partners who used aggressive CMS had a 1.53 times greater likelihood of being in the partner verbal aggression victimization-only group compared with the no aggression reference group. We observed only one significant demographic variable (biological sex). Being male had a medium-sized effect of increasing the likelihood of being in the partner verbal aggression victimization-only group by an odds ratio of 2.55 compared with the no aggression reference group and lowering the likelihood of being in the victim–offender overlap group by a small effect size, that is, odds ratio of 0.65 (offending-only group by a small effect size, that is, an odds ratio of 0.37). Marijuana use and illicit drug use were also statistically significant.
For the IPV physical abuse model (Table 3), those high in self-control were 0.42 times less likely to be in the victim–offender overlap physical abuse group compared with the no physical abuse group. Those respondents who used aggressive CMS had a 1.34 times greater likelihood of being in the physical abuse offending-only group compared with the no physical abuse reference group (and 1.14 times more likely to be in the victim–offender overlap group). Those respondents’ partners who used aggressive CMS had a 1.2 times greater likelihood of being in the partner physical abuse victimization-only group compared with the no physical abuse reference group (and 1.12 times more likely to be in the victim–offender overlap group). Males were 0.04 times less likely to be in the IPV physical abuse offending-only group compared with the reference group. We observed several other significant variables (age, income, and illicit drug use).
In Table 3, for the IPV sexual abuse multinomial logistic regression model, those who were high in self-control were 0.58 times less likely to be in the victim–offender overlap sexual abuse group and the offender-only group compared with the no sexual abuse reference group. Those respondents’ partners who used aggressive conflict management had a 1.14 times greater likelihood of being in the partner sexual abuse victims-only group compared with the no sexual abuse reference group. We also observed some other statistically significant variables (age, ethnicity, prescription drug use, illicit drug use, and life stressors).
Multivariable Models of Verbal Aggression and Physical Abuse within Nonpartners
In Table 4, for the nonpartner (friends and acquaintances/strangers) verbal aggression model, those who were high in self-control were 0.44 times less likely to be in the verbal aggression offending-only group compared with the no aggression reference group (and 0.39 times less likely to be in the victim–offender overlap group compared with the no aggression reference group). Those respondents who used conciliatory conflict management with their nonpartners were 1.04 times more likely to be in verbal aggression offending-only group and victim–offender overlap group compared with the no aggression reference group. Those who used aggressive conflict management with their nonpartners had a 1.36 times greater likelihood of being in the verbal aggression offending-only group compared with the no aggression reference group (and 1.42 times more likely to be in the victim–offender overlap group). Those respondents’ nonpartners who used aggressive conflict management had a 2.16 times greater likelihood of being in the partner verbal aggression victimization-only group compared with the no aggression reference group (and 2.19 times more likely to be in the victim–offender overlap group). We observed three other statistically significant variables (marijuana, prescription drugs, and illicit drugs).
For the nonpartner physical abuse model (Table 4), those respondents who used conciliatory conflict management tactics with their nonpartners were 0.08 times less likely to be in physical abuse offending-only group compared with the no physical abuse reference group. Those respondents who used aggressive conflict management with their nonpartners were 0.18 times less likely to be in the physical abuse victimization-only group compared with the no physical abuse reference group (and 1.14 times more likely to be in the offender-only physical abuse group). Those respondents’ nonpartners who used aggressive conflict management had a 1.28 times greater likelihood of being in the nonpartner physical abuse victimization-only group compared with the no physical abuse reference group (and 1.14 to be in the offender-only physical abuse group and 1.32 times more likely to be in the victim–offender overlap group). Being male had a medium-sized effect of increasing the likelihood of being in the nonpartner physical abuse victimization-only group by an odds ratio of 2.15 compared with the no aggression reference group. We observed several other significant variables—age, ethnicity, and the life stressors variable.
Discussion
The current study examined the overlap of victimization and offending among adult couples 18 to 32 years old using a nationally representative general population sample. First, we noted that our rates of aggression/abuse were fairly similar in general size to other national studies (Coker, Sanderson, Cantu, Huerta, & Fadden, 2008; Smith et al., 2016; Straus et al., 1996). For example, research covering the perpetration of verbal aggression has detected rates of 74% to 83% (Straus et al., 1996); iCOR results fall within that range with a rate of 77%.
We observed support for our first hypothesis that the prevalence of a victim–offender overlap would be high across measures of verbal aggression, physical abuse, and sexual abuse measures for both the young adults’ identified intimate partnership and their nonpartner relationships. Our results were consistent with earlier research identifying an overlap between victimization and offending in interpersonal relationships, including a local convenient sample of adults involved in the criminal justice system which covered general violence (Felson et al., 2018) or IPV specifically (Muftić et al., 2015), general population youth violence in sixth and seventh grades from a multicity study (Jennings et al., 2010), and a nationally representative sample of adolescents/young adults that covered IPV (Reingle et al., 2012; Tillyer & Wright, 2014). As predicted by our first hypothesis, descriptively we observed that the perpetration-only group represented a smaller percentage of cases than the victim–offender overlap group for all of our abuse/aggression measures. While descriptively we observed that the victim-only group represented a higher percentage of cases than the victim–offender overlap group for partner sexual abuse and partner physical abuse, we observed that the victim-only group represented a smaller percentage of cases than the victim–offender overlap group for verbal aggression (partner and nonpartner) and physical abuse (nonpartner). The current study provides additional evidence for a victim–offender overlap not only within a single type of relationship but also across relationships, for those young adults who were in intimate and nonintimate relationships.
Consistent with our second hypothesis, self-control and how the respondent and their partners and nonpartners manage conflict were our most consistent predictors of the victim–offender overlap (with generally small effect sizes, according to Cohen’s convention; Cohen, 1988). First, our measure of self-control was a significant protective factor for the victim–offender overlap in all of our models, except for physical abuse involving partners and nonpartners. Our work provides further support for Gottfredson and Hirschi’s (1990) self-control theory that those with lower self-control are at risk of becoming both an offender and a victim. Our results align with research on low self-control serving as a risk factor for the victim–offender overlap (Flexon et al., 2016; Jennings et al., 2010; Schreck, 1999) and being related to verbal aggression (partners and nonpartners) and sexual abuse with partners.
The key component of this study was examining the CMS of the study participants and exploring their link to the victim–offender overlap. We observed a fairly consistent association for our measures of aggressive CMS and the overlap, with some exceptions. For our nonpartner abuse measures, we observed when nonpartners use aggressive CMS toward the respondent, the respondents have a greater likelihood of being in the victim–offender overlap group for verbal aggression and physical abuse compared with the no aggression/abuse reference group. Similarly, respondents’ use of aggressive CMS against a nonpartner is associated with a greater likelihood of respondents themselves being in the victim–offender overlap group for verbal aggression compared with the no aggression reference group (but not physical abuse nonpartner overlap).
There was only partial support for this hypothesis using the partner abuse data and aggressive management tactics. When a partner uses aggressive CMS toward the study respondent, the respondent is more likely to be in the victim–offender overlap physical abuse group compared with the no abuse reference group (but not verbal aggression and sexual abuse overlap groups). Respondents’ use of aggressive CMS against a partner is associated with a greater likelihood of the respondent being in the victim–offender overlap group for verbal aggression and physical abuse (but not for sexual abuse) compared with the no aggression/abuse reference group.
These results suggest that where we find members of the general population in intimate relationships using aggressive CMS against a partner, or having these strategies used against them, we are generally likely to also find these same people as both victims and offenders of partner and nonpartner physical abuse and verbal aggression. While we reported some cross-situational consistency in the use of CMS and its effects on the victim–offender overlap for physical abuse and verbal aggression across interactions with partners and nonpartners, we did not see those same effects for sexual abuse within partnerships. This finding likely is predicated on the greater prevalence of unidirectional sexual abuse (three out of five respondents were solely victims of sexual abuse). However, more research is needed to better understand why aggressive CMS was not associated with the victim–offender overlap for partner sexual abuse. Perhaps sexual abuse involves substantially more dominant behavior by one person over another and less of the back-and-forth associated with verbal aggression and physical abuse (Kaukinen, Gover, & Hartman, 2012). For example, we did observe that a partner’s aggressive CMS did increase the likelihood of a sexual abuse “victimization-only” experience compared to the no aggression group for the respondent if their partner used such a strategy. It is not that aggressive management is not problematic in relation to sexual abuse, as it predicts sexual victimization by itself, it is just that it does not seem to be associated with the more limited number of cases of sexual abuse overlap. Rather than individual CMS, issues such as lower levels of self-control and drug use are stronger predictors of the sexual abuse victim–offender overlap.
Our data on conciliatory CMS and the victim–offender overlap are less intuitive. Those respondents who use conciliatory CMS are more likely to be in the victim–offender overlap group for partner verbal aggression and nonpartner verbal aggression (compared with the no aggression reference group) and had no effect on the victim–offender overlap for physical and sexual abuse. While we expected that being conciliatory would de-escalate a conflict, in the case of verbal aggression it seems to make the situation worse. Perhaps conciliatory CMS is seen as a thin veil for passive-aggressive behavior carried out by the offender and not taken as genuine or it is done by an offender because they know they did something wrong and want to try and improve their relationship. In some cases, the conciliatory strategy may be perceived as a sign of weakness that invites a more belligerent person to abuse the respondent. We need more research to better understand the mechanisms linking a seemingly helpful de-escalatory approach that nonetheless leads to iatrogenic findings related to the verbal aggression overlap.
There was some support for our third hypothesis that we would see similar significant sociodemographic factors and measures of substance use across the victims-only, offenders-only, and the victim–offender overlap groups. A number of the hypothesized correlates significantly predicted the victim–offender overlap, including: partner verbal aggression (biological sex and marijuana use), partner physical abuse (age and illicit drug use), partner sexual abuse (prescription drug use, illicit drug use, and recent life stressors), and nonpartner physical abuse (age and “other” race compared with White respondents). While gender has not been reported to be strongly associated with the IPV victim–offender overlap in some studies (Muftić et al., 2015; Reingle et al., 2012; Tillyer & Wright, 2014), we observed in our sample that males were less likely to be in the victim–offender overlap group and the offender group for verbal aggression in intimate relationships than females. Males also had an increased likelihood of being in the partner verbal aggression victim-only group compared with the reference group, with an odds ratio of 2.55 being one of our bigger effects in the medium-sized range. Similar outcomes emerged for males being more likely to be in the nonpartner physical abuse victim-only group and less likely to be in the IPV physical abuse offending-only group compared with the reference group.
Exploring gender within an IPV overlap study is important given the historically patriarchal nature of U.S. society, where women are typically less empowered financially and physically, with implications for relationship violence (A. G. Johnson, 2005). Also, many IPV studies only investigate male perpetrators or female victims (Tillyer & Wright, 2014). Our broader approach to sampling and measuring abuse showed that while both females and males are in the victim–offender overlap group, there were some important differences, with males less likely to be offenders of verbal aggression and physical abuse of their intimate partners. This gender result is consistent with other research that men are somewhat more likely to be victims of less serious forms of aggression than women. (Moffitt & Caspi, 1999; Straus, 2008). These results need to be further explored in future research, inclusive of measures of victim injuries and fear. Researchers should also explore the function of IPV in a relationship which might sometimes move beyond control/domination for some couples, as seen with male IPV against women.
The one significant result for biological sex and overlap will need to be explored in future research as it was nonsignificant for all of our other overlap measures. With only one significant finding on biological sex and the overlap, it is difficult to determine whether the results have strong implications. For example, we cannot assert support or nonsupport for feminist theories that suggest that IPV is an expression of male domination over women (Dobash, Dobash, Wilson, & Daly, 1992; Lawson, 2012), where we would thus expect little overlap between victimization and offending with women mostly being victims only and males being offenders.
Older participants are less likely to report being in the physical abuse victim–offender overlap group compared with the no abuse group, in nonpartner relationships. This finding is supported by the aging-out phenomenon of crime (Hirschi & Gottfredson, 1983), that people are less involved in crime as they get older. This protective effect of getting older was also apparent in terms of the risk of being in the victim–offender overlap group for IPV physical abuse and the risk of being in the offender-only group for IPV sexual abuse relative to the no abuse reference group.
Consistent with Reingle and colleagues (2012), illicit drug use, prescription drug misuse, and marijuana use were associated with selected victim–offender overlap outcomes in this study. As offenders are known to use drugs, it may be that misusing drugs may lower the presence of capable adult guardians and lead to victimization and offending (Reingle et al., 2012).
Limitations
The current study uses cross-sectional data. While this is a fairly common design among overlap studies, it is not possible to make temporal inferences with these data. For example, it is not clear whether the aggressive CMS caused the various forms of abuse we measured or was a consequence of the abuse. Next, as a household sample, iCOR does not include high-risk individuals or members of the military, and our results might look different if they were included. As with all self-report data, our respondents could suffer from recall and social desirability biases, although this form of online survey measurement is common in the social sciences and has been shown to generate reliable and valid estimates of risky behaviors (Thornberry & Krohn, 2000). Next, we assessed alcohol and drug use over the past 6 months before the survey and were not able to assess its use at the time of the abusive event(s). Therefore, it is unclear how event-specific substance use relates to our abuse outcomes and the overlap. The current study draws on the responses of a single reporter, which may mask different perspectives of the counterpart in a given conflict. We do not have measures of the amount of contact between the respondent and partners and nonpartners, although the extent of contact may be a correlate of aggressive behaviors. As with other IPV overlap studies that have used summed measures of physical abuse (Reingle et al., 2012; Tillyer & Wright, 2014), we treated different forms of abuse with an equal weight so that weapon use counted the same as slapping. In this article, punching a partner once in the last year is equal to punching once a week. Overlap researchers will need to explore additional measurement constructions for assessing frequency and intensity of abuse. Finally, we note that it was important to present all of the models across Tables 3 and 4, despite the possibility that the large number of tests may increase the chances of Type I error. However, the consistent findings on a number of significant predictors across models (e.g., CMS and self-control) indicate strong association between these factors and the victim–offender overlap.
Implications and Conclusions
Our results have a number of implications for victim services and prevention. First, many victim service providers are either not configured to address victims who are also offenders or explicitly exclude offenders from receiving victim services (Trulson, 2005). Some victims can also become ineligible for rights and services if their victimization resulted from participation in a criminal act (Trulson, 2005). Our results suggest that given the large prevalence of IPV and non-IPV victims who are also offenders and vice versa, victim service providers we will need to adjust their protocols to help this large subgroup of victims to make greater in-roads to preventing violence. Providers need to reconsider such blanket exclusions, acknowledging that victims sometimes present histories with offending and victimization (Muftić et al., 2015).
Next, many prevention programs, including evidence-based programs such as Shifting Boundaries to address IPV (Taylor, Stein, Mumford, & Woods, 2013) or Green Dot to reduce interpersonal violence in high schools (Coker et al., 2017), operate under the assumption that one group of people are the offenders and another group are the victims. Our results and other research suggest that a reorientation of these program curricula to acknowledge the likely overlap of victims and offenders could be beneficial. Also, we believe the curricula should include elements addressing aggressive CMS. While further research is necessary to understand the nuances of conciliatory approaches to conflict management, the evidence that young adults are not using conciliatory tactics effectively for the resolution of verbal conflicts—which are associated with escalation to violent encounters—presents an opportunity for early intervention. Prevention curricula should also build in teaching youth self-control. Gottfredson and Hirschi’s (1990) work suggests that self-control appears to be malleable in the early years but remains relatively stable after age 10 (Higgins, Jennings, Tewksbury, & Gibson, 2009). Other research shows that self-control is resistant to justice interventions after adolescence (Mitchell & MacKenzie, 2006). Thus, it is critical that interventions begin early in life (Jennings et al., 2010).
Criminal justice officials should begin to consider and respond to the risk factors that increase both victimization and perpetration and teach nonaggressive CMS in high-risk populations, incorporating substance use programming. Given the high prevalence for those in intimate relationships to use abuse not only against their partner but also with friends, acquaintances, and strangers, IPV interventions may need to work with IPV offenders not only on how they treat their partner(s) but people in general. While helping IPV victims, IPV prevention education could lead to a displacement of IPV crimes to nonpartner aggression and abuse.
In conclusion, we studied the IPV victim–offender overlap for young adults in intimate relationships, as done in previous research, and also investigated the same young adults’ interactions with friends and strangers, a distinction not seen in the published research. We observed a high degree of overlap between victimization and offending across verbal aggression and physical abuse for partners and nonpartners and overlap for sexual abuse. We also observed that victims and offenders share some similar characteristics. Our models revealed a range of consistent set of risk factors for the victim–offender overlap for partner abuse and nonpartner abuse. In particular, we observed a strong relationship between CMS and the overlap. Future research is needed to determine nuances of CMS and how different strategies are applied in high-risk populations (examining specific outcomes within varying local samples and contexts).
Footnotes
Authors’ Note:
This research was funded by the National Institute of Justice (Grant No. 2015-VF-GX-0110). Points of views in this document are those of the authors and do not necessarily represent the official position or policies of the U.S. Department of Justice or any other organization. We would like to thank Noelle Miesfeld and Ethan Rogers for significant contributions to designing the project survey.
Authors’ Contributions
B.T., E.A.M., W.L., and Berg jointly conceived the overall study, secured funding, and participated in its design and coordination. Bohri provided additional input to study coordination, data management, literature review, and drafting. Bohri and B.T. conducted the analyses. B.T. drafted the manuscript with substantive input to the design, interpretation, and results from E.A.M., Berg, and W.L. All authors read and approved the final manuscript.