
Abstract
We conducted an online national survey to examine how undergraduate health psychology is taught, offer information about course design and content, and provide a needs analysis. Health psychology instructors (N = 126) answered questions about course format, teaching tools, importance of covering specific topics, and needed resources. A principal components analysis of topic importance ratings revealed five domains: chronic illness, stress and adjustment processes, health psychology in practice, health behavior change, and basics and background. Participants noted that health disparities were not sufficiently addressed in textbooks. A need for integrating digital media and class activities as teaching tools was apparent. Although the number of health psychology courses has increased, there is some inconsistency in how the subject is taught and a clear need for teaching resources.
Near 70% of U.S. psychology departments offer a course in health psychology (Norcross et al., 2016). Health psychology is featured in recent introductory psychology textbooks (e.g., Griggs, 2014) and rated as one of the most important and interesting topics covered in introductory psychology (McCann, Immel, Kadah-Ammeter, & Adelson, 2016), a course taken by approximately 1.5 million students a year (Gurung et al., 2016). Although health psychology courses are becoming more prevalent, there is limited information on what content should be covered (Brack, Kesitilwe, & Ware, 2010; Gurung & Rittenhouse, 2015). We extend and update past findings with a much-needed survey on the nature of this important psychology elective.
Corresponding to the emergence of the Society for Health Psychology (SfHP; Division 38 of the American Psychological Association [APA]), DiMatteo and Friedman (1982) developed a model course in social psychology and health in the early 1980s. The course focused largely on the aspects of the patient role, patient–physician communication, adherence to medical regimens, illness, the family, and the process of dying. In 2016, approximately 10 undergraduate health psychology textbooks are being used in classrooms across North America, many having multiple editions.
The past decades have seen an increase in the teaching of health psychology at higher education institutions (Dunn et al., 2010). In 2014, 69% of undergraduate psychology programs offered a health psychology course (Norcross et al., 2016) compared to 48% in 2005 (Stoloff et al., 2010) and less than 26% in the previous decade (Perlman & McCann, 1999). A review of 300 university catalogs showed the most common topics (with percentage of the sample who taught it) included the biopsychosocial model (93%), chronic illnesses (90%), adherence (87%), and behavior change (80%; Brack et al., 2010). Brack et al. also examined 30 syllabi and found most instructors used lecture (97%), discussion (87%), and video (77%) to provide information and assessed student progress using writing assignments (97%), examinations (97%), and student presentations (73%).
There is limited information on learning outcomes. In one of the sole studies on learning outcomes in health psychology, Gurung and Rittenhouse (2015) randomly sampled course syllabi and conducted a national review of student learning objectives in health psychology courses. Examining 50 syllabi from different universities, the authors found 13 major themes. In general, syllabi contained specific learning outcomes relating to a wide range of topics. Whereas many learning objectives were applicable to any psychology course (e.g., critical thinking, general learning, terms and concepts, interpreting research, and the scientific method), a number of learning objectives were specific to health psychology (e.g., health-related professions, roles of psychosocial constructs, biopsychosocial model, patterns of health behavior, and personal health).
But how are instructors organizing and designing their courses? What content is critical for a health psychology course according to those teaching it? Educators in the vibrant and dynamic discipline of health psychology and those who teach about health psychology in introductory psychology courses need to have a sound sense of the state of education in the field. Recent work on this topic has been limited to small (≤50) sample sizes (Brack et al., 2010; Gurung & Rittenhouse, 2015). To capture a more detailed, in-depth picture, we conducted an online national survey to gather information on how and by whom health psychology is taught, offer information about course design and content, and provide a needs analysis that can serve future health psychology instructors.
Method
Procedure
Electronic mail invitations to complete an online survey were sent to faculty using a variety of listservs (e.g., Division 38 and Division 2 of APA) and Facebook group pages (e.g., Division 2) from March to May 2016. We also sent invitations to the 61 area department heads, chairs, or faculty at health or clinical health psychology programs across the United States listed on Division 38 (SfHP) webpage of PhD programs in health psychology (https://societyforhealthpsychology.org/training/programs/). To be eligible, participants had to have taught a health psychology course at least once. The survey took approximately 10–20 min to complete.
Materials
The survey contained 26 questions; some were quantitative measures and others open-ended questions. Participants provided information on the content and organization of the course, their education, rank and teaching experience, the method of assessment and evaluation, use of teaching tools in addition to textbooks, and additional teaching resources they would need or want.
Background information
Instructors were asked to indicate their gender, rank (graduate student, adjunct lecturer, assistant professor, associate professor, or full professor), area in which they received their PhD (social, clinical, counseling, developmental, experimental, and other), and the number of years they have been teaching health psychology. We also asked how many health psychology courses were offered each year in their department and how many undergraduate students each year took an introductory-level course in health psychology.
Course design
Survey respondents were asked whether they used an undergraduate health psychology textbook and if they organized their course by topic, illness, or both. On a 10-point scale, respondents also answered how many times they used each of the following teaching resources in their course: guest speakers, journal articles, social media links, debates, exams, discussion of media, or news articles. To capture course grade breakdown, health psychology instructors described what percentage of the overall grade was assigned to the following evaluation methods (if applicable): papers, exams, participation, presentation, behavior change paper, blogs, and other.
We also asked about the importance of teaching 25 topics (e.g., health behavior change, chronic illness, research methods, coping, stress) within a health psychology course. The list was developed by examining current health psychology textbooks, handbooks, and a convenience sample of syllabi. Respondents indicated the importance of including a particular topic using a 1 (strongly disagree) to 5 (strongly agree) scale.
Needs assessment
To assess needs of instructors with respect to content, tools, and/or resources, we asked open-ended questions regarding what topics participants felt were missing from health psychology textbooks and what resources they would like to see on the SfHP webpage.
Results
One hundred twenty-six instructors of health psychology, predominantly women (71%), completed the online survey. There was wide variation in the length of time respondents had been teaching an undergraduate health psychology course, ranging from less than a year to 35 years (M = 8.37 years, standard deviation [SD] = 8.85, Mdn = 5.00). The range also varied for teaching at the master’s and doctoral level: Participants had been teaching at the master’s level for 3.94 years (SD = 7.76) and the doctoral level for 5.83 years (SD = 8.87). Close to 20% of the sample could be labeled as novice teachers, having taught health psychology for less than a year, but others had been teaching health psychology since the inception of the field. Respondents were at all academic ranks: full (37%), associate (21%), and assistant professors (25%) as well as graduate student and adjunct lecturers (18%). Participants had been trained in the following areas of psychology: clinical (42%), social (23%), experimental (12%), counseling (8%), developmental (1%), and other (14%); 18 respondents did not provide any information about their training area. On average, participants reported that approximately 2.98 (SD = 2.3) health psychology courses were offered in their respective departments. There was wide variation in the number of students enrolled in an introductory health psychology course over the academic year, ranging from 4 to 900 students (M = 142.62, SD = 178.12, Mdn = 60.00).
Course Design
In the early days of the field, many texts and handbooks were organized by topic (e.g., coping) and by disease (e.g., diabetes). Almost all of the classes described in our survey were organized by topic only (47%) or by topic and disease (51%); only 3% organized their class by disease alone. The majority of our sample used a health psychology textbook for class (81.7%).
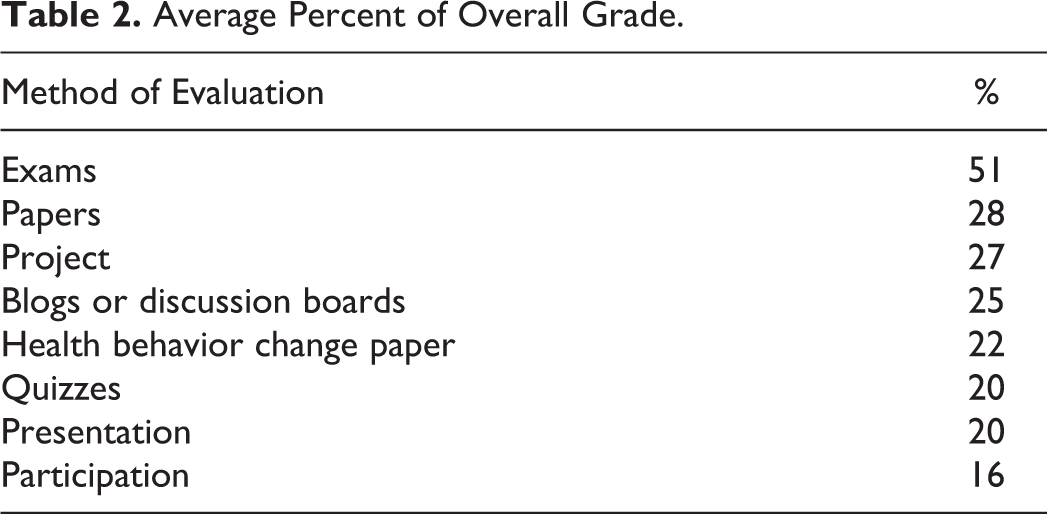
In addition to textbooks, what resources do instructors of health psychology draw upon when teaching? As shown in Table 1, participants reported using journal articles most often followed by video, print, and social media, respectively. In comparison, they used guest speakers and debates infrequently. With respect to evaluation and grade composition, exams constituted the major method of assessment, accounting for approximately 50% of the overall grade. Class participation was the least commonly used method of evaluation, contributing 16% to the overall grade, on average. Papers and projects each accounted for approximately 30% of the overall grade (see Table 2).
Teaching Tools Most Commonly Used in Class.

Average Percent of Overall Grade.
Course Content
A major focus of this article was to determine which content areas instructors of undergraduate health psychology courses consider most important to teach, as a reflection of their importance in the field. As Table 3 displays, there was little variation in importance ratings across the 25 topics presented. Many topics were rated as important or very important; even the lowest ranked topic had a mean rating of 3.5 on a 5-point scale. Eight topics were rated as either important or very important by 96% of the sample: stress, coping, social support, chronic illness, health behavior theories, health behavior change, health disparities, and interventions.
Ratings of the Importance of Topics (Individual Items).
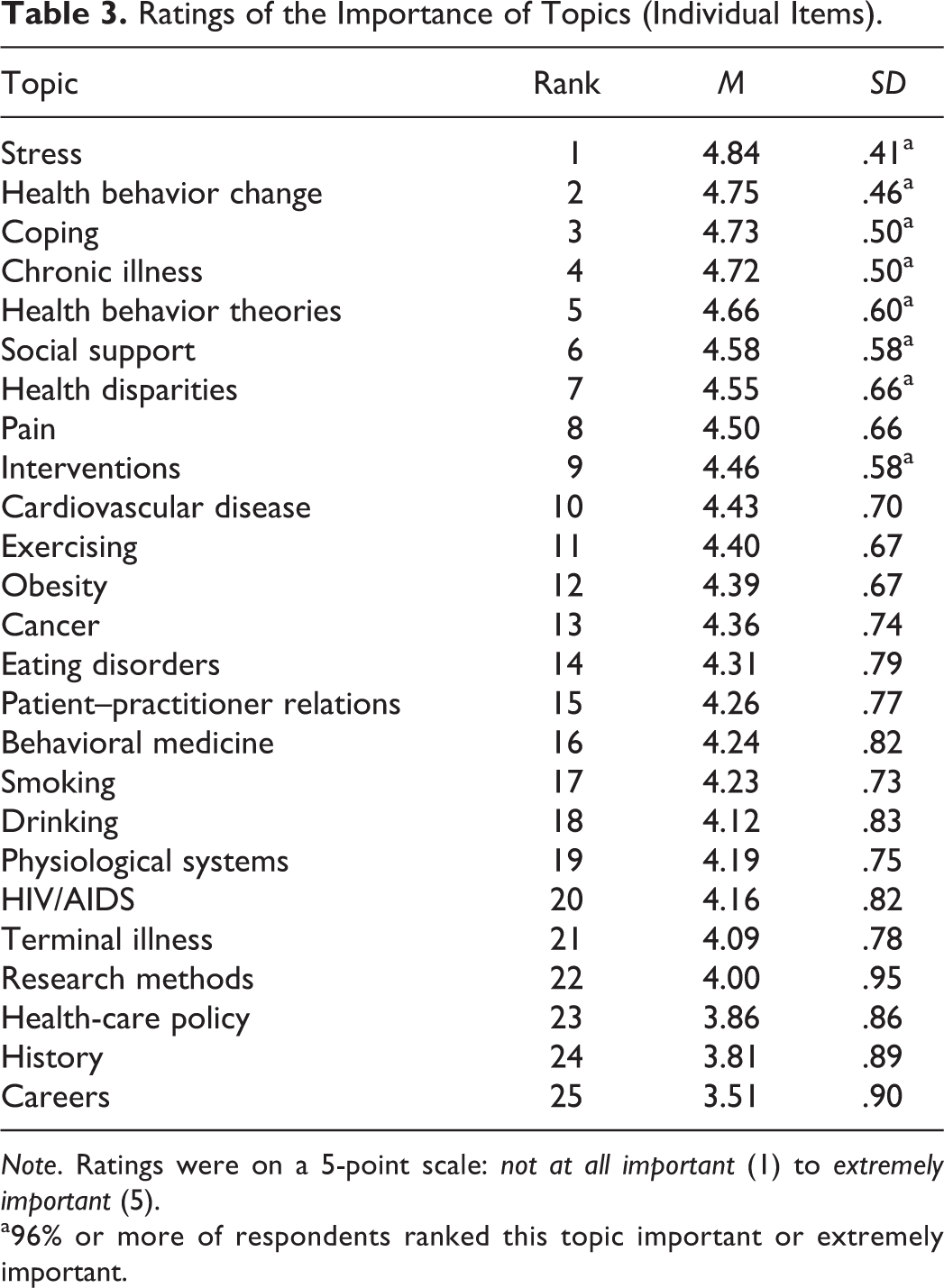
Note. Ratings were on a 5-point scale: not at all important (1) to extremely important (5).
a96% or more of respondents ranked this topic important or extremely important.
As we expected topics to be related thematically, an exploratory principal components analysis was conducted to determine whether there was a smaller set of factors underlying the 25 topics. With the criterion set at eigenvalue >1, seven factors emerged, but an oblique rotation indicated that several items did not load on any factor and many items loaded ≥.40 on more than one factor. A five-factor solution with oblique rotation fit the data well, explaining 58% of the common variance. The factors were labeled: chronic illness, health psychology in practice, stress and adjustment processes, health behavior change, and basics and background. Table 4 presents the items in each factor and their loadings. Scales were created by averaging the items in each factor. The five scales were moderately correlated (mean r = .28; rs ranged from .20 to .31) and internal consistency reliabilities (Cronbach’s α) ranged from .59 (basics and background) to .85 (health behavior change). Using these five scales, we conducted analyses to identify whether characteristics of the instructor and course were related to importance ratings.
Factor Loadings of Course Topics.
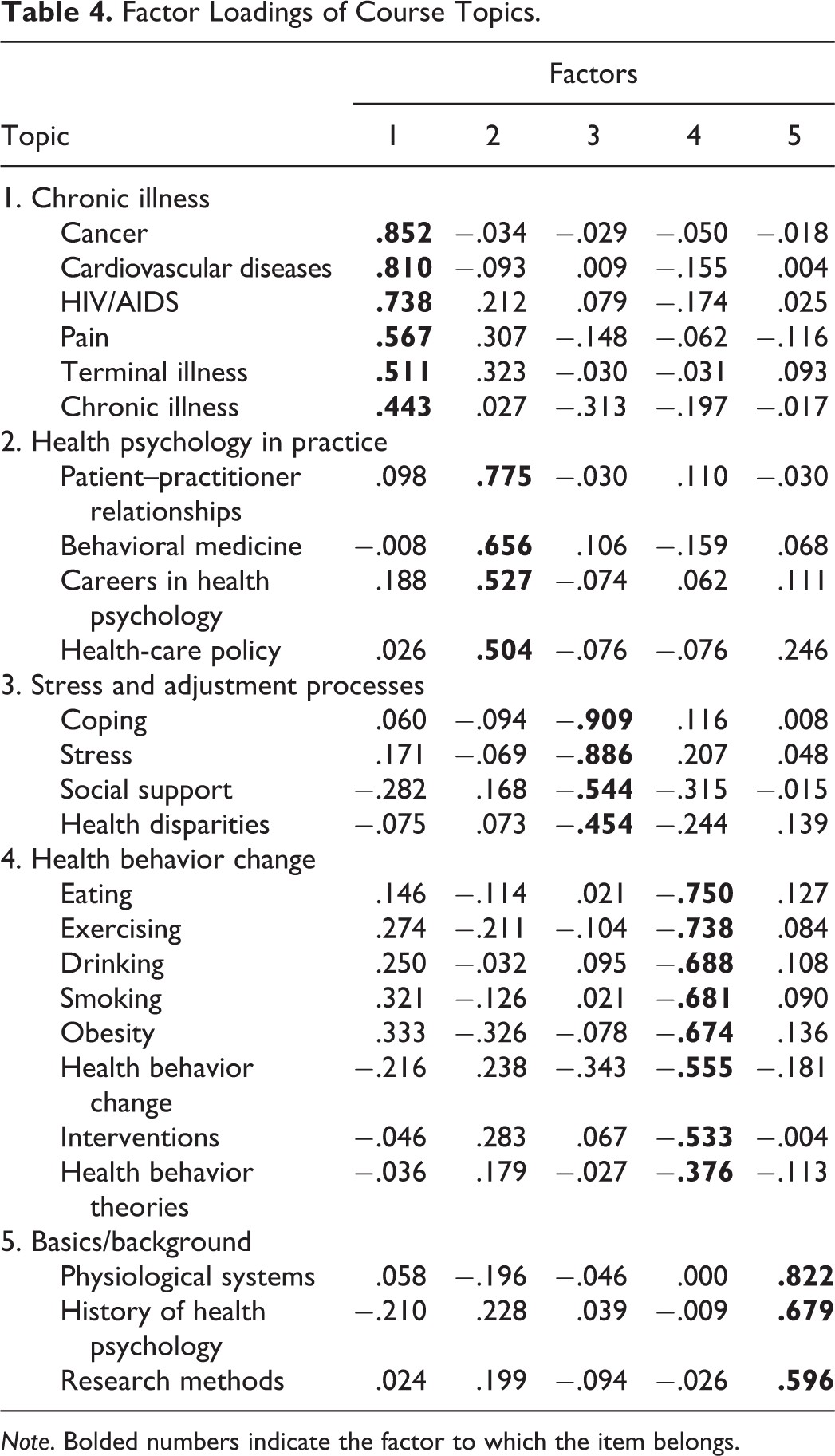
Note. Bolded numbers indicate the factor to which the item belongs.
Academic rank
For these analyses, we combined graduate student and adjunct instructors into one category. A univariate analysis of variance showed that academic rank was related to only one of the five importance factors: background and basics, F(3, 112) = 4.71, p = .004, η2 = .11. Specifically, assistant professors were less likely to consider basics and background topics important (M = 3.67, SD = .69) compared to adjunct professors/instructors/graduate student instructors (M = 4.10, SD = .77), associate professors (M = 4.01, SD = .52), or full professors (M = 4.22, SD = .53), although Tukey’s post hoc analyses revealed that only the difference between assistant professors and full professors was significant (p = .002, 95% CI [3.41, 3.92]).
Academic training
We created three groups for analyses: experimental psychology, clinical counseling, and social developmental. Significant differences were found for two of the five importance scales: disease, F(2, 97) = 3.44, p = .04, and health behavior change, F(2, 97) = 3.14, p = .05, η2 = .06. Tukey’s post hoc analyses revealed that instructors trained in clinical or counseling psychology (M = 4.49, SD = .43) were likely to consider diseases more important to cover than those trained in social or developmental psychology (M = 4.21, SD = .65), p = .04. They also considered health behavior change (M = 4.50, SD = .41) to be more important compared to those trained in experimental psychology (M = 4.16, SD = .44), p = .048.
Number of enrolled students
Because of the wide range in number of students who took health psychology classes, we created a three-group categorical variable for analyses: less than or equal to 50 students; 51–100; 101 or more. There was a trend for one importance factor: basics and background, F(2, 93) = 2.91, p = .06, η2 = .06. Participants whose departments had 50 or fewer (M = 3.88, SD = .73) students in health psychology classes were less likely to rate the basics and background domain as important compared to those with 50–100 students (M = 3.98, SD = .56) or greater than those with 100 students in health psychology classes.
Organization of the course
Instructors who organized their class by both topic and disease were more likely to rate chronic illness (M = 4.55, SD = .41) as more important than those who organized their class by topic alone (M = 4.16, SD = .57), t(87) = −4.05, p < .0001, Cohen’s d = .79.
Needs Assessment: Content and Resources
We asked an open-ended question about topics that instructors felt were missing in health psychology textbooks. The frequencies are presented in Table 5. Approximately 30% of respondents described material on health disparities and culture to be missing; this was followed by information on health-care systems, global and public health, and health policy (13%). Approximately 12% of the sample reported that information on sleep, dieting, and nutrition—important aspects of both health behavior change and risk profiles—was lacking. Participants were also asked to report what teaching tools or resources they wished they had (see Table 6). The most cited was digital media resources (e.g., videos, documentaries, movies, and podcasts), but this was reported by less than half (41%) of the sample. Instructors listed in-class activities or demonstrations (32%) and assignments and/or rubrics (21%) as other sought-after resources.
What Is Missing From Health Psychology Textbooks?
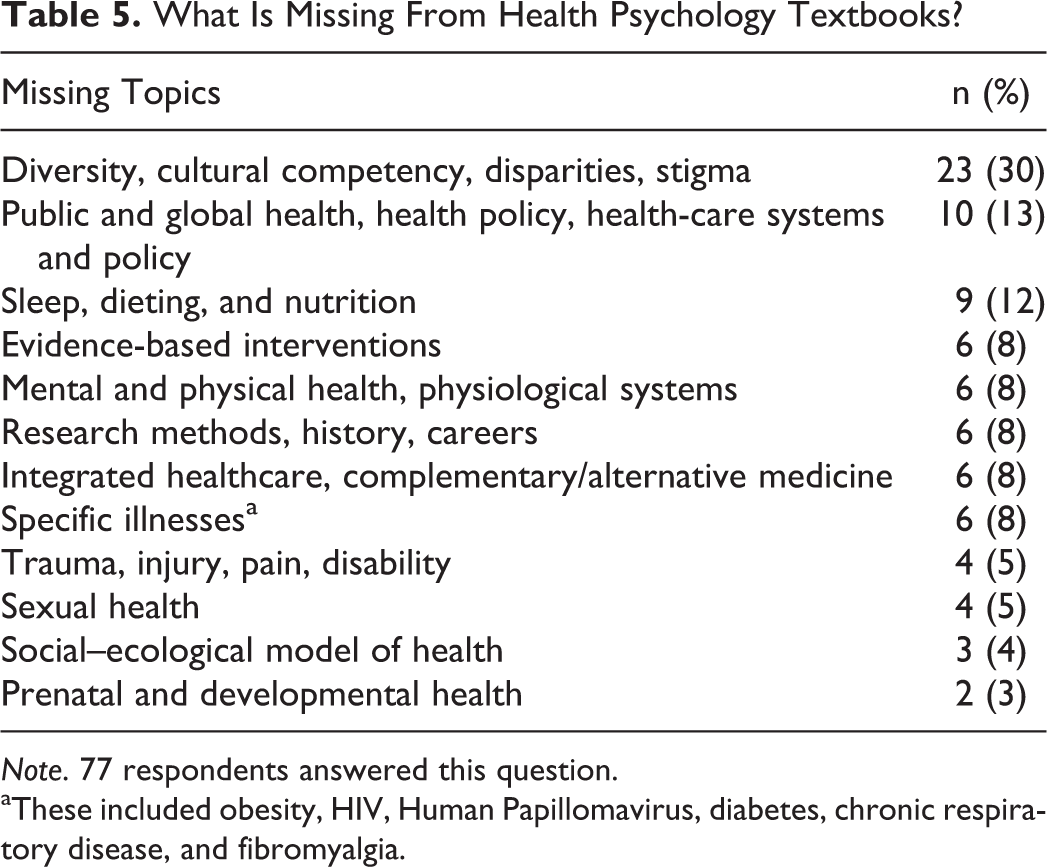
Note. 77 respondents answered this question.
aThese included obesity, HIV, Human Papillomavirus, diabetes, chronic respiratory disease, and fibromyalgia.
What Resources Do Health Psychology Instructors Wish They Had?
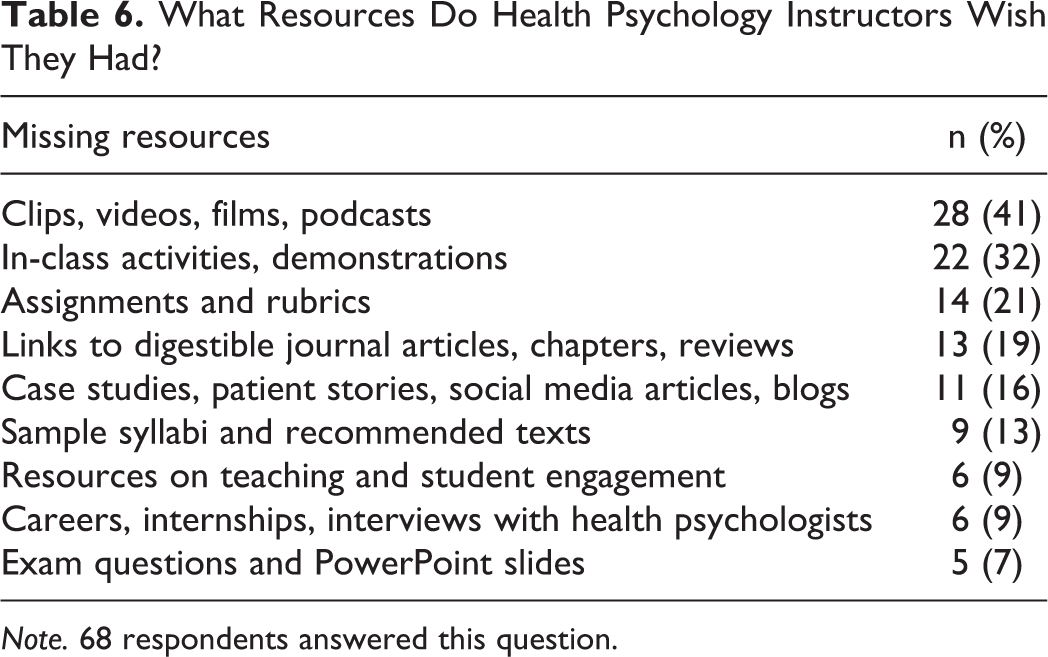
Note. 68 respondents answered this question.
Discussion
As with any course, there is no single way to teach health psychology. Most instructors did not rely solely on a textbook, but used journal articles, videos, newspaper articles, and social media to augment their lessons. We were surprised at the low percentages of instructors who went “outside of the box,” making the subject closer to students by inviting in guest speakers or holding debates on health policy or scientific evidence. For example, the third author of this article has a primary care physician come to class to discuss issues of patient–physician communication and how cultural barriers affect medication adherence, whereas both the first and second authors have cancer survivors speak on issues of coping, support, and survivorship. Student evaluation methods were not different than most undergraduate courses: Papers and exams were the most consistently used methods of evaluation and tended to contribute the majority of points to students’ grades. Quizzes, presentations, and class participation were infrequently used to calculate grades.
Unmet Needs
Our study revealed a number of unmet needs that went beyond the standard resources of textbook exam item banks and PowerPoint presentations. Over 40% of respondents noted a need for video, films, or podcasts to expand on concepts taught in the textbook or the lecture. Approximately one third reported a need for class activities or demonstrations. Reading through the responses, one concludes that health psychology instructors are requesting tools to foster student engagement with course content. The SfHP is beginning to address this need with materials on their education and training webpage, but it is clear that in the 21st century, one cannot teach by textbook alone. The Society for the Teaching of Psychology (Division 2 of APA) has some materials on its website to address this (see http://teachpsych.org/page-1603066); however, one quickly notes the absence of a health psychology category. Health psychology instructors could clearly benefit from a curated list of helpful links to videos, activities, or assignments that are content-specific.
The “Ideal” Health Psychology Class—or Is There One?
There is no scholarship of teaching and learning that compares difference whether different course design is associated with different levels of learning. Do students in a course with a textbook learn material better than students in a course with only primary source material? Do students tested with multiple-choice exams and short answers learn material in the same way as students who are tested in different ways? Our search of the literature on health psychology revealed a significant gap in knowledge, and one impetus for this article was to stimulate research on optimal course design. More instructors need to assess how their course design and topic selection relates to learning of material.
A clear, even didactic, presentation of both central and peripheral topics in a health psychology course may be helpful for those designing new syllabi. We were surprised that some respondents, particularly assistant professors, rated history or methods as less important topics to cover. Understanding methods such as randomized controlled trials is critical to appreciating how behavioral medicine interventions work. Similarly, a working knowledge of how stress affects many organ systems, culminating in allostatic load (McEwen, 2004), is essential for understanding the biopsychosocial model that has been the guiding paradigm of the field since its inception. Although each professor has the freedom to design her own syllabus, our data suggest that there are cornerstone topics that must be covered for students to have a basic knowledge of the field, for example, models and strategies for health behavior change, stress and coping processes, and chronic illness and adjustment. In this day and age, students would also benefit from being well versed in biobehavioral relationships linking cognition, behavior, and affect, with disease. It is an empirical question as to whether incorporating key topics or a specific sequence of topics will lead to students learning better.
We believe that the teaching of health psychology at the undergraduate level should be evidence based, including theories with empirical support as well as community and policy applications of those theories. Conveying these strengths as well as the central topics within health psychology should be a priority for instructors, including health psychology, as topic introductory psychology courses to create awareness of the field should also be considered.
Does Health Psychology Need a Common Core?
It is difficult to ascertain if health psychology courses have a common core. A cursory examination of textbooks reveals significant overlaps in chapter titles and content, but it is unclear if course content is similarly consistent. Few studies in the teaching of psychology examine course content. In introductory psychology, the cumulative research highlights the variety and inconsistency of topics, leading to the conclusion that students in different institutions, sometimes even within the same institution, are not being exposed to the same content (Homa et al., 2013). This is contrary to recent educational recommendations for commonality of coverage, as typically exists in the introductory courses for science, technology, engineering, and mathematics disciplines.
Common content across health psychology courses provides a singular message to students and the public about what constitutes the field of health psychology. Lack of conceptual and content consistency can also complicate assessment. Whether across instructors or time, at department levels or institutional, assessment necessitates having a consistent, if not standardized experience. Health psychologists may want to consider designing a common assessment tool to benchmark learning in the health psychology courses across institutions.
Our survey findings depict how health psychology is being taught across the United States. Listings of important course topics map closely onto textbook chapters while also suggesting new topics for inclusion (e.g., health disparities; see Tables 3 and 4). The material that was uploaded and attached to the surveys provides a set of exemplars that, once published on the web, can serve as essential resources for novice instructors. We are working with the SfHP to make these resources available on its website (https://societyforhealthpsychology.org). It is clear that the respondents to our survey saw the need for more resources. From a larger perspective, it is also evident that the way the field is seen and taught today is not the same as when it was first taught 30 years ago. Our factor analysis of topics provides an empirical picture of the five main areas that courses are carved into, and it also allows for instructors to ensure they have all health psychology bases covered.
Limitations
The survey was voluntary, so our sample may not be representative of the whole population of doctoral students, adjuncts, and professors who teach health psychology nationally. It is likely that those who responded hold more of an identity of “teacher” or were currently teaching a health psychology course. Even with this caveat, it appeared that younger, less experienced instructors were asking for help with creating more engaging courses with up-to-date content, perhaps because they were the only one at their university to be teaching health psychology. We also did not ask for demographics of the student populations that participants were teaching such as the proportion of psychology majors, premed, or nursing students. It may be that health psychology classes need to be tailored to the student population to make them even more relevant.
The results of this survey present a rich picture of the way health psychology is taught today. As one of the most vibrant areas of psychology, the findings of this survey serve to inform both instructors of health psychology and instructors including health psychology in introductory psychology classes. Most importantly, our findings provide an important benchmark to gauge how this course is taught today, enabling future comparisons for tracking the evolving nature of the field.
Footnotes
Acknowledgments
We thank Patrice Saab, Mary Davis, and Peggy Zoccola for providing helpful input at various stages of the process.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded in part by the Education & Training Council of the Society for Health Psychology (SfHP; Division 38 of the American Psychological Association).