
Abstract
The need for psychosocial intervention programmes to address the negative consequences of the COVID-19 pandemic and its associated lockdown restrictions on the mental health of young people is evident. Using a within subject pretest-posttest design, this study aimed to evaluate the effects of online Cognitive Behavioural Therapy (CBT)-based anxiety and depression management psychoeducation programmes on mental health and coping skills in youth ages 14–20. The Demographic Information Form, Revised Child Anxiety Depression Scale, and KidCope were administered before and after the psychoeducational programme to assess programme outcomes. The results indicate significant decreases in levels of anxiety, significant decreases in avoidance of anxiety-provoking situations and significant increases in coping skills following the online CBT Anxiety Management Psychoeducation Program. A significant decrease in depression scores was noted among the online CBT Depression Management Psychoeducation Program participants. Although these results should be interpreted cautiously due to limitations of the study (e.g., no control group, high attrition), they suggest that psychological prevention or intervention programmes may be beneficial for young people who are physically unable to go to school or who cannot interact face-to-face with social support networks.
Introduction
COVID-19 has developed into an ongoing pandemic since it was first sighted in Wuhan, China in December 2019. As a result, restrictions have been implemented across the world in an attempt to contain the spread of COVID-19. In Turkey, from the onset of the COVID-19 pandemic strict precautionary measures were taken for children and adolescents. According to a report published by the Turkish Science Academy (2020), online education started on March 23, 2020, and a curfew for youth aged 20 and under was enforced from May 6, 2020 (Republic of Turkey Ministry of Interior, 2020). As of June 1, 2020, despite the easing of restrictions and the “new normal”, youth continued their online education and were only allowed to go out at certain hours (Republic of Turkey Ministry of National Education, 2020). This continued until July 1, 2021, until all of the restrictions were completely removed.
Based on Erik Erikson’s (1950) Stages of Psychosocial Development Theory, the impact of not physically attending school or having in-person contact with social support networks is of particular importance from the perspectives of identity development and social relationships. The psychological impact of school closures and prolonged lockdown have led to increased frustration, lack of sleep and difficulty concentrating in children and youth (Golberstein et al., 2020; Wang et al., 2020). Marques de Miranda et al. (2020) documented an increase in depression and anxiety levels in youth during the pandemic and identified social isolation, difficulty with online schooling, lack of motivation and boredom as the main contributors (Sibley et al., 2021). A study conducted in China during the first few months of the pandemic identified 40.4% of 584 youth to be at risk for developing psychological problems due to COVID-19 (Liang et al., 2020), mainly due to social distancing (Cao et al., 2020). Additionally, anxiety rates of 24.9%, depression rates of 19.7% and stress rates of 15.2% were identified among primary and secondary school children in China (Tang et al., 2021). In Germany, low life satisfaction (40.2% of participants aged 7–17) and increased anxiety levels (24% of participants indicating a 10% increase) were reported in comparison to pre-coronavirus levels (Ravens-Sieberer et al., 2021). Increased anxiety symptoms were also observed in Spain with 67.9% of 1,028 child and adolescents aged 6–18 displaying symptoms (Lavigne-Cerván et al., 2021). In a study conducted with 745 adolescents aged 12–18 in Turkey, it was reported that feelings of isolation and anxiety increased due to the closure of schools and quarantine periods, while 58.1% reported an increase in health anxiety (Kılınçel et al., 2020). Similarly, Loades et al. (2020) suggest a relationship between isolation and loneliness and symptoms of depression and anxiety. Other studies also show that social restrictions and isolation due to the pandemic have had a negative impact on the psychological wellness of youth (Gabor et al., 2020; Munasinghe et al., 2020). Together, these findings highlight the increase of psychological problems in youth during the pandemic.
Since the beginning of the COVID-19 pandemic, many mental health professionals have opted to use telemental health and have carried out their work remotely (Jurcik et al., 2021; Perrin et al., 2020; Sharma et al., 2020). As a result, online videoconferencing systems have been used more widely in mental health settings to establish a connection between clients and mental health practitioners and implement interventions (Jurcik et al., 2021; Kalvin et al., 2021; Sharma et al., 2020). Internet-based Cognitive Behavioral Therapy (CBT) consists of structured web pages and related applications containing a series of tasks and homework accompanied with multimedia (Kumar et al., 2017) whereas videoconference-based CBT is carried out in real time with face to face interaction via a videoconference programme (Himle et al., 2006; Kim et al., 2018). In particular, it has been reported that the Zoom videoconferencing system offers an enjoyable and useful method for delivering psychoeducation programmes to treat the anxiety of children with autism spectrum disorder (Kalvin et al., 2021; Shah et al., 2019). Many studies support CBT approaches and techniques due to their efficacy; hence they are frequently used for the treatment of anxiety and depression in youth (Brown et al., 2019; Sclare et al., 2015). A randomized control study (Stice et al., 2008) and some other intervention group programmes (David-Ferdon & Kaslow, 2008; Wignall, 2006) reported that CBT was effective in reducing the level of depression in youth, but the effect of internet-based inverventions against depression symptoms was not significant (Ye et al., 2014). In a systematic literature review, Olsson et al. (2021) reported that children and adolescents with symptoms of anxiety and depression who participated in individual / group CBT interventions reported medium to high treatment satisfaction and all between and within group comparisons revealed CBT to be effective. A CBT programme with online modules was also effective in reducing anxiety levels of adolescences with anxiety disorder (Stjerneklar et al., 2018).
Adolescence is a developmental phase featuring psychological challenges. Therefore, stressful life events experienced during adolescence increase the risk for developing anxiety disorders or depression (Fox et al., 2010; Grant et al., 2004). Besides, Frydenberg et al. (2004) showed that effective coping skills are important to reduce the risk of depression during adolescence. A study that was carried out in China showed that negative coping style is a predictor of depression, anxiety and stress in adolescents (Novak et al., 2021). Therefore, improving effective and positive coping skills are critical to minimize depression and anxiety development in the adolescent period.
Considering social relationships as an important event of Erik Erikson’s (1950) Stages of Psychosocial Development in adolescence, the impact of distancing from social environments due to the pandemic will make intervention and prevention studies targeting this group particularly valuable. However, to the best of our knowledge, until the current study, there was no publication showing any other study about a group-based and videoconferencing psychoeducation programme aimed at young people in order to help them cope with the emerging or increasing distress during COVID-19. Ghosh et al. (2020) indicate psychosocial support during COVID-19 pandemic is needed due to school closure, lack of outdoor and physical activities, sleeping habits, distress, and the development of other psychiatric problems. In addition, a study conducted with 11,000 adolescents by Mansfield et al. (2021) highlighted that school closure during COVID-19 showed the strongest associations with mental health problems and suggested implications for appropriate educational and mental health support. Another recent study drew attention to the importance of the social support for all school communities including students, families, and teachers in terms of coping with stress, anxiety, and depression symptoms (Hatzichristou et al., 2021).
This study aimed to examine the effectiveness of online CBT Anxiety and Depression Management Psychoeducation Programs at minimizing the negative psychological impact of COVID-19 pandemic on Turkish youth aged 14–20, who were subjected to preventive pandemic restrictions during the period of May- June 2020. It was hypothesized that the psychoeducation programmes would be associated with decreases in participants’ anxiety and depression symptoms and increases in their coping skills.
Method
Participants
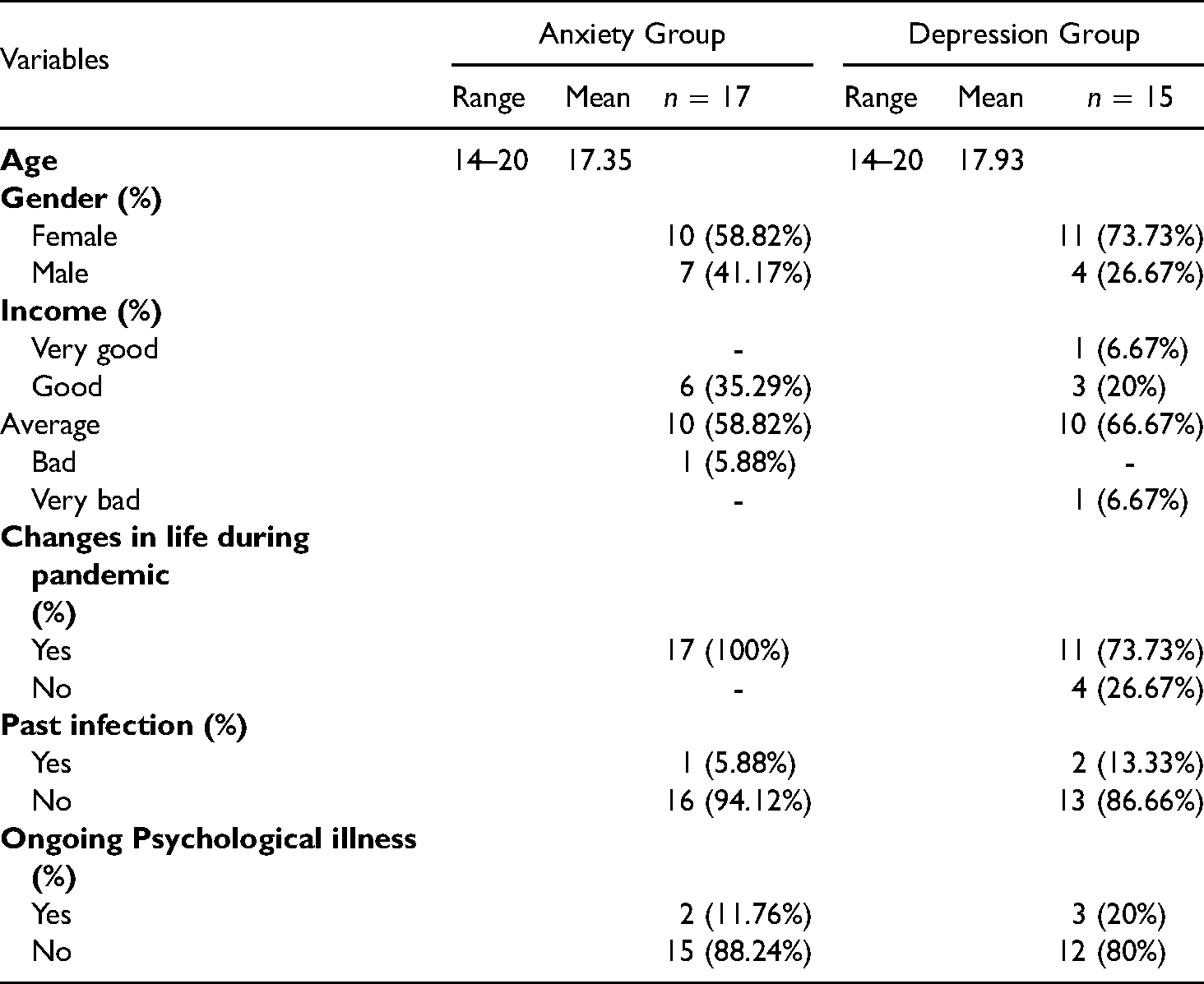
From September to December 2020, 698 participants were recruited from a non-clinical sample through online applications, of which 478 completed the online surveys required for participation in the programme. As home restrictions were enforced for youth aged 20 and under during this time, this group was targeted. In order to form a somewhat homogeneous age group, high school students 14 and over were included. Apart from the age group, the other inclusion criteria included living in Istanbul, Turkey and being able to speak and understand Turkish. Instructional manipulation check (IMC) questions were used to enhance data quality by identifying respondents who were not paying close attention to survey questions. Data were excluded from 60 applicants who were aged above 20, completed the documentation more than once, and/or answered the IMC question incorrectly. A total of 389 applicants were invited to attend the 4-Session Psychoeducation Program provided via the videoconferencing tool Zoom. Written informed consent was obtained from all participants, and parental consent was obtained for participants younger than 18 years of age. Detailed demographic information about participants who attended and completed the online CBT Anxiety and Depression Management Psychoeducation Programs can be found in Table 1.
Demographic information of intervention groups.
Study design and procedure
Initially participants were reached via mailings and social media platforms and surveys were completed by participants online via SurveyMonkey. A within subject pretest-posttest design was utilized to determine the effectiveness of online CBT Psychoeducation Programs during COVID-19 pandemic. Online within subject designs are advantageous for a number of reasons including the need for fewer participants which saves time and can also be seen as economical for participants. Furthermore, within subject designs are more sensitive to the manipulations of the experimental effects which makes them more advantageous statistically (Breakwell et al., 2006).
Initially, the intervention programmes were planned to ensure that participants received psychological support in the area they needed it the most. Thus, applicants were categorized according to their questionnaire scores. However, due to the small number of applicants who consented to participate in the intervention group all were included in the study. Those who accepted this assignment were then assigned to groups, with those whose symptom profile was predominantly depression being included in the depression group and those whose symptom profile was predominately anxiety being included in the anxiety group. To enable interaction within groups and with group leaders the groups were kept relatively small, but keeping in mind dropout rates each group was assigned a maximum of 14 participants. In addition, as promised from the onset, individual psychotherapy was then offered (after the study concluded) to those who expressed their need or desire, and the participants who participated in all sessions had the chance to win a smart watch by participating in the drawing as an incentive.
In total, 4 Anxiety Psychoeducation and 2 Depression Psychoeducation groups were formed and to reduce potential dropout rates, all groups were organized according to the out-of-school time of the participants. Of the 2 Depression Psychoeducation groups, 28 participants attended the initial session, but 15 completed all 4 sessions. Additionally, of the 4 Anxiety Psychoeducation groups, 50 participants attended the initial session while 17 completed all 4 sessions. Each session lasted approximately 90 min in duration. This videoconference-based CBT was developed and implemented under the supervision of one of the authors (VG) who is an internationally accredited trainer and supervisor of CBT. The sessions were conducted under the guidance of 4 specialist psychologists who had received training in at least the basics of CBT and held a MSc in clinical psychology or psychological counselling (age range: 26–46 years, mean age: 31.8 years; professional experience range: 2–23 years; mean experience: 8.3 years). They also received training and supervision regarding implementation of the sessions from the supervisor of this online CBT programme.
In terms of treatment integrity, all sessions were video- recorded and evaluated by the supervisor. In this evaluation, the extent to which the pre-determined content of the session (specified in Tables 2 and 3) was complied with and the proficiency level of the session were evaluated informally, and the therapy practice skills that were missing or needed to be developed were identified and intervened. Although the evaluation results at the end of each session showed that the programme met the expectations in practice and remained faithful to the content, this situation was not analysed quantitatively.
Online cognitive behavioral therapy (CBT) depression management psychoeducation program sessions.
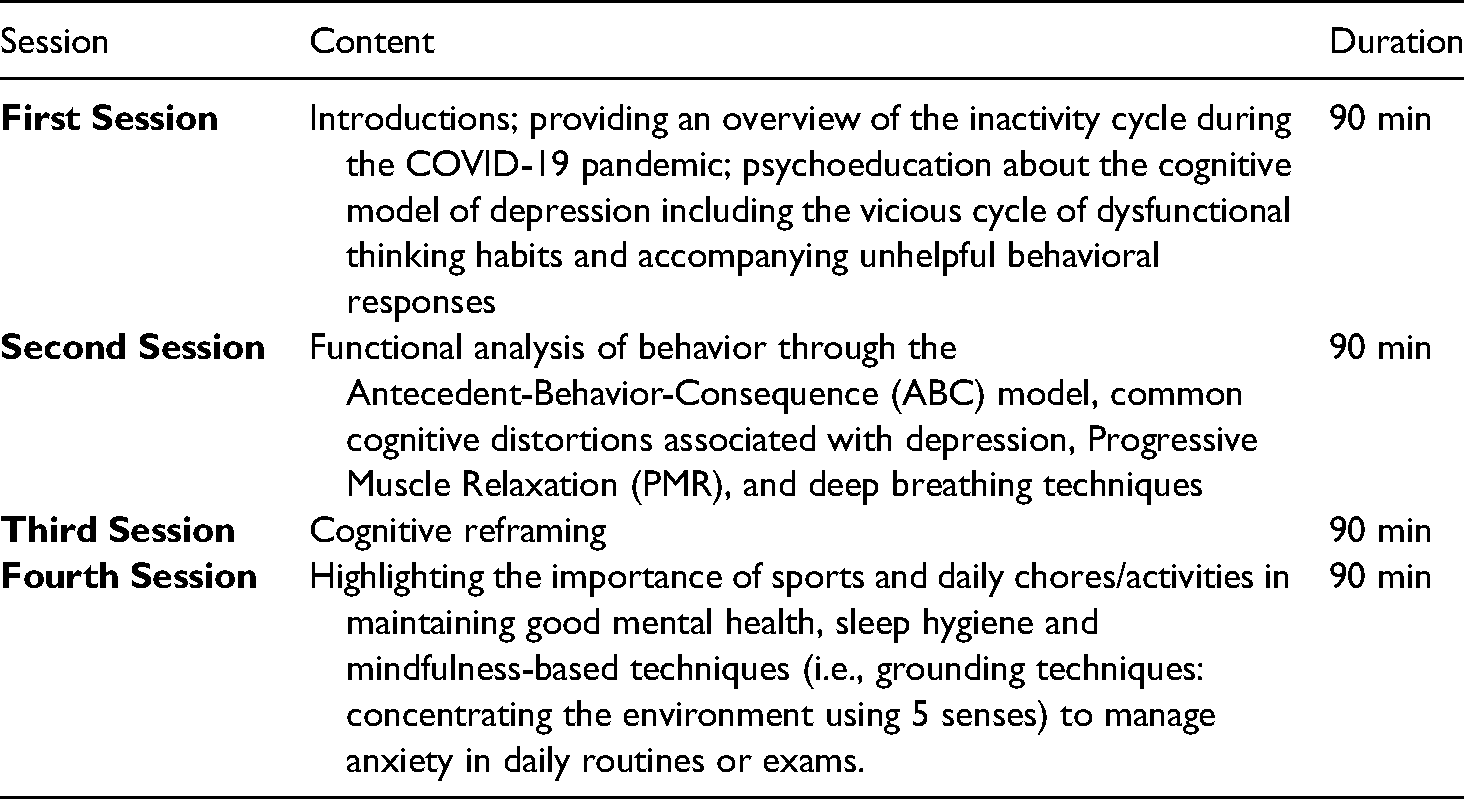
Online cognitive behavioral therapy (CBT) anxiety management psychoeducation program sessions.

Measures
Demographic information form
The demographic information form was developed by the research team. This form comprised of questions pertaining to participants’ age, gender, education, psychiatric status (assessed with the question ‘Do you have ongoing psychiatric illness?’), and whether they had been infected by the COVID-19 (see Table 1).
Primary outcomes
Secondary outcomes
Psychoeducation program sessions
Details about the online Cognitive Behavioral Therapy (CBT) Depression and Anxiety Management Psychoeducation Program sessions are provided in the Table 2 and Table 3.
Statistical analyses
The data were analysed with SPSS 25.0 (IBM Corp., 2017). Preliminary analyses were conducted to determine normality and differences in pretest conditions between depression and anxiety symptoms of the two groups. Due to the small sample size and normality violations, nonparametric tests were used to analyse data. After the psychoeducation programme, Wilcoxon signed rank test was used to compare the differences in anxiety symptoms, depression symptoms, and coping skills of participants at pre- and post-psychoeducation programme.
Results
Wilcoxon signed rank test
Anxiety psychoeducation group
According to the Wilcoxon Signed Rank Test results for the Anxiety Psychoeducation group, adaptive coping strategies increased (T = 55.00, z = 2.87, p = .004, r = .49), while avoidant coping strategies (T = 18.00, z = −1.95, p = .050, r = −.33) and anxiety scores (T = 30.00, z = −2.20, p = .028, r = −.37) decreased. A meaningful difference was not reported in depression scores and maladaptive coping strategies (p > .05, see Table 4).
Comparison of pretest and posttest psychoeducation in anxiety group (n = 17).
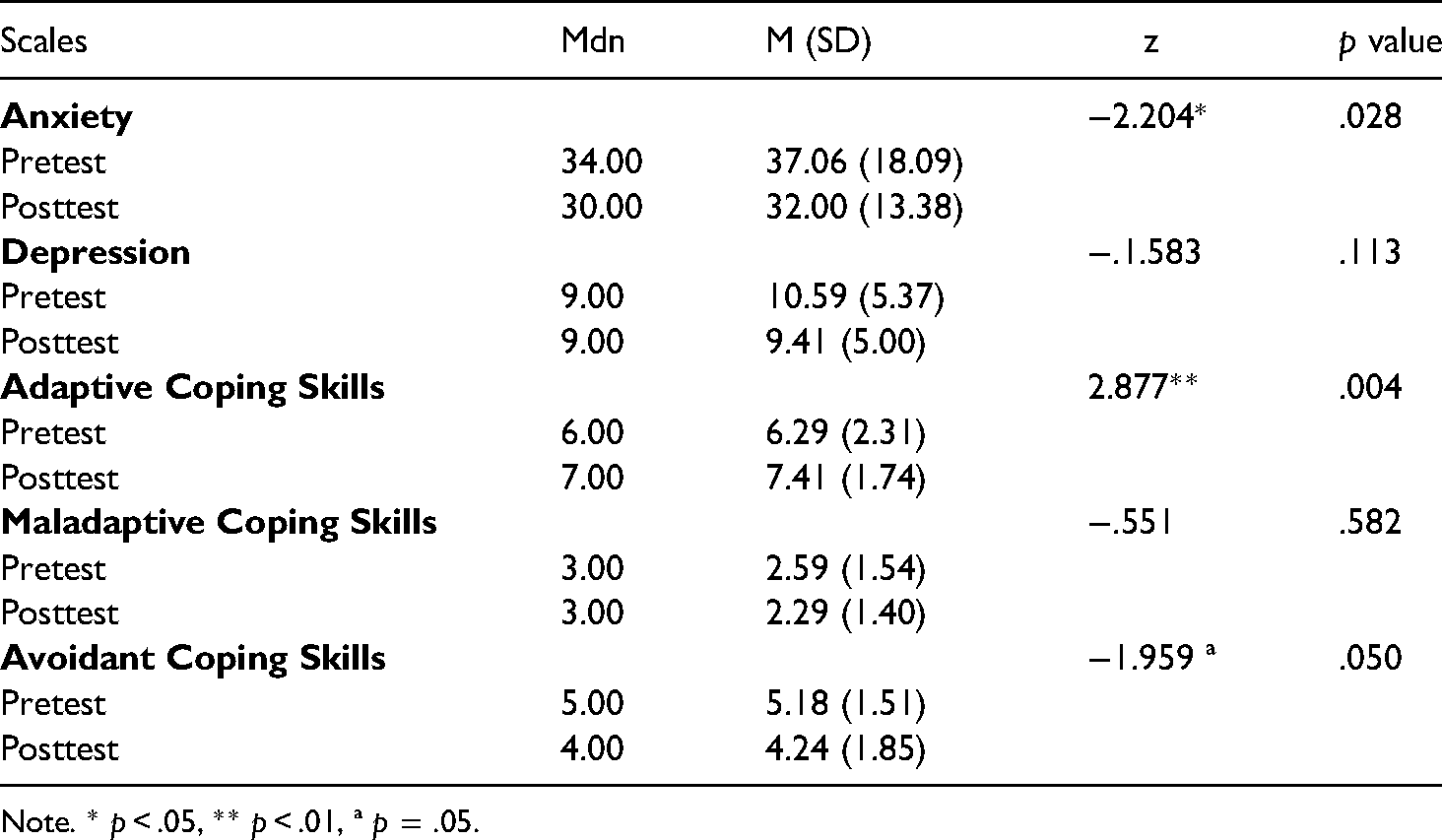
Note. * p < .05, ** p < .01, ª p = .05.
Depression psychoeducation group
For the Depression Psychoeducation group, a significant decrease in depression scores was found (T = 25.00, z = −1.99, p = .046, r = −.36). No changes were noticed in anxiety scores and coping skills (p > .05, see Table 5).
Comparison of pretest and posttest psychoeducation in depression group (n = 15).
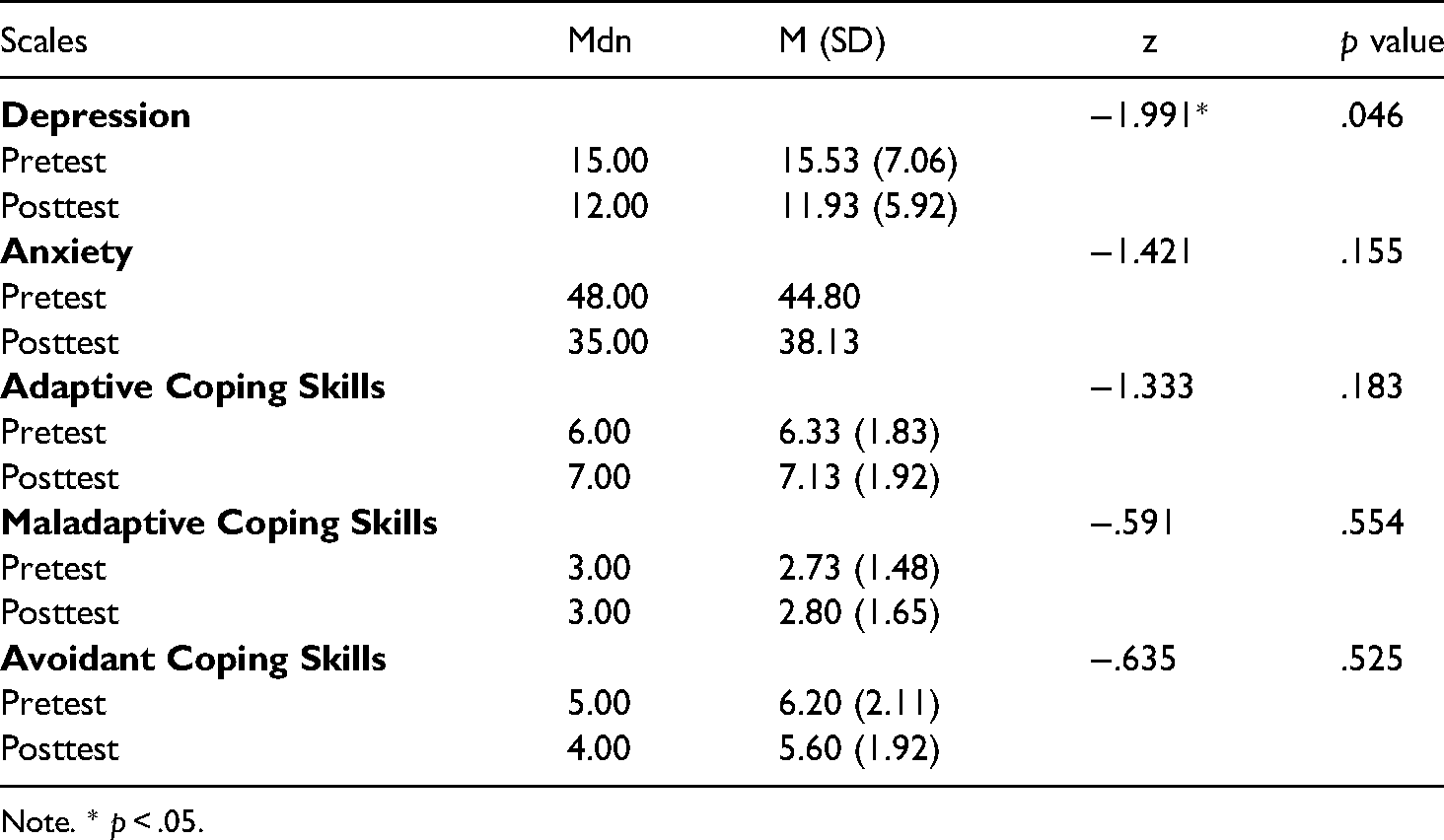
Note. * p < .05.
Discussion
The 4-session online CBT Anxiety and Depression Management Psychoeducation Programs offered during the pandemic seem to be associated with some positive outcomes. When post-test to pre-test results were compared, a reduction in anxiety levels within the anxiety group and similarly a reduction in depression levels within the depression group were observed. Although limitations in the study design (e.g., lack of control group) and sampling (e.g., high attrition) make it impossible to know whether these results are due to the implementation of the programmes, these results are consistent with previous findings using CBT targeting anxiety and depression (Brown et al., 2019; Olsson et al. (2021); Sclare et al., 2015; Wignall, 2006). Our results were also coherent with other studies that were conducted online for youth with anxiety (Stjerneklar et al., 2018), however they were inconsistent with findings for depression (Ye et al., 2014). The depression symptoms were decreased in the present study unlike the results in the meta-analysis of Ye et al. (2014). However, they noted that the therapist involvement was responsible for the effect difference between depression and anxiety studies. Further, they also pointed out that the depression and anxiety were two different disorders in spite of high prevalence of comorbidity. Since psychoeducational approaches in CBT can have a transdiagnostic effect, especially in anxiety spectrum disorders and depression-anxiety axis, we also investigated how anxiety scores in the depression-targeted group and depression scores in the anxiety-targeted group changed. Contrary to our expectations, there were no significant changes in either group. While there are many explanations for this, one possible explanation is that our intervention programme may have offered a high degree of specificity to the area of psychopathology. Therefore, it could be said that our results provide an example for internet-based disorder specific CBT for anxiety and depression, as alluded to by Ye et al. (2014).
The participants of the anxiety group in this study reported increases in adaptive coping skills including cognitive restructuring, problem solving, and emotion regulation. They also reported a decline in avoidant coping skills including distraction, social distancing, and social withdrawal. Upon further examination, the increase in adaptive coping strategies and decline in avoidant coping strategies seen in the anxiety group were consistent with previous findings (Hogendoorn et al., 2014).
Unlike the anxiety group, no differences were found in adaptive or avoidant coping strategies in the depression group. Furthermore, no meaningful changes were found in maladaptive coping strategies including self-criticism, blaming others in neither the depression group nor the anxiety group. The ongoing pandemic period, restrictions of attending school in-person and limited in-person social interactions may account for ongoing difficulties in mental health of youth (Loades et al., 2020), potentially contributing to no meaningful changes in maladaptive coping strategies.
Behavioral activation and activity scheduling are effective in the treatment of depression and anxiety (Kanter et al., 2010). Beck (2011) also highlights the importance of behavioral activation in CBT, noting “one of the most important initial goals for depressed patients is scheduling activities” (p. 80). A comprehensive review of 150 articles conducted by Paterson et al. (2021), summarizing the relationship between activity and the COVID-19 pandemic in youth during the first year of the pandemic, reports a decline in physical activity time, and increases in total sedentary behaviour and sleep duration. The ongoing restrictions of behavioural and social activities during the COVID-19 period may have led to the reduced number of possible behavioural interventions provided within the psychoeducation programmes. This may have contributed to the lack of meaningful change found in coping skills within the depression group. Additionally, interventions targeting anxiety and depression are typically not limited to 4 sessions (Hamdan-Mansour et al., 2009). It takes time and practice for new behaviors to develop and become second nature. Participants were not able to assimilate and effectively utilize the coping skills introduced within the depression group. In a meta-analysis examining 31 studies for effectiveness of CBT for children and adolescents with depression, the individual/group CBT interventions for children and adolescence had a mean number of 10.6 sessions (range 5–16), a mean duration of 8.8 weeks and an average of 10.1 intervention hours (Oud et al., 2019). Therefore, it is assumed that more than 4 sessions are required for coping skills to increase which may also account for the absence of change in coping strategies.
This study is important for a number of reasons. It aims to fill a gap in the research, as previous studies have alluded to the importance of the psychosocial support for children and adolescents during COVID-19 pandemic (Jiao et al., 2020; Wang et al., 2020). Additionally, this study focuses on reducing anxiety and depression symptoms while increasing coping skills in at risk youth during the COVID-19 pandemic context. The psychoeducation programmes being limited to 4 sessions may be considered as a limitation; however, this may also be a strength of the study for practical reasons. Young people may prefer limited number of group-based approaches due to practicality as such programmes do not take up much time and can be taken alongside school studies. Additionally, it could be economical for both participants and practitioner. This study highlighted the possibility that even only 4 sessions of interactive psychoeducation programmes might prove beneficial, although further examination in future psychoeducation studies is warranted. Considering social relationships as an important event of Erik Erikson’s (1950) Stages of Psychosocial Development in adolescence, the impact of distancing from social environments due to the pandemic will make intervention and prevention studies targeting this group particularly valuable.
Practical implications
As highlighted in the Introduction section, the importance of social support to cope with distress, anxiety and depression symptoms has been shown in the literature (Ghosh et al., 2020; Hatzichristou et al., 2021; Mansfield et al., 2021). Considering internet-based anxiety and depression intervention programmes for youth, most programmes included more sessions (Ye et al., 2014). However, this study, consisting of 4 sessions, suggests possible benefits within a short period of time during pandemic. Such short psychoeducation programmes might be easier to apply in different settings including school, hospitals, virtual or counselling centres, making them time saving and economical.
The current study suggests that group-based online psychoeducation programmes can be effective in situations where structured therapy practices with behavioural interventions such as exposure and behavioral activation tailored to the individual's subjective needs are not possible (due to insufficient facilities or extraordinary conditions such as pandemic). The fact that a group-based online psychoeducation programme appeared to be associated with reductions in some psychological symptoms in a non-clinical sample with low symptom levels may also indicate that such practices may have possible preventive and protective effects.
Limitations
The present study has a number of limitations. The small sample size limits the reliability and generalizability of the results. The pretest-posttest design without a control group is also a limitation, since it cannot be said with certainty that the observed changes were due to the interventions. Additionally, it could also be worthwhile to have follow-up results to determine whether the participants maintain the decrease in depression and anxiety symptoms after posttest. Another limitation of this study may be the use of videoconferencing. Since the participants were attending the sessions from their homes, they might face distractions that interfere with the desired outcomes. In addition, there were more female participants then male participants. However, past research suggests high rates of anxiety and depressive disorders in women (Kessler et al., 1994).
In the present study, people who did not complete the required forms were not offered intervention. Nevertheless, to lessen this ethical limitation, a free call centre service was offered to all members of the community in need of psychosocial support. Another problem was the high dropout rate. From the 28 participants who initially joined the anxiety group, only 15 completed the psychoeducation programmes indicating a dropout rate of 46%; and from the 50 participants who initially joined the depression group, only 17 completed the psychoeducation programmes indicating a dropout rate of 66%. Due to the high dropout rates, we compared the pretest scores of the participants who dropped out with those who completed the programme. It was observed that there was no significant difference in pretest results between those who dropped out from depression group and those who completed the programme. This may indicate that the dropout in the depression group was random. However, it was observed that the anxiety levels of the participants who dropped from the anxiety group were significantly lower than those who completed the programme. In this case, we do not know whether the difference between pretest and posttest results in the anxiety group would have remained significant if all participants completed the programme.
The reasons for the high attrition rate should also be explored in future investigations. It is possible the increase in online activities like online-schooling contributed to “Zoom fatigue” and thus the high dropout rates. Dropout rates in internet-based interventions are found to be high in general. For instance, a review by Melville et al. (2010), of 56 internet-based psychotherapy studies conducted between 1990 and 2009, found a broad range of dropout rates reaching up to 83%. It would be also worthwhile to have a specific comparison of dropout rates across online intervention programmes targeting youth during the pandemic. Furthermore, researchers in future studies should ensure effective planning and monitoring to minimize attrition, due to the high dropout rates that may occur during implementation.
Future directions
Considering the results of the present study, future studies should pay special attention to high dropout rates. For example, future online psychological intervention programmes targeting youth may consider including incentives in order to reduce dropout rates. In the depression intervention group, decreases in depression were noted. However, significant changes were not found in the utilization of adaptive coping skills. This could be attributed to pandemic related restrictions limiting behavioural activation and hindering the development of coping skills, which are considered a major component of the treatment of depression with CBT. This will also be applicable for future online depression interventions, particularly if pandemic related restrictions continue or if social interactions remain limited in youth. Another important point is that this study was carried out as a psychoeducation programme rather than a group therapy session. While efforts were taken to provide an interactive environment for participants, in reality however, individual and group interaction and engagement was limited. Therefore, future studies including programmes designed to include active participation may be considered. Moreover, it would strengthen the methodological design of the study to have a control group and follow up test.
Conclusion
Targeted depression and anxiety programmes were developed to counteract the changes and limitations COVID-19 has placed on social relationships in youth. Four sessions of online psychoeducation programmes were associated with (a) decreases in depression in the depression group, and (b) decreases in anxiety, increases in adaptive coping skills and decreases in avoidant coping skills in the anxiety group.
Footnotes
Acknowledgements
We would like to thank the Istanbul Development Agency (ISTKA, grant number TR10/20/COVID/0633) who funded the present study as part of the ‘Improving the psychological well-being of young people with rising anxiety for the future during COVID-19’ Project. We would also like to thank Ms. Pınar Koç Yıldırım for her support and guidance of the depression psychoeducational groups and Mr. Abdulkadir Alemdar for his ongoing administrative support; BU, FT, DS, MST, SG and IEA contributed to the data collection, literature review, analyses, manuscript preparation and submission. All other authors contributed to overall design, review, and editing.
Ethics approval
This study was approved by the Ibn Haldun University Ethics Committee (NO. 14/09/2020-689) as part of a larger project.
Availability of data and material
The data are not publicly available due to privacy/ethical restrictions.
Code availability
Not applicable.
Consent to participate and consent for publication
Informed consent was obtained from participants and all participants confirmed they were participating voluntarily.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study was implemented as part of a larger project titled ‘Improving the psychological well-being of young people with rising anxiety for the future during COVID-19’ and was funded by the Istanbul Development Agency (ISTKA, grant number TR10/20/COVID/0633); the Istanbul Kalkinma Ajansi.