
Abstract
Empirically supported risk factors are predictive of sexual re-offense regardless of whether individuals suffer from a major mental illness. A small subgroup of individuals with major mental illness may be more likely to demonstrate acute psychotic symptoms at the time of their sexual offending behavior (Smith & Taylor, 1999). This study reviewed archival data from a high-risk sample to identify 55 individuals with major mental illness who had committed a total of 176 sex offenses. The relationship between acute psychiatric symptoms and criminogenic needs was explored. Most sex offenses were not temporally related to acute psychiatric symptoms. The apparent effect of mental health symptoms on criminogenic factors over the individual’s life was rated. Where acute symptoms were associated with worsened criminogenic factors, this most often involved Grievance Thinking, Poor Emotional Control, and Poor Problem-Solving. Typologies emerged based on the pattern of criminogenic needs along with demographic and offense characteristics. Assessment and treatment implications are discussed.
In recent years, there has been a surge of research exploring the relationship between major mental illness (MMI) and violence. Much of this research has sought to examine whether certain MMI symptoms and diagnoses might be unique risk factors for violence. Some research has found a relationship between certain types of MMI symptoms and violence (e.g., threat control override symptoms; Link, Stueve, & Phelan, 1998; Swanson, Borum, Swartz, & Monahan, 1996). Keers, Ullrich, DeStavola, and Coid (2014) found that individuals who had never received treatment for schizophrenia were about 3 times more likely to engage in violence as compared to those without psychosis. This effect was related to the higher presence of persecutory delusions in this group than other MMI groups. A large longitudinal study of released Swedish prisoners found that schizophrenia spectrum disorders and bipolar disorder were associated with an increased hazard of violent reoffending in men even after age, immigration status, sociodemographic, and criminological variables were controlled (Chang, Larsson, Lichtenstein, & Fazel, 2015).
Other researchers have not found significant effects between factors unique to MMI and violence (Appelbaum, Robbins, & Monahan, 2000). Skeem and colleagues (2006) examined the acuity and temporal effect of MMI symptoms, including threat control override symptoms, on violent behaviors within a civilly committed psychiatric sample with histories of violence. Only symptoms of hostility were associated with increased violence. However, the results were likely tempered by the fact that patients with active delusions were specifically excluded from the study. Only 11% of the sample was diagnosed with psychotic spectrum disorders, and the sample had a low rate of previous psychiatric hospitalizations.
Utilizing the archival data from the MacArthur Violence Risk Assessment Study, Skeem, Kennealy, Monahan, Peterson, and Appelbaum (2016) found psychosis preceded 19.2% of the 182 violent incidents that occurred with the 56 individuals who experienced both psychosis and violence. However, only 8.9% exclusively demonstrated psychotic symptoms prior to each of their violent incidents. The majority (64.3%) of the cases did not exhibit psychosis at the time they engaged in violence. Peterson, Skeem, Kennealy, Bray, and Zvonkovic (2014) found that a majority of the crimes committed (64.7%) were not associated with mental illness symptoms. The authors reported that only 7.5% of the crimes were directly related to mental illness.
Overall, the available research has not demonstrated a clear link between MMI and violence. Although the rate of violence is reported to be higher when compared to general community samples, this difference appears better explained by factors that would be predictive of violence for individuals without MMI (e.g., personality disorders, substance use; Bonta, Blais, & Wilson, 2014; Douglas, Guy, & Hart, 2009; Monahan et al., 2001). Individuals with mental illness, especially women, are likely more at risk to be victims of violence than to perpetuate violence (Teplin, McClelland, Abram, & Weiner, 2005). Further research that explores the complexity of this relationship is needed. Meanwhile, professionals must balance the importance of communicating factual information to avoid fueling public misperceptions regarding the relationship between MMI and violence as well as the creation of emotionally reactive, stigmatizing policies (Appelbaum, 2006).
Sex Offending and MMI
Individuals with sex offense histories and MMI are doubly stigmatized, as these individuals are members of two highly marginalized social groups (Guidry & Saleh, 2004). This group represents only a small minority in both mental health and traditional sex offense treatment programs (Kelley & Thornton, 2015). This may account for the paucity of research in this area and raises the question regarding the extent to which traditional assessment and treatment approaches apply to such individuals.
Few studies have examined whether causal relationships exist between symptomatology and sexual offending for individuals with a history of sex offenses and major mental illness (SOMMI). Smith and Taylor (1999) completed an archival study of 84 patients with schizophrenia who had been hospitalized after committing a sex offense. They found the majority of these patients was psychotic at the time of the sex offense (n = 80), but most of the exhibited symptoms were not considered to be a causal factor. Of the 80 cases, some patients exhibited symptoms that had an indirect effect on the sex offense (i.e., 25% for delusions and 18% for hallucinations). Fewer manifested symptoms that were deemed to have a direct causal effect on the sex offense (i.e., 18% for delusions and 15% for hallucinations).
In a large sample of 1,215 individuals convicted of sex offenses, Långström, Sjöstedt, and Grann (2004) found that sexual recidivism was associated with psychosis, diagnosis of a psychiatric disorder, and with any inpatient care. A much stronger association was found with diagnosis of a substance use or personality disorder, however. In a study of California parolees, mental health concerns predicted recidivism even after controlling for homelessness, place of residence, and employment (Singer, Maguire, & Hurtz, 2013). Moulden, Chaimowitz, Mamak, and Hawes (2012) reported that psychosis, antisocial personality disorder, and paraphilic disorders each made significant, independent contributions to the prediction of sexual recidivism.
Criminogenic Needs and MMI
Research has more consistently demonstrated that risk factors, or criminogenic needs predictive of reoffending violently or sexually, in non-MMI populations are also empirically related to re-offense risk factors in MMI populations. Furthermore, these well-known risk factors tend to be more predictive of risk than the presence of factors unique to MMI. For example, treatment noncompliance, suicidal ideation, preoccupation with violence, impulsivity, hostility, and residing in neighborhoods with high crime rates tend to be predictive of violence regardless of the presence or absence of MMI (Monahan et al., 2001; Silver, Mulvey, & Monahan, 1999; Swanson et al., 2006). A meta-analysis by Bonta and colleagues (2014) found well-known criminogenic factors, such as procriminal attitudes, antisocial personality traits, and substance abuse, were more predictive of violence than the presence of psychosis in a mentally disordered offender population. This was found in general as well as among those determined to be Not Guilty by Reason of Insanity.
Criminal history has been found to be the best predictor for violence among both mentally disordered and non–mentally disordered offenders (Bonta, Law, & Hanson, 1998). Criminal history was also the best predictor for future arrests in an outpatient civil psychiatric sample, while psychotic symptoms have shown an inverse relationship with future arrests in some studies (Prins, Skeem, Mauro, & Link, 2015). Skeem, Winter, Kennealy, Louden, and Tatar (2014) found that MMI symptoms were not predictive of re-arrest in parolees, but did predict return to custody for technical violations. Skeem and colleagues (2014) also found individuals with MMI scored higher on formal measures of risk. For this sample, the Level of Service/Case Management Inventory (LS/CMI; Andrews, Bonta, & Wormith, 2004) appeared to be more effective at capturing the criminogenic needs associated with risk for re-offense. Additional variables that may be unique to MMI, such as medication noncompliance, did not increase the prediction of risk. Lee and Hanson (2016) found that the rate of sexual recidivism was significantly higher for individuals with psychiatric histories. However, this effect was not significant once static and dynamic risk factors (i.e., criminogenic factors) for sexual risk were controlled. Thus, those with psychiatric hospitalizations had more static and dynamic risk, resulting in higher rates of sexual recidivism.
Aims of the Current Study
We sought to explore whether and to what degree MMI may contribute to sex offending within a sample legally designated as high risk for sexually reoffending using archival records. As we used risk factors from the Structured Risk Assessment framework (Thornton, 2002), we used the language of the Structured Risk Assessment framework for referencing criminogenic needs. The Structured Risk Assessment framework theoretically understands criminogenic needs as long-term vulnerabilities (LTVs) to emphasize that individuals can learn to manage criminogenic needs, but that such risk factors do not disappear. For example, an individual who is sexually attracted to children may go months without exhibiting this LTV in a secure setting because stimuli that might trigger the LTV are less common and less intense in the controlled environment, and he is more easily able to regulate a weakly triggered LTV (e.g., he appropriately avoids television shows and catalogs featuring children; he is able to demonstrate the ability to suppress deviant arousal on penile plethysmograph testing). However, the LTV may re-emerge when he returns to the community and encounters children. The following were specific aims of the study:
To examine the proportion of sexual offenses where psychotic symptoms were proximal to the offenses or were deemed to have a direct or indirect influence on them in a high-risk SOMMI sample.
To examine the proportion of individuals in a high-risk SOMMI sample for whom specific LTVs existed prior to the onset of MMI symptoms, and the proportion of LTVs that were exacerbated when MMI symptoms were more acute.
To examine the extent to which an individual’s overall density of MMI symptoms related to the likelihood of having any sex offenses that were deemed influenced by MMI symptoms, and the number of LTVs that were exacerbated when MMI symptoms were more acute.
If the results supported the differentiation of a subgroup of SOMMI for whom MMI symptoms either exacerbate underlying criminogenic needs or influence their sexual offending through other routes, then we also aimed to explore whether demographic and offense characteristics could help to differentiate these individuals.
Method
This study is based on an archival record review of case files available at Sand Ridge Secure Treatment Center. No contact with participants was made. Approval of the study was obtained through the Institutional Review Board at Sand Ridge.
Participants
The sample consisted of 55 adult males ranged in age from 30 to 78 years (M = 50.75, SD = 10.07) who were referred for civil commitment consideration under Wisconsin’s statutory criteria for sexually violent persons (SVP) and residing at Sand Ridge. The majority of the sample had been committed pursuant to SVP (90.9%). The legal status of others included probable cause for commitment (7.3%) and discharged (1.8%). The data for the one case that had been discharged only included relevant information prior to, or during, his time while committed at Sand Ridge. Actuarially, the sample was Above Average Risk for re-offense as measured by the Static-99R (M = 5.44, SD = 1.85).
The majority of the sample was charged with serious sexual offenses, which is expected given the statutory criteria for civil commitment. We collapsed the offense charges into the following categories: (a) sexual offenses involving substantial force/restriction of liberty (e.g., kidnapping, use of weapon in commission of offense, endangering safety), (b) sexual offenses involving attempted or completed penetration (e.g., rape, first- through third-degree sexual assault, sexual intercourse with a child), (c) offenses involving attempted or completed sexual contact without force or penetration (e.g., fourth-degree sexual assault, child enticement, indecent behavior with a minor), (d) noncontact sexual offenses (e.g., exposure), (e) cooperative but illegal sexual offenses (e.g., statutory offenses, fornication), and (f) an “other” category (e.g., court deferments, institutional sanctions, unknown charges). Out of the 176 coded sexual offenses, 13.1% involved substantial force/restriction of liberty, 56.3% involved sexual offenses with attempted or completed penetration, 13.6% involved attempted or completed sexual contact without force or penetration, 6.3% involved noncontact sexual offenses, 0.7% involved cooperative, but illegal sexual offenses, and 10.2% were placed in the “other” category. Individuals could have been charged with more sexual offenses than the four that were coded.
Sample selection was based on a qualifying MMI diagnosis made by the most recent SVP evaluator or a treating psychiatrist. Qualifying diagnoses for study inclusion were schizophrenia (34.5%), schizoaffective disorder (30.9%), other psychotic spectrum disorders (25.5%), and bipolar I disorder (7.3%). Bipolar II disorder was not included because it does not involve psychosis or mania and does not typically necessitate psychiatric hospitalizations. Co-morbid diagnoses of paraphilias and personality disorders included pedophilic disorder (47.3%), other specified paraphilic disorder (23.6%), sexual sadism disorder (5.5%), antisocial personality disorder (50.9%), and other specified personality disorder (23.6%).
The age of MMI onset (M = 23.74, SD = 8.54, Mdn = 19.50) typically coincided with age at first psychiatric hospitalization (M = 21.40, SD = 7.24, Mdn = 22.00), which included only psychiatric units within hospitals or forensic settings, but not secure forensic treatment centers whose purpose was other than psychiatric stabilization. The sample had an average of 6.49 psychiatric hospitalizations prior to arrival at Sand Ridge (SD = 9.30, Mdn = 4.00, range = 0-60).
Most of the sample had experienced at least one consenting sexual experience in the community (81.8%); however, only 30.9% had prior stable intimate relationships. A minority had a history of live-in relationships lasting at least 2 years (18.2%), and 40% had engaged in problematic sexual behavior prior to the age of 13. The prevalence of problematic sexual behavior increased during adolescence (65.5%). Most of the sample began nonsexual and sexual criminal behavior during their late adolescence, with an average age at first arrest for any criminal offense of 17.00 (SD = 7.44) and age at first sex offense of 17.40 (SD = 6.23). Prior to arrival at Sand Ridge, the sample had been charged an average of 7.89 times for nonsexual offenses (SD = 5.83, Mdn = 8.00), 4.47 times for contact sexual offense offenses (SD = 2.34, Mdn = 4.00), and 1.56 times for noncontact sexual offenses (SD = 2.94, Mdn = 0).
Measures and Procedure
SOMMI Data Collection Form
The SOMMI data collection form was created to provide structure and coding rules for identifying relevant information from the archival records. It was created as a Microsoft Excel–based spreadsheet with definitions, directions, and examples for more complicated variables. The spreadsheet is separated into four areas including (a) demographic data, (b) psychiatric history, (c) offense pathways, and (d) LTV and MMI. The SOMMI Data Collection form utilizes drop-down menus with a selection of possible answer choices. Most fields used data validation to increase accuracy, but there were also open text fields to allow coders to provide a rationale or file source for later consensus scoring.
The first two sections of the SOMMI data collection form were straightforward. The demographic section collected data such as age at rating, relationship status, and basic offense information. The psychiatric history section covered hospitalizations, age of MMI onset, diagnoses, medications, and symptom history. The third section, offense pathways, required coders to respond to 14 items about each sex offense, such as relationship to victim, victim age and gender, symptoms at the time of offense, and severity of physical injury involved. Seven items were based on the violence coding guide for instrumental and hostile-reactive incidents developed for prior research (Cornell et al., 1996). Some of these items were modified to work better with the current population. We also adapted the coding instructions for one item, effect of psychiatric symptom on sex offense, from Smith and Taylor (1999). Additional items were created by the authors. The earliest and most recent sex offenses were coded, as were up to two additional offenses for which the most information was available in the archival record. If a case only had four or fewer sex offenses on record, all recorded offenses were coded. A full description of the variables coded for this offense pathway section is available as Online Supplemental Material (in the online version of this article).
The fourth section, LTV and MMI, identified the overall relevance of nine LTVs to the individuals’ sexual offense histories. The LTVs included Sexual Preoccupation, Offense-Related Sexual Interests, Difficulty Forming or Sustaining Romantic Relationships With an Adult, Emotional Congruence With Children, Grievance Thinking, Poor Empathy, Oppositional Reactions to Rules or Supervision, Poor Emotional Control, and Poor Problem-Solving. These LTVs were selected from 17 LTVs identified in the original Structured Risk Assessment tool. The original Structured Risk Assessment tool is a Structured Professional Judgment instrument designed to assess the relevance of LTVs for making risk management and treatment needs decisions. Selection of the nine items coded for this study was based on information available in file records, a desire to include LTVs from most of the Structured Risk Assessment domains, and our professional opinions regarding LTVs most likely to be impacted by the presence of MMI.
Coders first rated whether each LTV was present for a specific case, regardless of any potential impact by MMI. LTVs identified as being clearly relevant for a case were then rated with respect to whether the LTV preexisted the onset of MMI. Coders also rated how the presence or operation of the LTV was affected when the individual psychiatrically decompensated (i.e., whether acute MMI symptoms had exacerbating, mitigating, or no effect on the identified risk factor). For example, sexual preoccupation may be exacerbated by increased symptoms of mania, but mitigated by the presence of catatonia.
Symptom Density Rating Scales
We created two symptom density scales to examine whether the density of MMI symptoms was related to their influence on sex offending. Similar symptom scales have been created to explore the relationship between MMI and re-arrest (e.g., Prins et al., 2015). In the psychiatric history section, coders indicated whether each of nine psychotic symptoms were ever present in an individual’s history. The symptoms (and sample prevalence) included command auditory hallucinations (49.1%), auditory hallucinations without commands (78.2%), visual hallucinations (45.5%), grandiose delusions (45.5%), paranoid delusions (74.5%), somatic delusions (21.8%), erotomanic delusions (16.4%), jealous delusions (7.3%), and other types of delusions (20.0%). Each symptom was coded as present (1) or absent (0), resulting in a total score ranging from 0 to 9. Internal scale consistency was limited, α = .68. We found that internal consistency increased when two items were dropped: jealous delusions and other types of delusions. The revised total score ranged from 0 to 7 and demonstrated acceptable internal consistency, α = .77. Thus, we retained the second version and named the scale the Hallucinations and Delusions (HALDEL) Rating Scale.
The second symptom density scale was developed to describe the density of manic symptoms associated with schizoaffective and bipolar I. Again, coders indicated whether each of eight manic symptoms were present at any point in an individual’s history. These symptoms (and sample prevalence) included inflated self-esteem/grandiosity (50.9%), decreased need for sleep (41.8%), talkative/pressured speech (41.8%), flight of ideas/racing thoughts (38.2%), distractibility (61.8%), increased goal-directed activity (23.6%), excessive involvement in pleasurable activities (47.3%), and other manic symptoms (23.6%). Coded ratings produced a total score from 0 to 8 with good internal consistency, α = .81. We found that the internal consistency was improved when the item, other manic symptoms, was dropped, α = .82. Thus, the final scale was limited to seven items with a maximum possible total score of 7. We named this second scale the MANIA Rating Scale. The two scales were not correlated with one another, r = −.07, p = ns.
Data Collection
Archival file review was used to code information into the SOMMI data collection tool. The following information was generally available in the case file: police reports, criminal complaints, presentencing investigation reports, psychiatry reports, hospital admission and discharge summaries, and psychological evaluation reports. We also used Competency to Stand Trial and Criminal Responsibility reports when available. Coding each case typically required 4 to 8 hours to review available records and complete the data collection form. Data collection occurred between 2015 and 2017.
Training and Reliability
Three coders completed data entry for this study. Coders were licensed psychologists with primary employment completing SVP evaluations and prior experience assessing and treating individuals with MMI within psychiatric hospitals. A half-day training was provided regarding the SOMMI data collection tool, and coders completed a practice case for calibration purposes. Coder feedback identified weaknesses in the data collection processes, which were addressed by providing more detailed coding instructions.
Thirty of the 55 cases were randomly assigned to be independently coded by the second coder to assess inter-rater reliability. Items of interest for assessing reliability were unable to be coded for one case, leaving a total of 29 analyzable cases. Each of the three coders received about the same number of cases to code. Where variables had been coded by two raters, ratings from the primary rater were used in subsequent analyses, and ratings by the second coder were used only to assess inter-rater reliability.
Variables selected for inter-rater reliability analyses were those associated with the primary study aims (i.e., the influence of MMI on sex offending) and the use of structured clinical judgment in the coding. These include the effect of MMI on the sex offenses (i.e., direct, indirect, or either), primary motivation for sex offenses (i.e., MMI, disinhibited, deviant arousal, or general criminality), presence or absence of LTVs, existence of LTVs prior to MMI onset, and the impact of MMI on LTVs. Each variable was qualitatively coded, and features/symptoms coded as present or absent during a sexual offense were coded 1 (present) or 0 (absent).
Kappa coefficients were used to assess inter-rater reliability. Kappa measures inter-rater agreement corrected for the level of agreement expected simply by chance, and can be expressed as

Kappa can be interpreted as follows: <.20 = unacceptable; .20 to .39 = questionable; .40 to .59 = good; .60 to .79 = very good; and >.79 = almost perfect (Regier et al., 2013).
As described, some variables were coded at the level of the individual offense and, in the results section, descriptive information is provided at this level. However, we also transformed these offense-level variables into person-level variables for many of our analyses. For example, while individual offenses were coded according to whether the rater deemed that MMI symptoms had a direct effect on the offense occurring, we then created a corresponding person-level variable based on whether MMI symptoms had been rated as having a direct effect on any of the sex offenses coded for that individual. Inter-rater reliability for these person-level variables was as follows. Coders demonstrated very good agreement in determining whether or not MMI symptoms had some influence on any of the individual’s sex offenses (kappa = .79, p < .001). They demonstrated better agreement determining whether or not MMI symptoms had a direct effect on any of the individual’s sex offenses (kappa = .59, p = .002) rather than indirect influence (kappa = .31, p = .086). In judging the primary motivation for the sex offenses, coders most often agreed when MMI was identified as having a causal effect (kappa = .72, p < .001) and when a deviant arousal pattern was deemed to be present (kappa = .66, p < .001). Questionable reliability was found when the primary motivation for an offense was identified as due to disinhibition (kappa = .24, p = .046) and general criminality (kappa = .25, p = .170).
Ratings related to LTVs were made at the person level, not at the level of the individual offense, but they were made separately for each of the LTVs. Summary scores were then created by summing ratings across LTVs. For example, the number of LTVs rated as present was determined (PRESENCE-LTV), as was the number of LTVs that preexisted MMI (PRE-LTV), and the number of LTVs that were exacerbated by MMI (IMPACT-LTV). An intraclass correlation coefficient (ICC) for single measures was used to determine inter-rater reliability. Coders had moderate agreement for PRE-LTV (ICC = 0.68, p < .001) and IMPACT-LTV (ICC = 0.69, p < .001). Inter-rater reliability could not be determined for PRESENCE-LTV owing to lack of variance. Essentially, raters agreed that some LTVs were present for almost all cases while one LTV was generally rated as absent. However, coders substantially agreed with one another regarding whether there was clear evidence of the presence of the following LTVs: Sexual Preoccupation (89.7% agreement), Offense-Related Sexual Interests (93.1% agreement), Difficulty With Romantic Relationships (93.1% agreement), Emotional Congruence With Children (86.2% agreement), Grievance Thinking (86.2% agreement), Poor Empathy (79.3% agreement), Opposition to Rules and Supervision (79.3% agreement), Poor Emotional Control (86.2% agreement), and Poor Problem-Solving (100% agreement). Accordingly, PRESENCE-LTV was not used in the analyses.
Analytic Strategy
Analyses focused on testing the hypothesis that a portion of this sample of SOMMI could be identified for whom their MMI symptoms either exacerbate underlying criminogenic needs or (more rarely) influence their sexual offending through other routes (e.g., command hallucinations). One set of analyses were at the level of the offense, with three offenses analyzed for each individual. Descriptive statistics are presented showing the percentages of offenses with features relevant to this hypothesis including the frequency with which offenses were rated as being influenced (directly or indirectly) by MMI symptoms. We did not use inferential statistics to compare differences between offenses in these features as we had no a priori hypothesis. The second set of analyses focused on differences between individuals. While these included descriptive statistics (percentages, means, standard deviations), correlations, cross-tabulations, and associated tests of statistical significance were used to explore associations between variables or differences between groups. Where a continuous variable had been broken down into categories, we used the linear component of chi-square to test relationships with other variables. All analyses were carried out with IBM SPSS Statistics Version 25.
Results
Sex Offense Characteristics
Eighty percent of the sample had at least three sexual offenses for which the available records were sufficient to identify the characteristics involved. There were 25 cases (45.5%) with four or more sexual offenses resulting in a total of 176 coded sex offenses. When reporting frequencies for offense characteristics, only the first three sexual offenses were reported as fewer than half the sample had four. This resulted in a total of 151 sex offenses. As shown in Table 1, stranger victims were more common in the first and second offense but having specific and close victims became more common by the third offense. The first offense included near equal proportions of prepubescent, pubescent, and adult victims. Having a pubescent victim became less common while having an adult victim became more common during later offenses. Approximately, a third of the sample had prepubescent victims for all three offenses. While few sex offenses were committed when the subject was using other drugs, alcohol use was involved in approximately half of the sex offenses. Overall, alcohol use decreased at the time of the third sexual offense, but this appeared limited to those who minimally drank at the time of past sex offenses. Approximately half of the sex offenses involved some sort of planning, although when planning was present, it tended to be minimal. Violence or assaultive behavior causing the victim physical injury was not evident in the majority of the sex offenses. When force was used, it was an instrumental effort to obtain victim compliance as opposed to losing emotional control or reacting to arousal to the use of aggression.
Frequency of Characteristics Within First Three Sex Offenses
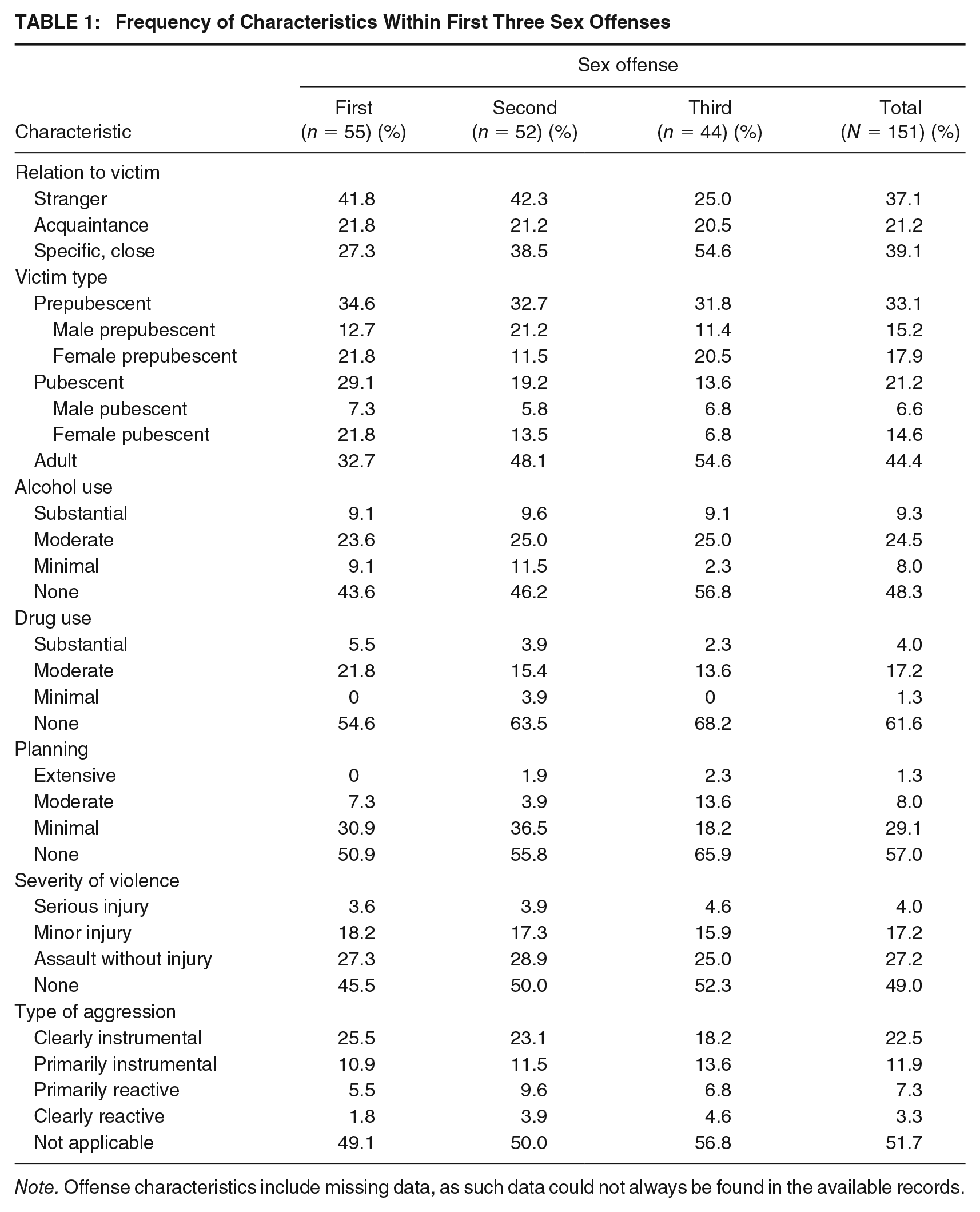
Note. Offense characteristics include missing data, as such data could not always be found in the available records.
Relationship Between Symptoms and Sex Offenses (Aim #1)
To address potential influence of MMI symptoms on sex offending behavior, we examined the extent to which specific features unique to MMI were present during the sex offenses. Features included psychosis at or near sex offenses, mania at or near sex offenses, compliance with psychiatric medication, effect of psychiatric symptoms on sex offenses, and motivation for sex offenses. The results can be found in Table 2.
Frequency of Symptoms Within First Three Sex Offenses
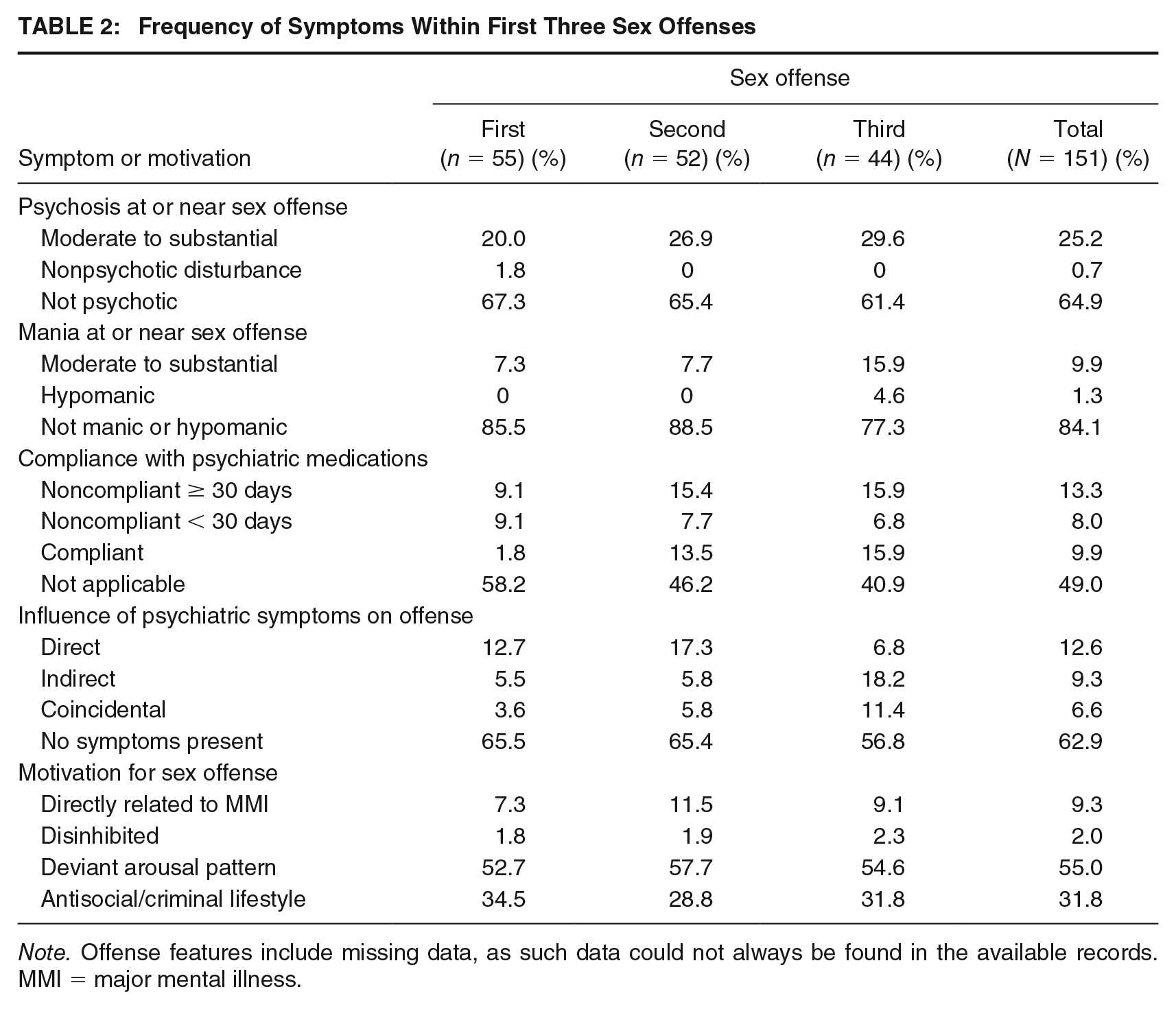
Note. Offense features include missing data, as such data could not always be found in the available records. MMI = major mental illness.
The majority of individuals were not psychotic or manic at the time of their offenses. When psychiatric symptoms were present, coders judged them to have more of a direct effect on the sex offending behavior during the first two offenses than on the third. Overall, direct effects were present in 12.6% of offenses, indirect effects in 9.3% of offenses, and coincidental symptoms in 6.6% of offenses. The majority of the sex offenses appear to be primarily related to individuals’ deviant arousal patterns. It should be noted that when coders identified deviant arousal pattern as the primary motivation for an offense, it did not preclude secondary motivators, such as general criminality, from also being present. The second most frequently identified motivator for sex offenses included antisocial attitudes/general criminality (in the absence of notable paraphilia).
The relationship between symptom density and direct influence of MMI symptoms on sex offenses was also examined. The HALDEL symptom density score was significantly correlated with determinations that MMI symptoms had a direct effect (r = .47, p < .001), but not with symptoms having an indirect effect (r = .24, p = .097). The MANIA density score demonstrated the opposite pattern; it was not correlated with determinations that MMI symptoms had direct effects (r = −.06, p = .690), but it was significantly correlated with judgments that MMI symptoms had indirect effects (r = .40, p = .007).
Relationship Between MMI and LTVs (Aim #2)
The prevalence of each LTV within the sample, whether they were present prior to the onset of MMI, and whether they were affected by MMI is provided in Table 3. Most LTVs were rated as having been present in the current sample. Specifically, eight of the nine LTVs were relevant for 67.3% to 98.2% of the sample. The exception, Emotional Congruence With Children, was rated as present in only 16.4% of the sample. Among individuals identified with a particular LTV, the majority were rated as clearly having the LTV prior to the onset of MMI. Very few LTVs were mitigated by the presence of MMI symptoms, and when it did occur, it was uncommon. Some LTVs were not affected by the presence of acute MMI symptoms; however, exacerbation of LTVs by MMI symptoms was not uncommon. The most commonly affected LTVs included Grievance Thinking, Poor Emotional Control, and Poor Problem-Solving.
Frequency of LTVs and MMI Effect (N = 55)
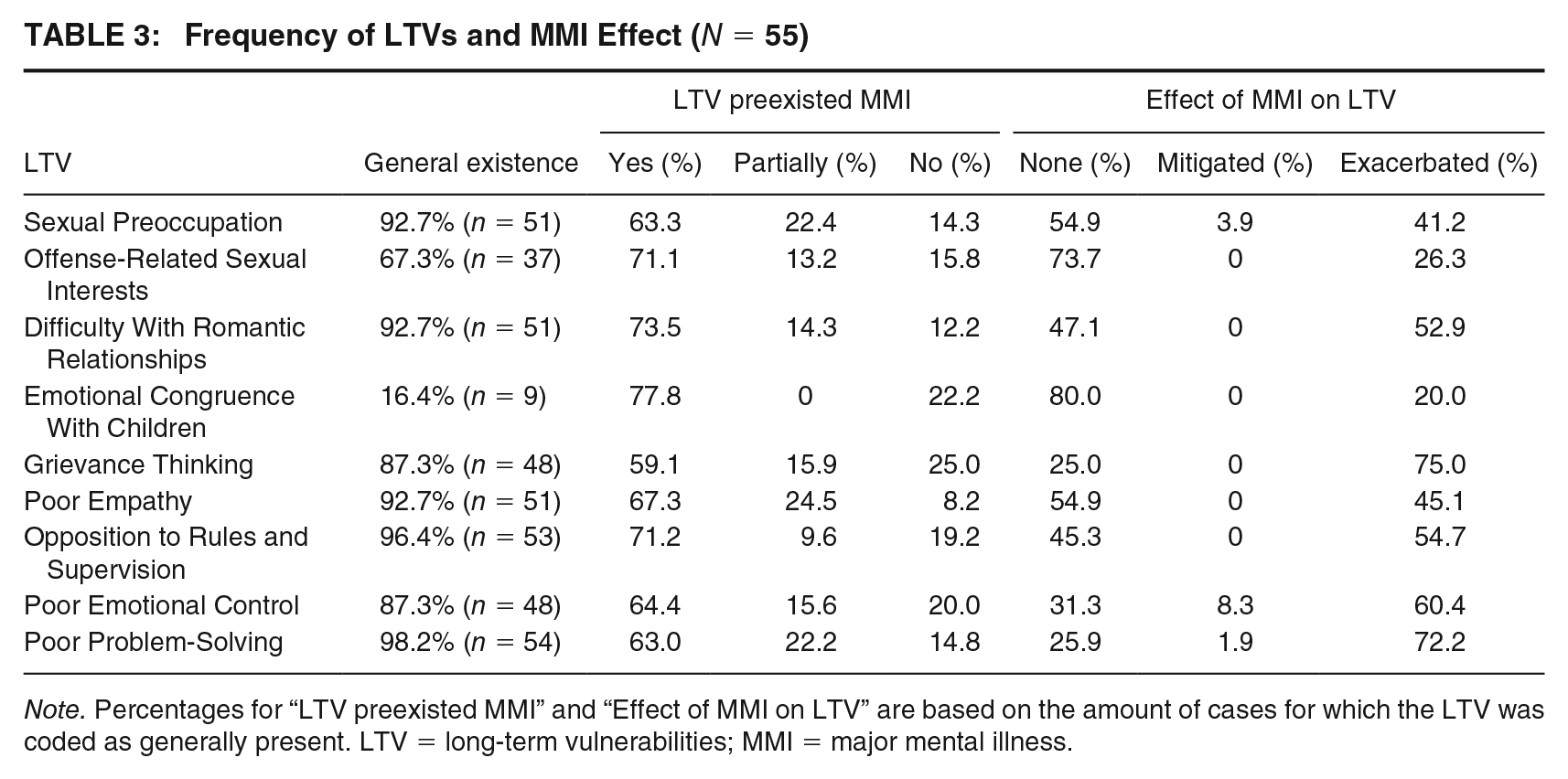
Note. Percentages for “LTV preexisted MMI” and “Effect of MMI on LTV” are based on the amount of cases for which the LTV was coded as generally present. LTV = long-term vulnerabilities; MMI = major mental illness.
Relationship Between Symptom Density, LTVs, and Sex Offenses (Aim #3)
The mean score on IMPACT-LTV was 3.93 (SD = 2.76), indicating that in this sample, on average, about four LTVs were rated as exacerbated by acute MMI symptoms. Density of symptoms was related to IMPACT-LTV. Specifically, there was a significant correlation with the HALDEL scale (r = .53, p < .001, n = 50), but not the MANIA scale (r = .23, p = .132, n = 46). The correlations between each of the exacerbated LTVs and the symptom density scales are provided in Table 4. Overall, eight of the nine exacerbated LTVs were significantly correlated with density of symptoms on the HALDEL scale. Emotional Congruence With Children was not correlated with the HALDEL scale but was significantly correlated with the MANIA scale. There were only 10 cases relevant for Emotional Congruence With Children limiting further conclusions about this result.
Correlations Between MMI Density and LTVs Exacerbated by MMI (N = 55)
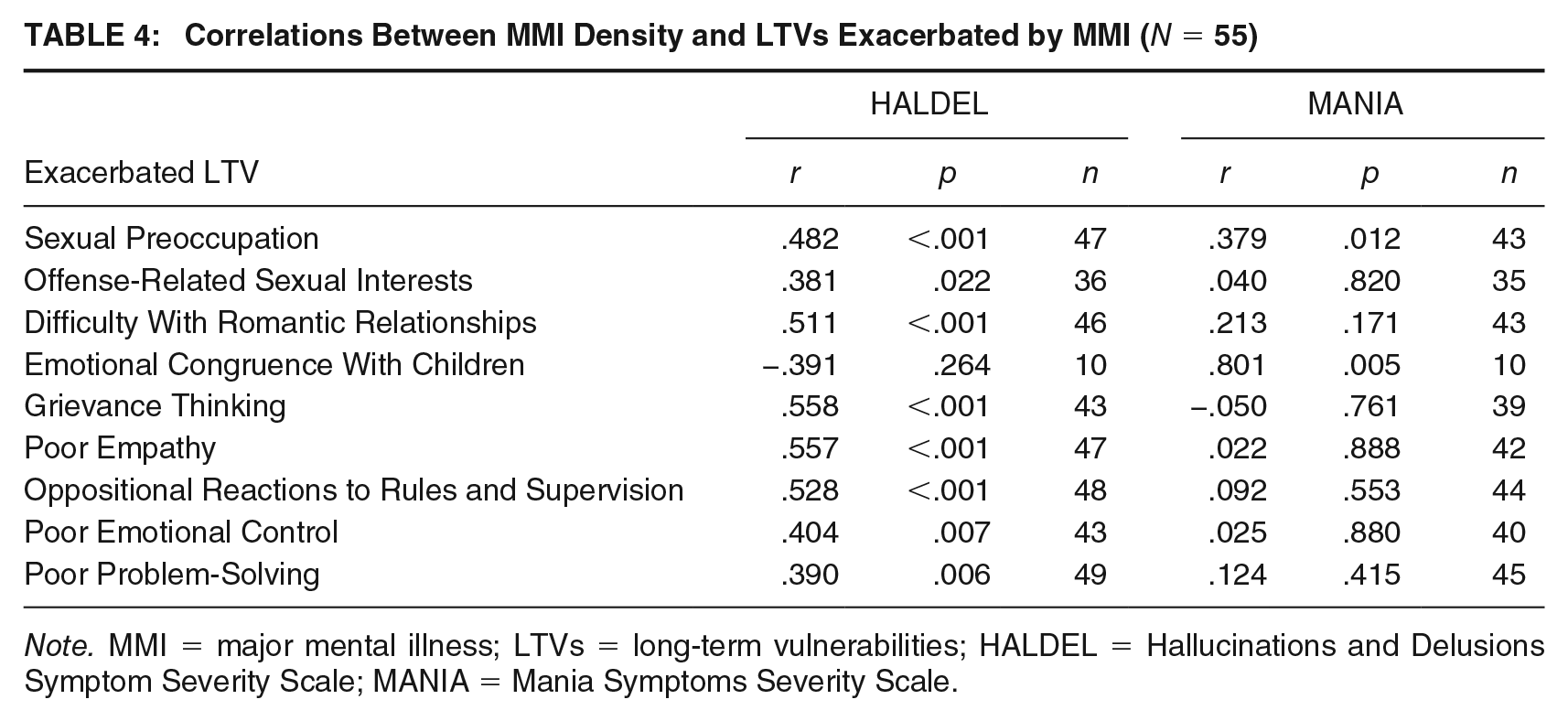
Note. MMI = major mental illness; LTVs = long-term vulnerabilities; HALDEL = Hallucinations and Delusions Symptom Severity Scale; MANIA = Mania Symptoms Severity Scale.
The sample (N = 55) was sorted into four categories based on IMPACT-LTV scores that represented how many LTVs were exacerbated by the presence of acute MMI symptoms: zero LTVs/none (21.8%), one to three LTVs/mild (18.2%), four to five LTVs/moderate (25.5%), and six to nine LTVs/high (34.5%). Linear-by-Linear Association Tests analyzed associations between characteristics in the sample’s early history and these LTV exacerbation categories (none, mild, moderate, or high). As can be seen in Table 5, these exacerbation categories were unrelated to onset of problematic sexual behavior before the age of 13, but were related to problematic sexual behavior emerging in adolescence and number of previous psychiatric hospitalizations. Specifically, those with zero to one prior hospitalization had fewer LTVs identified as being affected by MMI symptoms, whereas repeated psychiatric hospitalizations were associated with more LTVs affected by MMI symptoms.
Linear-by-Linear Association Test Results of LTVs Exacerbated by MMI, Sample, and Offense Characteristics
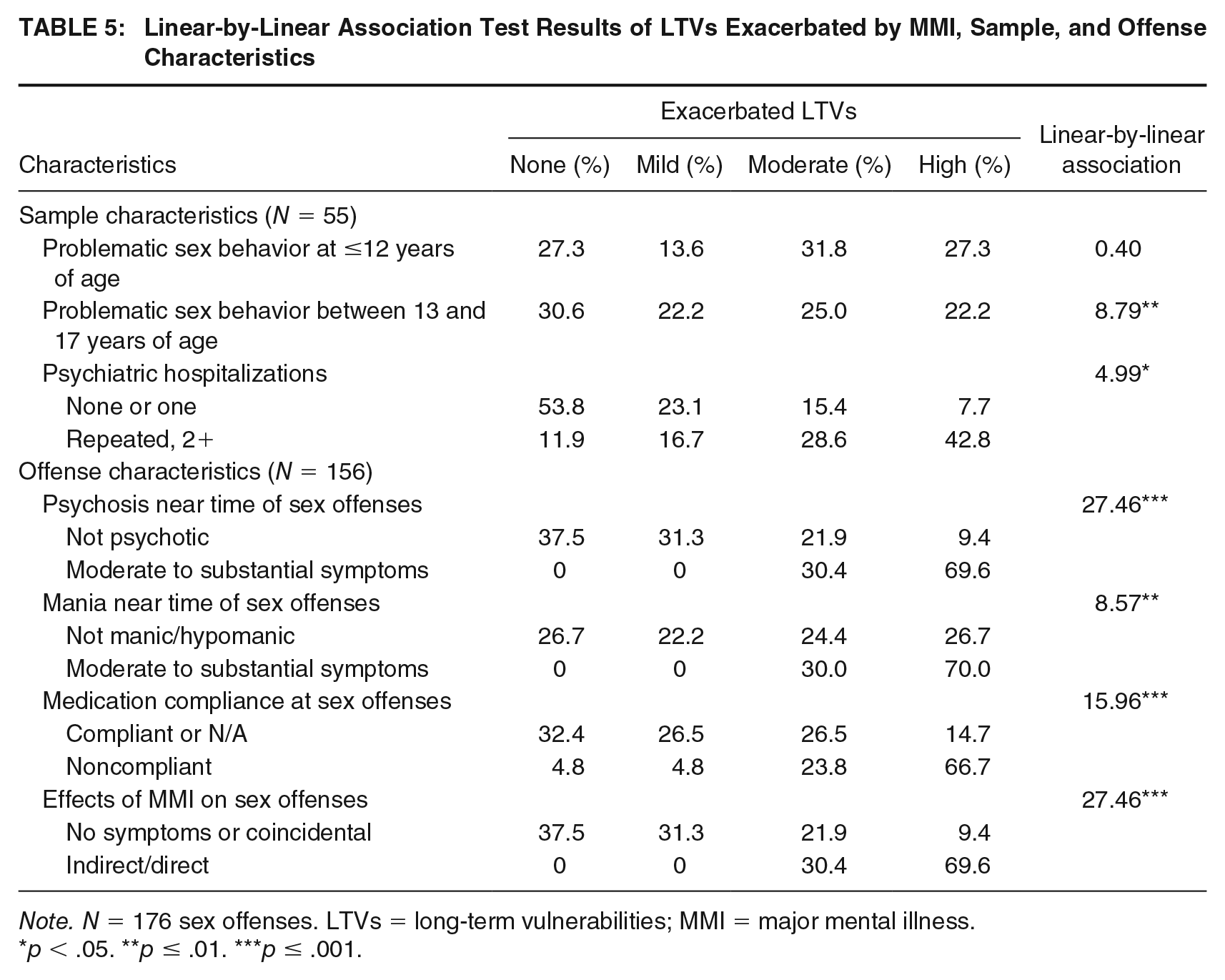
Note. N = 176 sex offenses. LTVs = long-term vulnerabilities; MMI = major mental illness.
p < .05. **p ≤ .01. ***p ≤ .001.
As noted in Table 5, Linear-by-Linear Association Tests were also used to analyze associations between sex offense characteristics and exacerbation category. For these analyses, the offense-level variables were combined at the person level to represent the most severe form present in any offense. For example, the psychotic symptoms present at or near the time of an offense were coded at the person level as were psychotic symptoms present at or near the time of any offense.
Having more LTVs rated as exacerbated by acute MMI symptoms was associated with raters attributing a number of features relevant to the influence of symptoms on offending. It was associated with having psychotic and, to a lesser extent, manic symptoms present at or near the time of sexual offenses. It was also associated with medication noncompliance at the time of sexual offenses, and with raters indicating that MMI symptoms had an effect (especially a direct effect) on offending.
Differentiation of SOMMI Subgroups (Aim #4)
An initial review of the Linear-by-Linear Association Tests presented in Table 5 indicated a relationship between number of psychiatric hospitalizations, effects of MMI on sex offenses, MMI symptoms and medication compliance at the time of sex offenses, and whether LTVs tend to be exacerbated by MMI. To explore the plausibility of the hypothesized subgroups within the current SOMMI sample, we created three dichotomous variables to capture the following: (a) repeated psychiatric hospitalizations (2+) versus none or one, (b) direct and indirect influence of MMI symptoms on sex offenses versus coincidental or no MMI symptoms, and (c) a moderate to high number of LTVs being rated as exacerbated by MMI symptoms versus none or few. These three groups were significantly associated with each other, that is, psychiatric hospitalizations and exacerbated LTVs, χ2(1) = 9.67, p = .002; influence of MMI and exacerbated LTVs, χ2(1) = 22.65, p < .001; and psychiatric hospitalizations and influence of MMI, χ2(1) = 6.71, p = .01. These variables were then combined to create a prototype score based on how many of these variables applied to the cases ranging from zero to three. Overall, one or none of the three variables applied to 43.6% of the sample, whereas two or three of the variables applied to 56.4% of the sample.
Discussion
Findings obtained in this study were broadly supportive of the hypothesis that the SOMMI population can be divided into two prototypical groups. MMI symptomatology and criminogenic needs operate largely independently in one group while, in the other prototypical group, variation in the acuity of MMI symptoms is associated with an increase in risk-related functioning. Evidence for a group for whom MMI symptomatology and criminogenic needs operate largely independently includes the following: (a) For about 8 in 10 sexual offenses, raters identified no direct or indirect effect of MMI symptoms on the offense; (b) for over 6 in 10 sexual offenses, raters determined the individual was not psychotic at the time of the offense; and (c) for about 4 in 10 of the sample, few LTVs were rated as exacerbated by MMI symptoms.
There was also evidence that, for some individuals, variation in the acuity of MMI symptoms is associated with an increase in risk-related functioning. This included (a) raters agreed with reasonable reliability that some participants (about 2 in 10) experienced MMI symptoms that directly or indirectly increased their risk; (b) raters agreed with reasonable reliability that for some participants (about 6 in 10), when their MMI symptoms were more acute, a broad range of LTVs were exacerbated; (c) these two ratings correlated with each other such that if raters saw MMI symptoms as influencing offending, they tended to also see them as exacerbating LTVs; and (d) both these ratings were also associated with the medication noncompliance and acute psychotic symptoms being temporally proximate to offenses.
It is important to recognize that, although these results are consistent with and supportive of our hypothesis, they do not prove that MMI symptoms are exercising the postulated causal influence. Proving causality is hard even when the proposed causal factor can be experimentally varied (how do you know you only varied the factor of interest) and is essentially impossible in an archival study of the present kind. Given that limitation, it is worth considering potential counter-hypotheses that might explain the results. One possibility is that the intra-individual temporal correlation between MMI symptoms and LTV exacerbation being described by raters reflects temporal variation in the third variable. Evidence against this possibility is that raters actively searched for coincidental presence of MMI symptoms and offending but generally did not find this. Nevertheless, it cannot be ruled out. A possibility would be that environmental factors, including stressful events (e.g., increased conflict with family members/authority figures and reduced supervision) impaired both regulation of MMI symptoms and also activated LTVs.
This would be an important variant of our basic hypothesis, but even under this interpretation, this would imply the existence of a subgroup that shows a distinctive and marked instability of functioning in response to environmental challenges.
We suggest labels for the two prototypical groups. Under our hypothesis, the first group, SOMMI-Traditional (43.6%), reflects traditional risk and treatment issues seen within the wider sex-offending population. This group also happens to have MMI issues. However, LTVs of SOMMI-Traditional type individuals evidenced little or no change in the face of acute MMI symptoms. They had very few prior psychiatric hospitalizations, and most showed little to no MMI symptoms at the time of sex offenses. The second type, SOMMI-MMI (56.4%), identifies individuals for whom treatment of MMI symptoms appears to be a primary need both for their overall functioning and for risk reduction. SOMMI-MMI type individuals demonstrated exacerbated LTVs in the presence of acute MMI symptoms. This group had repeated psychiatric hospitalizations, medication noncompliance near the time of sex offenses, and moderate to substantial psychiatric symptoms at the time of sex offenses. In this group, MMI symptoms were more likely to be rated as having a direct or indirect influence on sex offending.
In providing empirical support for this typology, this study goes beyond previous research. Previous studies have examined the influence of MMI symptoms on violent offending, as well as the predictive validity of formal risk instruments (Kingston et al., 2016; Peterson et al., 2014). This is the first study to examine the influence of MMI symptoms on repeat sex offenses and how MMI symptoms might influence the stability of how criminogenic needs are expressed. Our results are consistent with previous research in some respects. Similar to findings by Peterson and colleagues (2014) and Skeem and colleagues (2016), only a small proportion of sex offenses were identified as being directly related to MMI symptoms. Most sex offenses were related to a deviant arousal pattern or an antisocial personality pattern, which is consistent with research on sex offending in general (Mann, Hanson, & Thornton, 2010).
LTVs typically preexisted the onset of MMI. Within this sample, sex offending and non–sex offending criminal behavior tended to occur during adolescence, prior to the onset of MMI which usually occurred during early adulthood. Thus, it is not surprising that some LTVs would be present before MMI symptoms emerged (e.g., offense-related sexual interests) and would remain unchanged during psychiatric decompensation. LTVs most likely to be exacerbated by MMI symptoms were Grievance Thinking, Poor Emotional Control, and Poor Problem-Solving. The density of symptoms, especially psychotic symptoms, was associated with a larger number of LTVs being exacerbated by psychiatric decompensation. This influence was also evident when examining number of prior psychiatric hospitalizations and whether MMI symptoms were present at the time of the sex offenses. These findings lend further support to the idea that MMI largely has an indirect effect on risk through criminogenic needs as has been identified in previous work (Lee & Hanson, 2016).
Implications for Practice
Research results have been inconsistent regarding potential relationships between MMI symptoms and risk of violent and/or sex-offending behavior (e.g., Keers et al., 2014; Peterson et al., 2014; Smith & Taylor, 1999). Sample differences due to varying inclusion criteria (such as including common mental health diagnoses like depression, anxiety, or attention-deficit/hyperactivity disorder [ADHD] with diagnoses of MMI) may account for some divergent findings. Research has demonstrated predictive validity of risk assessment tools with this population; however, there may be a subgroup of individuals for whom traditional risk assessment tools do not fully capture risk and treatment needs due to fluctuations in mental states. In other words, a criminogenic profile may only be a snapshot in time. Its applicability could be very different depending on whether the individual was psychiatrically stable or decompensated. For example, when utilizing an actuarial measure of criminogenic needs, a single score associated with a probability of risk for sexual recidivism may either underestimate or overestimate risk if the density of criminogenic needs is notably affected by the acuity of their mental illness.
Evaluators may struggle when completing risk tools for individuals with MMI. For example, how should an individual’s psychiatric stability be viewed in a secure facility where medication adherence is closely monitored when he also has a history of medication noncompliance when unsupervised in the community? As previously identified by Sachsenmaier, Thornton, and Olson (2011), evaluators may handle such considerations inconsistently and over-attribute evidence to mental illness when it actually reflects the presence of an underlying risk factor. Furthermore, even when using measures that provide a route to assess future release settings, assumptions that the SOMMI population has a homogeneous level of risk tend to be pronounced.
We suggest that an early step in assessing risk for an individual with MMI would be to identify the individual’s SOMMI typology. Are the individual’s characteristics better represented by features of the SOMMI-Traditional or SOMMI-MMI type? This can be accomplished through a review of available records to determine whether the onset of MMI predates the onset of sex offending, previous psychiatric hospitalizations, and evidence of any relationship between MMI symptoms and past sex-offending behaviors. The individual’s entire offense history should be examined for evidence of any relationships between MMI symptoms and sexual offending behavior, not simply the index offense. As indicated in the current data, offense patterns may change over time. The Structured Assessment Resource (StAR) is a condensed version of the SOMMI data collection form used in this study. StAR was developed to help clinicians identify information needed to determine SOMMI typology, and StAR can be obtained from the first author.
We advocate the use of traditional measures of criminogenic needs with SOMMI-Traditional types whose LTVs are not exacerbated by MMI symptoms. MMI is not likely to have a direct or indirect causal effect on sex offending for these individuals. The risk assessment and identified treatment interventions should be those traditionally seen with a sex-offending population; however, MMI should be addressed as a responsivity issue (i.e., risk–needs–responsivity [RNR]; Andrews & Bonta, 2010). For SOMMI-MMI type individuals, whose risk may fluctuate as a function of mental status, we propose coding criminogenic items based on the individual’s best and worst psychiatric functioning. This captures the full range of possible risk and provides structure for special considerations if needed (e.g., medication compliance at discharge). Consideration of protective factors, such as community support and living circumstances, can provide important information to better understand risk and risk management needs (for further discussion of this issue, see Thornton, Kelley, & Nelligan, 2017). An important point for evaluators to keep in mind is that even within a small, specialized population like SOMMI, there appears to be some heterogeneity. A “one size fits all” approach may not adequately capture risk or address effective management of risk in this population. For example, assuming all discharged SOMMI patients are at increased risk due to medication noncompliance is not consistent with the present data.
Treatment interventions and strategies will likely vary based on the extent to which MMI is related to offending and the type of MMI present. For SOMMI-MMI individuals, priority should be given to treating the MMI through psychiatric medication. Cognitive behavior therapy for psychosis (Hagen, Turkington, Berge, & Grawe, 2011) and treatments designed to improve social cognition and theory of mind (Fiszdon & Reddy, 2012) have demonstrated some effectiveness. Traditional sex offense–specific treatment interventions focused on offense disclosures, and precipitating factors may be of little value for an individual who was floridly psychotic at the time of past sex offenses. This is particularly true for such individuals without a paraphilic arousal pattern or antisocial personality style. The individual’s memory of past sex offenses may be the version they encoded at the time they were experiencing delusional beliefs. Treatment in these cases should focus on increasing receptiveness to protective factors, such as medication compliance and case management support, to manage risk. For SOMMI-MMI cases with deviant arousal pattern and/or antisocial personality pattern in addition to MMI symptoms, treatment goals should help the individual achieve psychiatric stability. This permits them to participate in other interventions addressing criminogenic needs, as well as increasing their receptiveness to protective factors.
Limitations and Future Directions
This study was based on a sample of 55 cases, reflecting the strict inclusion criteria regarding MMI diagnoses. Strict inclusion criteria reduced the available sample but avoided potential analytic and interpretational problems that might have arisen had more commonly diagnosed disorders, such as ADHD, depression, and anxiety, been included. Although the sample size was relatively small, each case contributed multiple sex offenses, resulting in a total of 176 coded sex offenses.
Although coders had access to a large set of archival records, data related to specific variables were sparse (e.g., information on family members). Missing data may have impacted the analytical results. On the other hand, the majority of the sex offenses contained sufficient information to code whether MMI symptoms were present at the time of the offenses. This is likely due to the fact that we had access to police and probation reports as well as psychiatric hospital records.
The cases were also drawn from a highly selected, high-risk group of individuals who had committed a variety of sex offenses and had been detained under Wisconsin’s civil commitment law regarding SVPs. Given the nature of the high-risk sample and that individuals must have a history of a statutorily qualifying sexually violent offense, individuals had committed very serious sex offenses. This highly selected, high-risk group may limit generalizations to other SOMMI samples.
Pursuant to Wisconsin’s SVP law, individuals with MMI found Guilty but Not Guilty by Reason of Mental Disease or Defect can be civilly committed. This is not necessarily true for other states. There was a notable portion of cases who demonstrated profound MMI, but generally sex offending began prior to the onset of MMI in this sample. Many cases did not demonstrate notable psychiatric symptoms at the time of past sex offending. Additional research is underway in Massachusetts; however, that SOMMI sample is similar to the current one. Similar research with a psychiatric hospital sample would be beneficial to evaluate the generalizability of current results. It is possible that a psychiatric hospital sample will have a different composition of SOMMI cases (e.g., earlier onset of MMI; later onset of problematic sexual behavior; lower static risk as measured by the Static-99R; less serious histories of sex offending). A psychiatric hospital sample may also demonstrate a different pattern of how MMI symptoms affect LTVs. It will be important to determine if the typologies identified in this study apply to a psychiatric hospital sample.
The current results are based upon nine LTVs from the Structured Risk Assessment framework. It would be worthwhile to determine whether an actuarial measure of criminogenic needs can be scored reliably with this population. For example, Sachsenmaier and colleagues (2011) found that evaluators demonstrated particular difficulty with inter-rater reliability when coding the Structured Risk Assessment–Forensic Version among a group with intellectual disabilities and/or MMI. It appeared that some raters had discounted evidence that would otherwise have supported a risk factor because they attributed it solely to low IQ and/or MMI. Further exploration of criminogenic need patterns of the different SOMMI typologies utilizing actuarial criminogenic measures would provide further insight into assessing and treating this population.
Supplemental Material
Supplementary_file – Supplemental material for Exploring the Relationship Between Major Mental Illness and Sex Offending Behavior in a High-Risk Population
Supplemental material, Supplementary_file for Exploring the Relationship Between Major Mental Illness and Sex Offending Behavior in a High-Risk Population by Sharon M. Kelley, David Thornton, Ryan Mattek, Letitia Johnson and Gina Ambroziak in Criminal Justice and Behavior
Footnotes
Authors’ Note:
The views expressed are those of the authors and not necessarily those of the Wisconsin Department of Health Services. The authors would like to acknowledge and thank Laurie Guidry, Psy.D., for her consultation in this research project and James Mundt, PhD, for his helpful comments on an earlier draft of this manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.