
Abstract
The consideration of future consequences (CFC) is a cognitive-motivational construct describing the extent to which individuals consider the future outcomes of behavior during decision-making. The current research examined the extent to which CFC may be a domain-specific, as opposed to global, temporal construct. Across three surveys, adults (n = 498; 66.9% female; 41.2% students) completed the 14-item general CFC scale, five newly adapted domain-specific CFC scales, and self-report measures of behavior in five substantive domains (work, health, the environment, money, and college). Confirmatory factor analyses replicated the two-factor model in the CFC-14, supporting the distinction between CFC-Future and CFC-Immediate in domain-specific CFC-14 scales. Hierarchical regression analyses indicated that domain-specific, and not the general, CFC subscales were most strongly associated with the relevant domain-specific behavior and revealed differential patterns of association between domain-specific CFC subscales and behaviors in particular domains. The applied implications for behavioral interventions are discussed.
Outcome expectancies are core aspects of human decision-making and behavior (Adams & Nettle, 2009). As behavioral outcomes tend to be temporally situated, understanding the nature of temporal individual difference constructs, as well as their impact on behavioral decision-making, is an important endeavor. The consideration of future consequences (CFC; Strathman, Gleicher, Boninger, & Edwards, 1994) is one of the most widely researched temporal constructs in psychological science. Defined by Strathman and colleagues as the extent to which individuals consider the future outcomes of their present day behavior, and the extent to which their decisions are influenced by these potential outcomes, individual differences in CFC have been linked to motivation, decision-making, goal pursuit, and behavior across a variety of important life domains, including work, health, the environment, finances, and education (for a review, see Joireman & King, 2016). To date, individual differences in CFC have predominantly been examined using general (or global) scale items under the assumption that CFC is a unitary, or domain-free, construct. Recent evidence, however, suggests that intertemporal decision-making may be domain-specific (e.g., Hardisty & Weber, 2009; McKay, Perry, Cole, & Magee, 2017). The current study examines the extent to which individual differences in CFC differ across five substantive life domains.
The CFC Scale: Background
In 1994, Strathman and colleagues introduced a 12-item measure to capture the extent to which individuals are concerned with the relatively immediate or more distant outcomes of their current actions. Exploratory and confirmatory factor analyses supported the presence of a unidimensional scale (the CFC-12) whereby total scores are calculated as the sum or average of the five future scale items and the seven reverse-coded immediate scale items. Low-scoring individuals are expected to prioritize maximizing immediate benefits and exhibit little regard for the potential future costs of their present day behavior. Conversely, high scorers are expected to prioritize the future implications of their current actions, and sacrifice immediate gratification to obtain long-term benefits (Strathman et al., 1994). For example, compared to low scorers, high scorers on the CFC-12 have been shown to be more likely to exercise (Ouellette, Hessling, Gibbons, Reis-Bergan, & Gerrard, 2005), eat healthily (Jakul, 2011), recycle (Bruderer Enzler, 2015), exhibit transformational leadership in stable work environments (Zhang, Wang, & Pearce, 2014), and engage in financial planning (Adams & Nettle, 2009).
In a more recent examination of the CFC-12 factor structure, Joireman, Balliet, Sprott, Spangenberg, and Schultz (2008) reported that a bidimensional conceptualization consisting of two underlying factors was psychometrically valid, as well as theoretically and practically advantageous. In this revised conceptualization, rather than manifest on a single continuum, the consideration of immediate and future consequences exist as two related, but discrete temporal constructs. The two-factor solution distinguished between a seven-item CFC-Immediate (CFC-I) subscale and a five-item CFC-Future (CFC-F) subscale. However, studies adopting this model often reported suboptimal reliability coefficients for the CFC-F factor (Joireman, Shaffer, Balliet, & Strathman, 2012), while other investigations of the scale’s psychometric validity found superior fit indices for a one-factor (e.g., Crockett, Weinman, Hankins, & Marteau, 2009) and a bifactor (e.g., McKay, Morgan, van Exel, & Worrell, 2015) model. Subsequently, Joireman and colleagues (2012) added two new future scale items to improve the psychometric properties and structural validity of the CFC scale. The revised 14-item CFC scale thus consists of two negatively correlated seven-item CFC subscales to distinguish between CFC-Future and CFC-Immediate.
Converging evidence supports the psychometric distinction between the CFC-F and CFC-I subscales within the CFC-14 (e.g., McKay, Perry, Percy, & Cole, 2016; Nigro, Cosenza, Ciccarelli, & Joireman, 2016), and this distinction is important to consider not only on a conceptual level, but also on a practical level. Differentiating between the subfactors facilitates a more precise understanding of whether concern for future or immediate behavioral consequences (or both) is more strongly associated with engagement in a particular behavior or a behavioral outcome. For example, Adams (2012) reported that an individual’s body mass index and smoking status were most strongly associated with scores on the CFC-I subscale, whereas Joireman et al. (2012) found that exercise and healthy eating motivation were most strongly associated with scores on the CFC-F subscale. Understanding these patterns of association, then, allows for more precise specification of bespoke behavior change interventions. For example, tailoring intervention content to emphasize either the long- or short-term motivational factors that facilitate behavioral uptake or cessation (Joireman et al., 2012).
Despite promising implications, a review of CFC literature to date evidences two notable concerns. First, studies of associations between CFC scores and behavior typically report small, and sometimes negligible, effect sizes (Murphy & Dockray, 2018). Second, previously reported associations between CFC scores and particular behaviors have not been consistent. For example, some studies have found significant associations between CFC and health behaviors such as smoking and physical activity (e.g., Adams & Nettle, 2009; Wininger & DeSena, 2012), whereas others fail to detect these relationships (e.g., Adams & White, 2009; Daugherty & Brase, 2010). Small and inconsistent effects may in part be linked to the history of CFC conceptualization and measurement. Prior to the year 2012, few researchers distinguished between the CFC-F and CFC-I subscales. Instead, the immediate and future scale items of the CFC-12 were averaged into a single CFC score, a practice which may attenuate observed effect sizes or hinder the interpretation of the relationship between CFC and a given behavior (Joireman et al., 2012). Another explanation for inconsistent reports and small effect sizes concerns the general (or global) nature of the CFC construct.
CFC Domain Specificity
In CFC literature, CFC scores are assumed to represent a stable, domain-free present- or future-oriented mind-set (McKay et al., 2017; Strathman et al., 1994). However, it is possible that an individual can consider future behavioral outcomes in one domain (e.g., work) and relatively immediate outcomes in another (e.g., health). Failure to conceptualize and measure the CFC construct at the domain level may contribute to the weak effect sizes observed between CFC scores and behaviors within particular domains. For example, a participant may interpret and respond to one scale item in relation to health outcomes, but another item in relation to academic outcomes. Similarly, the same general scale item may elicit considerations of different life domains for different participants, such that two participants may interpret the same scale items differentially within or across studies. Nevertheless, short of asking every participant to describe their interpretation of each scale item, it is not possible to know the extent to which general CFC scale items elicit domain-specific responses. Furthermore, as studies of CFC typically focus on a single life domain, it has not yet been possible to make cross-domain comparisons of CFC scores (McKay et al., 2017).
The proposal that the CFC construct is domain-specific aligns with previous reports of domain specificity in related temporal constructs, such as future discounting (i.e., the tendency for individuals to devalue an outcome as a function of time; Acuff et al., 2017), and the mental construction of possible selves (i.e., future-oriented self-conceptions that guide decision-making, motivation and behavior; Markus & Nurius, 1986). For example, Chapman and Elstein (1995) described “domain independence” after observing that an individual’s level of future discounting for different reward types (namely, monetary and health-related rewards) was not highly correlated. Similarly, Hoppmann, Gerstorf, Smith, and Klumb (2007) found that participants who imagined hoped for possible selves in the domains of health and social relations performed significantly more daily activities within each domain (i.e., more health-related and social daily activities, respectively). To date, a handful of studies have examined the extent to which temporal considerations are domain-specific, although these studies adopted distinct conceptual and methodological perspectives. Van Beek, Antonides, and Handgraaf (2013) measured CFC at a behavioral level, creating two tailored CFC scales to measure consideration of immediate and future consequences specifically in relation to eating and exercise behavior (the CFC-food and CFC-exercise scales). Results showed that scores on the CFC-food scale were related to eating but not exercise behavior. Conversely, scores on the CFC-exercise scale were associated with both eating and exercise behavior. In a subsequent study, Dassen, Houben, and Jansen (2015) reported that only the CFC-food, and not the CFC-general, subscales were significantly associated with healthy eating behavior. Although food and exercise behaviors are subsumed under the same domain of health, these studies were the first to suggest that tailoring CFC scale items to the relevant domain may improve their predictive utility.
More recently, McKay et al. (2017) developed a new 18-item measure to examine the extent to which adolescents consider the future across different life domains. The measure was developed using items from the CFC scale as well as related measures of individual differences in future thinking (e.g., the future time perspective scale; Husman & Shell, 2008). Exploratory structural equation modeling and confirmatory factor analysis indicated the presence of four factors with small-to-moderate intercorrelations: (a) health and well-being, (b) global warming, (c) finances, and (d) school. McKay, Perry, and Cole (2018) subsequently tested the measure in a sample of University students and found that domain-specific subscales significantly distinguished between groups in the appropriate domain (e.g., between sports players and nonsports players, and recyclers and nonrecyclers). Most recently, (Murphy & Murphy, 2018) adapted the CFC-14 items to measure consideration of future and immediate behavioral outcomes in the driving domain. Results showed that associations with driving behaviors (e.g., phone use when driving, driving violations and tire checking) were stronger for the CFC-driving subscales than for the CFC-general subscales. Collectively, these recent reports form an evidence base to conceptualize and further investigate domain specificity in the CFC construct.
The Current Research: Aims and Hypotheses
To examine domain specificity in CFC, we created five domain-specific adaptations of the general CFC-14 scale: CFC-college (for college students), CFC-work (for working nonstudents), CFC-health, CFC-money, and CFC-environment. Although domain-specific in nature, McKay et al.’s (2017) 18-item measure was developed using items from several existing temporal measures which are known to assess temporal constructs that are conceptually distinct from CFC (Cole, Andretta, & McKay, 2017; Percy, McKay, Perry, & Cole, 2018; Shipp, Edwards, & Schurer Lambert, 2009). To date, no study has examined the convergent validity of this new 18-item measure using the CFC-14 (general or tailored to a specific domain). As such, the scale cannot yet be considered a domain-specific measure of the CFC construct. Furthermore, McKay and colleagues’ measure assesses domain specificity in future-oriented concerns only. Despite considerable debate, many in the field have reported evidence to substantiate the presence of two conceptually related, but distinct, temporal factors within the CFC-14 (e.g., Joireman et al., 2012; McKay et al., 2016; Percy et al., 2018). As such, it stands to reason that individuals may not only differ in the consideration of future consequences across domains, but also in the consideration of immediate consequences.
We first examined the factor structure of five domain-specific CFC-14 scales. We hypothesized that, similar to the general scale, domain-specific scales would each consist of two related, but distinct, subscales (Hypothesis 1). We then analyzed the pattern and strength of associations between all CFC subscales (domain-specific and global). We anticipated that, similar to the general scale, correlations between domain-specific CFC-F and CFC-I would be negative and moderate in size (Hypothesis 2a), that domain-specific CFC-F (CFC-I) subscales would correlate positively and moderately with the general CFC-F (CFC-I) subscales (Hypothesis 2b), and that intercorrelations between domain-specific CFC subscales would be small to moderate in size (Hypothesis 2c). Finally, to speak to the potential improved predictive utility of domain-specific CFC-14 scales, we compared associations between CFC scales (general vs. domain-specific) and self-reported behavior in each domain. We hypothesized that, relative to the general subscales, domain-specific CFC subscales would be more strongly associated with behavior within the relevant domain (Hypothesis 3).
Method
Participants completed three online surveys approximately 1 week apart. In Survey 1, participants provided basic demographic information and completed the general CFC-14 scale. In Surveys 2 and 3, participants self-reported behavior in two life domains. Following self-report measures of behavior in one domain, participants completed the relevant domain-specific CFC-14 scale. Survey 2 focused on the domains of health and work for nonstudent participants, and the domains of health and college for student participants. Survey 3 focused on the domains of money and the environment for all participants. In Surveys 2 and 3, domains were counterbalanced to control for order effects.
Scale adaptation required tailoring the 14 general CFC scale items to each domain while adhering as closely as possible to the intent and form of the original items. This was an iterative process; following initial adaptation of scale items by the authors, domain-specific CFC items were revised following extensive qualitative feedback from a convenience sample of University students (n = 10). Participants were provided with a copy of each domain-specific scale and asked to evaluate the items of each measure for face validity and item readability. Lay descriptions of the concepts were provided, and checks of the participant’s accuracy of understanding were completed. Participants then met with one of the two researchers individually to provide verbal and written feedback, and the items of each measure were subsequently revised. This process was repeated with the same participant group to finalize the items. Domain-specific CFC-14 scales are available in Supplementary Materials.
Participants
Participants were required to be English-speaking adults above the age of 18 years. Recruitment efforts were initially directed at convenience samples of social media users as well as the student population at the local University, and then on Prolific, an online crowdsourcing platform. 1 Participants recruited on Prolific were paid a total of £2.32 for their participation. A total of 817 individuals initiated participation. Forty-five individuals failed an instructional manipulation check (IMC) that told participants to click one particular response option among a range of options (Oppenheimer, Meyvis, & Davidenko, 2009). These participants were, therefore, excluded from all analyses. Nine participants were excluded for selecting the same response option for all items in one or more CFC-14 scales (e.g., choosing the midpoint option for all scale items). Finally, a total of 265 participants failed to complete either the second or third survey. As a primary aim of the research was to examine CFC-14 scores across all domains, these participants were, therefore, excluded from all analyses.
In total, 498 participants completed all three surveys (response rate = 64%; 333 females; 300 from Prolific). The CFC-college scale and measures of academic behavior were completed by college students only (n = 205). Of the 293 nonstudent participants, 16 were not currently in employment. These participants did not complete the CFC-work scale or measures of occupational behavior and, as such, analyses in the work domain were conducted using data from the remaining 277 nonstudent participants. For CFC scales and measures of self-reported behavior in the domains of health, money, and the environment, data from all 498 participants were analyzed. The mean age of the entire sample was 32.12 (SD = 12.86; range = 18-85 years). The mean age of the college student sample was 22.41 (SD = 5.02; n = 205), and the mean age of the nonstudent sample was 37.90 (SD = 11.00; n = 277). The sample was predominantly Irish (35.9%), British (31.7%), and American (16.1%). The remaining 16.3% represented 25 different nationalities (e.g., 1.4% Australian, 1.2% Portuguese, 0.6% Dutch, and 0.2% Hungarian).
Measures
Survey 1
Participants reported their age, sex, nationality, and student/work status before completing the general CFC-14 scale (Joireman et al., 2012). Joireman and colleagues previously reported good internal consistency for the CFC-14 subscales (α = .82 and .84 for CFC-F and CFC-I, respectively). A 7-point scale ranging from 1 (very unlike me) to 7 (very like me) was used for all CFC scales (general and domain-specific). We calculated total and subscale scores for all CFC scales.
Survey 2
Smoking status
Smoking status was measured based on the Centers for Disease Control and Prevention (2011) smoking classifications. Respondents were asked to identify as one of the following: an everyday smoker, an occasional smoker, an ex-smoker for less than 12 months, an ex-smoker for more than 12 months, and a nonsmoker/never smoker.
Eating behavior
Fruit and vegetable consumption was measured using two 8-point scales ranging from 1 (never or hardly ever) to 8 (5 or more times a day). Fast food consumption was measured using an 8-point scale ranging from 1 (never or hardly ever) to 8 (everyday). Following reverse-scoring of the fast food item, participant responses to these three items were summed so that higher scores indicate healthier eating behavior.
Exercise behavior
Participants were asked to report how often they participated in each the following activities: stretching or strengthening exercises, walk for exercise, jog or run, swim or do aquatic exercise, cycle (including on stationary exercise bikes), and use aerobic exercise equipment. Responses were provided on a 5-point scale ranging from 1 (never) to 5 (more than 3 hr/week). Items were summed so that higher scores indicate greater exercise participation.
Health monitoring behavior
Participants were asked to indicate how like/unlike them it was to do each of the following: (a) get general doctors check-ups (visits that are not for specific ailment or injury), (b) perform regular self-examinations for signs of cancer or other illnesses, (c) attend appropriate cancer screening services for their age/sex, (d) wash hands or apply hand rubs to avoid contracting or spreading infection, and (e) make a doctor’s appointment if feeling unwell or are suspicious that they may be unwell. Responses were provided on a 7-point scale ranging from 1 (very unlike me) to 7 (very like me). Items were summed so that higher scores indicate greater health monitoring behavior.
Work proactivity
Work proactivity (i.e., the extent to which individual’s take action to improve their work environment; Bateman & Crant, 1993) was measured using four items adapted from Bateman and Crant’s (1993) proactivity personality scale. Items were adapted to represent proactivity specifically in the workplace. For example, “I am constantly on the lookout for new ways to improve at my job” and “I am great at turning problems into opportunities at work.” Response options were provided on a 7-point scale ranging from 1 (very unlike me) to 7 (very like me). Items were averaged so that higher scores indicate greater work proactivity (α = .82).
Organizational citizenship
Organizational citizenship (i.e., discretionary behavior that promotes the effective functioning of an organization; Podsakoff, MacKenzie, Paine, & Bachrach, 2000) was measured using four items from Podsakoff, MacKenzie, Moorman, and Fetter’s (1990) organizational citizenship scale. Example items include the following: “My attendance at work is above the norm” and “I don’t take extra breaks at work.” Response options were provided on a 7-point scale ranging from 1 (very unlike me) to 5 (very like me). Items were averaged so that higher scores indicate greater organization citizenship (α = .66).
Academic commitment
Academic commitment (i.e., long-term persistence with one’s studies; Human-Vogel & Rabe, 2015) was measured using the five-item level of commitment subscale from Human-Vogel and Rabe’s (2015) academic commitment scale. Example items include “I want to continue with my studies” and “I am determined to complete my studies successfully.” Response options were provided on a 5-point scale ranging from 1 (strongly disagree) to 5 (strongly agree). Items were averaged so that higher scores indicate greater academic commitment (α = .78).
Academic investment
Academic investment (i.e., investment in one’s studies to date; Human-Vogel & Rabe, 2015) was measured using the five-item academic investment subscale from the same academic commitment scale. Example items include the following: “I feel very involved in my studies—like I have put a great deal into them” and “Compared to others I know, I have invested a great deal of time and effort in my studies.” Response options were provided on a 5-point scale ranging from 1 (strongly disagree) to 5 (strongly agree). Items were averaged so that higher scores higher scores indicate greater academic investment (α = .92).
Academic engagement
Academic engagement (i.e., the extent to which students engage in academic activities that are associated with high-quality learning outcomes; Krause & Coates, 2008) was measured using five items adapted from Skinner, Kindermann, and Furrer’s (2009) behavioral engagement and emotional engagement scales from their Engagement Versus Disaffection with Learning measure. This measure was initially developed for use in primary and secondary school students. For the purposes of the current research, however, items were adapted to suit a college student sample. Example items include “I listen carefully in lectures,” and “I try very hard in college.” Noting the limited scope of academic engagement behaviors in the original measure, an additional eight items were generated. For example, “I usually put a lot of effort into essays and other coursework,” and “I usually complete essays and other coursework on time.” The 13 items were combined and the average was used as a measure of academic engagement. Response options were provided on a 5-point scale ranging from 1 (very unlike me) to 5 (very like me). Items were averaged so that higher scores indicate greater academic engagement (α = .84).
Survey 3
Proenvironmental behavior
Proenvironmental behavior was measured using 10 items from Yavetz, Goldman, and Pe’er’s (2009) environmental behavior scale. Participants were asked to indicate how often they engaged in each behavior on a 5-point scale ranging from 1 (never) to 5 (very often). The measure includes environmental behaviors such as reusing plastic bags, purchasing environmentally friendly products, and conserving energy at home by twitching off electrical appliances. For the purposes of the current study, four items were generated to measure four additional environmental behaviors that are not represented in Yavetz and colleagues’ scale (e.g., using public transport instead of traveling by car, and leaving the TV/computer on standby overnight). Items were averaged so that higher scores indicate more engagement in proenvironmental behavior (α = .74).
Financial planning
A single question on time period for financial planning was used. Participants were asked to indicate which of the six time periods was the most important to them for planning their own (and/or their family’s) saving and spending. Response options provided were as follows: “the next few weeks,” “the next few months,” “the next year,” “the next few years,” “the next 5 to 10 years,” or “longer than 10 years.” This item has been previously used in research on the role of CFC in socioeconomic inequalities in health behavior (e.g., Adams, 2009).
Saving behavior
Participants were asked to indicate whether they saved regularly (yes/no response format). Those who answered yes were asked to indicate the typical amount of money they save per paycheck. Response options were as follows: “practically none,” “10%,” “25%,” 50%,” “75%,” and “almost all of what I receive or earn.”
Compulsive spending
Compulsive spending was measured using the seven-item diagnostic screener for compulsive buying tendencies (DSCB; Faber & O’Guinn, 1992). Example items include “If I have any money left at the end of a pay period, I just have to spend it,” and “Bought things even though I couldn’t afford them.” Response options were provided on a 5-point scale ranging from 1 (never) to 5 (very often). Items were averaged so that higher scores indicate lower compulsive buying tendencies (α = .84). Due to researcher error, scores on this measure were only available for the Prolific Academic participant sample (n = 300).
Data Analysis
Confirmatory factor analysis was conducted using RStudio Version 1.1.463 (RStudio Team, 2015). Multivariate normality was assessed using Mardia’s (1970) multivariate skew and kurtosis coefficients. Statistically significant values indicate multivariate nonnormality (Cain, Zhang, & Yuan, 2017). Model fit was evaluated using the nonnormed fit index (NNFI), comparative fit index (CFI), the standardized root mean square residual (SRMR), and the root mean square error of approximation (RMSEA). NNFI and CFI values of .95 or higher indicate good model fit. SRMR values below .08 and RMSEA values below .07 indicate good fit (Hu & Bentler, 1999). To more formally compare one- and two-factor models of the CFC-14, we conducted a series of chi-square difference tests (Hypothesis 1).
Pearson’s product moment correlations were calculated to examine the direction and strength of associations between CFC-14 subscales (Hypotheses 2a, 2b, and 2c). Finally, general and domain-specific subscales were entered into a series of hierarchical regression models with Bonferroni corrections to compare their associations with each behavior (Hypothesis 3).
Results
Attrition Analysis and Descriptive Statistics
Participants who completed all three surveys (n = 498) were significantly older (M = 32.12 years, SD = 12.86) than those who did not complete the full study (n = 265; M = 27.49 years, SD = 9.81), t(670.248)= −5.124, p < .001. Levene’s test indicated unequal variances (F = 28.70, p < .001), so degrees of freedom were adjusted accordingly. There was a significant difference between completers and noncompleters by sex, χ2(2, N = 763) = 0.09, p = .13; females were more likely than males to complete the full study. There were no significant differences between completers and noncompleters in CFC-F, t(761)= −0.350, p = .726; CFC-I, t(761) = 1.442, p = .150; or total, t(761)= −1.092, p = .275, general CFC-14 scores. Table 1 provides descriptive statistics. All CFC-14 scales and subscales exhibited good internal consistency.
Descriptive Statistics for CFC Scales.
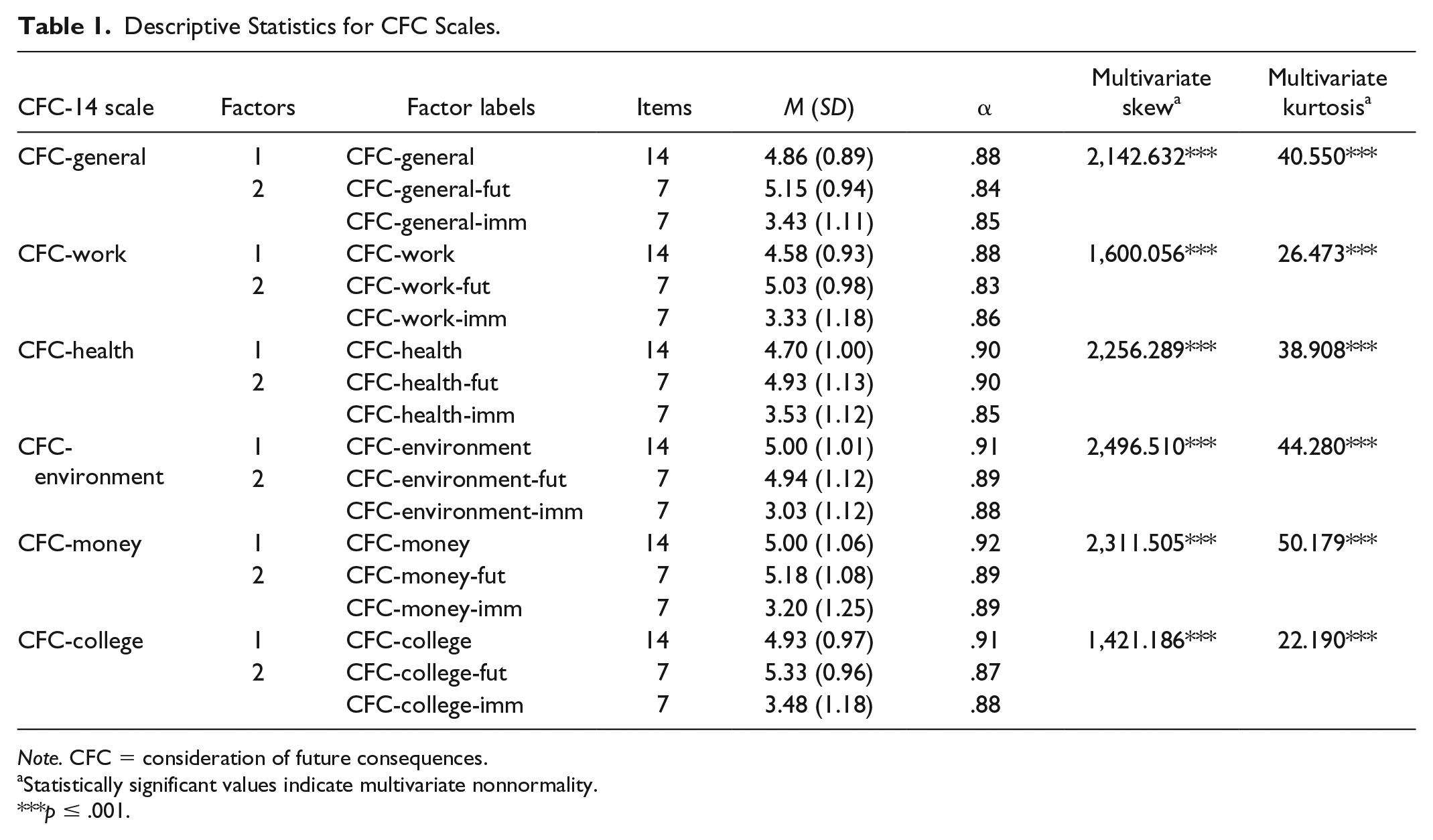
Note. CFC = consideration of future consequences.
Statistically significant values indicate multivariate nonnormality.
p ≤ .001.
Confirmatory Factor Analyses (Hypothesis 1)
To account for multivariate nonnormality (Table 1), we used robust maximum likelihood estimation with robust standard errors and a Satorra–Bentler-scaled test statistic (MLM). To test the validity of the two-factor model in the general and domain-specific CFC-14 scales, we compared the fit of the two-factor solution with the one-factor solution in all six scales. As presented in Table 2, the original one-factor models (“a” models) fit the data poorly. Alternatively, the two-factor models (“b” models) all showed a reasonable fit to the data. Paralleling previous studies (e.g., Joireman et al., 2008; Joireman et al., 2012; Vásquez-Echeverría, Antino, Alvarez-Nuñez, & Rodríguez-Muñoz, 2018), we estimated six theoretically appropriate correlated error terms (between the error terms of Items 1 and 2, 2 and 13, 3 and 4, 7 and 8, 9 and 10, and 13 and 14) to achieve acceptable fit (i.e., RMSEA below .07, SRMR below .08, and NNFI and CFI near .95; Hu & Bentler, 1999; Steiger, 2007) for all two-factor models. As shown, these two-factor models (“c” models) all provided a good fit for the data. Finally, to ensure fair model comparisons between one- and two-factor models, we estimated a one-factor model incorporating the same six correlated error terms in all CFC scales. As illustrated in Table 2, one-factor models with the same estimated error terms (“d” models) all provided reasonable fit for the data. Results of chi-square difference tests indicate that, for all CFC-14 scales, the two-factor solution with six incorporated correlated error terms was the most robust model overall (Table 3).
Goodness-of-Fit Indices for All CFC Models.
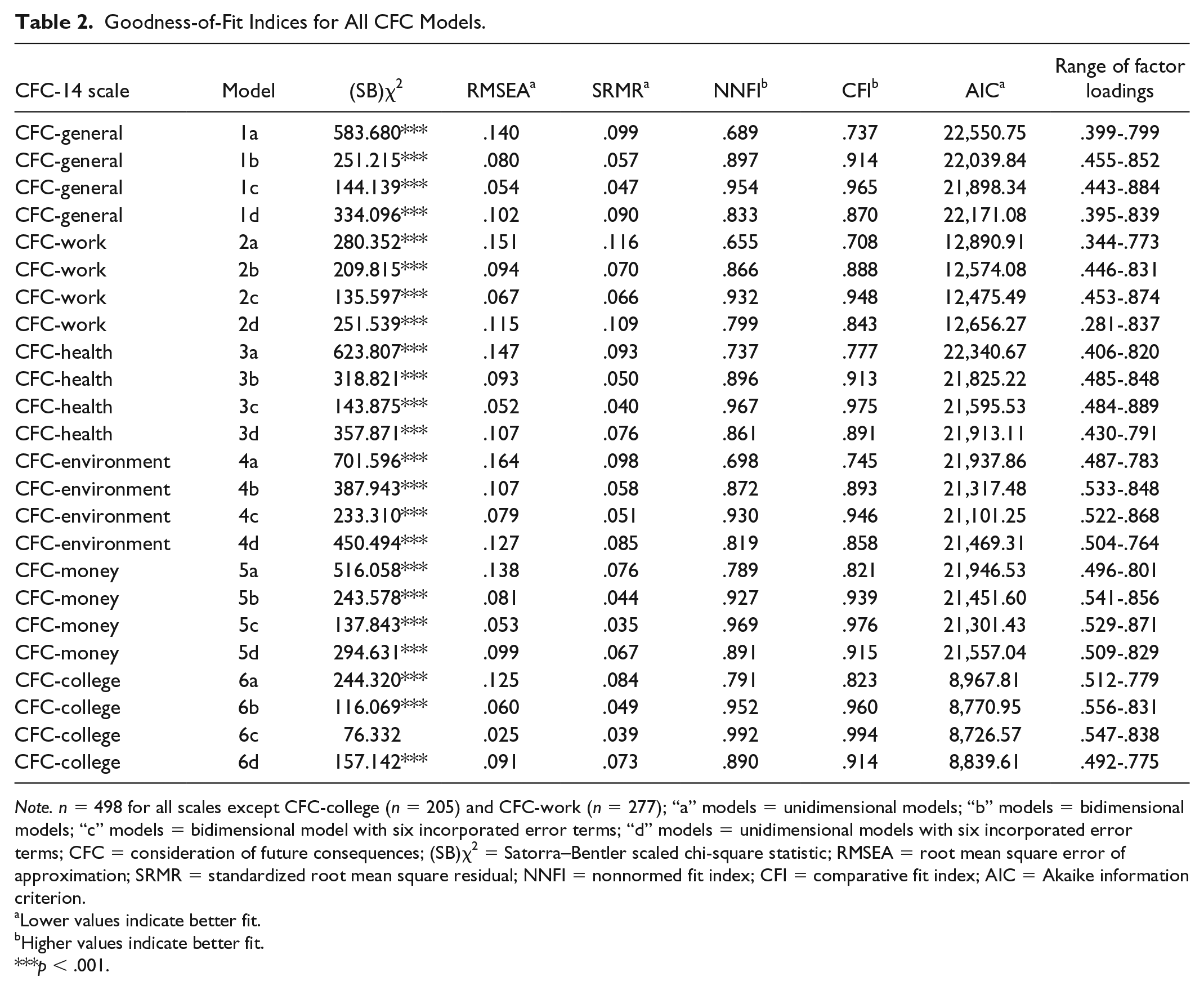
Note. n = 498 for all scales except CFC-college (n = 205) and CFC-work (n = 277); “a” models = unidimensional models; “b” models = bidimensional models; “c” models = bidimensional model with six incorporated error terms; “d” models = unidimensional models with six incorporated error terms; CFC = consideration of future consequences; (SB)χ2 = Satorra–Bentler scaled chi-square statistic; RMSEA = root mean square error of approximation; SRMR = standardized root mean square residual; NNFI = nonnormed fit index; CFI = comparative fit index; AIC = Akaike information criterion.
Lower values indicate better fit.
Higher values indicate better fit.
p < .001.
Results of Model Comparisons.
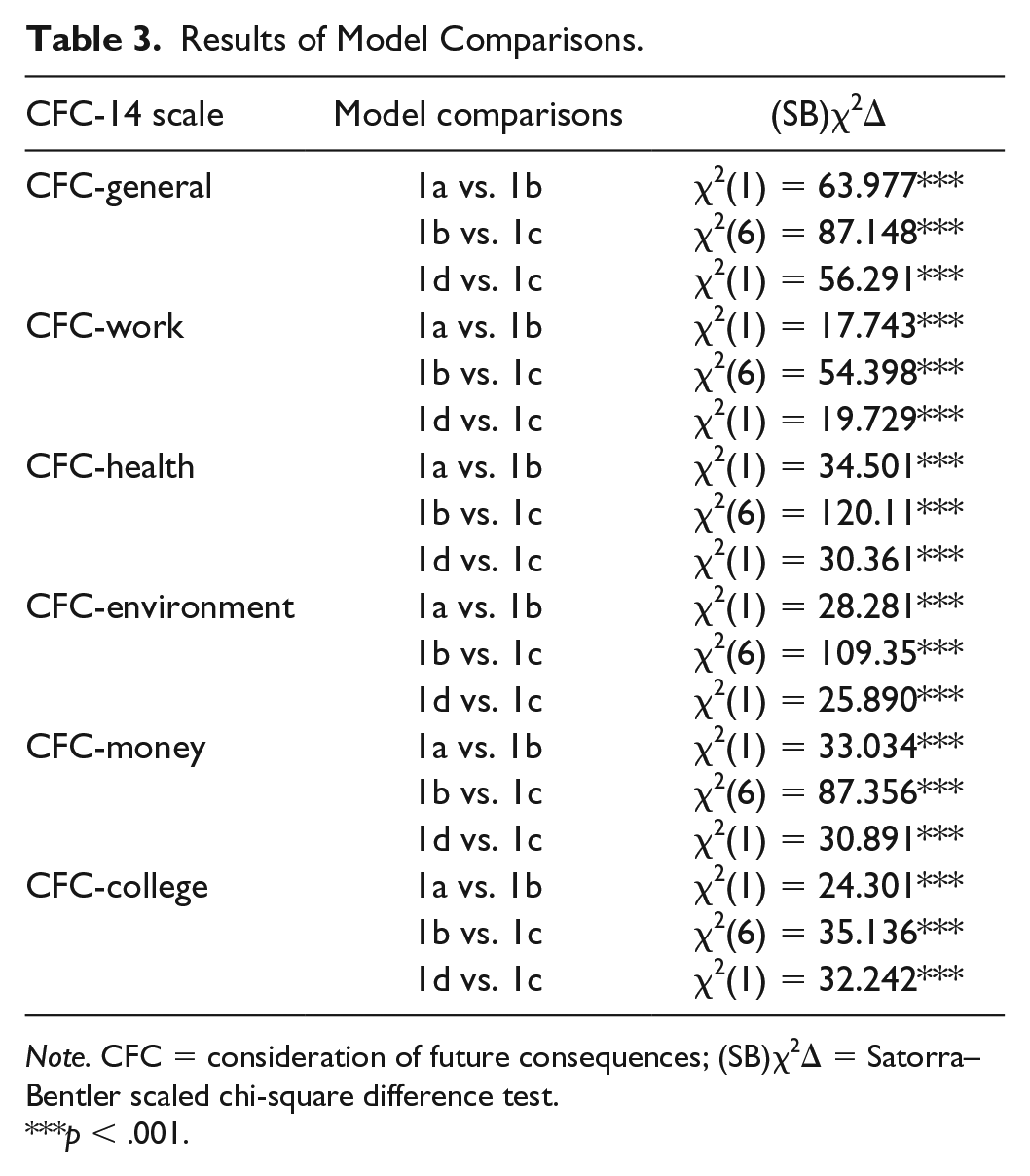
Note. CFC = consideration of future consequences; (SB)χ2Δ = Satorra–Bentler scaled chi-square difference test.
p < .001.
Bivariate Correlations (Hypotheses 2a, 2b, and 2c)
Correlation coefficients are presented in Table 4. As expected, correlations between all CFC-14 future and immediate subscales were negative (Hypothesis 2a). Furthermore, all domain-specific future subscales correlated positively with general CFC-F, and all domain-specific immediate subscales correlated positively with general CFC-I (Hypothesis 2b). Finally, intercorrelations between domain-specific CFC subscales were all small to moderate in size (Hypothesis 2c). Correlations between domain-specific and general CFC subscales were predominately moderate, albeit some large, with some domain-specific subscales correlating more strongly with general subscales than others (e.g., r = .59 between the CFC-general and the CFC-college future subscales, whereas r = .34 between the CFC-general and CFC-environment future subscales).
Zero-Order Correlations Between General and Domain-Specific CFC-14 Subscales.
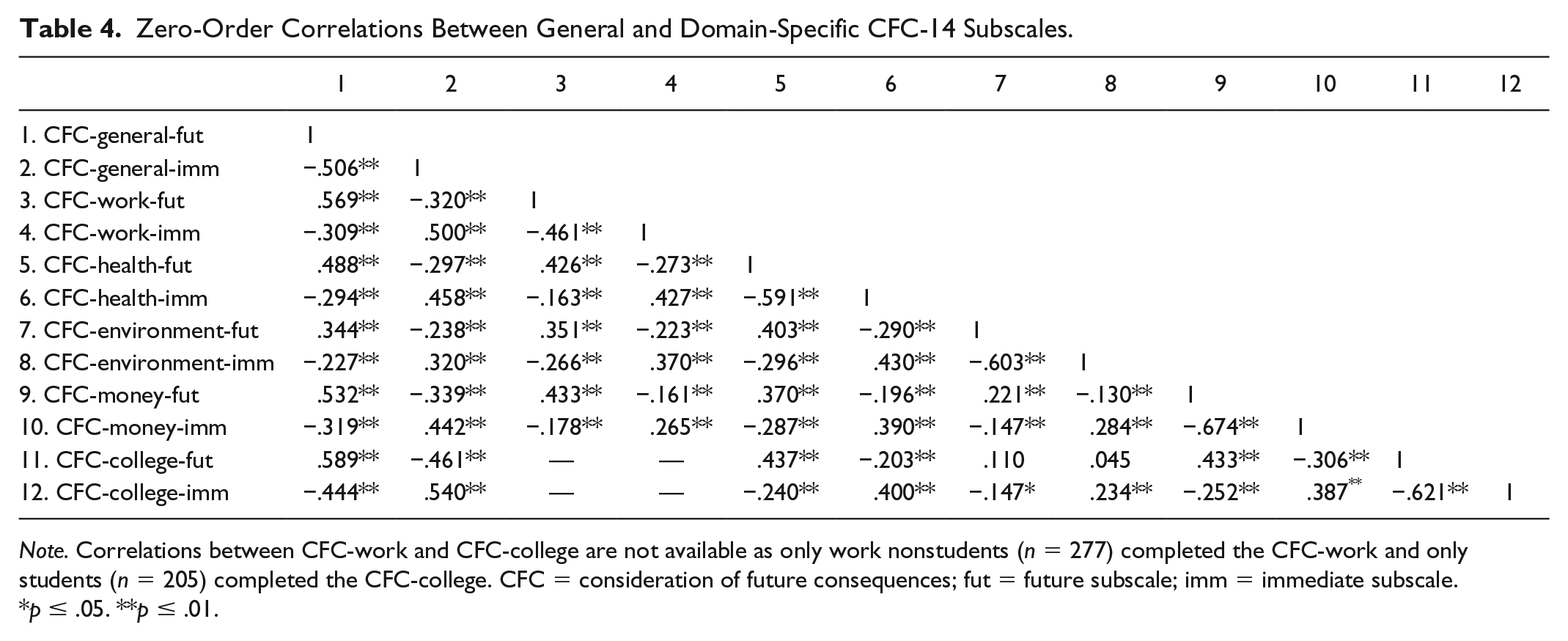
Note. Correlations between CFC-work and CFC-college are not available as only work nonstudents (n = 277) completed the CFC-work and only students (n = 205) completed the CFC-college. CFC = consideration of future consequences; fut = future subscale; imm = immediate subscale.
p ≤ .05. **p ≤ .01.
Hierarchical Regression Analyses (Hypothesis 3)
A series of hierarchical regression analyses with Bonferroni corrections were conducted to examine the unique contributions of general and domain-specific CFC-14 subscales in self-reported behavior. We first conducted independent samples t tests to test for sex differences in CFC subscale scores. There were no significant differences between males and females in any of the CFC subscales (general or domain-specific). We then calculated correlation coefficients to examine associations between age and CFC subscales. Age correlated significantly with six out of 12 CFC subscales. Although all correlation coefficients were small in magnitude (r ranged from .09 to .19), we completed all regression analyses adjusting for age. A regression analysis was performed for each behavior in each domain, and general and domain-specific subscales were entered simultaneously at Step 2. Results are provided in Tables 5-9.
Regression Analyses of the Future and Immediate Subscales of the CFC-General and CFC-Work in Self-Reported Work Behaviors.
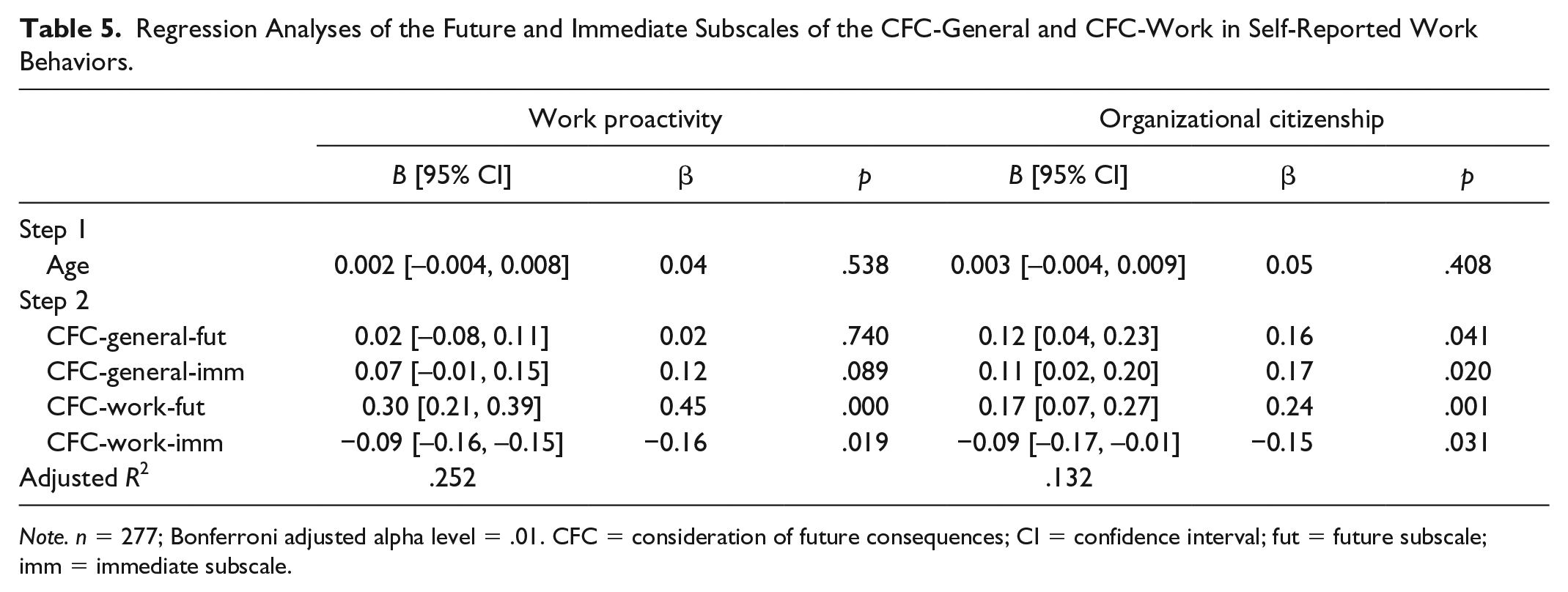
Note. n = 277; Bonferroni adjusted alpha level = .01. CFC = consideration of future consequences; CI = confidence interval; fut = future subscale; imm = immediate subscale.
Regression Analyses of the Future and Immediate Subscales of the CFC-General and CFC-Health in Self-Reported Health Behaviors.
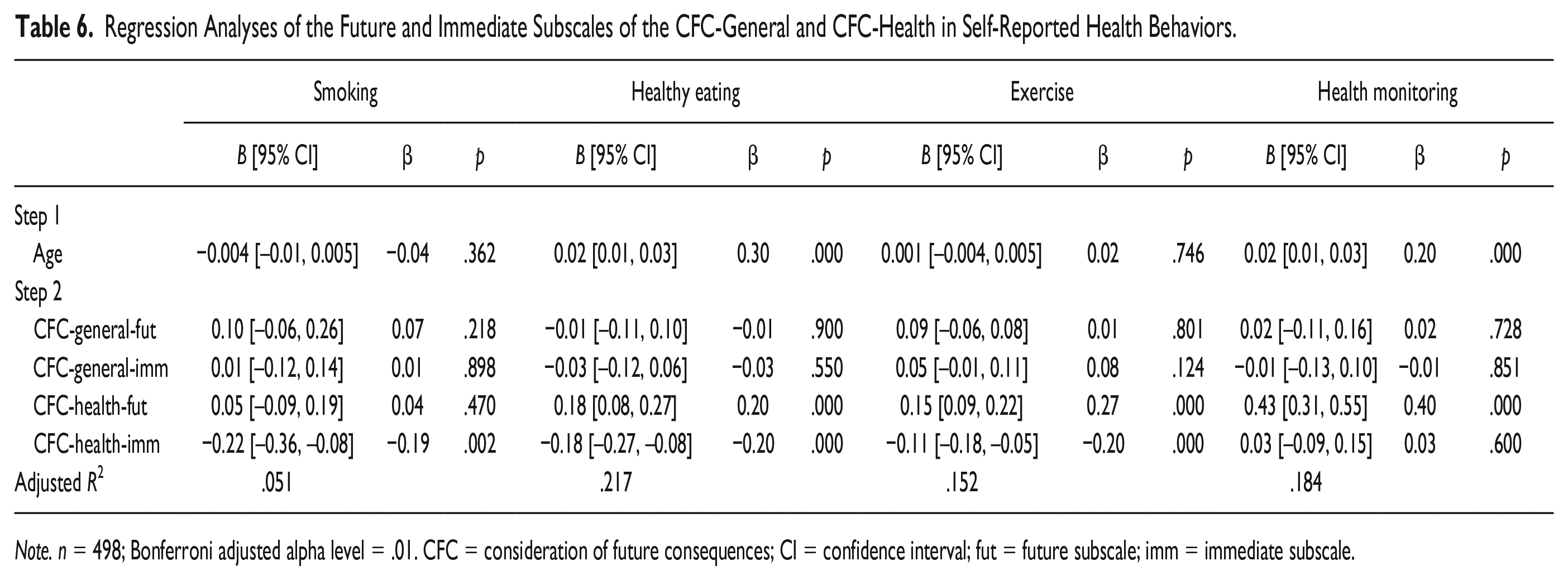
Note. n = 498; Bonferroni adjusted alpha level = .01. CFC = consideration of future consequences; CI = confidence interval; fut = future subscale; imm = immediate subscale.
Regression Analyses of the Future and Immediate Subscales of the CFC-General and CFC-Environment in Self-Reported Pro-Environmental Behaviors.
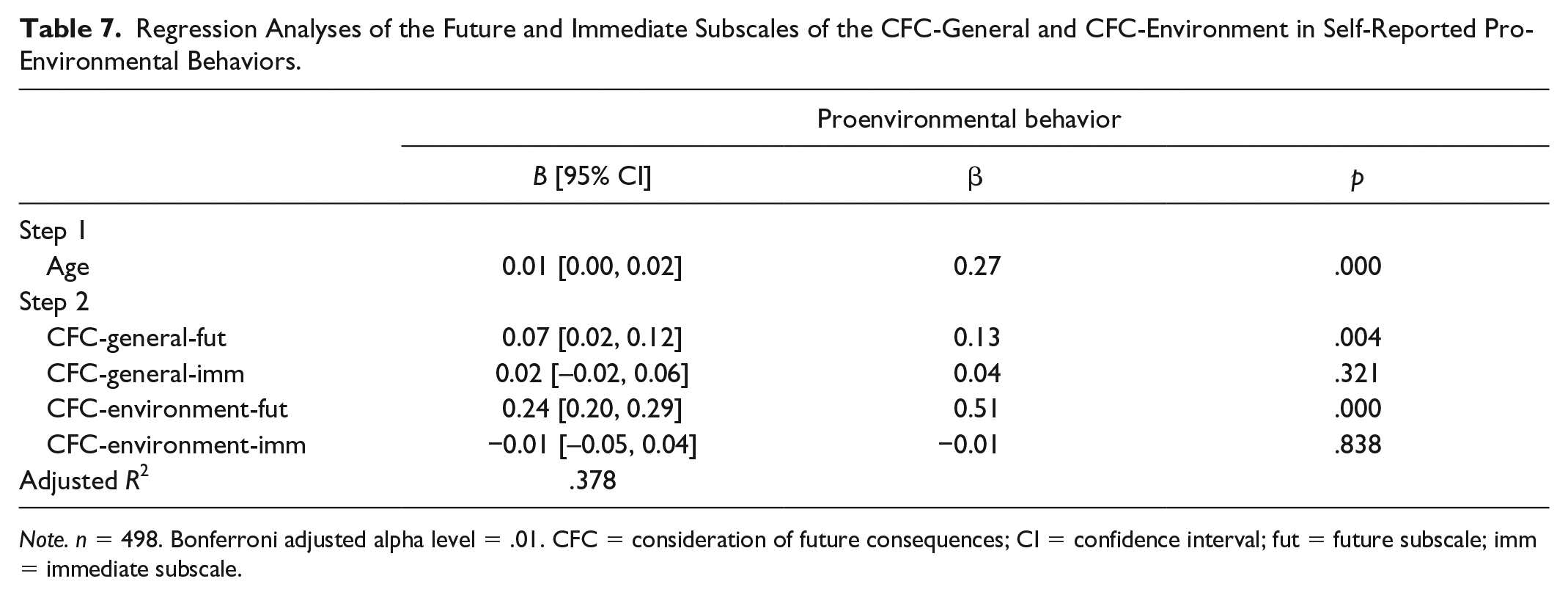
Note. n = 498. Bonferroni adjusted alpha level = .01. CFC = consideration of future consequences; CI = confidence interval; fut = future subscale; imm = immediate subscale.
Regression Analyses of the Future and Immediate Subscales of the CFC-General and CFC-Money in Self-Reported Financial Behaviors.
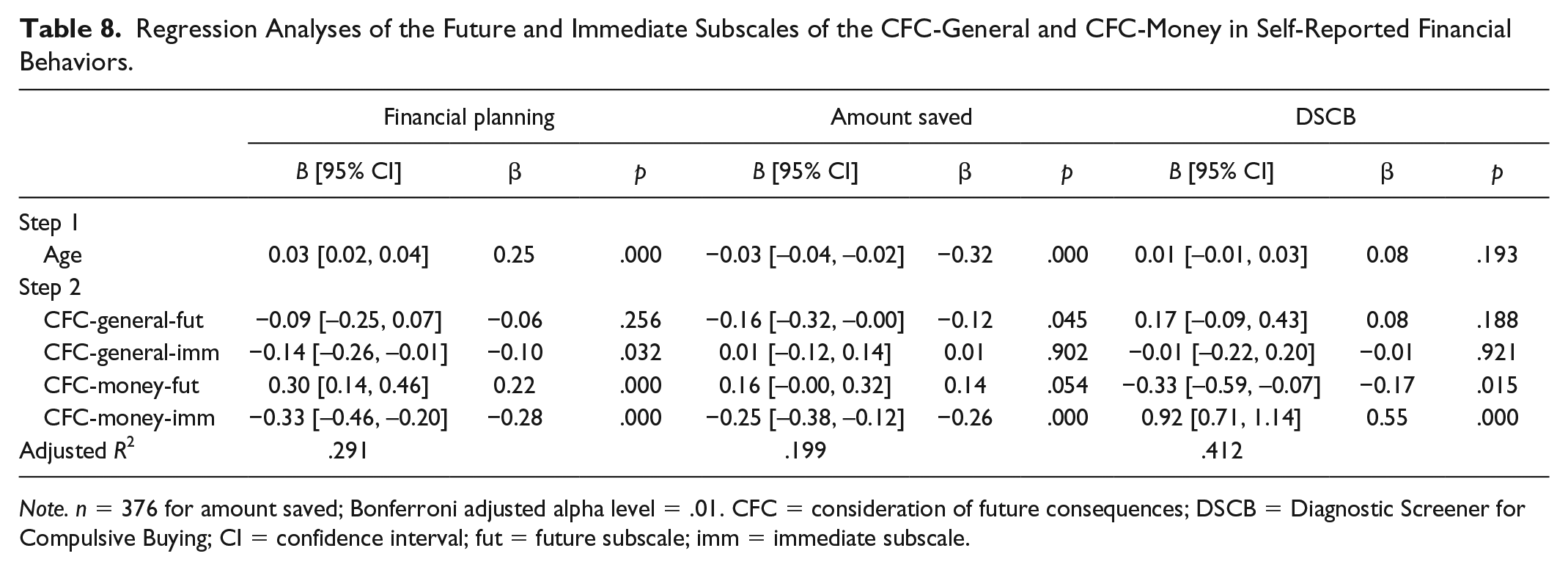
Note. n = 376 for amount saved; Bonferroni adjusted alpha level = .01. CFC = consideration of future consequences; DSCB = Diagnostic Screener for Compulsive Buying; CI = confidence interval; fut = future subscale; imm = immediate subscale.
Regression Analyses of the Future and Immediate Subscales of the CFC-General and CFC-College in Self-Reported Academic Behaviors.
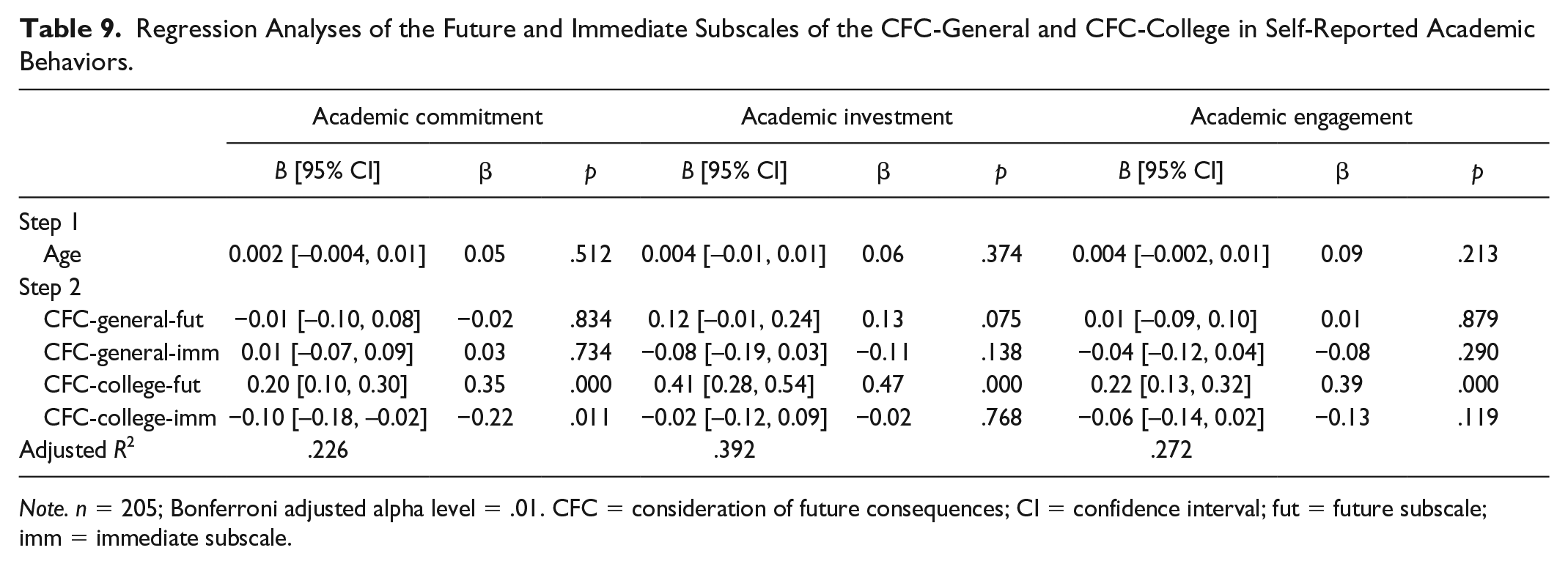
Note. n = 205; Bonferroni adjusted alpha level = .01. CFC = consideration of future consequences; CI = confidence interval; fut = future subscale; imm = immediate subscale.
With the exception of proenvironmental behavior, the results indicated that only domain-specific, and not the general, CFC-14 subscales were significantly associated with behaviors in each domain. The CFC-general and CFC-environment future subscales were both significantly related to self-reported engagement in proenvironmental behavior. However, the CFC-environment future subscale was most strongly associated with proenvironmental behavior overall (β = 0.13 and β = 0.51, for CFC-general and CFC-environment future subscales, respectively).
All associations between domain-specific subscales and self-reported behavior meet or exceed Ferguson’s (2009) minimum recommended effect size representing practical significance (β ≥ 0.2), the only exception being the relationship between the CFC-health immediate subscale and smoking status (β= −0.19). Associations were strongest between CFC-work future and work proactivity (β = 0.45), CFC-health future and health monitoring (β = 0.40), CFC-environment future and pro-environmental behavior (β = 0.51), CFC-money immediate and compulsive spending behavior (β = 0.55), and CFC-college future and academic investment (β = 0.47).
In many instances, only one CFC subscale was significantly related with self-reported behavior. In the work domain, work proactivity and organizational citizenship were significantly related to scores on the CFC-work future subscale, but not the immediate subscale, and in the health domain, smoking status was significantly associated with scores on the CFC-health immediate subscale, but not the future subscale, whereas the opposite pattern was true for self-reported engagement in health monitoring behavior. Engagement in proenvironmental behavior was significantly related to scores on the CFC-environment future subscale, but not the immediate subscale. Conversely, amount of money saved and compulsive spending were only significantly related to the CFC-money immediate subscales, but not the future subscale. In the academic domain, academic commitment, engagement, and investment were only significantly related to scores on the CFC-college future subscale, but not the immediate subscale. Finally, there were some behaviors, which were significantly related to both future and immediate domain specific subscales, namely, healthy eating, exercise and financial planning.
Discussion
The overall aim of the current study was to examine domain specificity in the CFC construct. Specifically, we examined the psychometric validity of the two-factor model of CFC in five domain-specific CFC-14 scales. We analyzed the pattern and strength of associations between domain-specific and general CFC-14 subscales, and compared associations between these subscales (general vs. domain-specific) and self-reported behavior in five substantive domains.
Consistent with previous reports of domain specificity in related temporal constructs, such as future discounting (e.g., Chapman, 1996) and the mental construction of possible selves (e.g., Hoppmann et al., 2007), the results of the current study provide evidence for domain specificity in CFC. First, by replicating the two-factor structure in five domain-specific CFC-14 scales, the findings provide further evidence for the distinction between the consideration of future and immediate behavioral outcomes in five distinct life domains. As in previous studies (e.g., Joireman et al., 2008; Joireman et al., 2012; Vásquez-Echeverría et al., 2018), incorporating pathways between a small number of error terms improved model fit for all CFC-14 scales, general and domain-specific. Although the addition of two future scale items by Joireman et al. (2012) is said to have stabilized the two-factor solution within the CFC-14 (McKay et al., 2016), similarity of item wording or intent, particularly on the future subscale, likely introduces a method effect (Vásquez-Echeverría et al., 2018). Incorporating correlated error terms on these items, therefore, adjusts for this effect. However, the use of correlated error terms to facilitate satisfactory fit has been criticized, as the technique may yield findings that are sample-specific (McKay et al., 2015). This being said, the added pathways between items in the current study were theoretically appropriate, given their conceptual, as well as semantic, overlap. For example, Items 1 and 2 describe a focus on how current behaviors influence the future (e.g., “Often I engage in a particular behavior to achieve outcomes that may not result for many years”; Item 2), Items 9 and 10 capture the belief that negative outcomes can be dealt with at some point in the future rather than now (e.g., “I think that sacrificing now is usually unnecessary as future outcomes can be dealt with at a later time”; Item 10), and Items 13 and 14 both capture cognitive based considerations of the future (e.g., “when I make a decision, I think about how it might affect me in the future”; Item 13).
Second, correlation coefficients between domain-specific CFC subscales were of the expected direction and magnitude (i.e., small to moderate), indicating that the subscales represent constructs that are related, but not uniform, across domains. Finally, with the exception of pro-environmental behavior, only domain-specific CFC subscales were significantly associated with self-reported behavior within each domain. For all behaviors, one or both of the domain-specific subscales of the CFC-14 met or exceeded Ferguson’s (2009) minimum recommended effect size magnitude for practical significance (with the exception of the association between the CFC-health immediate subscale and smoking status which fell just short of Ferguson’s recommendation of .2; β= −0.19). In addition, while only two effect sizes met Ferguson’s moderate effect size threshold (β ≥ 0.5), a number of other effect sizes approached this threshold (e.g., β = 0.45 for CFC-work future and work proactivity, β = 0.43 for CFC-health future and health monitoring, and β = 0.47 for CFC-college future and academic investment).
Consistent with a pattern of findings from previous studies of CFC and behavior (e.g., Adams, 2012), domain-specific CFC-I subscales were most strongly associated with engagement in risk behaviors, whereas domain-specific CFC-F subscales were most strongly associated with engagement in protective behaviors. These findings align with the buffering and susceptibility models of CFC, which treat CFC as a moderator of risk of self-control failure (Joireman et al., 2008). Put briefly, the buffering model posits that high CFC-F buffers against failures in self-control. Alternatively, the susceptibility model proposes that high CFC-I increases the risk of self-control failure. In the current study, domain specific CFC-I subscales were most strongly related to behaviors that are often attributed to failures of self-control (e.g., cigarette smoking and compulsive spending), whereas domain-specific CFC-F subscales were most strongly related to behaviors that require self-control, among other forms of self-regulation (e.g., health monitoring and academic engagement).
In the financial domain, the CFC-money immediate subscale was the strongest overall correlate of behavior. Both CFC-money subscales were significantly associated with time period for financial planning, but the stronger relationship observed was that between the immediate subscale and financial planning, where low CFC-money immediate scores were associated with longer-term financial planning. Furthermore, only the CFC-money immediate subscale was significantly associated with saving money, where low CFC-money immediate scores were associated with a greater amount of money saved. As planning and saving by nature are future-oriented constructs, one would expect any indicators of planning and saving to be more strongly linked with a measure of future orientation (e.g., Adams & Nettle, 2009; Anong & Fisher, 2013). Thus, the reason for these findings is not readily apparent. Distinguishing between the CFC subscales in the two-factor conceptualization means that low CFC-I scores do not necessarily denote greater concern for future consequences. Similar to other conceptualizations of present-oriented thinking, such as present hedonism (Zimbardo & Boyd, 1999), high CFC-I scores have been linked to high levels of impulsivity and lower trait self-control (e.g., Joireman et al., 2008). As such, low CFC-I scores may represent an ability to forgo immediate gratification and reward. Therefore, one possible explanation for this finding is that financial planning and saving may, at least in part, be driven by an awareness of and ability to overcome the immediate factors that facilitate compulsive spending.
Implications
The findings of the current study hold several important theoretical and potentially applied implications. The results indicate that the distinction between domain-specific CFC-F and CFC-I is meaningful with regard to self-reported behavior in particular domains. When Joireman et al. (2012) published the revised two-factor CFC-14 scale, they did so with a view to developing a scale with conceptual and practical utility. Some, albeit few, studies have evidenced the conceptual utility of a two-factor model by demonstrating that immediate and future CFC scale items differentially predict meaningful outcomes (e.g., Adams, 2012; Arnocky, Milfont, & Nicol, 2014; Dassen et al., 2015). Consistent with these reports, the current study found differential patterns of association between CFC-14 subscales and behaviors in some domains. Importantly, however, these patterns were only evident when measuring CFC using the domain-specific, but not the general, CFC-14 scales. For example, only scores on the CFC-health future and CFC-health immediate subscales were significantly associated with health monitoring behavior and smoking status, respectively. Overall, the findings challenge the pervasive assumption that high CFC-F (CFC-I) scores are indicative of a global future-oriented (present-oriented) outlook irrespective of domain (McKay et al., 2017), and highlight the importance of examining domain specificity not only in future-oriented considerations, but also in relatively immediate ones.
Understanding domain specificity in CFC may also have implications for improving the predictive utility of conceptual models of behavior and their use in applied contexts. A handful of previous studies have examined the validity of incorporating CFC (general) into such models. For example, Orji, Vassileva, and Mandryk (2012) tested an extended health belief model (Rosenstock, 1966) that included general CFC as an additional determinant of healthy eating behavior. Results indicated that incorporating individual differences in CFC improved the predictive utility of the model overall. The current findings suggest that incorporating domain-specific measures of CFC into such conceptual models might further improve their predictive utility, and this is particularly important for behaviors that affect an individual’s current and/or future well-being.
Although research on domain specificity in CFC is nascent, evidence from the current and recent studies suggests that conceptualizing CFC as a domain-specific construct may hold important practical implications for designing behavioral interventions with a temporal focus. Determining an individual’s level of CFC-F and CFC-I within a particular domain may provide valuable insight into the strategies by which to facilitate successful and sustained behavior change. For instance, a behavioral intervention for individuals with high CFC-I scores in the health domain could emphasize the following: (a) the immediate factors that best promote engagement in a healthy behavior, (b) the immediate consequences of not adopting a given healthy behavior, or (c) both. Equally, researchers can draw upon knowledge of an individual’s domain-specific CFC to design interventions that involve a temporal manipulation. In a recent study, Pancani and Rusconi (2018) reported that, compared with nonsmokers, smokers delayed the estimated onset time of both mild and severe smoking-related conditions (i.e., they placed the health-related consequences of smoking further into the future than nonsmokers). In the current study, only the CFC-health immediate subscale was significantly associated with smoking status, such that individuals with high scores on the CFC-health immediate subscale were more likely to smoke regularly or heavily. Interventions that aim to manipulate the perceived onset time of the adverse consequences of health-damaging behaviors like smoking may be especially beneficial for high CFC-I scorers in the health domain. Finally, as evidence of domain specificity in CFC accumulates, it may be usefully applied by health practitioners working with clients. Drawing awareness to an individual’s domain-related variability in present- and future-oriented considerations, and how this variability might correspond to their current lifestyle choices and behavior patterns, may facilitate the behavior change process.
Limitations and Future Research
Despite converging evidence for domain specificity in the CFC construct from the current and previous studies (e.g., Murphy & Murphy, 2018), little is known about why CFC may be a domain-specific construct. One possibility is that it may be related to an individual’s values. Individuals have different value priorities, and values have long been considered inherently linked to human behavior (Schwartz, 2007). Theoretical approaches to understanding the influence of values on human behavior adopt a value systems approach. For example, Rokeach (1968, 1973) described a value hierarchy encompassing 18 core values that guide decision-making and behavior (e.g., family security, national security, and social recognition), and in an early study, observed changes in behavior corresponding to changes in individuals’ value priorities (Rokeach & McLellan, 1972). With evidence of meaningful links between CFC scores and values orientations in the health and environmental domains (e.g., Joireman & Liu, 2014; Olsen & Tuu, 2017), future work could examine whether domain differences in CFC-14 scores correspond to, and can therefore be explained by, differences in value priorities across domains.
The main focus of this research was to test the concept of domain specificity in the CFC construct. We considered the most valid approach to test our hypotheses was to adapt the CFC-14 items to specific domains. However, scale adaptation or development was not the primary focus of the study, and so additional examination of the scales’ psychometric properties is required (e.g., examination of test–retest stability). Inspection of the item loadings for all two-factor domain-specific models indicated strong factor loadings overall. With the exception of eight factor loadings (out of 70 loadings on domain-specific scales) in the range of .4 to .6, all factor loadings were within the range of .6 to .9. However, the general CFC scale items have received some criticism with regards to readability (e.g., Crockett et al., 2009). Examination of domain-specific scale items raises similar readability concerns, and so a refinement of item wording may be required. Furthermore, the future subscale of the CFC-college scale did not correlate significantly with either subscale of the CFC-environment scale. As domain-specific CFC measures represent variants of the same overarching temporal construct, one would expect domain-specific subscales to be somewhat related. It is plausible that some domains may be more conceptually linked, for example, considerations of outcomes related to money and work, than others, such as considerations of outcomes related to college and the environment. However, it may be useful to conduct qualitative focus groups or interviews to gain some insight into participants’ interpretation of domain-specific scale items, to facilitate item refinement, and to map how domains may be conceptually and relationally organized. To date, no study has employed a qualitative approach to understanding the nature of the CFC construct, and what immediate and future behavioral outcomes participants might actually consider when responding to each item. This may inform further development of domain-specific scales and would also be a welcomed contribution to CFC literature.
Some scholars (e.g., Dassen et al., 2015; van Beek et al., 2013) have suggested that it may be more beneficial to measure CFC at a behavioral level. For instance, van Beek and colleagues developed two behavior-specific CFC scales (i.e., CFC-food and CFC-exercise), and found that eating behavior was most strongly associated with scores on the CFC-food scale, whereas exercise behavior was most strongly associated with scores on the CFC-exercise scale. In the current study, however, the CFC-health scale was significantly associated with both eating and exercise behaviors, suggesting that it is sufficient to measure CFC at the domain level. There is a risk in developing adaptations of the CFC scale that are too task-specific, as studies that measure more than one behavior type would require the inclusion of multiple behavior-specific CFC scales. This would require greater time commitment on behalf of respondents, which may not be necessary if a domain-specific measure is sufficient. This being said, it may be useful for future studies to compare the predictive utility of domain- and behavior-specific CFC-14 scales with regard to behavior within a given domain.
An important limitation of the current study is that all data were based on self-report measures of behavior. In CFC literature, there is a dearth of studies that incorporate objective measures of behavior (Joireman & King, 2016; Murphy & Dockray, 2018). Examining domain specificity in CFC using objective indicators of behavior across domains would strengthen confidence in the current findings. Furthermore, despite the fact that data were collected at three time points several weeks apart, they nevertheless constitute cross-sectional data. As such, examining domain specificity in a longitudinal design would provide evidence for prospective associations between domain-specific CFC scales and meaningful outcomes over time. Finally, while we believe that the concept of domain specificity in the CFC construct holds important conceptual and applied implications, given the limitations of the current study, particularly with regard the self-report nature of the data collected, it is important to rigorously test domain specificity in CFC using other forms of data to support the potential implications outlined above.
Contributions and Conclusion
Overall, the findings suggest that domain-specific CFC-14 scales represent empirically and conceptually distinct temporal constructs. This may explain why studies of CFC often produce small effect sizes for associations between general CFC and behavior (Murphy & Dockray, 2018), and why reports of associations between general CFC and some behaviors tend to be inconsistent (e.g., Adams & Nettle, 2009; Adams & White, 2009). Based on the results presented here and elsewhere, the use of the general CFC-14 scale in studies of behavior within a particular domain may diminish effect sizes or reduce the likelihood of detecting significant associations between CFC scores and the behavior of interest. The domain-specific adaptations of the general CFC-14 employed in the current study consist of items closely modeled to the intent and form of the general scale items. Using these scales, the findings suggest that individuals may vary in the extent to which they consider both future and immediate behavioral outcomes across substantive life domains, and furthermore, that measuring CFC within a specific domain facilitates a more accurate examination and understanding of how temporal considerations might influence decision-making around and engagement in domain-relevant behavior.
Supplemental Material
Murphy_OnlineAppendix – Supplemental material for The Consideration of Future Consequences: Evidence for Domain Specificity Across Five Life Domains
Supplemental material, Murphy_OnlineAppendix for The Consideration of Future Consequences: Evidence for Domain Specificity Across Five Life Domains by Lisa Murphy, Eimer Cadogan and Samantha Dockray in Personality and Social Psychology Bulletin
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Irish Research Council under Grant GOIPG/2015/15952.
Notes
Supplemental Material
Supplemental material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.