
Abstract
This pre–post follow-up randomized trial investigated the receptiveness and responsiveness of 82 incarcerated men undergoing reentry to feedback (discussion-based, form-based, or none–minimal) regarding their criminogenic risk–needs assessment results. Both short-term outcomes (self-perceived risk–needs, motivation for change, treatment readiness, and feedback satisfaction) and longer-term outcomes (intuitional conduct, rearrest, or halfway house return) were examined. As hypothesized, among study completers (n = 67), motivation for change was significantly higher following discussion feedback, and both feedback formats were rated favorably by participants. Contrary to hypotheses, feedback recipients, including those who showed gains at post, did not appear reliably distinct from others on longer-term outcomes; nor were most outcomes significantly associated with baseline risk scores. Feedback about risk and needs may be useful in correctional treatment for motivation enhancement and treatment orienting, but special attention to measurement, contextual, and intensity factors is warranted.
Given the substantial human and financial costs of criminal recidivism, correctional rehabilitation is an important penal strategy (Dvoskin et al., 2012; Lipsey & Cullen, 2007). The risk–need–responsivity (RNR) model is the leading framework for designing, implementing, and evaluating correctional rehabilitation services (Bonta & Andrews, 2017). RNR’s overarching principles respect people and norms, theory and evidence, human service, and crime prevention. The core RNR principles direct the use of risk assessment to match service intensity and extensiveness to client risk and needs, prioritization of targeting criminogenic needs over other issues, and utilization of evidence-based and individually tailored services to enhance client responsiveness. The structured assessment principles call for assessments of a wide range of need and strength factors, and permits judicious professional discretion. The program delivery–dosage principle reminds of the importance of matching service intensity and extensiveness to recidivism risk, and managing risk for attrition. The staff practices principles stress the importance of staff using good relationship and structuring skills with clients. Finally, the organizational principles advocate for good agency management practices, a preference for community-based services, and provisions for continuity of services across settings.
Many of RNR’s principles have meta-analytic support (Andrews, 2000). For example, most meta-analyses have yielded support for the risk, need, general responsivity, and specific responsivity principles (Wormith & Zidenberg, 2018). Supportive evidence is also exemplified by individual studies. For example, regarding the risk and general responsivity principles, Lowenkamp et al. (2006) found that, across 97 residential and nonresidential correctional treatment programs in Ohio, reductions in recidivism were maximally achieved by programs that targeted higher risk adults under community supervision and provided them with more cognitive-behavioral services for a longer duration. As another example, regarding the need principle, Peterson-Badali et al. (2015) found in general that, among 148 justice-involved youth, criminogenic needs were significantly and sizably related to recidivism, and youth who received services matched to their needs reoffended at significantly lower rates. However, while promising evidence abounds, some RNR principles, including the core principle of specific responsivity, warrant further validation (Andrews et al., 2011).
Specific Responsivity
The specific responsivity principle directs for consideration of the individual characteristics of persons who are justice-involved that may influence responsiveness to different treatment modes. Due to the problem of treatment attrition (Olver et al., 2011; Sturgess et al., 2016), the specific responsivity factors of motivation for change (which focuses on internal factors to the person) and treatment readiness (which focuses on internal and external factors to the person) have received increased attention (Mossière & Serin, 2014; Ward et al., 2004). Motivational enhancement approaches have been the primary focus in this area; there is a dearth of studies of pretreatment interventions targeting other specific responsivity factors (McMurran & Ward, 2010).
The lesser attention that has been paid to evaluating efforts to modify specific responsivity factors other than motivation–readiness may be due in part to lesser conceptual clarity about the nature of some of these factors. Problem recognition and outcome expectancies, for instance, are two factors that may be distinct specific responsivity issues related to self-awareness (e.g., a denial–minimization response style; Andrews et al., 2004). Alternatively, they may be more related to criminogenic needs (e.g., antisocial cognitions). Outside of corrections, self-evaluations and evaluations made by others have been shown to both contribute to and bias the prediction of behavior (e.g., Epley & Dunning, 2006). While several prior studies have examined self-perceived risk and needs and the predictive utility of this information among persons in custody, whether such self-perceptions can be modified has not been examined. Accordingly, additional research about the nature and modifiability of specific responsivity factors beyond motivation–readiness, such as self-perceptions, is warranted.
Assessment Feedback for Enhancing Specific Responsivity
Assessment feedback is an early treatment strategy that can target both motivation–readiness and self-awareness (Bollich et al., 2011; Miller & Rollnick, 2009). A variety of evaluator-perceived benefits of feedback have been reported (e.g., aid interpretation, improve client understanding, ascertain client agreement or disagreement, increase motivation to follow recommendations, enhance wellbeing; Smith et al., 2007). The provision of psychological assessment feedback is normative, although the forensic–correctional context has been a reported barrier (Curry & Hanson, 2010).
Feedback is considered an intervention in and of itself when it involves the sharing and exploration of individualized assessment results in an empathic and collaborative manner (Finn & Tonsager, 1997). It may be administered verbally, in writing, or via a combination of the two modalities, and the limited available evidence suggests that a combined method may be most satisfying to clients and may enhance the effects of feedback (Fallows & Hilsabeck, 2013). Meta-analyses have found significant and sizable effects for psychological testing feedback (e.g., for working alliance, client-perceived helpfulness, client understanding, symptoms, hospitalizations, and binge drinking episodes; Hanson & Poston, 2011; Poston & Hanson, 2010). However, no correctional samples were included in these meta-analyses.
In RNR, assessment results, including about risk, needs, strengths, and responsivity factors; and implications, such as the consequences of treatment refusal, are meant to be reviewed with persons who are justice involved. The goal is to develop mutually agreeable service plans—that is, determining individually tailored strategies for capitalizing on preexisting strengths and changing criminogenic needs into additional strengths—as a means of enhancing treatment readiness. For instance, readiness may be enhanced via improved self-awareness and outcome expectancies, and agreement about the treatment rationale and plan. It is expected that enhanced readiness will improve response to treatment and decrease risk for attrition, and in turn decrease risk. Accordingly, feedback about assessment results is considered a fundamental strategy in RNR: the importance of feedback is stressed in trainings for providers, and the rationale for including case management sections in newer level of service (LS) risk–need assessment tools was to “increase the likelihood that service providers will conduct these important discussions with offenders” (Andrews et al., 2011, p. 742; see also Andrews et al., 2010).
Relatedly, motivational interviewing (MI; Miller & Rollnick, 2009) is recognized as a core provider practice in RNR (Andrews & Bonta, 2010), and motivational enhancement therapy (MET) is a variant of MI that includes structured assessment feedback (Miller et al., 1992). Motivation enhancement strategies associated with these and other popular models (e.g., transtheoretical stages-of-change model; Prochaska et al., 1992) include providing personalized feedback; acknowledging responsibility and prerogative for change; offering clear, supportive, and professional advice–guidance; presenting a menu of change strategies and goals from which to choose; conveying accurate empathy for the client’s plight and experience; supporting self-efficacy for change; addressing misconceptions about therapy; incentivizing and reinforcing consideration of, movement toward, and accomplished change; eliciting internally generated change talk; and reframing problems and obstacles in more optimistic, surmountable ways (Ogrodniczuk et al., 2005). Investigations of MI in corrections contexts have yielded some supportive evidence (see McMurran, 2009, for a review of 19 primary studies). For example, one study found that attendance was better for MET compared to drug counseling comparison groups (Carroll et al., 2006); another study found that participants showed enhanced motivation and decreased substance use and reported problems following MET (Sinha et al., 2003). However, motivation enhancement and other specific responsivity effects of RNR-based assessment feedback specifically, and variability of effects by feedback format, are in need of direct investigation.
Current Study
The purpose of this longitudinal multiarm parallel-group randomized trial was to address the dearth of prior research on correctional assessment feedback and add to the modest evidence base on motivation for change, treatment readiness, self-perceived criminogenic needs (problem recognition), and self-perceived criminogenic risk (outcome expectancies) in correctional rehabilitation. Whether feedback would function as a brief intervention was also of interest, given the realities of barriers to human services in corrections, including limits on the availability of treatment programs in prison and jails and relatively brief periods of incarceration in jails. Three feedback formats (none–minimal, form-based, and discussion-based) were investigated with men in custody on general population units.
The primary hypotheses were that participants who received more than minimal feedback would show significant, moderate increases in evaluator-rated and self-perceived risk–needs agreement, motivation for change, and treatment readiness. Secondary hypotheses were that increases would be strongest for the discussion condition and that feedback would be rated favorably. Exploratory hypotheses were that institutional conduct and community recidivism would be associated with evaluator- and self-appraised risk and that participants who received more than minimal feedback and evidenced postfeedback gains would, presumably due to improved responsivity, demonstrate better institutional conduct and recidivism outcomes.
Method
Participants
The study was approved by a university Institutional Review Board, state correctional agency, and private corrections company. Men in custody at a prerelease correctional rehabilitation facility in New Jersey were eligible for inclusion. Potential participants were randomly solicited (every third admission to the general population units) within approximately a week of admission (N = 127). The two exclusion criteria were (a) inability to communicate in English and (b) reading difficulties for study materials (Flesch-Kincaid Grade Levels ranged from 4.2 to 7.7). No compensation was provided for participation.
As seen in Table 1, participants were primarily African American men in their thirties who were single, did not have a college education, had committed a variety of offenses (most often drug-related offenses), and were medium to high risk (there were few low-risk and very high-risk cases, and no very low-risk cases). Few demographic differences were found between study completers and noncompleters, and among the three study conditions. In addition, the final sample’s demographics (age, ethnicity, and index offense) roughly approximated that of the state’s populations of persons in prisons or halfway houses (Office of Policy and Planning, 2012). Analyses were therefore not adjusted for participant characteristics. 1
Demographic Characteristics of Sample
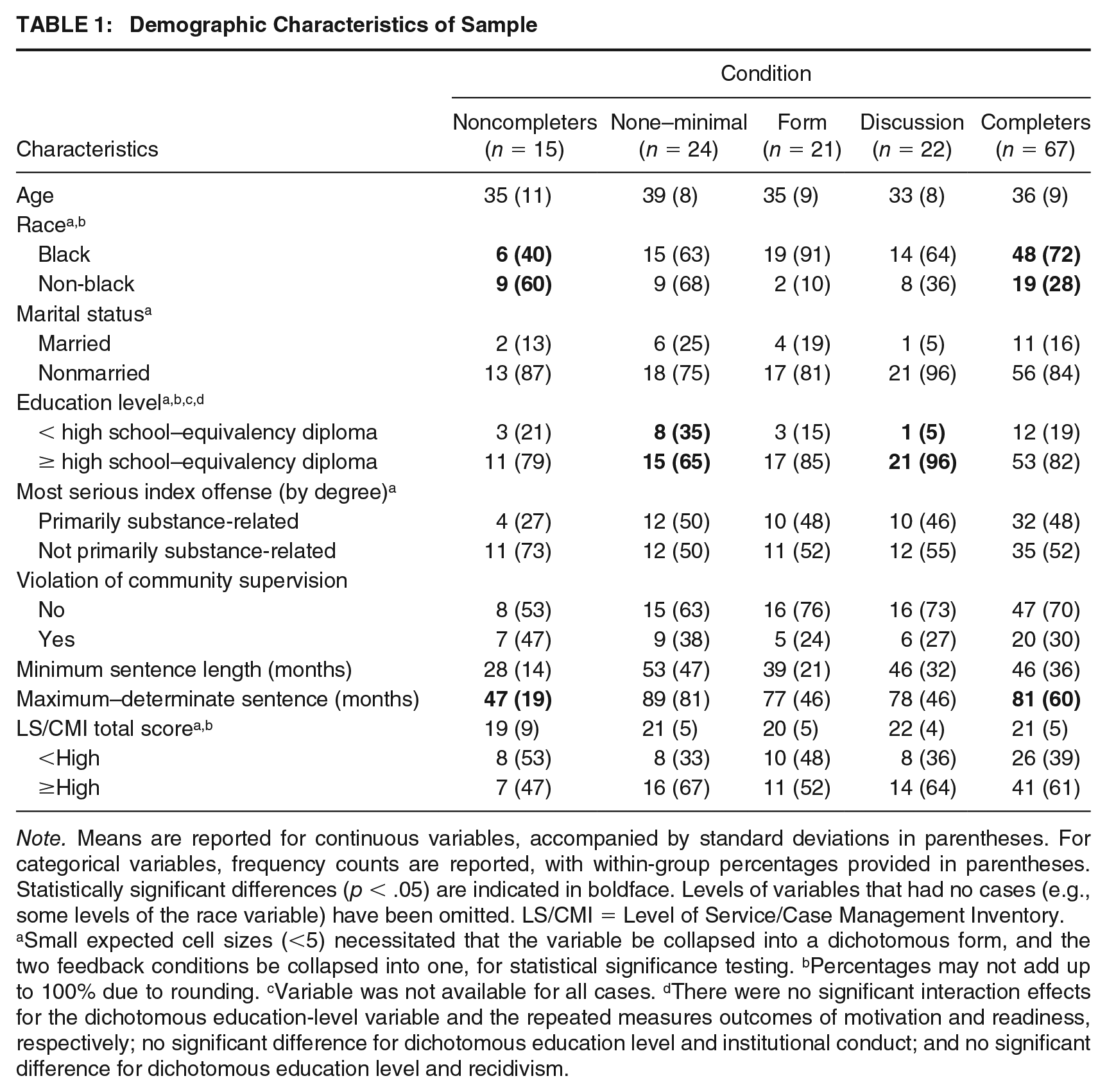
Note. Means are reported for continuous variables, accompanied by standard deviations in parentheses. For categorical variables, frequency counts are reported, with within-group percentages provided in parentheses. Statistically significant differences (p < .05) are indicated in boldface. Levels of variables that had no cases (e.g., some levels of the race variable) have been omitted. LS/CMI = Level of Service/Case Management Inventory.
Small expected cell sizes (<5) necessitated that the variable be collapsed into a dichotomous form, and the two feedback conditions be collapsed into one, for statistical significance testing. bPercentages may not add up to 100% due to rounding. cVariable was not available for all cases. dThere were no significant interaction effects for the dichotomous education-level variable and the repeated measures outcomes of motivation and readiness, respectively; no significant difference for dichotomous education level and institutional conduct; and no significant difference for dichotomous education level and recidivism.
An a priori power analysis for the most demanding planned analysis (two-way mixed analysis of variance [ANOVA]) was conducted using the following parameters: alpha (α) = .05; power (β) = .95; effect size (f) = 0.25 (medium-sized effect converted from η p 2 = .06 based on the large effect sizes observed in a study of a more intensive motivation enhancement program, Anstiss et al., 2011); correlation among repeated measures = .5; and nonsphericity correction (ε) = 1. The estimated necessary sample size was N = 66. In anticipation of an estimated 15% attrition rate, the target enrollment sample size was N = 75, with approximately 25 participants per condition completing the study. Once the minimal follow-up period had concluded for the last enrolled participant, recidivism data were collected and final analyses were performed.
A computerized random number generator was used to construct a fixed blocked randomization sequence so that each of the three study conditions would be populated by 25 participants at baseline, with enrollment then continuing until the necessary minimal sample size of 66 with complete pre–post data for all measures was achieved. The first author, who conducted all participant contacts, generated the assignment sequence prior to participant enrollment, enrolled participants, and assigned them to groups.
Measures
The first author administered all measures except the evaluator-rated risk–needs assessment tool, which was administered by facility staff, and extracted certain participant data (i.e., administrative and recidivism information, and evaluator-rated risk–needs assessment scores) from electronic systems either directly into separate electronic data sets or using paper forms for subsequent entry into electronic data sets. The presentation order for the self-report measures was counterbalanced. Paper data (demographic information, item responses for the self-perceived risk–needs and feedback helpfulness measures, scale–index and subscale–subcomponent scores for the other study measures) were double entered into an electronic data set by two research assistants. The first author resolved discrepancies. The retest interval for all measures for the none–minimal condition—the condition used for retest reliability analyses, given the lack of a feedback confound—ranged from 21 to 49 days (M = 34.13, SD = 8.83).
Risk Need Perception Survey
The Risk Need Perception Survey (RNPS) Version 1 (Brooks Holliday et al., 2013) was developed as a measure of self-perceived criminogenic needs. Version 1 has 30 items that reflect RNR’s Central Eight risk factors as well as other factors (responsivity factors, weak covariates of criminal recidivism, and factors likely unrelated to reoffending). Individual items are scored as 1 = Not Important, 2 = Possibly Important, and 3 = Definitely Important. Some Central Eight risk factors are measured via a single item (e.g., Criminal History: “Your criminal history”), whereas others are an index of two or more items (e.g., Education–Employment: “Your education level” and “Your work life [over the past 3 years]”).
Toward further refinement of the measurement of self-perceived risk–needs, three slightly modified versions of the RNPS (Versions 2–4) were used in this study (the details of these modifications are noted in Table 2), though participants’ questions about the RNPS were addressed via the same verbal clarifications irrespective of the version that was used. Version 2 was administered to two participants. It reflected an update to the wording of some items and response options from Version 1 to improve clarity, and the addition of three items about antisocial personality pattern, probabilistic risk, and categorical risk, respectively. Versions 3 and 4 were administered to 73 and 7 participants, respectively. They reflected some additional minor adjustments to the wording of response options in light of some recurring questions from respondents.
Descriptives for Study Measures and Outcomes

Note. Means are reported with standard deviations in parentheses (RNPS, URICA, CVTRQ, institutional conduct); medians are reported with the interquartile range in brackets (FHS). Three versions of the RNPS were used. Response options in instructions were as follows: Version 2: 1 = No (not present in your life, or not a problem if it is), 2 = Somewhat, and 3 = Yes; Version 3: 1 = No (area is not a problem for you), 2 = Somewhat (area is a medium problem for you), and 3 = Yes (area is a major problem for you); Version 4: 1 = No (area is not a problem for you for reoffending), 2 = Somewhat (area is a medium problem for you for reoffending), and 3 = Yes (area is a major problem for you for reoffending). Response grid reminder and anchors were as follows: Version 2 and 3: Present and could make you more likely to reoffend if not changed and No, Somewhat, and Yes; Version 4: Area could make you more likely to reoffend if not changed and No (Not problem), Somewhat (Medium problem), and Yes (Major problem). The FHS items were as follows: “I agree with the feedback”; “I found the feedback helpful”; “The feedback told me things about myself that I did not already know”; “Because of the feedback, I now have a better understanding of the issues that might make me more likely to commit a crime”; “Because of the feedback, I now have a better understanding of the things I need to work on in treatment”; and “I think the feedback would be helpful for other people who are in jail or prison for committing crimes.” RNPS = Risk Need Perception Survey; LS/CMI = Level of Service/Case Management Inventory; URICA = University of Rhode Island Change Assessment; CVTRQ = Corrections Victoria Treatment Readiness Questionnaire; FHS = Feedback Helpfulness Survey.
Individual Central Eight risk factor items and indexes on Versions 2 to 4 were scored similarly to Version 1 (Brooks Holliday et al., 2013). Several experimental total score indexes were then generated, since the study of Version 1 had only examined individual risk factor scores and their correlation with corresponding risk factor scores on the LS/CMI (Brooks Holliday et al., 2013). The LS/CMI–RNPS concordance score was the total number of approximate agreements (participants rating themselves at the same or one risk level higher using three risk bins) for Central Eight risk factors: (a) LS/CMI Very Low or Low and RNPS No or Somewhat; (b) LS/CMI Medium and RNPS Somewhat or Yes; and (c) LS/CMI High or Very High and RNPS Yes (possible range = 0–8; retest r = .33). The number and level of criminogenic needs score was the sum of RNPS Central Eight risk factor endorsements (0 = No, 1 = Somewhat, 2 = Yes; possible range = 0–16; retest r = .28). The number of criminogenic needs score was the sum of any RNPS Central Eight risk factor endorsements (0 = No, 1 = Somewhat or Yes; possible range = 0–8; retest r = .42). The probabilistic risk score was a 0% to 100% item (retest r = .48). The categorical risk score was a Likert-type item (1 = Not at all, 2 = Slightly, 3 = About 50/50, 4 = More likely than not, 5 = Definitely; retest r = .41). Owing to unacceptably low retest reliability for each of these indexes, reported results were not interpreted beyond the two possibilities that the RNPS was unreliable or self-perceptions were unstable.
University of Rhode Island Change Assessment
The University of Rhode Island Change Assessment (URICA; McConnaughy et al., 1983, 1989) is a 34-item measure of motivation for change for a general or specified behavior (directions here focused on offending). The URICA is comprised of Likert-type items with a rating scale of 1 = Strongly Disagree, 2 = Disagree, 3 = Undecided, 4 = Agree, and 5 = Strongly Agree. The continuous scoring method—which assumes that individuals at later stages of change will endorse fewer Precontemplation items (with the Precontemplation subscale score thus subtracted from the sum of the Contemplation, Action, and Maintenance subscales)—was used in light of prior reliability and validity evidence with persons who were justice-involved (Polaschek et al., 2010). Potential scores range from 2 to 14, with higher scores indicating a higher stage of change (2–8 = Precontemplation; 9–11 = Contemplation; 12–14 = Preparation into Action Taking). Retest reliability was acceptable in the current sample (r = .75).
Corrections Victoria Treatment Readiness Questionnaire
The Corrections Victoria Treatment Readiness Questionnaire (CVTRQ; Casey et al., 2007; Day et al., 2009, 2010) is a 20-item measure of readiness for correctional treatment. Respondents rate Likert-type items using a scale of 1 = Strongly Disagree, 2 = Disagree, 3 = Unsure, 4 = Agree, and 5 = Strongly Agree, with several items being reverse scored. Total scores range from 20 to 100, with higher scores indicating greater readiness. The CVTRQ has demonstrated good internal consistency and convergent, divergent, and predictive validity. In the current sample, retest reliability was good (r = .87).
Feedback Helpfulness Survey
Given the absence of a previously validated measure of perceptions of correctional assessment feedback, a 6-item experimental questionnaire was generated based on prior theory that feedback facilitates enhanced client understanding and ascertainment of agreement with indicated treatment targets (Smith et al., 2007). The survey was used at post to measure the extent to which participants in the form and discussion conditions found feedback to be accurate, informative, useful, and recommendable. Response options were 1 = Strongly Disagree, 2 = Slightly Disagree, 3 = Slightly Agree, and 4 = Strongly Agree. The individual items, all of which were written to capture unique information (the language of the items is noted in Table 2) were indexed to yield a total score ranging from 6 to 24, with higher scores indicating more positive ratings of the feedback service. The index had good internal consistency (n = 43, M = 20.30, SD = 3.29, Cronbach’s alpha [α] = .81, standard error of measurement using α [SEMα] = 1.43).
Level of Service/Case Management Inventory
The Level of Service/Case Management Inventory (LS/CMI; Andrews et al., 2004) is an evaluator-rated criminogenic risk–needs assessment tool. Section 1 (General Risk/Need) consists of 43 items that are ultimately scored dichotomously as 0 or 1 = Yes (a very or relatively unsatisfactory situation) or 2 or 3 = No (a satisfactory or relatively satisfactory situation) based on record and interview information. The final dichotomous item scorings (1 = Yes, 0 = No) are combined in an actuarial manner to assign an individual to one of five risk bins for each of the Central Eight risk factors, as well as for categorical risk overall (Total score: 0–4 = Very Low, 5–10 = Low, 11–19 = Medium, 20–29 = High, and 30+ = Very High).
The LS/CMI is one of the most widely used risk–needs assessment tools, and it has demonstrated good psychometric properties (Andrews et al., 2010). In addition to evidence of acceptable to good internal consistency and interrater and retest reliability (Andrews et al., 2004; Labrecque et al., 2017), the LS/CMI and other LS tools have demonstrated adequate to excellent predictive validity for a range of recidivism indicators (e.g., rearrest, institutional misconduct, and halfway house failure; Olver et al., 2014). In the current sample, internal consistency for the LS/CMI Total score was poor (n = 82, M = 20.73, SD = 5.65, α = .58, SEMα = 3.66). However, only scores on the eight Section 1 subcomponents were coded, rather than all of the Section 1 items. Consequently, the calculation of α with just these eight scores likely underestimated internal consistency, given the metric’s sensitivity to low item number.
Outcome Variables
Facility electronic records were used to extract several outcome variables. The first set was participants’ positive (merits, which staff could log for any observed desirable conduct, whether related to one’s treatment plan or not) and negative behaviors (demerits, which staff could log for any observed problematic conduct) following study participation and until transfer from the facility. Staff used standardized merit–demerit categories in addition to miscellaneous entries that sometimes included narrative specification. Examples of merits included helpfulness and good participation during a group, and examples of demerits included unreceptive to staff direction and disruptive during a group. Institutional conduct was then operationalized primarily as number of merits minus demerits, and secondarily as number of merits and demerits separately. The other outcome variable extracted from facility records was any return to a more secure correctional facility following transfer to a halfway house (1 = Yes, 0 = No). Finally, data concerning any rearrests or reconvictions (1 = Yes, 0 = No) were obtained at a local courthouse. However, only rearrest data were ultimately used, and because recidivism rates were somewhat low (see Table 2), as a combined rearrest or halfway house return variable.
Procedure
The study design was a quasi-controlled trial with blocked randomization. The first contact with participants involved random solicitation, informed consent, random assignment, and baseline administration of the RNPS, URICA, and CVTRQ. All participants received treatment as usual at the facility (see Table 3; see also Brooks Holliday et al., 2012, for a pre–post program evaluation using the LS/CMI with different participants at the facility). This included administration of the LS/CMI by master’s-level facility assessment staff (who were trained and supervised in LS/CMI administrations by a licensed psychologist) within the first few weeks of intake (n = 50, 61%), unless it had already been administered within the preceding 2 years (n = 32, 39%). Although completion rates for treatment were not measured, it was presumed that most participants completed assigned programming, as participation in the facility’s programming was mandatory for all residents.
Summary of Feedback Conditions
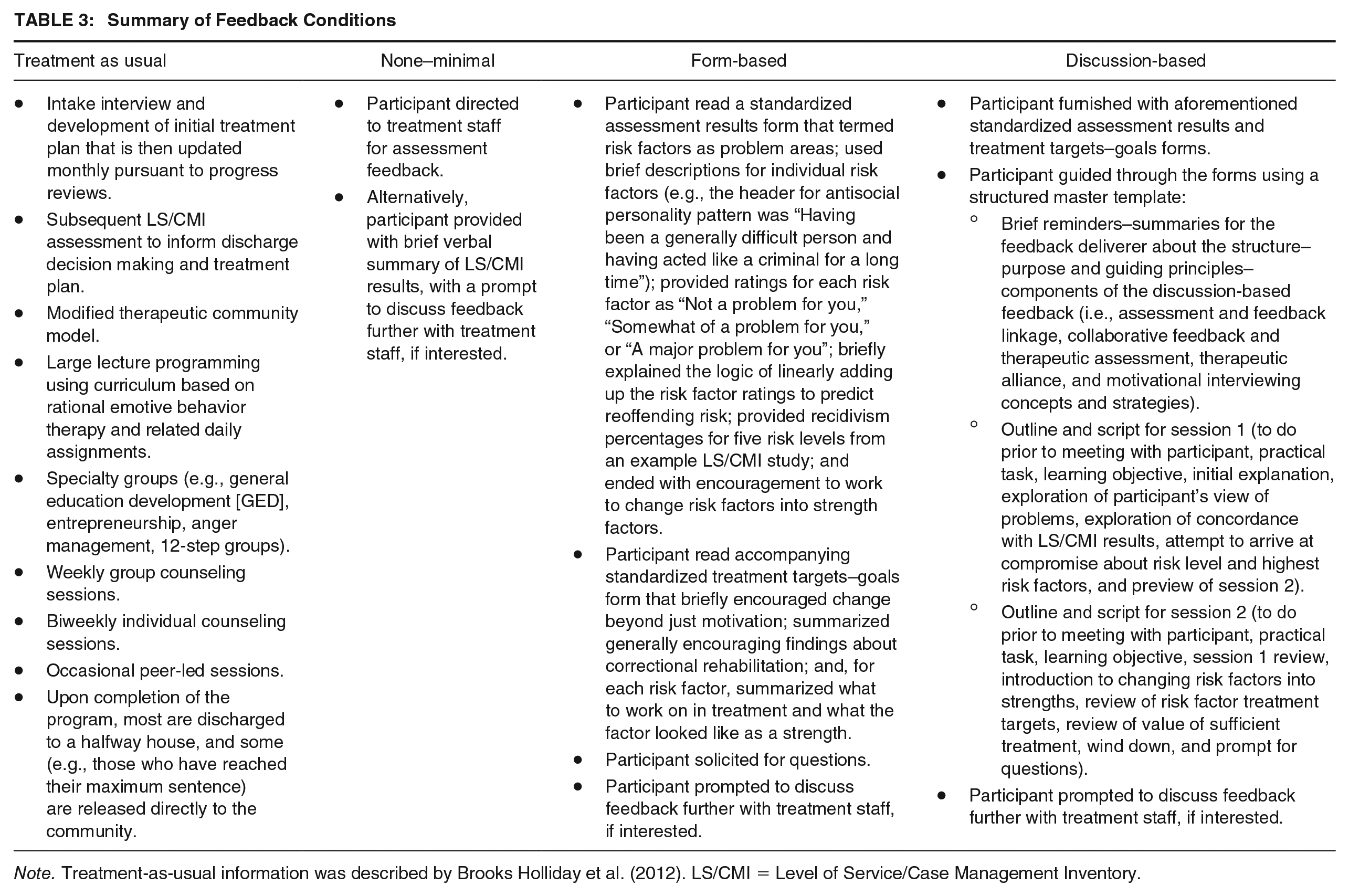
Note. Treatment-as-usual information was described by Brooks Holliday et al. (2012). LS/CMI = Level of Service/Case Management Inventory.
The second participant contact involved the provision of one or two sessions of discussion-based feedback, a single session of form-based feedback, or none or minimal feedback, approximately 1 month after LS/CMI results became available. A summary of the feedback conditions is provided in Table 3. The feedback conditions were inspired by therapeutic assessment (Finn, 2007), MI (Anstiss et al., 2011), and therapeutic alliance sources (Ross et al., 2008). LS/CMI results, sample actuarial risk rates from a retrospective LS/CMI validation study (Rettinger, 1998, as cited in Andrews et al., 2004, p. 120), and treatment goals derived from Andrews and Bonta (2010, pp. 58–60, 500) constituted the primary content covered during feedback. Standardized assessment results and treatment targets–goals forms were used for the form and discussion conditions, and a standardized script was used for the discussion condition. All feedback was provided individually and all participants were free to ask questions.
The none–minimal condition constituted treatment as usual plus, in some cases, rapid (i.e., approximately 5–10 minutes) feedback, or more typically, a recommendation to request feedback as part of individual meetings with treatment staff (which would not have involved study feedback materials). The differences between the form and discussion feedback conditions, respectively, were duration (approximately a half-hour versus approximately 2 hours, on average); the depth of explanations provided (brief, unscripted explanation of key concepts followed by a prompt for any questions, versus a lengthier scripted and more involved explanation); and the extent and style of discussions surrounding prior experiences, release plans, and the personal import of the assessment results (psychoeducational versus greater attention paid to MI principles, including a greater emphasis on questioning and elucidation, validation, constructive shaping, and supporting). Otherwise, similarities between the form and discussion conditions were intentional and related to a tertiary interest in feasibility—that is, the minimum necessary intensity to produce desirable effects. As such, formally measuring whether the form and discussion conditions were consistently and sufficiently distinctive (e.g., via observations and ratings, or manipulation checks) was not an objective of the study and did not occur.
After feedback, approximately half of the feedback participants were immediately re-administered the self-report measures (n = 24), whereas the other half waited approximately a week (n = 19) to allow for an evaluation of possible immediacy effects, which were not detected. None–minimal participants were re-administered self-report measures using approximately the same schedule. The follow-up period was a minimum of 1 year, beginning after the last enrolled participant was transferred from the study site.
Analytic Strategy
All available participant data were used, without transformation. Missing data were rare; pairwise deletion was used. No outliers were removed. Interpretation focused on effect sizes and corresponding confidence intervals in lieu of a multiple-comparisons correction.
Descriptive statistics were conducted for all study variables (Table 2). Regarding primary (self-report at post) and secondary hypotheses (feedback format, satisfaction), scores on the URICA and CVTRQ were analyzed between and within groups simultaneously using two-way mixed ANOVA. There were five outliers for the URICA and two for the CVTRQ. The form condition evidenced non-normality for the URICA at pre and post, and for the CVTRQ at post. The assumptions of homogeneity of variances and covariances were satisfied for both measures. The planned parametric procedure was retained because the overall number of outliers was relatively low, the ANOVA procedure in general is fairly robust to deviations of normality, and there is a lack of widely used nonparametric alternatives to the two-way mixed ANOVA. However, post hoc analyses were conducted for the URICA and CVTRQ using nonparametric alternatives to the independent samples t-test (Wilcoxon rank-sum test, W) and dependent samples t-test (Wilcoxon signed-rank test, V), respectively, owing to a few outliers (one to three) and non-normality for some comparison levels for the CVTRQ. For feedback helpfulness ratings (feedback helpfulness survey [FHS]), there was one outlier FHS score, and FHS scores were non-normally distributed. Therefore, one-sample Wilcoxon signed-rank tests were used to compare groups’ median scores to the mid-point of the measure, and a Wilcoxon rank-sum test was used for a between-group comparison.
Regarding exploratory hypotheses (variables related to proximal and distal outcomes), for intuitional conduct, there were three outlier scores across study conditions, and non-normality was evident. Therefore, a nonparametric alternative to ANOVA (Kruskal–Wallis test, Kruskal–Wallis χ2) and Wilcoxon rank-sum tests were used. When feedback participants were dichotomously classified as to whether they demonstrated any categorical gain on the URICA at post compared to baseline, and similarly, continuous gain on the CVTRQ, there were six outliers on the URICA and three outliers on the CVTRQ, and the scores on the measures were non-normal. Accordingly, Wilcoxon rank-sum tests were used. For rearrest or halfway house return, all expected cell counts were greater than 5 for study condition and dichotomous URICA and CVTRQ gain classifications, and so chi-square tests of independence (χ2) were used. For both institutional conduct and rearrest–halfway house return, there was homogeneity of variances for all measures correlated with these outcomes. However, the number of outliers ranged from none to two across the URICA, CVTRQ, and LS/CMI variables for these analyses, and the URICA had a non-normal distribution. Accordingly, nonparametric alternatives to Pearon’s correlation (Spearman correlation, ρ); point-biserial correlation (rank-biserial correlation, ρ rb ); and semipartial point-biserial correlation (semipartial ρ rb ) were used.
Results
As shown in Figure 1, 82 individuals provided informed consent to participate and completed baseline measures; 67 participants completed both baseline and postmeasurements (24, 21, and 22 participants completed the none–minimal, form, and discussion conditions, respectively). Noncompletion was due to transfer from the study site before administration of postmeasures (n = 6), self-withdrawal due to loss of interest or irritation about the feedback (n = 7), or incomplete LS/CMI Section 1 data (n = 2 plus a participant who was removed for one of the other reasons). One participant was only missing 4 of 39 LS/CMI Section 1 items and so the first author scored these items based on a brief interview. Follow-up data were obtained for all 82 participants.

Participant Flow Diagram
The first phase of the study (enrollment through postmeasurement) took place between October 2012 and February 2014; the second phase (follow-up period) proceeded between May 2014 and October 2015. Participants’ average length of stay at the facility was 78.68 days (SD = 25.27, range = 16–139). The average number of days between feedback and post for the form (M = 2.67, SD = 3.48) and discussion conditions (M = 6.27, SD = 7.24) differed by 3.61 days, which was significant, t(41) = −2.07, p = .05, and attributable to four outlier participants in the latter condition who completed post 10, 14, 21, and 28 days after feedback. The follow-up period ranged from 12.67 to 29.66 months (M = 21.76, SD = 4.76 months), and there were no significant differences in follow-up duration among the three conditions, F(2, 79) = .32, p = .73. The descriptives for institutional conduct for the total sample were, for merits, M = 2.38, SD = 2.73, range = 0 to 10; for demerits, M = 2.41, SD = 3.00, range = 0 to 15; and for merits minus demerits, M = −.04, SD = 3.89, range = −15 to 9. The base rates for the different recidivism indicators for the total sample were 26% for halfway house return, 17% for rearrest, and 9% for reconviction. Time at risk was significantly correlated with any rearrest–halfway house return, ρ rb = .33, p = .003.
Primary and Secondary Hypotheses: Scores at Post Would Differ by Feedback Condition and Feedback Would Be Rated Favorably
Regarding the concordance between criminogenic needs rated by evaluators (LS/CMI) and participants (RNPS), the retest reliability coefficient for none–minimal feedback participants was unacceptably low. Planned significance testing for this variable was thus contraindicated.
The simple main effect of time for motivation for change (URICA) was only significant for the discussion condition, F(1, 21) = 15.68, p = .001. Consistently, only the discussion condition yielded a significant dependent samples post hoc effect, V = 2.56, p = .001, r = .70, 95% confidence interval (CI) [.53, .88]. The simple main effect of condition was also significant at post, F(2, 64) = 4.47, p = .02. Participants in the discussion condition yielded significantly higher URICA scores at post compared to both none–minimal participants, p = .05, difference in means (MD) = 1.41, 95% CI [.02, 2.79], and form participants, p = .02, MD = 1.62, 95% CI [.19, 3.05]. Consistently, independent samples post hoc effects at post were only significant for the discussion condition over the none–minimal condition, W = 5.03, p = .02, r = .36, 95% CI [.10, .61], and form condition, W = 4.84, p = .01, r = .39, 95% CI [.12, .66], respectively. There was a significant interaction between condition and time, which explained 14% of the variance, F(2, 64) = 5.39, p = .007, η p 2 = .14, 95% CI [.01, .29].
The main effect of time for readiness for correctional rehabilitation (CVTRQ) was significant, F(1, 64) = 8.90, p = .004, η p 2 = .12, 95% CI [.01, .27]. The simple main effect of time was only significant for the discussion condition, F(1, 21) = 11.04, p = .003, and a consistent result was obtained using post hoc dependent samples tests, with only the discussion condition yielding a significant result, V = 2.74, p = .002, r = .65, 95% CI [.46, .87]. While the main effect for condition was not significant, F(2, 64) = 2.09, p = .13, η p 2 = .06, 95% CI [0, .18], the simple main effect was significant at post, F(2, 64) = 4.16, p = .02, with the discussion condition yielding a significantly higher CVTRQ score than the none–minimal condition, p = .02, MD = 6.76, 95% CI [0.93, 12.59]. Independent samples post hoc effects at post were significant only for the discussion condition over the none–minimal condition, W = 4.97, p = .01, r = .39, 95% CI [.12, .66], and form condition, W = 5.00, p = .05, r = .31, 95% CI [.03, .59], respectively. There was no significant interaction effect between condition and time, F(2, 64) = 2.31, p = .11, η p 2 = .07, 95% CI [0, .19].
The median feedback helpfulness (FHS) scores for the form and discussion conditions were significantly higher than the mid-point of the measure (15), and these effects were large, form: V = 5.20, p = .001, r = .76, 95% CI [.59, .93]; discussion: V = 5.53, p = .001, r = .87, 95% CI [.82, .91]. Although FHS scores did not significantly differ between the form and discussion conditions, there was a trend in favor of the discussion condition, W = 5.06, p = .07, r = .28, 95% CI [.00, .57].
Exploratory Hypotheses: Feedback Condition, Postfeedback Improvements, and Risk Would Be Associated With Institutional Conduct and Recidivism
The conditions did not significantly differ in institutional conduct postparticipation, Kruskal–Wallis χ2 (2, N = 67) = .31, p = .86, ε2 = .00, 95% CI [0, .04]. However, there were significant trends when individually examining merits, Kruskal–Wallis χ2 (2, N = 67) = 6.16, p = .05, ε2 = .09, 95% CI [0, .25], and demerits, χ2(2, N = 67) = 6.20, p = .05, ε2 = .09, 95% CI [0, .21], respectively. Post hoc comparisons revealed that control participants had significantly more merits than discussion participants, W = 5.91, p = .02, r = .34, 95% CI [.08, .59], whereas the discussion condition had significantly fewer demerits than the control condition, W = 5.92, p = .01, r = −.36, 95% CI [−.62, −.11]. The three conditions did not differ in rearrest or halfway house return, χ2 (2, N = 67) = 2.66, p = .26, V = .20, 95% CI [.17, .45]. Differences in outcomes were not observed among feedback participants who evidenced increased motivation for change on the URICA, institutional conduct: W = 5.22, p = .44, r = −.12, 95% CI [−.41, .19]; rearrest or halfway house return: χ2 (1, N = 43) = .01, p = .91, r = .02, 95% CI [−0.27, 0.31]; nor increased readiness for correctional rehabilitation on the CVTRQ, institutional conduct: W = 5.55, p = .50, r = .11, 95% CI [−.19, .40]; rearrest or halfway house return: χ2 (1, N = 43) = 1.96, p = .16, r = .21, 95% CI [−.09, .48].
Participants showed wide variability in their self-appraisals of risk and tended to endorse the presence of about four of the Central Eight risk factors. However, the low retest reliability estimates for RNPS scores among none–minimal participants suggested that participants’ risk–needs self-perceptions were unstable, and influenced by factors other than feedback condition. LS/CMI Total score was not related to intuitional conduct, ρ = −.15, p = .17, 95% CI [−.36, .07], though there was a significant trend for demerits only, ρ = .22, p = .05, 95% CI [.00, .41]. However, LS/CMI Total score was inversely related to recidivism, ρ pb = −.22, p = .05, 95% CI [−.41, .00], although this was only a trend after controlling recidivism by time at risk, semipartial ρ rb = −.16, p = .07, 95% CI [−.39, .04]. These results diminished the value of conducting predictive analyses.
Discussion
As hypothesized, receipt of risk–needs assessment feedback, and particularly highly structured discussion-based feedback, was associated with increased motivation for change. Tentative support was also found for the hypothesized increase in readiness for correctional treatment following feedback, again favoring the discussion condition. Treatment readiness is theoretically quite broad (e.g., Ward et al., 2004), with motivation only one of several influencing factors. However, the CVTRQ focuses on person-level factors rather than environmental factors. Thus, the roughly similar results for the CVTRQ and URICA, consistent with prior observations of associations between the CVTRQ and different stage of change measures (Casey et al., 2007; Day et al., 2009), suggest that these two instruments measure partially overlapping person-level constructs.
While all three study conditions started and ended within the contemplation stage of change on the URICA, the discussion group was closer to the preparation–action cutoff score at post. The size of this effect was comparable to that observed by Anstiss et al. (2011), who measured stage of change using a different measure before and after participation in a four- to five-session MI-based intervention. The stylistic and content differences between the two feedback conditions may have accounted for the superior gains observed among discussion participants. Both feedback conditions used standardized and personally tailored forms to convey information about risk–needs assessment results and their meaning and import. However, the discussion condition also employed a standardized script and was of lengthier duration to involve more psychoeducation (e.g., analogies, repetition) and attention to motivation enhancement strategies (e.g., elucidation, validation, flexibility, supporting strengths, and self-efficacy).
In contrast, the experimental RNPS measure did not evidence adequate retest reliability to warrant testing of the hypothesized effect of feedback on evaluator–participant concordance, nor the predictive utility of self-perceived risk needs. It is unclear whether the unreliable RNPS scores reflected measurement error or unstable participant self-perceptions (e.g., limited insight). If the latter, more intensive feedback or other preparatory interventions may be necessary if an early goal of correctional rehabilitation is client buy-in to the treatment targets suggested by evaluators risk–needs assessments. While the RNPS was selected due to a measure development objective secondary to this study, had pilot testing occurred, the need to instead opt for an already validated self-report measure of criminogenic risk needs (e.g., Self-Appraisal Questionnaire; Loza, 2005) may have been apparent.
As hypothesized, participants rated both feedback formats favorably. Participants slightly disagreed with only one thing: that the feedback told them things about themselves that they did not already know. While this is possibly inconsistent with the low evaluator–client concordance observed at baseline, an alternative interpretation is that participants may have some intuitive appreciation of a risk–needs case conceptualization. Indeed, this is suggested by the medium- to high-risk sample’s tendency to endorse several criminogenic needs as being applicable to themselves, both before and after feedback. This, in turn, may be promising for yielding mutually agreeable service plans (i.e., persons in custody tend to acknowledge that they have issues for treatment).
Contrary to our hypothesis, we did not find support for receipt of feedback or postfeedback gains having effects on institutional conduct or recidivism, beyond some modest, inconsistent group effects when positive and negative institutional conduct was examined separately. A more intensive feedback service (e.g., several sessions and maintenance sessions), or one focused on institutional functioning, may be necessary to influence external behavior. Also contrary to our hypothesis, the LS/CMI did not evidence predictive utility for institutional conduct or recidivism, except when demerits were examined separate from merits. The lack of an association between the LS/CMI and community recidivism raises questions about the quality of the evaluators’ LS/CMI ratings, despite them having been trained and having used collateral records, interview, and supplemental testing; and the impact on recidivism of participants having had been involved in a protracted process of closely supervised reentry. Regarding the latter, the follow-up period may not have been long enough to adequately capture rearrest if participants’ illicit conduct tended to be dealt with via community supervision violations—data which were not available for this study.
The mixed support for the aforementioned hypotheses is consistent with findings from other evaluations of correctional pretreatment motivation enhancement and feedback programs. In contrast to the promising effects for instrumental or process outcomes (Austin et al., 2011; Harper & Hardy, 2000; Kistenmacher & Weiss, 2008), null effects on recidivism have been observed (Campbell et al., 2014; Troquete et al., 2013; Walters et al., 2010).
Study Limitations
There were several limitations that may have impacted the internal validity of the study. Concerning the independent variable of study condition, the extent to which interpersonal variables, such as attention alone, accounted for observed effects is unclear. Feedback sessions were not recorded, preventing assessment of the extent to which experimenter bias manifested itself and the consistency and quality of the feedback across participants and conditions. The amount of experimental separation between the form and discussion conditions was not as wide as it could have been, although this was by design. In particular, the discussion condition differed from the form condition both in format (required discussion and using a script) and amount of information conveyed, making unclear whether observed effects were attributable to format or information amount. Moreover, some of the control participants received minimal feedback (and how many did was not documented), such that there was no true control condition, but rather only a quasi-control condition, which may have further obscured effects.
Regarding dependent variables, it was not possible to oversee the staff-administered LS/CMI assessments or the documentation of participant merits and demerits by facility staff. Two of the five measures used in this study were novel, and three slightly different versions of one of these measures were administered. The adjustments to the RNPS may have impacted the reliability of measured self-perceived risk–needs. Moreover, self-awareness regarding risk–needs were elicited using differently worded prompts than other studies have used, and these prompts omitted certain information (e.g., a specified time frame to which to limit the prediction, such as months, or a prompt to focus on more specific outcomes, such as rule infractions at the facility). Also, the measure of correctional treatment readiness that was used, like other available readiness measures, focuses exclusively on internal characteristics, thereby not accounting for external (environmental) factors, which are more difficult to measure and were beyond the scope of this study (Casey et al., 2007). Lower-than-expected recidivism rates were also observed (cf. Department of Corrections, State Parole Board, & Juvenile Justice Commission, n.d.), and some recidivism indicators were unavailable (e.g., self-report; technical violations; administrative return to a correctional facility other than a privately operated reentry assessment center, such as prison). Moreover, treatment engagement (e.g., attendance and attrition rates and quality of participation) and reductions in evaluator-rated criminogenic needs subsequent to treatment as usual were not measured, despite their closer conceptual connection to motivation and readiness enhancement strategies than the more indirect ultimate outcomes that were examined.
As for power, this study involved a fairly small sample size with some uneven attrition among conditions. This prompted the decision to forego a multiple-comparisons correction. It also may have resulted in insufficient power to detect an interaction effect—that is, of the magnitude observed versus anticipated a priori—for the CVTRQ. Moreover, the extent to which assumptions for various statistical tests were met by the data was variable, often requiring the use of less-powerful nonparametric tests.
Finally, the sample presented limits with respect to external validity. Although the sample appeared comparable to the state’s population of persons who were imprisoned with respect to several demographic characteristics, generalizability was hindered by the exclusive focus on a population undergoing prison reentry (versus other justice-involved populations), and the lack of women and few low or very high-risk cases in the sample.
Implications and Future Directions
Findings from this study suggest that providing RNR assessment feedback can increase motivation for change and possibly also readiness for correctional treatment, and that persons in custody regard such a service favorably. While these types of effects may be necessary for establishing a productive therapeutic alliance, they may not be sufficient if a promising responsivity prognosis is partially defined as a stable, mutually agreed to profile of criminogenic risk and needs, and ongoing motivation for behavior change and readiness for correctional rehabilitation. Repeated collaborative and conversational feedback sessions based on valid assessments may be necessary to persuade persons who are justice-involved to adopt their results as an accurate portrayal of their risk–needs, and conversely, to persuade evaluators that some of their initial risk–needs opinions may need revision. Similarly, ongoing feedback sessions will likely be necessary to maintain the stability of relevant self-perceptions and motivation and readiness for correctional rehabilitation.
Thus, providers and agencies seeking to incorporate feedback systematically into correctional rehabilitation services may obtain the best effects if feedback sessions are designed as part of the assessment process, as a pretreatment service, and as an ongoing parallel service to primary interventions. More intensive, involved, and coordinated feedback services might include assessment and treatment staff routinely and systematically collaborating on treatment planning, the provision of more pretreatment feedback sessions, the provision of more preparatory psychoeducational materials, periodic reassessment of clients’ RNR factors, and periodic review and updating of case conceptualizations and intervention plans with clients. Use of validated self-report risk assessment tools is recommended, in addition to attending to external readiness factors (Duriez et al., 2018) and implementation issues concerning validated evaluator-rated risk–needs assessment tools (Baird, 2009).
Future research could help to determine which pretreatment service components are necessary to produce improvements in various outcomes, and whether early services can be enhanced to impact ultimate outcomes rather than just process–instrumental variables (e.g., via increased coordination with primary interventions, intensity, or repetition). To do so, future studies would ideally measure nonspecific feedback factors (e.g., multiple providers, feedback without human contact, and active placebo); assessment and feedback implementation integrity; and a wide range of instrumental (e.g., feedback buy-in; primary intervention attendance, participation, and attrition); and ultimate outcomes (e.g., change in risk–needs and types of recidivism indicators). Multiwave designs (e.g., pretreatment interventions, primary treatment, reentry, and unqualified release) would further this line of investigation. Use of large samples, multiple samples, and longer follow-up periods (e.g., 2–5 years) would also be ideal.
Additional research on self-perceived risk–needs is also warranted. Few studies have compared multiple risk–needs self-perceptions measures against each other, to an evaluator-scored tool, or across different types of samples (e.g., corrections and forensic mental health, adult and juvenile). Future comparative and incremental validity studies would help clarify the mixed findings in the literature concerning the utility of (and best methods for ascertaining) self-reported risk–needs, and the import of consistency with evaluator opinions. Moreover, future studies could help to clarify whether self-perceptions are a type of criminogenic cognition, a component of other specific responsivity factors (e.g., motivation, readiness, and denial–minimization), or distinct factors (e.g., problem recognition and outcome expectancy).
Ultimately, despite limitations in the underlying research base, RNR assessment feedback is already recommended practice, as is attending to specific responsivity factors (Andrews et al., 2011). Predictive validity considerations aside, eliciting self-perceived risk–needs and providing feedback is likely to be useful for both pretreatment and treatment purposes. It can help to facilitate agreed-upon treatment targets and service plans, individualize programming, and improve and maintain treatment-relevant understandings. The results of this study suggest that risk–needs self-perceptions elicited via face-valid means are highly unstable that motivation and readiness may increase in the short-term following receipt of feedback and that feedback will be regarded favorably by clients. However, as this study also evidences, adding to the achievement and maintenance of sufficient improvements in instrumental and ultimate outcomes in correctional rehabilitation via the use of feedback will likely require such feedback to be collaborative, valid, comprehensive, dynamic, and ongoing.
Footnotes
Acknowledgements
We thank employees at the study facility and the New Jersey Department of Corrections for access to participants.
Some of the data in this article were earlier presented in March 2014 and March 2016 at the annual meetings of the American Psychology-Law Society in New Orleans, Louisiana, and San Diego, California, respectively.
This research was supported by funding from the American Psychology-Law Society Grants-in-Aid Committee. At the time of data collection, the first author was affiliated with Drexel University.