
Abstract
The authors extended research linking individual differences in consideration of future consequences (CFC) with health behaviors by (a) testing whether individual differences in regulatory focus would mediate that link and (b) highlighting the value of a revised, two-factor CFC-14 scale with subscales assessing concern with future consequences (CFC-Future) and concern with immediate consequences (CFC-Immediate) proper. Exploratory and confirmatory factor analyses of the revised CFC-14 scale supported the presence of two highly reliable factors (CFC-Future and CFC-Immediate; αs from .80 to .84). Moreover, structural equation modeling showed that those high in CFC-Future engage in exercise and healthy eating because they adopt a promotion orientation. Future use of the two-factor CFC-14 scale is encouraged to shed additional light on how concern with future and concern with immediate consequences (proper) differentially impact the way people resolve a host of intertemporal dilemmas (e.g., health, financial, and environmental behavior).
Many health behaviors pose a conflict between the short-term and long-term consequences of one’s actions. For example, in the short run, exercise and healthy eating can require people to sacrifice things that give them pleasure such as sleeping in and eating delicious, high-fat foods. In the long run, however, exercise and healthy eating benefit the individual. Unfortunately, as the growing obesity epidemic confirms, many people fail to exercise and eat healthy foods, suggesting they are either strongly influenced by the immediate consequences of their actions or they fail to consider the long-term benefits of exercise and healthy eating.
Consideration of Future Consequences (CFC) and Health Behavior
Given their intertemporal nature, one factor that predicts health behaviors is an individual’s CFC (i.e., the extent to which people consider the potential distant outcomes of their current behaviors and are influenced by those potential outcomes; Strathman, Gleicher, Boninger, & Edwards, 1994). For example, relative to those scoring low, those scoring high on the CFC scale are more likely to exercise (Adams & Nettle, 2009; Ouellette, Hessling, Gibbons, Reis-Bergan, & Gerrard, 2005); control their diet (Piko & Brassai, 2009); report a lower body mass index (BMI; Adams & Nettle, 2009; Adams & White, 2009); accept free sunscreen (Orbell & Kyriakaki, 2008); limit sun exposure (Heckman, Wilson, & Ingersoll, 2009); use a condom (Appleby et al., 2005; Dorr, Krueckeberg, Strathman, & Wood, 1999); get tested for HIV (Dorr et al., 1999), diabetes (Crockett, Weinman, Hankins, & Marteau, 2009; Orbell & Hagger, 2006), and colorectal cancer (Orbell, Perugini, & Rakow, 2004); vaccinate their daughters against cervical cancer (Morison, Cozzolino, & Orbell, 2010); take actions to prevent future occurrence of past illnesses (Sirois, 2004); and quit smoking (Kovač & Rise, 2007). High CFCs are also less likely to use alcohol and tobacco (Adams & Nettle, 2009; Daugherty & Brase, 2010; Rappange, Brouwer, & Van Exel, 2009; Strathman et al., 1994) and expose themselves to environments promoting hearing loss (i.e., discotheques; Vogel, Brug, Van der Ploeg, & Raat, 2010). 1
Moving beyond main effects, many CFC/health behavior studies have taken an “interactionist” perspective. For example, Ouellette et al. (2005) examined how self-generated prototypes (of other exercisers) versus ideal possible selves (of the self in the future) influenced exercise behaviors of low versus high CFCs. Ouellette et al. hypothesized that ideal possible selves (of the self in the future) would be more motivating for high CFCs than for low CFCs, as the ideal possible self is a version of the self that exists in the future. As predicted, high CFCs (but not low CFCs) increased exercise behavior after first considering ideal selves (but not prototypes of other exercisers). Although not predicted, results also showed that low CFCs increased exercise behavior when they considered prototypes of other exercisers (but not ideal selves), which the authors suggest makes sense, in that low CFCs focus on the “here and now” and prototypes are “very much based in the present” (Ouellette et al., 2005; p. 617).
As another example, Orbell and her colleagues have reported a series of studies showing that high CFCs are more likely to engage in screening for diabetes (Orbell & Hagger, 2006) and colorectal cancer (Orbell et al., 2004), and accept free sunscreen (Orbell & Kyriakaki, 2008) when health messages emphasize the long-term benefits of these actions, while low CFCs are more likely to take the same actions when health messages emphasize the short-term benefits of these actions. Additional studies support this CFC × Tailored message approach (e.g., Kees, Burton, & Tangari, 2010; O’Connor, Warttig, Conner, & Lawton, 2009; Strathman et al., 1994).
Finally, several studies have explored mediators between CFC and health behaviors. Such studies have focused on the mediating effect of positive/negative thoughts about cancer (Morison et al., 2010), how procrastination mediates between CFC and health behavior intentions (Sirois, 2004), and how attitudes, subjective norms, behavior control, and thoughts in response to persuasive messages mediate the impact of the CFC × Message framing interaction on health intentions (Orbell et al., 2004; Orbell & Hagger, 2006; Orbell & Kyriakaki, 2008). 2
Gaps in the CFC–Health Behavior Literature
The preceding studies demonstrate that CFC predicts a range of health behaviors. At the same time, research linking CFC and health behaviors has at least two important gaps. First, there is growing debate regarding the factor structure of the CFC scale, with several studies arguing for a two-factor as opposed to a one-factor model (e.g., Adams, 2012; Joireman, Balliet, Sprott, Spangenberg, & Schultz, 2008; Petrocelli, 2003; Rappange et al., 2009; Toepoel, 2010). Second, with the few exceptions noted above, little research has attempted to identify mechanisms through which CFC predicts various health behaviors. The present studies address these limitations by reexamining the nature of the CFC construct and testing the hypothesis that CFC predicts an individual’s chronic regulatory focus orientation (i.e., promotion vs. prevention; Higgins et al., 2001), which in turn predicts exercise and healthy eating attitudes and intentions. Because the distinction between the two CFC subscales is central to our theoretical development, we first consider measurement of the CFC construct.
CFC: One Factor or Two?
Strathman and colleagues (1994) developed a 12-item scale to measure individual differences in CFC (Items 1-12 in the appendix). In keeping with its original conception, the majority of prior research has treated the CFC scale as a unidimensional scale (i.e., an average or sum of the future items and the reverse-coded immediate items). Recently, however, several studies have found that a two-factor model best explains responses to the scale (Adams, 2012; Joireman et al., 2008; Petrocelli, 2003; Rappange et al., 2009; Toepoel, 2010; for an exception, see Hevey et al., 2010). Arguably, the clearest two-factor solution distinguishes between a 7-item CFC-Immediate subscale and a 5-item CFC-Future subscale (Adams, 2012; Joireman et al., 2008; Rappange et al., 2009; Toepoel, 2010). A two-factor distinction implies that, although individuals may develop a dominant temporal orientation, concern with future and concern with immediate consequences are not polar opposites; that is to say, individuals may consider the future consequences of their actions, the immediate consequences of their actions, or both (for a similar line of reasoning, see Shipp, Edwards, & Lambert, 2009; Zimbardo & Boyd, 1999).
Although there appears to be growing support for a two-factor solution, distinguishing between CFC-Future and CFC-Immediate subscales has at least two disadvantages. First, personality researchers have often been criticized for unnecessarily adding new constructs to the large nomological net of existing constructs. Second, a two-factor solution complicates a researcher’s conceptualization and data analysis. Despite these concerns, distinguishing between the two CFC subfactors has several practical and theoretical advantages, as outlined below.
Practical and Theoretical Advantages of the Two-Factor Distinction
One advantage of a two-factor solution is that it allows researchers to determine whether consideration of future consequences (proper) is responsible for a given behavior, or whether the behavior is, in fact, better predicted by a consideration of immediate consequences. If researchers adopt a one-factor solution, they reverse code the immediate items and average them with the future items, resulting in a single “CFC score.” Although this single CFC score may predict a given behavior, the appropriate interpretation of this CFC/behavior relationship is not always clear.
For example, assume that the single CFC score correlates at r = .50 with exercise. Using the traditional (one-factor) interpretation, one would be tempted to conclude that “people who are concerned with the future consequences of their actions are more likely to exercise.” This reasoning is apparently logical, as the scale is called the “Consideration of Future Consequences Scale,” but a closer look reveals another interpretation: It is possible that the positive correlation between CFC and exercise is actually driven exclusively by the immediate items. In other words, a positive correlation between CFC and exercise behavior may occur because “people who are concerned with the immediate consequences of their actions are less likely to exercise.”
By merging the immediate and future items into a single CFC score, as has typically been done, a researcher could be overlooking an important conclusion: Exercise is not driven by a concern with future consequences (e.g., long-term health benefits) but rather by a concern with immediate consequences (e.g., inconvenience). The latter interpretation would have dramatically different implications. The first interpretation suggests that interventions aimed at increasing exercise should focus on convincing people to care about the long-term consequences of exercise (i.e., health benefits exercise can bring). In contrast, the second interpretation suggests that interventions aimed at increasing exercise should focus on decreasing people’s concern with immediate consequences or eliminating those immediate negative consequences altogether.
A second and related advantage of the two-factor solution is that it allows researchers to test competing models regarding how CFC is related to a given outcome. For example, in their article on CFC, ego depletion, and self-control, Joireman et al. (2008) articulated two competing theoretical models based on the distinction between CFC-Immediate and CFC-Future subscales. Briefly stated, the susceptibility model assumes that a high level of CFC-Immediate makes one susceptible to self-control failure, whereas the buffering model assumes that a high level of CFC-Future buffers one against self-control failure. As we note below, several studies have supported a two-factor distinction and highlighted the value of the susceptibility and buffering models.
Empirical Support for the Two-Factor Distinction
Most studies on the factor structure of the CFC scale have focused exclusively on factor analyses. Albeit important, construct validity studies (Marsh, 1996) that explore whether the distinction between the factors matters (i.e., do the CFC subscales differentially relate to various outcomes of interest?) are also critical in determining the value of a two-factor distinction.
For example, Joireman et al. (2008) reported a large-scale confirmatory factor analysis supporting the two-factor solution, a correlational study showing that trait self-control was only predicted by the CFC-Immediate subscale, and an experiment showing that the CFC-Immediate subscale moderated the impact of ego depletion (Baumeister, Muraven, & Tice, 2000) on temporal discounting. Results showed that CFC’s relationship with self-control and temporal discounting is due to a high concern with the immediate consequences of behavior rather than low concern with the future consequences of behavior, supporting the susceptibility model.
A more recent study linking CFC with compulsive buying tendencies and credit card debt provided additional support for the susceptibility model (Joireman, Kees, & Sprott, 2010). In that study, high levels of CFC-Immediate magnified the impact of compulsive buying tendencies on credit card debt, whereas the CFC-Future subscale did not predict credit card debt, consistent with Joireman et al.’s (2008) findings in the domain of self-control.
Finally, Rappange et al. (2009, Table 3) reported results more in line with the buffering model, in that the CFC-Future subscale tended to be a better predictor than the CFC-Immediate subscale of various health beliefs (e.g., “If I live unhealthy, I may die sooner”) and behaviors (e.g., self-reported healthy eating and exercise). Rappange et al. summarized their results by stating, “The important conclusion from [our] findings is that the underlying factors explain different aspects of (health) behavior and, therefore, their distinction is important” (p. 577).
In sum, theoretical and empirical arguments support the distinction between CFC-Future and CFC-Immediate subscales. However, as Joireman et al. (2008) noted, the reliability of the five-item CFC-Future subscale is often suboptimal (<.70). Accordingly, we added two items to the CFC-Future subscale and evaluated the validity of the revised CFC-14 scale using exploratory and confirmatory factor analysis. As outlined next, we also tested whether promotion versus prevention regulatory styles mediate the CFC subscales’ relationships with exercise and healthy eating attitudes and intentions.
Linking Individual Differences in CFC With Regulatory Focus
Regulatory focus theory (Higgins, 1997; Higgins et al., 2001) proposes that people can adopt one of two goal pursuit strategies. A promotion orientation facilitates achieving ideal goals (hopes and aspirations) by focusing an individual’s efforts on eagerly achieving positive outcomes. A prevention orientation facilitates achieving ought goals (duties and responsibilities) by focusing an individual’s efforts on vigilantly avoiding negative outcomes. Some studies treat regulatory focus as a state that can be momentarily primed by the situation (e.g., Cesario, Grant, & Higgins, 2004). Other studies, like ours, treat regulatory focus as a stable individual difference (e.g., Higgins et al., 2001; Zhao & Pechmann, 2007).
As we explain below, the goal-directed strategies involved in a promotion orientation—ideals, hopes and aspirations, eagerly seeking gains—are likely to arise out of a broader tendency to focus on the future consequences of one’s actions, whereas the goal-directed strategies inherent in a prevention focus—oughts, duties and responsibilities, and vigilantly avoiding losses—are likely to arise out of a broader tendency to focus on the immediate consequences of one’s actions. Restated, theoretical and empirical considerations suggest that people scoring high on the CFC-Future scale will tend to adopt a promotion orientation, whereas those scoring high on the CFC-Immediate scale will tend to adopt a prevent orientation.
Ideal Versus Ought Self-Guides and CFC
First, those who focus on the future consequences of their actions should be more likely to adopt ideal self-goals (hopes, aspirations), as ideal goals tend to be abstract and distal, and such construals are more in line with (i.e., provide a better fit with) a future orientation (Fessel, 2011; Trope & Liberman, 2003). For example, (future-oriented) Julie might exercise because she wants to be “in ideal shape.” Being in ideal shape could mean meeting any number of criteria, such as enhanced cardiovascular functioning, firm muscles, or a sense that she is physically fit. Although some of these criteria can be objectively assessed (e.g., cardiovascular functioning via VO2 max), the range of possible values that qualify as “in shape” may vary considerably from person to person, suggesting that ideal goals tend to be abstract. Moreover, pursuing ideal self-goals typically requires sustained effort over a long period of time, as there is always room for improvement toward an ever higher ideal. In sum, ideal self-goals typically involve striving toward an abstract future goal, which is more appealing for people who consider the future consequences of their actions.
By comparison, people who tend to focus on the immediate consequences of their actions should be more likely to adopt ought self-goals (duties and responsibilities), as these goals tend to be more concrete and proximal, and these construals are more in line with (i.e., provide a better fit with) a present orientation (Fessel, 2011; Trope & Liberman, 2003). For example, (present-oriented) John might exercise because important people in his life think he “should” exercise. When John does exercise, his friends and family may provide immediate positive feedback (e.g., it’s great that you’re getting into the gym!), and when he does not exercise, his peers may provide immediate negative feedback (e.g., we didn’t see you in the gym yesterday). Regardless of the valence of that feedback, the important point is that the feedback John receives is concrete and (relatively) more immediate (than the long-term gains associated with the ideal self). In sum, ought self-goals more often involve striving toward a concrete immediate goal, which is more appealing for people who consider the immediate consequences of their actions.
Eager Pursuit of Gains Versus Vigilant Avoidance of Losses and CFC
Regulatory focus theory’s emphasis on eagerly seeking positive outcomes versus vigilantly avoiding negative outcomes is also relevant to the CFC construct. For example, an eager pursuit of gains implies a willingness to move away from the (present) status quo in service of obtaining better but potentially uncertain positive future outcomes. Willingness to pursue such (uncertain) outcomes presumably rests in turn on optimism for the hoped-for future outcome. When one sets future goals, one tends to focus on potential successes (Gilovich, Kerr, & Medvec, 1993) and find it easier to envision a better possible future (Pennington & Roese, 2003; Snyder, Rand, & Ritschel, 2006). For example, assuming that Julie routinely considers the future consequences of her actions, she may be more optimistic that exercise will lead to the positive outcomes associated with her ideal goals, and she may be more likely to set realistic goals and use more effective strategies for achieving those goals (Sohl & Moyer, 2009).
By comparison, vigilant avoidance of losses implies a constant monitoring of threats to one’s present outcomes. This is important, because when people think about achieving an outcome in the near future, they tend to focus on possible failures (more than possible successes; Gilovich et al., 1993). This more pessimistic perspective may reduce thoughts about possible ideal goals and shift one’s focus onto actions that are necessary to maintain security and support the status quo (Hazlett, Molden, & Sackett, 2011). For example, if John routinely considers the immediate consequences of his actions, he may be disinclined to strive for future ideals and more likely to set immediate goals related to security (e.g., approval from peers). John’s tendency to focus on immediate outcomes may also make him more likely to accept smaller, immediate outcomes rather than striving for larger, delayed outcomes (i.e., to pursue the status quo).
Empirical Support for the Overlap Between the CFC Subscales and Regulatory Focus Orientations
Several studies support the line of reasoning just advanced. To help organize these studies, Table 1 summarizes key differences between promotion and prevention orientations and highlights studies illustrating the overlap between each of these orientations and the CFC construct. For example, with regard to self-guides, as noted earlier, Ouellette and her colleagues (2005) found that those scoring high in CFC were more motivated to exercise after contemplating their ideal future self, whereas those low in CFC were more motivated to exercise after contemplating prototypes of other exercisers (which presumably highlighted normative concerns of what one “should do”). With regard to end goals, research has shown that those scoring high on the CFC-Future subscale are more likely than those scoring low on the CFC-Future subscale to forgo smaller, certain rewards in favor of larger but less certain rewards (Joireman & Balliet, 2012), consistent with the idea that CFC-Future is associated with a tendency to focus on “pursuing (uncertain) gains.” Similarly, research has shown that those scoring high on the CFC-Immediate subscale are more likely to opt for smaller, immediate rewards over larger, delayed rewards (Joireman et al., 2008), consistent with the idea that CFC-Immediate is associated with a tendency to focus on “preventing (immediate) losses.” Finally, with regard to cognitive styles, research has shown that those scoring high in CFC are more optimistic than those scoring low in CFC (O’Brien-McElwee & Brittain, 2009; Strathman et al., 1994), suggesting connections with an “eager” style. On the other hand, high scores on the CFC-Immediate subscale are associated with higher trait hostility (Joireman, Anderson, & Strathman, 2003, data reanalyzed at the subscale level), suggesting connections with a more “vigilant” style.
Overlap Between Regulatory Focus Orientations and CFC Subscales
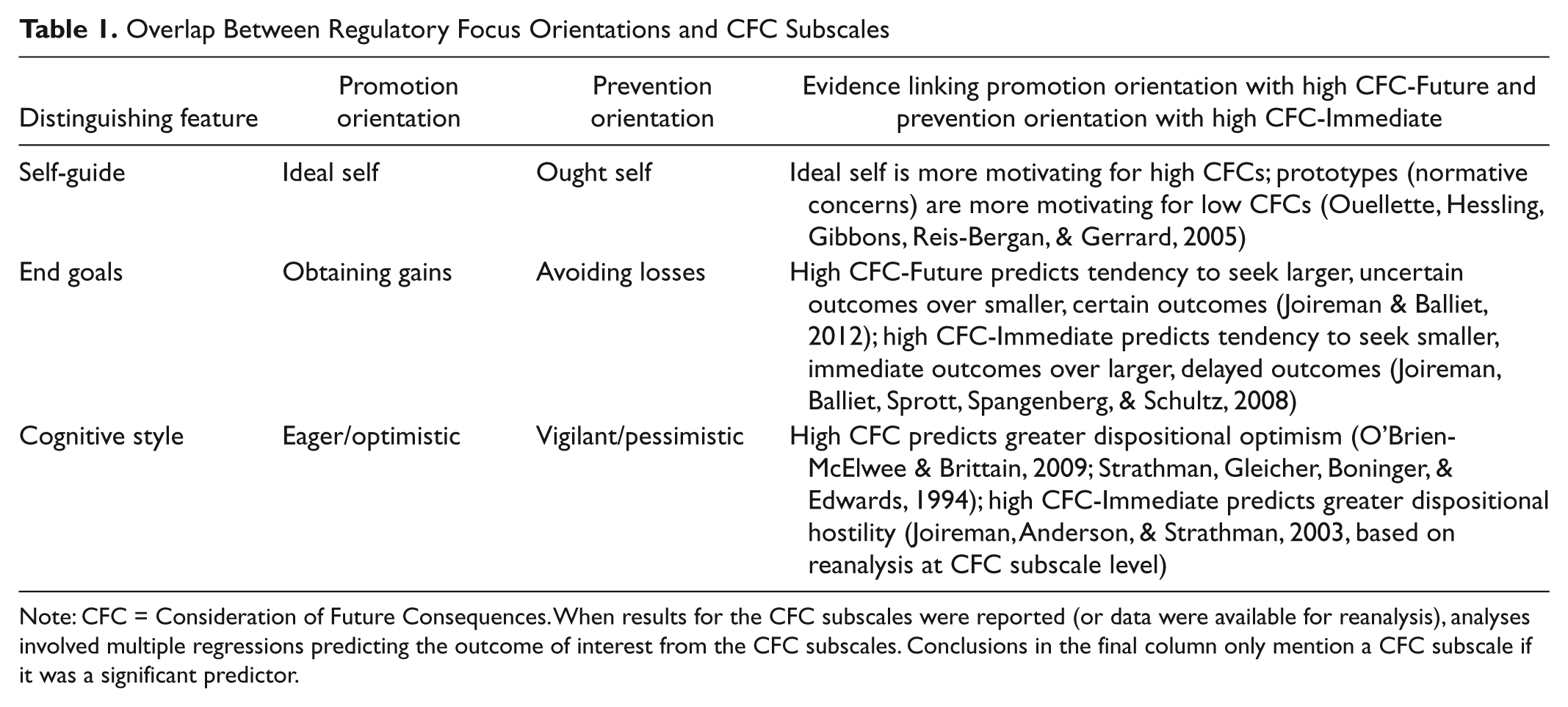
Note: CFC = Consideration of Future Consequences. When results for the CFC subscales were reported (or data were available for reanalysis), analyses involved multiple regressions predicting the outcome of interest from the CFC subscales. Conclusions in the final column only mention a CFC subscale if it was a significant predictor.
Complementing the above “common correlates,” research has also shown that consumers who are considering a distant purchase prefer promotion-framed products, whereas those who are considering an immediate purchase prefer prevention-framed products (Mogilner, Aaker, & Pennington, 2008). Even more directly relevant, Zacher and de Lange (2011) reported that future time orientation is positively correlated with a promotion orientation, whereas present time orientation is positively correlated with a prevention orientation though, as we note below, the authors’ conceptualization of time orientation was not identical to our focus on CFC.
Hypotheses
Based on the CFC/health behavior reviewed at the outset of our article, we predicted that the CFC-Future (CFC-Immediate) subscale would be positively (negatively) correlated with exercise and healthy eating attitudes and intentions. Building on the theoretical and empirical considerations just presented, we further hypothesized that those scoring high in CFC-Future should be more likely than those scoring low in CFC-Future to (chronically) adopt a promotion orientation, while those scoring high on CFC-Immediate should be more likely than those scoring low on CFC-Immediate to (chronically) adopt a prevention orientation. Finally, following this reasoning, we tested the hypothesis that promotion orientation would mediate the link between CFC-Future and exercise/healthy eating outcomes, whereas prevention orientation would mediate the link between CFC-Immediate and exercise/healthy eating outcomes.
Competing Hypotheses
Although the studies just reviewed provide conceptual support for our hypothesis, at least two studies have shown that those scoring high in CFC are more likely than those scoring low to respond favorably to “vigilant” messages. In one study, Kees et al. (2010) showed that low and high CFCs had similar risk perceptions and attitudes toward ads promoting a healthy diet and exercise using an “eager” style (e.g., seek healthy foods, seek exercise), whereas high CFCs had higher risk perceptions and more favorable attitudes toward ads using a vigilant strategy (e.g., avoid unhealthy foods, avoid inactivity). In another study, high CFCs spent more time reading information on testing for hypertension when the information was presented in a loss frame, whereas low CFCs spent more time reading the information when it was presented in a gain frame (O’Connor et al., 2009). Taken together, these studies suggest a competing set of hypotheses, namely, that high levels of CFC-Future will be related to a prevention orientation, whereas high levels of CFC-Immediate will be related to a promotion orientation.
We should also note that Zacher and de Lange’s (2011) study mentioned earlier suggested that regulatory focus (Lockwood, Jordan, & Kunda, 2002) precedes time orientation (Lang & Carstensen, 2002). Although Zacher and de Lange’s (cross-lagged panel) findings suggest that CFC may mediate the effect of regulatory style, it is important to recognize that their operationalization of future and present orientation is much different than our focus on CFC. In their study, Zacher and de Lange operationalized “future orientation” in terms of optimism over future “opportunities” and “present orientation” in terms of pessimism over future “limitations.” Arguably, Zacher and de Lange operationalize time orientation in more narrow and perhaps transient terms (a perception that one currently has future opportunities vs. limitations). By contrast, we focus on broader individual differences in the tendency to consider the future (vs. immediate) consequences of one’s actions, which we have argued theoretically give rise to (i.e., better fit with) promotion and prevention styles, respectively. Nevertheless, in light of Zacher and de Lange’s findings, we test the competing model suggesting that CFC mediates the link between regulatory style and exercise and healthy eating outcomes.
Overview of Studies
To further evaluate the nature of the CFC construct, and its links with regulatory focus, exercise, and healthy eating, we conducted two studies. In Study 1, we performed an exploratory factor analysis of the new CFC-14 scale and tested a structural model positioning regulatory focus as a mediator between the CFC subscales and exercise attitudes and intentions. In Study 2, we used confirmatory factor analysis on the CFC-14 scale to compare the fit of a one-factor and a two-factor model, and we tested a structural model positioning regulatory focus as a mediator between the CFC subscales and healthy eating attitudes and intentions.
Study 1
Exploratory Factor Analysis of the CFC-14 Scale and Links to Exercise
Method
Participants and procedure
Students enrolled in an introductory marketing class at a large state university participated for course credit. The sample (N = 119, 76% Caucasian) included 71 males and 48 females, with a median age of 21. All measures were completed via an online survey administered in a 10-station computer lab.
Measures
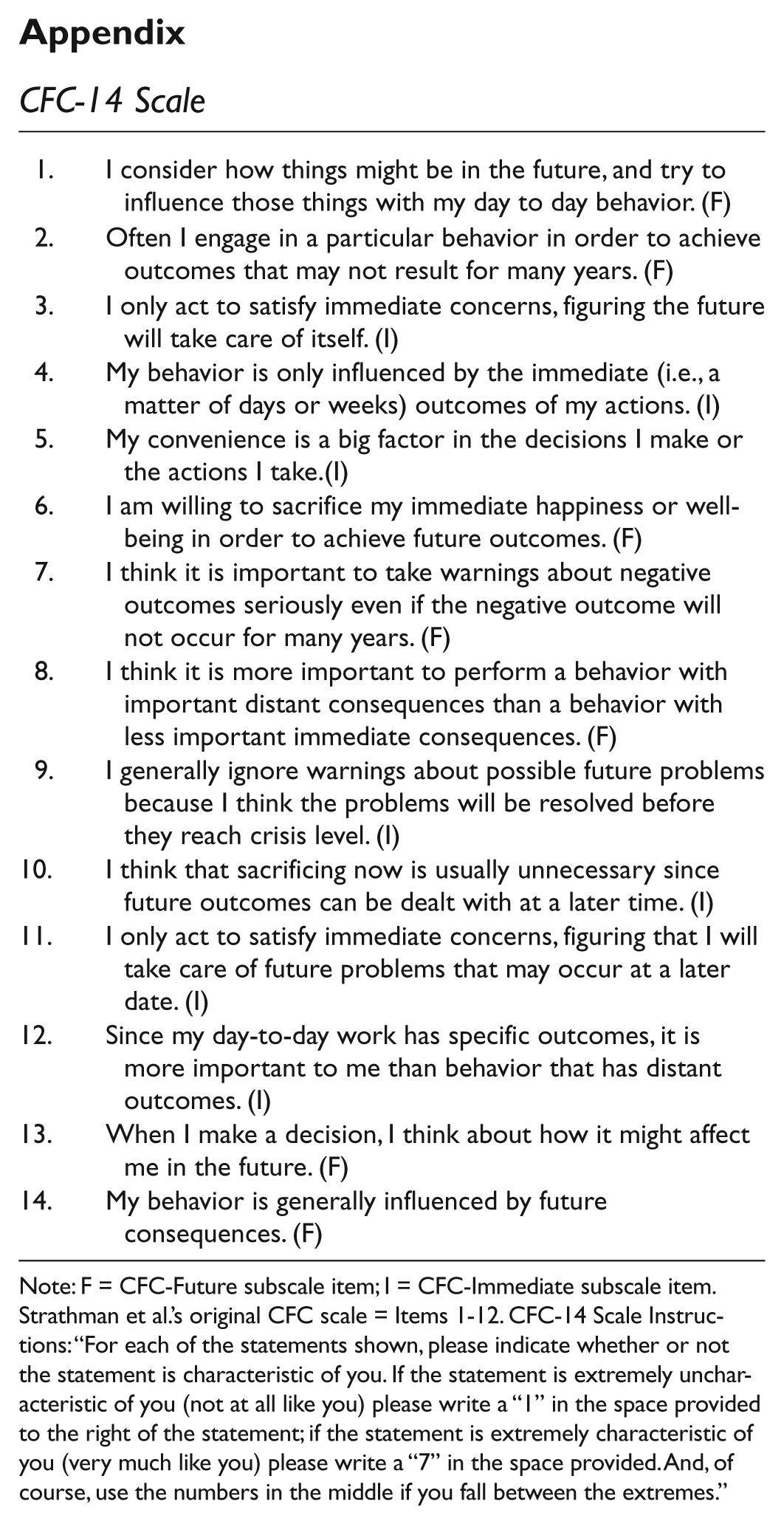
As part of a larger survey, participants completed Strathman et al.’s (1994) original CFC-12 scale, along with two additional (future-oriented) items. All items on the CFC-14 scale are shown in the appendix. The two new items were written by the first author and were designed to assess, as directly as possible, a “concern with future consequences” proper. Participants responded to each item on a 7-point scale (1 = very uncharacteristic of me; 7 = very characteristic of me). 3 In addition to the CFC-14 scale, participants completed Lockwood et al.’s (2002) 18-item measure of regulatory orientation (1 = not at all true of me; 7 = very true of me). Lockwood et al.’s scale contains two subscales assessing the strength of a promotion orientation (e.g., I frequently imagine how I will achieve my hopes and aspirations.) and a prevention orientation (e.g., In general, I am focused on preventing negative events in my life.), respectively. Both scales showed high internal reliability (Cronbach’s α = .84 and .80). 4
To gather evidence for the predictive validity of the CFC subscales, and mediation via regulatory focus, we also assessed exercise attitudes and intentions. Exercise attitudes were assessed with three items: (a) regular physical exercise is essential to good health, (b) regular physical activity makes one feel better, and (c) I enjoy physical activity. (Cronbach’s α = .72). Future exercise intentions were assessed with a single item: “Next week, how many times do you plan to exercise (how many different exercise sessions)?”
Results
Exploratory factor analysis
We submitted the CFC-14 to a principal components analysis followed by oblimin rotation. We used an oblimin rotation, as past research has shown that the CFC-Future and CFC-Immediate subscales are (negatively) correlated (e.g., Joireman et al., 2008). Prior to conducting the analysis, we examined three measures to assess the suitability of the data for factor analysis (Field, 2009): The Kaiser–Meyer–Olkin measure (KMO = .85) was acceptably high (in the “very good” range; Field, 2009); the determinant of the correlation matrix was .004 (exceeding the recommended .00001 value and ruling out multicollinearity); and Bartlett’s test of sphericity was significant, χ2(91) = 614.86, p < .001, revealing that the correlations were acceptably large for Principal Component Analysis (PCA). Turning to the main analysis, three eigenvalues exceeded 1 (5.02, 2.14, 1.04), suggesting the possibility of three factors. However, the eigenvalue > 1 criterion is known to lead to overextraction of factors (Zwick & Velicer, 1986). In addition, an examination of the scree plot (Cattell, 1966) clearly suggested the presence of two factors (see Figure 1). The two factors explained 51.2% of the variance and were negatively but not strongly correlated (Φ = −.27). The rotated item loadings on the two factors from the pattern matrix are shown in Table 2. As can be seen, all items loaded on their expected factor, and only one item showed a cross loading >.30. A reliability analysis further revealed that the seven-item CFC-Future and CFC-Immediate subscales were highly reliable (respective Cronbach’s αs = .80 and .84). As expected, we also found that the internal reliability of the original five-item CFC-Future subscale was relatively low (α = .70), compared with the seven-item CFC-Future subscale.
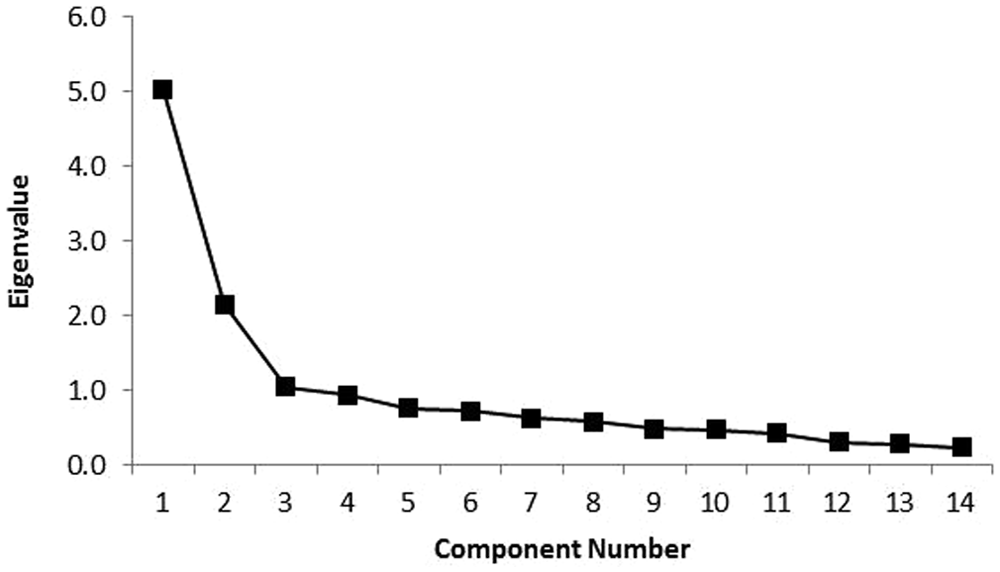
Scree plot of the CFC-14 Scale (Study 1)
Rotated Factor Loadings (Study 1)
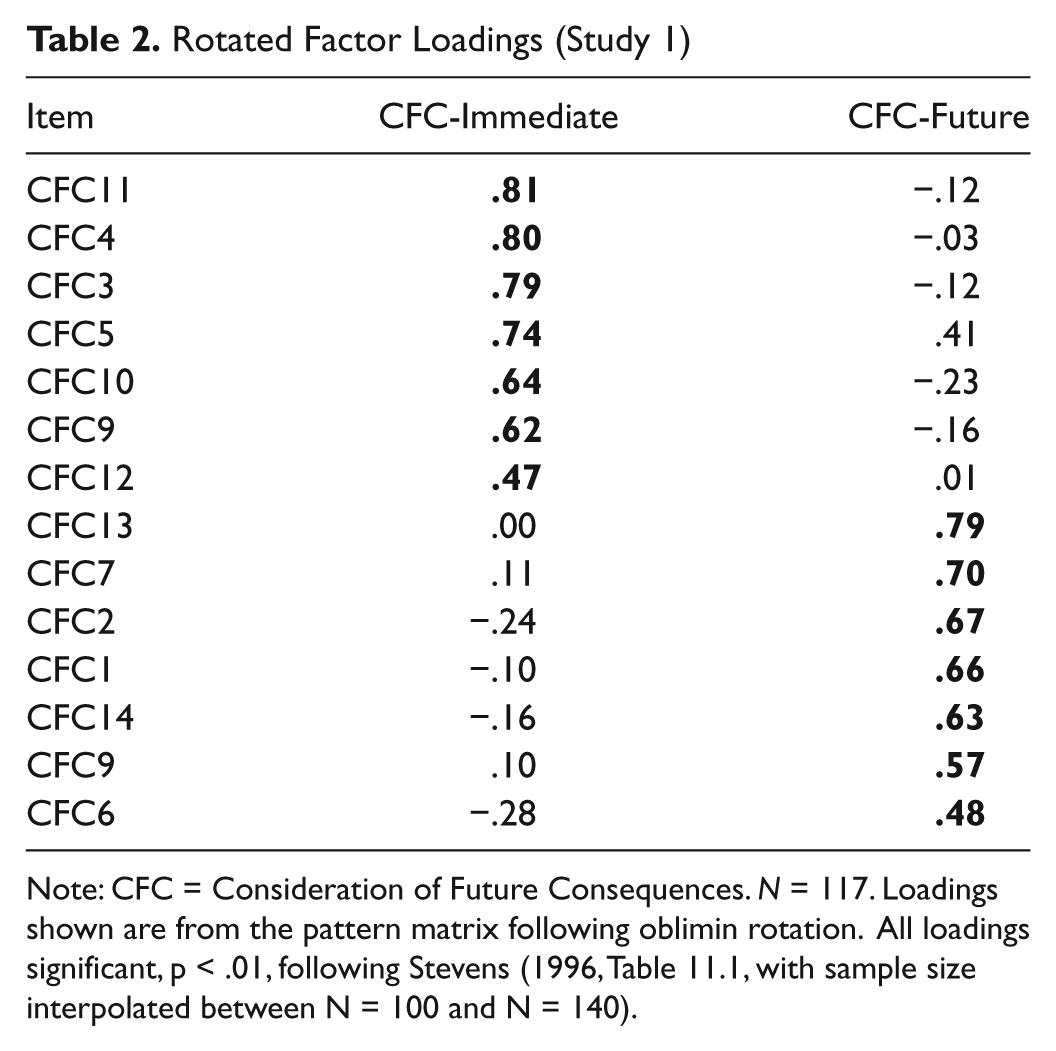
Note: CFC = Consideration of Future Consequences. N = 117. Loadings shown are from the pattern matrix following oblimin rotation. All loadings significant, p < .01, following Stevens (1996, Table 11.1, with sample size interpolated between N = 100 and N = 140).
Predicting regulatory orientation, exercise attitudes, and intentions
In the introduction, we argued that evidence for a two-factor solution should move beyond factor analysis and include an examination of the CFC subscales’ ability to differentially predict relevant outcomes. Accordingly, in the present study, we evaluated whether the CFC-Future and CFC-Immediate subscales differentially predict regulatory orientation and exercise attitudes and intentions. We also explored whether regulatory orientation would mediate the relationship between the two CFC subscales and the various exercise outcomes. Table 3 presents the simple correlations among all relevant variables. To summarize, CFC-Future showed a strong positive correlation with scores on the promotion scale, as well as exercise attitudes and intentions. Promotion orientation was positively related to exercise attitudes and intentions. And exercise attitudes were positively related to exercise intentions. CFC-Immediate correlated negatively with promotion orientation and was not significantly correlated with the exercise outcomes. 5
Correlations and Descriptive Statistics (Study 1)
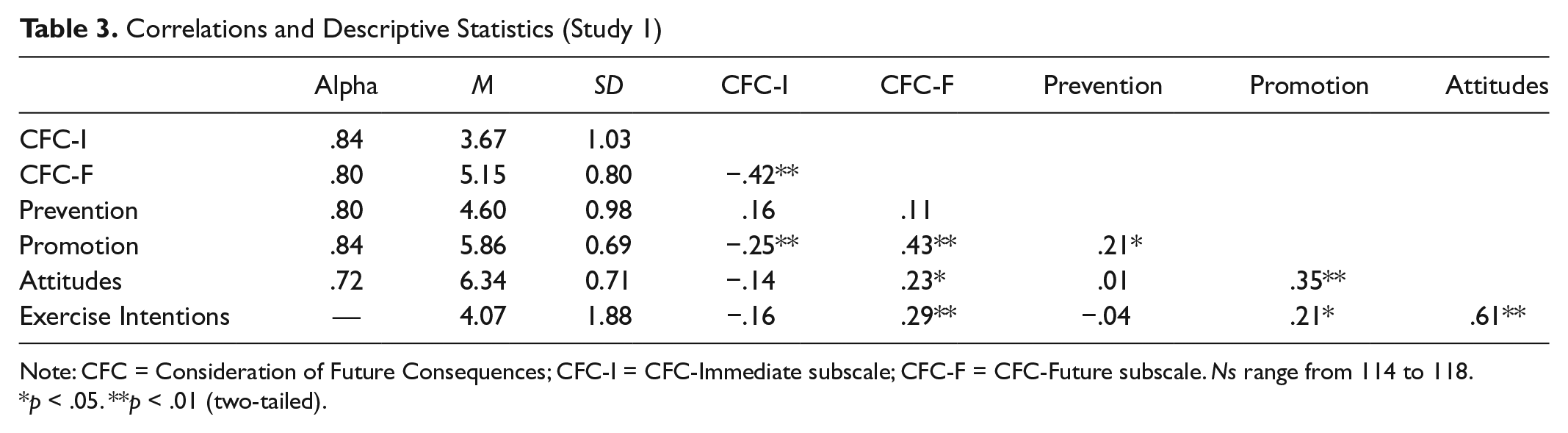
Note: CFC = Consideration of Future Consequences; CFC-I = CFC-Immediate subscale; CFC-F = CFC-Future subscale. Ns range from 114 to 118.
p < .05. **p < .01 (two-tailed).
Complementing these analyses, we next performed a path analysis to test whether regulatory orientation mediated between the CFC subscales and exercise attitudes, which in turn would predict exercise intentions. As shown in Figure 2, the path model fits the data well. 6 Following up on the path analysis, we conducted focused tests of the indirect effects implied by the model using the bootstrapping procedure developed by Preacher and Hayes (2008; see also Zhao, Lynch, & Chen, 2010). A summary of these analyses, shown in Table 4, provided good support for the proposed indirect links (with respect to CFC-Future). 7
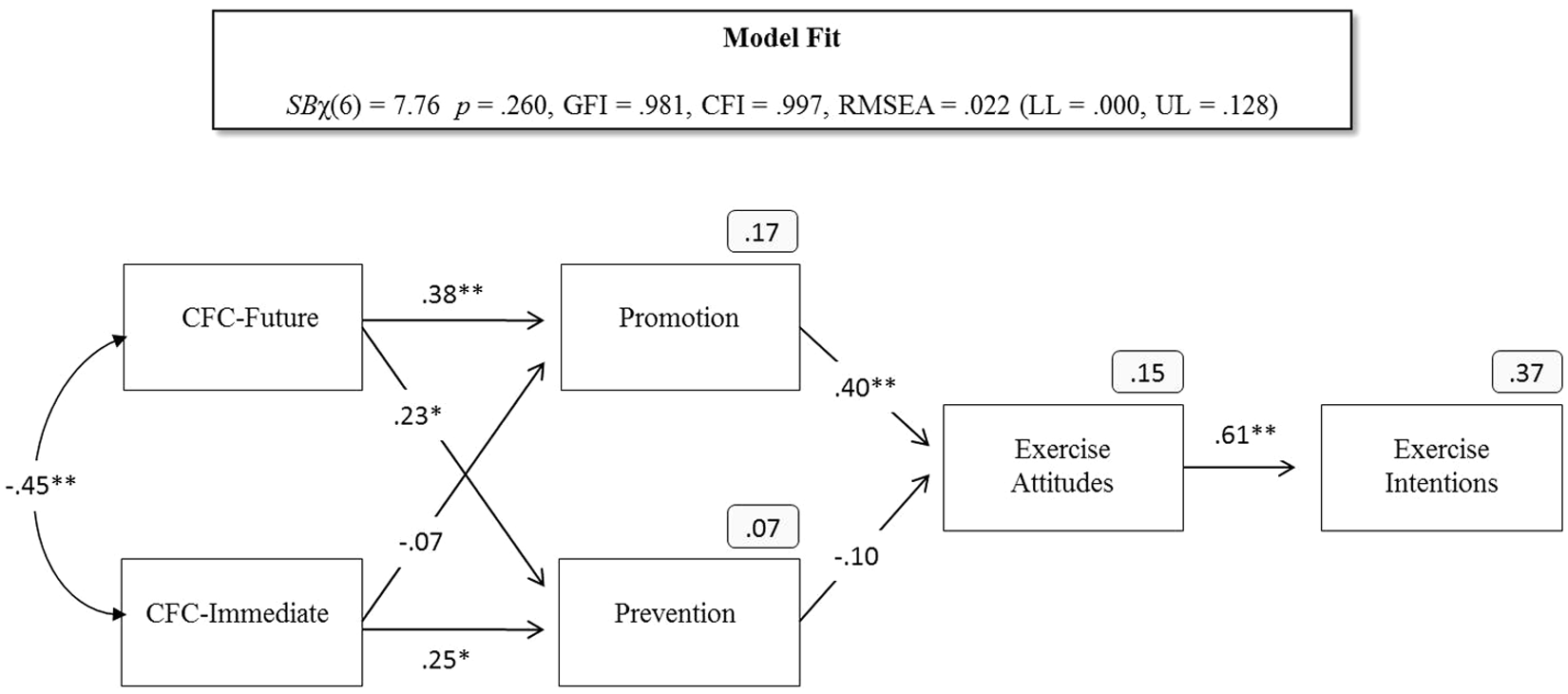
Path model linking CFC subscales with exercise outcomes via regulatory focus orientation (Study 1)
Summary of Indirect Effects Tests
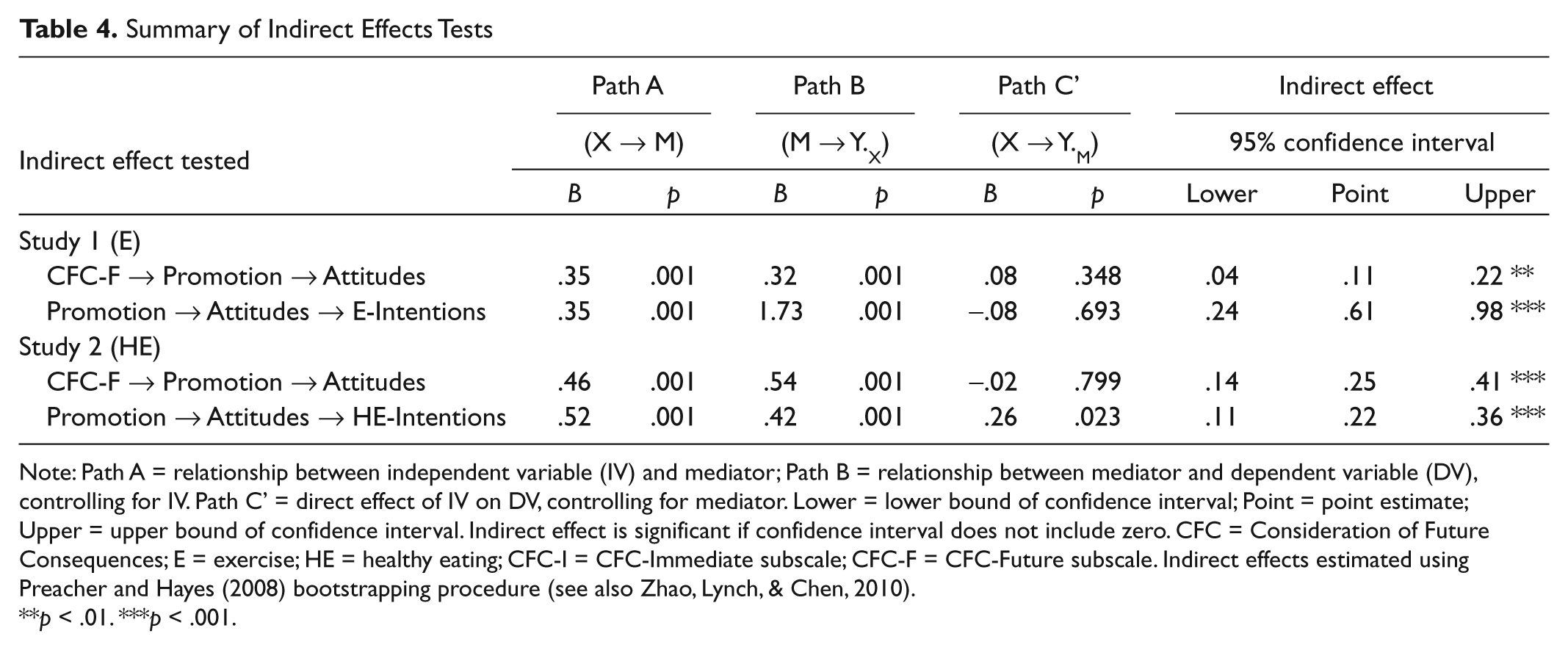
Note: Path A = relationship between independent variable (IV) and mediator; Path B = relationship between mediator and dependent variable (DV), controlling for IV. Path C’ = direct effect of IV on DV, controlling for mediator. Lower = lower bound of confidence interval; Point = point estimate; Upper = upper bound of confidence interval. Indirect effect is significant if confidence interval does not include zero. CFC = Consideration of Future Consequences; E = exercise; HE = healthy eating; CFC-I = CFC-Immediate subscale; CFC-F = CFC-Future subscale. Indirect effects estimated using Preacher and Hayes (2008) bootstrapping procedure (see also Zhao, Lynch, & Chen, 2010).
p < .01. ***p < .001.
Discussion
The present study yielded two important findings. First, in line with five recent articles (Adams, 2012; Joireman et al., 2008; Petrocelli, 2003; Rappange et al., 2009; Toepoel, 2010), the present study supported the presence of two underlying factors on the new CFC-14 scale (CFC-Future and CFC-Immediate), both of which were highly reliable. Second, the present study provided initial support for the hypothesis that the CFC-Future subscale would predict favorable exercise attitudes and intentions through its relationship with a promotion-oriented regulatory style. Moreover, in partial support of our second hypothesis, scores on the CFC-Immediate subscale were positively related to a prevention-oriented style (although, unexpectedly, so were scores on the CFC-Future subscale). In an effort to replicate and extend these findings, Study 2 used confirmatory factor analysis to compare the fit of a one-factor versus a two-factor model on the CFC-14 scale, and structural equation modeling to test the proposed links between CFC, regulatory focus, and healthy eating attitudes and intentions.
Study 2
Confirmatory Factor Analysis of the CFC-14 Scale and Links to Healthy Eating
Method
Participants and procedure
Students enrolled in an introductory marketing class at a large state university participated for course credit. The sample (N = 232, 80% Caucasian) included 118 males and 114 females, with a median age of 21. As in Study 1, all measures were completed via an online survey administered in a 10-station computer lab.
Measures
Participants completed the CFC-14 scale and the Lockwood et al. (2002) regulatory focus measure described in Study 1 (αs: CFC-Future = .82, CFC-Immediate = .84, Promotion = .86, Prevention = .80). In addition, to gather evidence for the predictive validity of the CFC subscales, and mediation via regulatory focus, we assessed healthy eating attitudes and intentions. Healthy eating attitudes were assessed with three items: (a) Eating healthy is essential to my well-being, (b) I enjoy eating healthy, and (c) I feel great personal satisfaction when I eat healthy (α = .81). Healthy eating intentions were assessed by asking participants to think about future breakfasts, lunches, and dinners and to rate how healthy those meals would be (1 = not healthy; 10 = very healthy; α = .81).
Results
Confirmatory factor analysis
To test the validity of the two-factor (vs. one-factor) models, we conducted confirmatory factor analysis. We began by evaluating the fit of the hypothesized two-factor model. The initial two-factor model showed a reasonable fit to the data, Sattora-Bentler (SB) χ2(76) = 164.85, p < .001, Goodness of Fit Index (GFI) = .890, Comparative Fit Index (CFI) = .892, root mean square error approximation (RMSEA) = .072 (lower limit [LL] = .057, upper limit [UL] = .087). However, to achieve acceptable fit (GFI and CFI near .95, and RMSEA below .05; Hu & Bentler, 1999), it was necessary to estimate seven correlated error terms. The final model, shown in Figure 3, fit the data well, SBχ2(69) = 97.69, p = .013, GFI = .943, CFI = .965, RMSEA = .043 (LL = .020, UL = .062). As can be seen, the correlation between the factors was not especially large (Φ = −.37), and the majority of the correlated errors were understandable, given the common wording on the correlated items (e.g., Items 2 and 6 contain the phrase “achieve future outcomes”; Items 3 and 4 mention “immediate concerns”; Items 6 and 10 mention “sacrificing”; and Items 7 and 9 mention “warnings”). Next, we estimated a one-factor model, including all of the correlated error terms shown in Figure 2, to make the model comparison a fair test of the differences between the models (i.e., the only difference between the models is the number of underlying factors hypothesized). The one-factor model, with the same correlated errors as shown in our final model, fit the data very poorly, SBχ2(70) = 329.90, p < .001, GFI = .734, CFI = .685, RMSEA = .129 (LL = .115, UL = .143). Furthermore, a direct comparison of the two models showed that the two-factor model fit the data significantly better than the one-factor model, SBχ2Δ(1) = 38.97, p < .001. In addition, if the correlation between the two factors is set to 1 (Benson & Hocevar, 1985), model fit is poor, SBχ2(70) = 222.10, p < .001, GFI = .896, CFI = .816, RMSEA = .099 (LL = .084, UL = .113), and is significantly worse than when the correlation between the factors is freely estimated, SBχ2Δ(1) = 38.97, p < .001. As noted earlier, and replicating Study 1, reliability analysis indicated that both of the CFC subscales showed impressive internal reliabilities (CFC-Future = .82; CFC-Immediate = .80). As before, the reliability of the original five-item CFC-Future subscale was acceptable but was again lower (α = .74) than the reliability of the seven-item CFC-Future subscale.
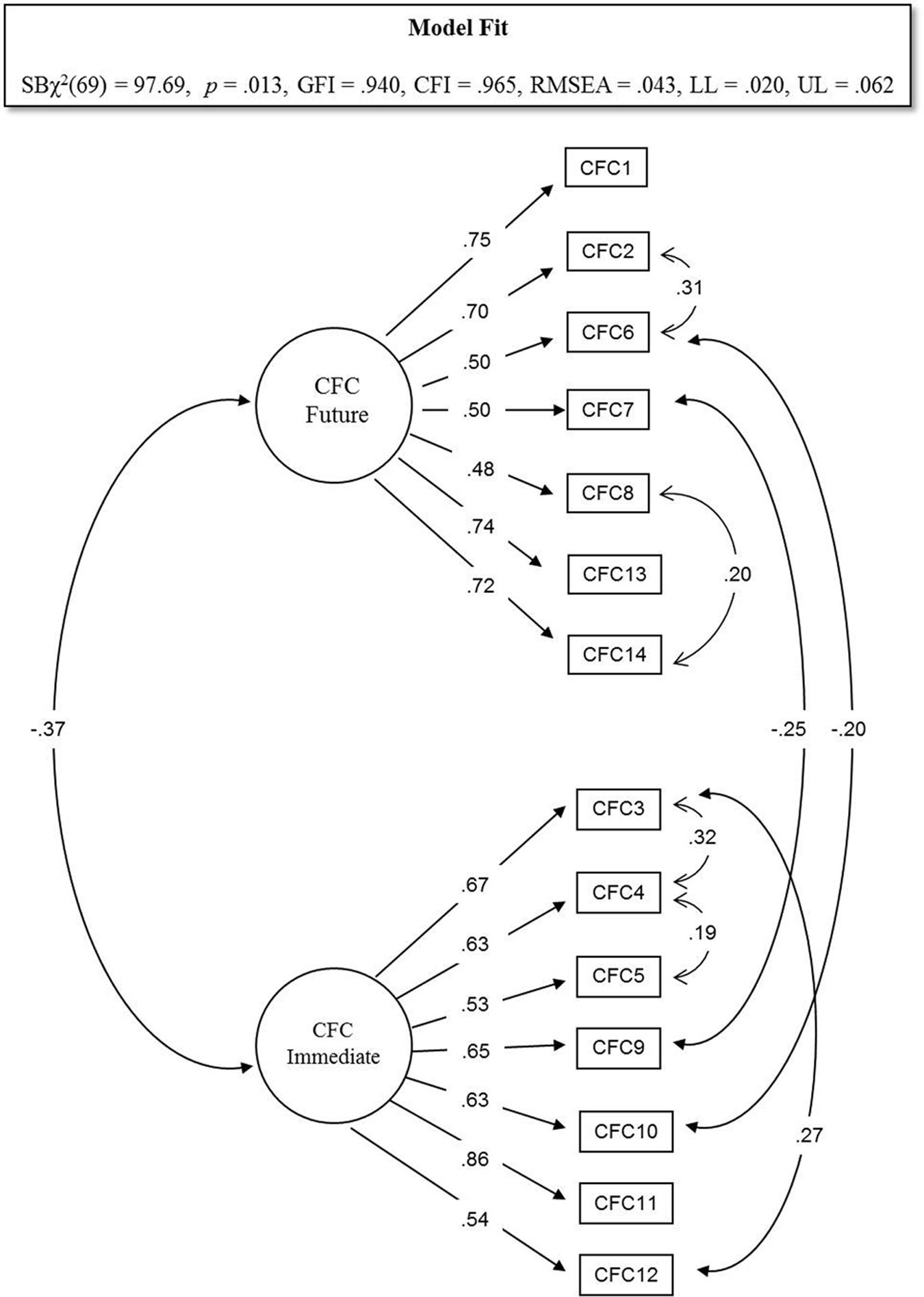
Confirmatory factor analysis of the CFC-14 Scale (Study 2)
Predicting regulatory orientation, healthy eating attitudes, and intentions
As in Study 1, we collected additional data to evaluate whether the two CFC subscales would differentially predict regulatory orientation and healthy eating attitudes and intentions. We also examined whether regulatory orientation would mediate the relations between the two CFC subscales and the healthy eating outcomes.
Table 5 presents the simple correlations among all relevant variables. To summarize, CFC-Future again showed a strong positive correlation with scores on the promotion scale, and moderate (but significant) positive relationships with healthy eating attitudes and future intentions. Promotion orientation was positively related to healthy eating attitudes as well as healthy eating intentions. Finally, healthy eating attitudes were positively correlated with healthy eating intentions. CFC-Immediate, by comparison, correlated negatively with promotion orientation, positively with prevention orientation, and was not significantly correlated with the healthy eating outcomes.
Correlations and Descriptive Statistics (Study 2)
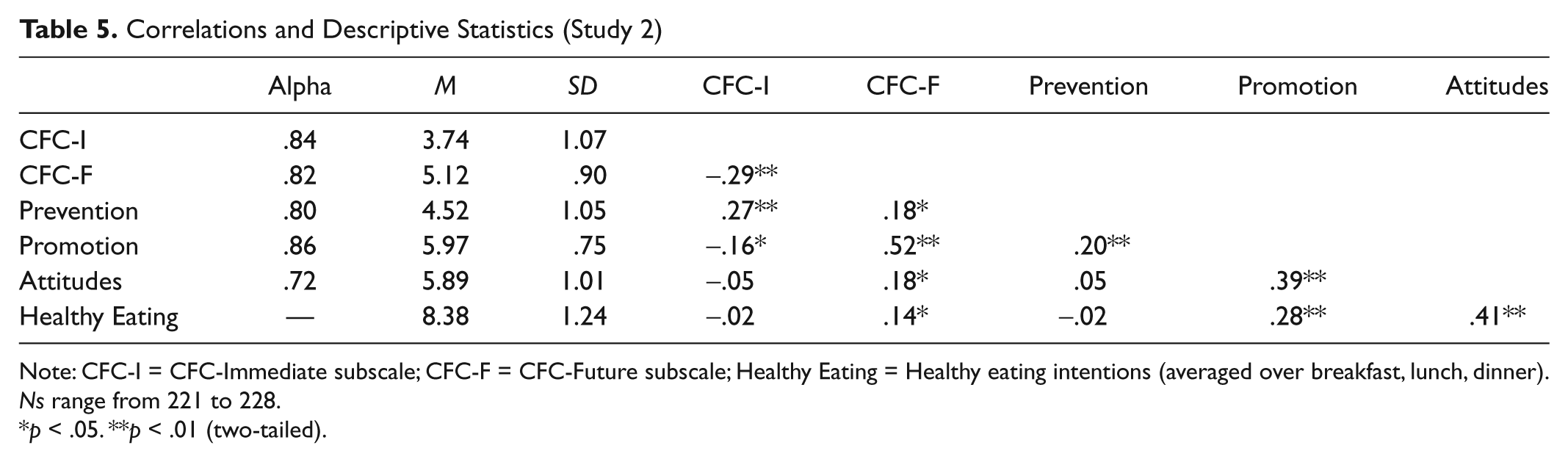
Note: CFC-I = CFC-Immediate subscale; CFC-F = CFC-Future subscale; Healthy Eating = Healthy eating intentions (averaged over breakfast, lunch, dinner). Ns range from 221 to 228.
p < .05. **p < .01 (two-tailed).
Complementing these analyses, we next performed a path analysis to test whether regulatory orientation mediated between the CFC subscales and healthy eating attitudes, which in turn would predict healthy eating intentions. The path model testing this sequence (Figure 4) fit the data well. 8 Following up on the path analysis, we conducted focused tests of the indirect effects implied by the model using the bootstrapping procedure developed by Preacher and Hayes (2008; see also Zhao et al., 2010). A summary of these analyses provided strong support for the three mediation paths implied by the model (Table 4).
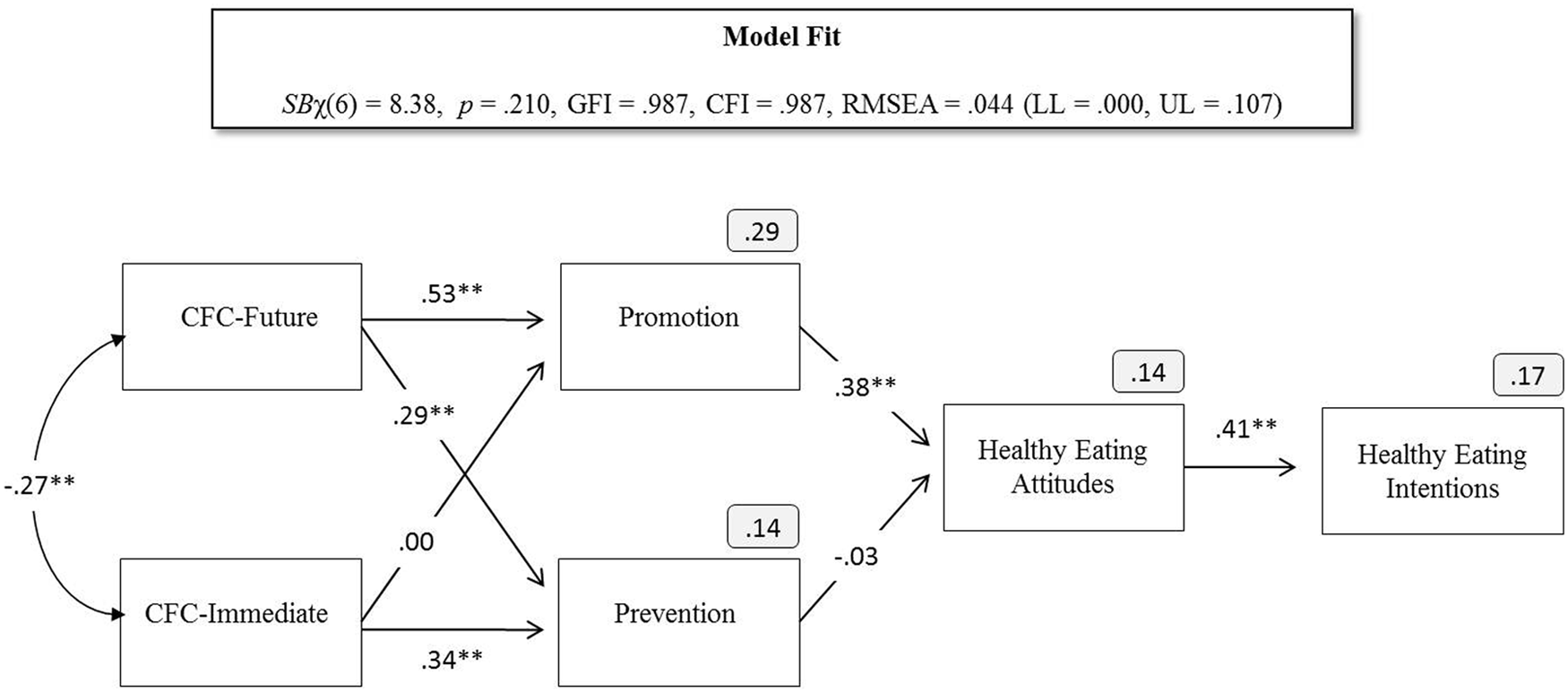
Path model linking CFC subscales with healthy eating outcomes via regulatory focus orientation (Study 2)
Discussion
Using confirmatory factor analysis, the present study provided additional support for the presence of two CFC subfactors on the revised CFC-14 scale, both of which were highly reliable. The present study also conceptually replicated our earlier findings by showing that a promotion orientation mediated the relationship between CFC-Future and healthy eating attitudes and intentions. Finally, consistent with our earlier findings, CFC-Future and CFC-Immediate were both equally (and positively) related to scores on the prevention orientation scale.
General Discussion
Over the past several decades, obesity has risen dramatically in the United States. Currently, it is estimated that roughly two thirds of Americans are overweight (with a BMI ≥ 25) and one third of Americans are obese (with a BMI ≥ 30; Flegal, Carroll, Ogden, & Curtin, 2010). Two of the most important steps people can take to curb obesity include engaging in regular exercise and eating a healthy diet. Unfortunately, because the alternatives (physical inactivity and a poor diet) offer more immediate benefits, many people fail to exercise and eat healthy foods. Given the intertemporal nature of such health behavior decisions, one factor that influences whether an individual exercises and follows a healthy diet is their CFC (Strathman et al., 1994). The present studies helped shed light on how CFC relates to exercise and healthy eating in two ways. First, consistent with five recent studies (Adams, 2012; Joireman et al., 2008; Petrocelli, 2003; Rappange et al., 2009; Toepoel, 2010), we provided evidence that responses to the new CFC-14 scale are best captured by two underlying factors: a seven-item CFC-Future subscale and a seven-item CFC-Immediate subscale. Second, we showed that a promotion orientation (Higgins et al., 2001; Lockwood et al., 2002) mediates the relationship between CFC-Future, on one hand, and exercise and healthy eating attitudes and intentions on the other hand. As detailed below, these results help extend work on CFC and health behavior by further supporting the discriminant validity of the two subscales, enhancing reliability of the CFC-Future subscale, and identifying a mediator between CFC-Future and two behaviors important in promoting healthy lifestyles and reducing obesity (exercise and healthy eating).
Extensions of the CFC-Health Behavior Literature
In 1994, Strathman and colleagues introduced the 12-item CFC scale to help researchers assess the extent to which people are concerned with and impacted by the future (vs. immediate) consequences of their behavior. Since that time, researchers have demonstrated that scores on the CFC scale predict a wide range of thoughts, feelings, and behaviors related to intertemporal decisions (for a broader review, see Joireman, Strathman, & Balliet, 2006). As summarized in our introduction, one important and highly productive line of CFC research has been in the area of health behavior. Although yielding important insights, most of this work has treated the CFC construct as a unidimensional construct, and few studies have attempted to understand why CFC predicts health-related outcomes. The present studies aimed to address these gaps in the literature.
As noted, our results provide additional support for the presence of two underlying CFC factors (CFC-Future and CFC-Immediate). This distinction is important because separating the two subscales adds clarity to CFC’s relationship with a given outcome. If researchers continue to reverse code the immediate items and then average over the entire set of CFC items, they will end up with a single CFC score, which may predict behavior, but whose interpretation is unclear. A positive correlation between CFC and a given outcome of interest (say exercise) can mean the following:
that those who are concerned with the future consequences of their behavior (proper) are more likely to exercise,
that those who are concerned with the immediate consequences of their behavior are less likely to exercise, or
both.
By clearly separating the future from the immediate items, a researcher can clearly tease apart these different explanations. Although the use of two CFC subscales will introduce some complexity to the analysis (and theorizing), we believe (based on our own findings and previous research; Joireman et al., 2008, 2010; Rappange et al., 2009) that the additional steps will be worth the effort, primarily because the distinction will help shed a more nuanced light on the relationship between CFC and a researcher’s given outcome of interest.
In particular, distinguishing between CFC-Future and CFC-Immediate allows a researcher to test the buffering and susceptibility hypotheses advanced by Joireman et al. (2008). These hypotheses hold important practical implications within the health domain. If CFC-Future is the primary predictor of a given health behavior, the buffering hypothesis is supported, and interventions should focus on encouraging people to value and become aware of the future consequences of their actions. On the other hand, if CFC-Immediate is the primary predictor, the susceptibility hypothesis is supported and interventions should focus on reducing a concern with the immediate consequences of an action or eliminating them altogether. Put in broader theoretical terms, the buffering hypothesis assumes that activation of a “cool,” conscious, and rational system will promote health behaviors, whereas the susceptibility hypothesis assumes that reducing the salience of “hot” triggers will lower the likelihood of unhealthy behaviors directed by unconscious impulses for immediate gratification (Metcalfe & Mischel, 1999).
In addition to shedding light on the underlying nature of the CFC construct, the present studies provided additional insight into why individual differences in CFC relate to health behavior. Specifically, we found that people scoring high on the CFC-Future subscale are more likely to exercise and eat healthfully because they adopt a promotion-oriented regulatory style. Based on theoretical arguments and empirical data offered in the introduction, we anticipated this. However, as we noted, it was equally plausible, based on some other studies that CFC-Future would be more closely linked with a prevention-oriented style. One possible reason for the difference in our results is that the current study directly correlated CFC with individual differences in regulatory focus, whereas the previously noted studies inferred that those scoring high in CFC adopt a prevention orientation based on their response and attention to persuasive messages. Clearly, future research is needed to better understand the link between CFC, regulatory focus, and health behaviors. Nevertheless, the current studies do seem to converge on the conclusion that, at the level of individual differences, those scoring high on the CFC-Future subscale adopt a promotion-oriented regulatory style. That said, results across both studies showed a secondary, small but significant positive relationship between CFC-Future and prevention orientation, suggesting that those scoring high on CFC-Future primarily aim to promote positive outcomes but are also attuned to preventing negative outcomes. However, in the present studies, prevention orientation was not related to the outcomes of interest, suggesting that the key path from CFC-Future to health outcomes runs through a promotion orientation.
Limitations and Future Directions
Before closing, we consider some limitations of the present studies and suggest several directions for future research. First, the current data are based on single administration, correlational data. As such, future research would benefit by looking at how CFC, regulatory focus, and health behavior relate over time. Second, the current data are based on self-reports. Future research incorporating actual behavioral measures would strengthen confidence in our findings. Third, although demonstrating a meaningful link between individual differences in CFC and regulatory focus, our data do not address the underlying mechanism that might link the two constructs. One possibility is that CFC predicts temporal discounting, delay of gratification, and/or temporal construals (e.g., Daly, Delaney, & Harmon, 2009; Joireman et al., 2006; Joireman et al., 2008), which in turn encourage the adoption of a promotion orientation. Finally, the current studies focused on two specific health behaviors. Given that CFC predicts a much wider range of outcomes, including academic performance (e.g., Joireman, 1999), financial decision making (e.g., Howlett, Kees, & Kemp, 2008), and environmental behavior (e.g., Ebreo & Vining, 2001; Kortenkamp & Moore, 2006), future research could examine whether regulatory focus explains the link between CFC and these other important outcomes.
Conclusion
Recently, the Centers for Disease Control and Prevention (CDC; 2011) advanced the “Healthy People 2020” initiative to support America’s efforts in becoming a “society in which all people live long, healthy lives.” Specifically, the CDC outlined a 10-year plan to improve the health of all Americans by providing science-based insights to help people make informed health decisions and monitor their health behaviors. To achieve such ambitious goals, it is important to understand the underlying mechanisms that influence health behaviors such as exercise and healthy eating. The present studies contributed to that effort by studying the relationship between CFC, regulatory focus, and health behaviors related to a host of important outcomes (e.g., weight control, diabetes, cardiovascular health). Across two studies, we found that individuals concerned with the future consequences of their actions (i.e., those scoring high on the CFC-Future subscale) had more favorable attitudes toward, and stronger intentions to engage in health-related behaviors (exercise and healthy eating) because they adopt a promotion orientation. We also found that concern with immediate consequences (i.e., the CFC-Immediate subscale) and prevention orientation were not related to exercise and healthy eating outcomes. These findings suggest that efforts to reach the CDC’s goals focus on promoting positive future benefits of exercise and healthy eating.
Footnotes
Appendix
CFC-14 Scale
| 1. | I consider how things might be in the future, and try to influence those things with my day to day behavior. (F) |
| 2. | Often I engage in a particular behavior in order to achieve outcomes that may not result for many years. (F) |
| 3. | I only act to satisfy immediate concerns, figuring the future will take care of itself. (I) |
| 4. | My behavior is only influenced by the immediate (i.e., a matter of days or weeks) outcomes of my actions. (I) |
| 5. | My convenience is a big factor in the decisions I make or the actions I take.(I) |
| 6. | I am willing to sacrifice my immediate happiness or well-being in order to achieve future outcomes. (F) |
| 7. | I think it is important to take warnings about negative outcomes seriously even if the negative outcome will not occur for many years. (F) |
| 8. | I think it is more important to perform a behavior with important distant consequences than a behavior with less important immediate consequences. (F) |
| 9. | I generally ignore warnings about possible future problems because I think the problems will be resolved before they reach crisis level. (I) |
| 10. | I think that sacrificing now is usually unnecessary since future outcomes can be dealt with at a later time. (I) |
| 11. | I only act to satisfy immediate concerns, figuring that I will take care of future problems that may occur at a later date. (I) |
| 12. | Since my day-to-day work has specific outcomes, it is more important to me than behavior that has distant outcomes. (I) |
| 13. | When I make a decision, I think about how it might affect me in the future. (F) |
| 14. | My behavior is generally influenced by future consequences. (F) |
Note: F = CFC-Future subscale item; I = CFC-Immediate subscale item. Strathman et al.’s original CFC scale = Items 1-12. CFC-14 Scale Instructions: “For each of the statements shown, please indicate whether or not the statement is characteristic of you. If the statement is extremely uncharacteristic of you (not at all like you) please write a “1” in the space provided to the right of the statement; if the statement is extremely characteristic of you (very much like you) please write a “7” in the space provided. And, of course, use the numbers in the middle if you fall between the extremes.”
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.