
Abstract
Introduction
This study investigated a training regimen for teachers of children with visual impairments (TVIs) who need to assess, plan instruction for, and teach students with cortical visual impairment (CVI), as well as the effect of these strategies on the visual behaviors of these students.
Method
TVIs learned CVI content knowledge and knowledge of a specific app-based system called CViConnect through a group workshop, seven asynchronous modules, and a year of mentorship from a TVI certified in CVI. When using the CViConnect system on iPads, data are captured during the instructional session, and the looking and touching behaviors of students are automatically saved to a remote server.
Results
TVIs with and without specific training used Phase I activities the most, but untrained TVIs used Phase II and III activities more than trained TVIs. Sessions conducted by trained TVIs averaged three times longer than those done by untrained TVIs. Students taught by TVIs without specific training touched items that were not meant to be selected (i.e., sprites and backgrounds) much more than students with trained TVIs, but students taught by trained TVIs looked at the screen more often—M = 0.08 looks/s versus M = 0.07 looks/s, t(3317) = 2.59, p = .005, d = 0.09—had longer sustained looks—M = 34.08 s versus M = 6.67 s, t(3317) = 10.11, p < .001, d = 0.35—and spent more time looking at the screen than students with untrained TVIs: M = 9.51 s versus M = 3.21 s, t(3317) = 4.12, p < .001, d = 0.14.
Discussion
Training led TVIs to be able to identify appropriate activities for their students with CVI, thus encouraging the children to use looking behaviors instead of becoming visually overwhelmed and randomly tapping on the screen.
Implications for Practitioners
These data seem to show that the training regimen in this project leads TVIs to choose activities of an appropriate level for their students with CVI and to use the CViConnect system to increase looking behaviors in their students.
Cortical visual impairment (CVI) results when the part of the brain that is responsible for processing visual information is damaged or is not functioning as it should be. CVI can also be referred to as cerebral visual impairment, neurological visual impairment, or cerebral/cortical visual impairment. The area of the brain affected by CVI are mainly posterior visual pathways including the occipital cortex, where initial processing of visual input takes place, as well as other parts of the visual processing pathway such as the thalamus and areas of the cortex associated with higher-order processing such as cortical areas associated with dorsal and ventral stream processing (Merabet et al., 2017). This complex neural network is essential for interpreting visual stimuli, and any disruption can severely impact visual perception and understanding.
Damage to the posterior visual pathways or the visual processing areas of the brain can result from peri- or postnatal hypoxia-ischemia, trauma, infection, the effect of drugs or poisons on the brain, and certain neurologic diseases such as epilepsy (Good et al., 2006). Typically, students with CVI demonstrate reduced visual acuity and visual fields, but some visual function is often present, even when the effects of CVI are severe. Children with CVI often have physically healthy eyes that are able to take in visual information, but their brains have difficulty translating and understanding what they are seeing (Jackel et al., 2010). Children with CVI often exhibit color preference, visual latency, attraction to movement, visual field preferences, difficulty processing complex scenes, a need for increased light, difficulty viewing distant or novel objects, uncommon visual reflexes, and lack of visually guided reach (American Association for Pediatric Ophthalmology and Strabismus, 2021; Chang & Borchert, 2020; Roman-Lantzy, 2018, 2019). CVI is diagnosed by a medical professional such as an ophthalmologist or a neuro-ophthalmologist, and factors contributing to the diagnosis may include a child's medical history (including any brain condition, trauma, or damage), results of an eye exam that do not explain the child's functional vision, and any unique visual or behavioral characteristics that impact the child's ability to understand what is seen (Roman-Lantzy, 2018, 2019).
Although CVI is considered the primary cause of visual impairment in children (Good et al., 2001; Merabet et al., 2017), it is often underreported, underdiagnosed, and undertreated condition (Perkins School for the Blind, 2023). Neilsen et al. (2007) indicate that for children with developmental disabilities, at least 10.5% may have CVI, while other estimates suggest that up to 70% of children with cerebral palsy also have CVI (Perkins School for the Blind, 2023). These numbers are partially explained by improved neonatal care which has led to an increase in children being born with CVI (Chang & Borchert, 2020; Luo et al., 2022). Some estimates of CVI prevalence place it at 30%–40% of children with visual impairments (McDowell, 2021; Roman et al., 2010), and others suggest that one in 30 elementary school-aged children have CVI-related vision problems (Williams et al., 2021). Because of these statistics, it is crucial that teachers of children with visual impairments (TVIs) are knowledgeable of this condition and are able to effectively teach children with CVI. Through systematic intervention strategies aimed at improving specific visual behaviors, such as helping children maintain a steady gaze on visual targets and enhancing their coordination between visual input and hand movements, many individuals with CVI show some improvement in visual acuity over time (Walker & Wegner, 2021), although typical visual acuity is not usually achieved (Handa et al., 2018). Although rehabilitative outcomes and methods for children with CVI are still poorly understood, continued investigation of potential intervention strategies remains a high priority in the educational field (Mazel et al., 2020).
Need for Training in CVI
Students with CVI have unique learning needs that differ in complexity from students with ocular visual impairments (Mazel et al., 2020). Although the prevalence of CVI is high among visually impaired children, there is still a lack of knowledge of CVI in the professional and educational systems. Recent priorities of the National Institutes of Health (Bernard, 2022) show more recognition for research and clinical services to incorporate the perspectives and experiences of individuals and families and to include neurodivergent perspectives in research (Fletcher-Watson et al., 2021). However, ophthalmologists have been found to have limited knowledge regarding clinical features, investigation, differential diagnosis, and visual prognosis of CVI in children (Maitreya et al., 2018), and parents and caregivers have expressed concern that both physicians and teachers are lacking in their training for working with children who have CVI (Jackel et al., 2010). Combined with a critical national shortage of education personnel who specialize in teaching students with visual impairments (Summers et al., 2006), this lack of knowledge means that many students with CVI do not receive the necessary services for their visual impairment. In fact, in a recent survey of parents of children with CVI, 42% indicated that their children received “consult only” or “no” services from a TVI and 47% indicated that their children did not receive any orientation and mobility services at all (Blackstone et al., 2021). According to Roman-Lantzy (2018), these children have fallen through the cracks of the special education system, with service providers holding low expectations for children with CVI and demonstrating a lack of knowledge of appropriate interventions (McCarty & Light, 2023). Since CVI has such a high prevalence, and because the number of CVI students is slated to increase (McDowell, 2021), TVIs need up-to-date and thorough training in CVI characteristics and CVI pedagogy to meet the particular needs of students with CVI. One area in which TVIs need direction is in determining which strategies and accommodations are most effective for students with CVI.
Methods
This study looked at the development and efficacy of a training regimen for practicing TVIs on how to effectively assess, plan instruction for, and teach students with CVI. The training encompassed both basic content knowledge about CVI and the use of a specific app-based tool called CViConnect. The CViConnect system is an iPad application that includes the CVI Range assessment. With results from conducting this assessment, a teacher plans activities for a student and delivers those activities in the classroom or assigns the student to access them at home using their iPad.
The system offers a library of activities created for CVI Phases I, II, and III. Although initial activities in the library were created by TVIs involved with CViConnect, any TVI using the system is able to create their own activity and upload it to the library for others to use. As a part of this project, a TVI who was adept at using the system was contracted to create activities to bolster the library offerings.
According to Roman-Lantzy (2018, 2019), a learner with CVI is placed in a phase based on their CVI Range score. A CVI Range score of 0–3 places a learner in Phase I, in which a child is building consistent visual activity (e.g., reaching without looking, visually responding in an appropriate environment). Activities for students Phase I might include single-color circles and sparkling effects moving around the screen or videos of single-color bubble machines. Each activity has several copies to allow the educational team to select the aspects (i.e., color, movement, or light) that meet the needs of their learner.
A learner with a CVI Range score above 3 to a score of 7 is in Phase II, in which a child begins integrating vision with function (e.g., reaching while looking, visually responding with additional noise or complexity). Activities for students in Phase II might include images of the learner's preferred toys for choice-making or stories with simple, realistic images.
Finally, a learner with a CVI Range score above 7 and up to 10 is in Phase III, in which a child refines visual behaviors (e.g., being able to respond to visual stimuli further away, having longer visual attention). Activities for students in Phase III might include tracing a letter on the iPad with their finger, color highlighting or word bubbling, or finding a target among an increasing complex array of objects. Activities can be individually assigned to a student as is, edited to meet a student's needs, or team members can create their own activities. Activities are displayed for students on an iPad, and many are designed to prompt a student response.
While the activity is running, the CViConnect system captures statistical data about the interactions of the student with the touch screen during a session. These data can then be used by the TVI to make data-based decisions when modifying instruction for a specific student. CViConnect utilizes a secure web-based dashboard to provide tools for charting the progress of a student as they work toward their goals (heatmaps, session event timelines, etc.). CViConnect is designed to use the iPad's forward-facing camera to detect whether a child is looking at or away from the displayed activity; if the child is looking, the system can detect within 2 cm of where the child is looking. Additionally, CViConnect captures decibel detection and touch detection throughout each activity. This information is correlated with what is displayed on the screen to help the family or teacher understand what target provides the best visual attention for the student, as well as how environmental complexity affects the child's ability to utilize their vision. This level of performance data allowed the project researchers to correlate student performance with teacher training and instructional effectiveness.
Distance education technology was used for conducting the training sessions. Web conferencing and case-based studies have been established as effective coaching platforms for the development of teachers for over 20 years (Bonk et al., 1998). TVIs and other special education providers participated in a large group training session about CVI and the CViConnect system. Then they were provided structured mentorship during the next year as they implemented CViConnect PRO into their teaching practice for students with CVI.
Training was comprised of an initial large group workshop that was followed by seven modules, including a 32-min module on understanding CVI; a 54-min presentation on CVI Range assessment; a 2.5-hr session on functional vision evaluation, learning media assessments, orientation and mobility (O&M) evaluations, and entering data into the CViConnect system; a 58-min session on understanding the phases of CVI; a 13-min session on the mechanics of the CViConnect system; a 43-min session on individualizing instructional activities using the system; and a 56-min session on analyzing data inside and outside of the system.
Each participant proceeded through the modules on their own schedule, with the goal of completing the material in approximately 3 months. The workshops had two foci: effective instructional processes for working with children with CVI and effective use of CViConnect PRO. Workshops were conducted by project staff members who were certified in CVI. Additionally, Dr Roman-Lantzy recorded content specifically for these workshops. Dr Roman-Lantzy is the foremost expert and author of the CVI Range, a functional vision assessment, as well as scaffolding instruction for individuals with CVI.
The training plan was for groups of TVIs, other special education providers, and parents to begin with a group workshop, via a large web conference platform, where presentations created using Microsoft's presentation software PowerPoint were used to guide participants through basic content. A second portion of the group workshop training made use of videos and descriptions of specific case subjects that were made available in digital format to all trainees. TVI participants were led through the process of finding individual data gathered by CViConnect for case subjects in the training. Student data were analyzed to develop targeted interventions to incorporate as the student's functional vision improved. TVIs who took part in the training were nominated by state-level vision professionals as TVIs who would benefit from CVI training.
In the last portion of the training, each participant was offered the opportunity to join the CViConnect Learning Community. This community asked each member to bring their knowledge, experiences, and expertise to the group as they gained new insights working with students with CVI and the CViConnect system. They were taught how to create new activities that followed the principles of best practice for students with CVI so that when their student needed practice with a specific skill that did not have an intervention in the CViConnect system, they would have the knowledge and skills to create a new intervention. That intervention was then integrated into CViConnect's Activity Library and became available for teachers to select and use with students who may benefit from that targeted activity. In this way, teachers involved in the project would contribute to improvement of the CViConnect system by having their input incorporated into the system in successive system refinements.
Each teacher in the training was also paired with a CVI mentor from the staff members of CViConnect. The mentor continued in the role over the year following the training as the teacher practiced and refined their skills using the CViConnect system with their students. During the mentoring phase, the five elements of effective coaching were utilized including:
individualized mentoring (one on one), intensive (connect every couple of weeks), sustained (over the year), context-specific (CVI services), and focused (examine specific student needs and progress; Foster, 2018).
Structured mentoring was selected for this project because of the complex and heterogeneous needs of students with CVI. It is likely that one teacher will have many students with CVI who have vastly different visual functioning. Because CVI is a condition that, by definition, occurs in individuals with documented brain damage, students with CVI often have a variety of medical diagnoses and multiple impairments. It can take time for a teacher to become acquainted with the medical terminology and etiologies involved with this population, a mentor can assist as the teacher gains new knowledge. In the large group workshop, the most common characteristics of CVI and how they are manifested in children were included in case studies, but less common presentations may be part of a teacher's caseload. The mentors were available to provide support and examples as the teacher gained new knowledge and skills so that each student received the highest level of assessment and intervention throughout the project. In particular, TVIs needed mentoring on adapting and applying CVI interventions so as to support augmentative and alternative communication (AAC) and CVI, literacy and CVI, and babies with CVI. Mentors also provided consultation support for individualized education program (IEP) teams and families.
At the group workshop, each participant and mentor were paired. They exchanged contact information and created a timeline for mentoring meetings. Ideally, each teacher met with their mentor for one-on-one mentoring sessions weekly for one to two semesters. Mentors were encouraged to keep the meetings focused on the specific context of CVI services and specifically the CViConnect system. The CViConnect trainers and university personnel were available to any mentors and participants who had questions as the project progressed.
After the initial group workshop, follow-up training modules were available on the video-sharing platform YouTube to walk users through each component of the app as a refresher after the training. As TVIs and other special education providers provided feedback on different aspects of the training process and as more outcome data were collected from students they were working with, the training materials were updated, and features were added to or updated in the CViConnect system and made available to all future users. This study was approved by the Institutional Review Board of Western Michigan University and followed approved guidelines on participant consent.
Results
In addition to the TVIs involved in this project, the CViConnect system is also used by a number of local education authorities, some of whom have accessed training from the CViConnect personnel and some who have not. TVIs who use CViConnect with students but have not accessed any training from study personnel or CViConnect personnel comprised a control group for TVIs and students with CVI in the study. Data were automatically collected by the CViConnect system during instructional sessions. TVIs who attended the study workshops will be referred to as “trained TVIs” in this paper. “Untrained TVIs” will refer to the group of TVIs who used the CViConnect system to work with their students but did not participate in the workshops or receive additional support while using the system with their students.
Data from 18 TVIs who went through the training process and submitted complete questionnaires before and after their participation in the training session show that 22% found it moderately useful, 28% found it fairly useful, and 50% found it extremely useful. Average comfort levels assessing students with CVI increased after training increased from 2.78 to 3.61 (on a scale of 5) and average comfort levels teaching students with CVI increased from 2.72 to 3.67. Demographics of TVIs who went through the project are shown in Table 1.
TVI Demographics.
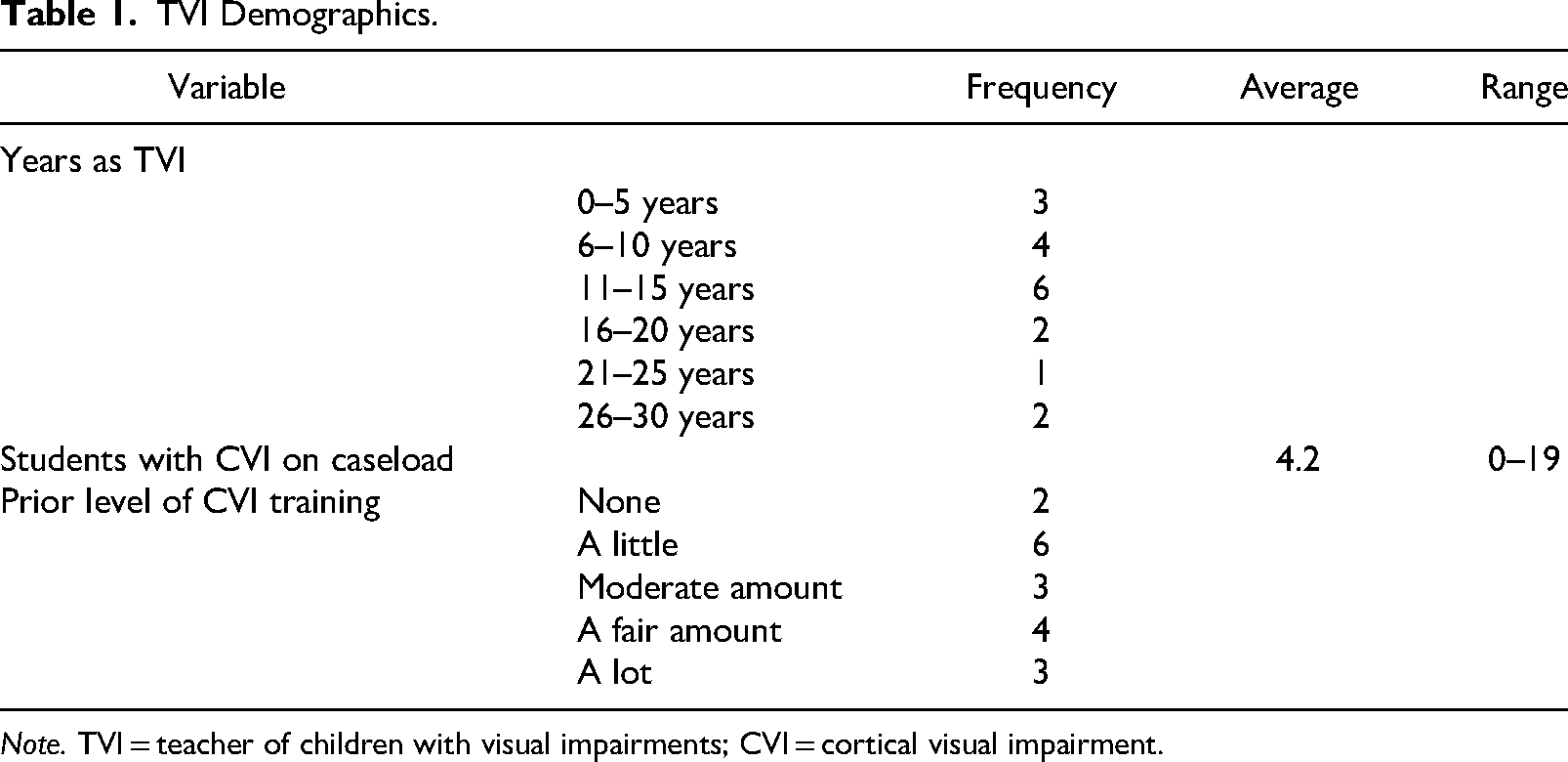
Note. TVI = teacher of children with visual impairments; CVI = cortical visual impairment.
For TVIs who indicated that they had received prior training in CVI, the sorts of training programs they listed included continuing education from state agencies or conference sessions (n = 9), coursework during university training (n = 6), Perkins School for the Blind training (n = 5), assistance from colleagues (n = 4), and watching videos (n = 2). There was no effect of the amount of prior training on the change in comfort level in teaching students with CVI after the training: 13 TVIs increased comfort level by one level on the response options, two TVIs increased comfort level by two response levels, two TVIs decreased comfort level by one response level, and one TVI remained at the same level of comfort.
Data were collected from about 3,318 instructional sessions on the CViConnect system across trained and untrained TVIs. As shown in Table 2, untrained TVIs used Phase I activities most frequently during their lessons (55.7%), followed by Phase II activities (26%), and Phase III activities (18.3%). Trained TVIs also used Phase I activities most often during their lessons (87.6%), followed by Phase III activities (7.4%), and Phase II activities (5.0%). All TVIs used Phase I activities more than Phase II or Phase III activities, but untrained TVIs used Phase II and III activities more frequently than trained TVIs did.
CViConnect Instructional Sessions.

Note. TVIs = teachers of children with visual impairments.
For all levels of activities, trained TVIs tended to have instructional sessions that lasted three times as long as untrained TVIs. Untrained TVI sessions lasted approximately 85.52 total seconds, whereas trained TVI sessions lasted 308.98 total seconds: t(3317) = 24.42, p < .001, d = 0.85. Untrained TVIs had students who touched sprites and backgrounds much more frequently than students with trained TVIs: M = 0.06/s versus M = 0.01/s, t(3317) = 13.10, p < .001, d = 0.46. Students with trained TVIs looked at the screen more often—M = 0.08 looks/s versus M = 0.07 looks/s, t(3317) = 2.59, p = .005, d = 0.09—had longer looks, M = 34.08 s versus M = 6.67 s, t(3317) = 10.11, p < .001, d = 0.35—and spent more time looking at the screen than students with untrained TVIs, M = 9.51 s versus M = 3.21 s, t(3317) = 4.12, p < .001, d = 0.14.
The data for Phase I activities were classified, since it was the most used level among both groups. The most popular lessons at the Phase I level were Color Glow: Red, with 454 (18.7%) instructional sessions; Bubble Machine, with 328 (13.5%) instructional sessions; and Color Glow: Yellow, with 325 (13.4%) instructional sessions. During those sessions, the average amount of time trained TVIs’ students looked at the screen was 10.67 s. Untrained TVIs’ students looked at the screen for an average of 4.83 s. Students of trained TVIs also had a higher “longest look” average of 38.41 s, compared to the students of untrained TVIs, whose longest look was averaged at 9.45 s.
Discussion and Conclusion
The trained TVIs themselves had to complete the workshops and coaching sessions to gain the knowledge they needed to use the CViConnect system as they tried to work on the proper supports and interventions so their students with CVI would receive appropriate lessons. The data collected from trained and untrained TVIs show that TVIs who were trained to use CViConnect spent more time working on Phase I activities. There was also a pattern whereby students working with an untrained TVI spent more time touching the screen (both task-related targets and background) and less time looking than students working with trained TVIs. It may be that training led TVIs to be able to identify activities that were most appropriate for their students’ phase, thus encouraging looking behaviors instead of having a situation in which a child becomes visually overwhelmed and randomly taps on the screen.
When Phase I activities were examined on their own, the students of trained TVIs also achieved a higher average amount of time in looking at the screen, and a significantly longer amount of time for their longest look. Although more research needs to be done on the CViConnect system and how it is implemented with students who have CVI, these data seem to show that the training regimen provided in this project has had the desired effect of leading TVIs to choose activities based on the needs of their students and encouraging them to use the CViConnect system effectively in increasing looking behaviors in their students.
This first study from the project focused on student engagement with the interventions provided in the CViConnect system. Further analysis of the data is designed to include CVI Range scores for students across a number of years. These data may lead to the identification of individual activities that can lead to improved vision for students with CVI. At the close of the project, all the training materials and an open-source version of the CViConnect system will be available at CViConnect.co. It is our hope that this training will be adopted by CVI training teams of vision professionals across the other 40 U.S. states and territories, thus, these materials will be used to train TVIs in every state and territory. Children with CVI and their families are in need of resources to meet their specific needs. When the appropriate interventions are provided, there is potential for improved vision for the child. We encourage vision professionals, families, caregivers, and individuals with CVI to use and benefit from the resources developed by this project.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Office of Special Education and Rehabilitative Services (grant number H327S200006).