
Abstract
Children with conduct problems are at greater risk for internalizing problems. The objectives of this study were to (1) examine trajectories of internalizing problems among children with and without clinically significant conduct problems during the transition to adolescence; and (2) identify how academic achievement, peer rejection, parent socioeconomic status, maternal distress, parental warmth, child temperament, and receptive verbal functioning explained differences between the two groups. Children with conduct problems (N = 388, 45% girls) and a comparison sample without conduct problems (N = 299, 52% girls) were recruited from Quebec, Canada, when they were between the ages of 7 and 10 years, and were followed across 4 years. Mothers and teachers provided information on internalizing problems each year. Having clinically significant conduct problems was associated with higher initial levels of internalizing problems according to mothers and teachers, but not with changes in internalizing problems over time. With regards to teacher ratings, academic achievement, peer rejection, and negative emotionality partially explained differences in internalizing problems for youth with and without conduct problems. For mother ratings, maternal distress, negative emotionality, and peer rejection completely explained the association for girls, and partially explained the association for boys. Findings supported a multi-rater approach for understanding risk for internalizing problems among children with and without conduct problems. In particular, they highlight the importance of differences across context for understanding factors associated with vulnerability to internalizing problems.
Internalizing problems (i.e., anxiety, depression) during late childhood and early adolescence cause considerable distress and are linked with later negative mental health outcomes (Colman, Wadsworth, Croudace, & Jones, 2007). Not all youth are equally likely to develop these problems, such that youth with conduct problems are more vulnerable to internalizing problems than their peers (e.g., Wolff & Ollendick, 2006). Using a multi-rater approach, the goal of the present study was to use existing theoretical frameworks to better understand vulnerability to internalizing problems among children with and without conduct problems during the transition to adolescence.
Adolescence has been previously highlighted as an important period for understanding developmental psychopathology more broadly (Cicchetti & Rogosch, 2002). The transition to adolescence is a particularly important period for understanding vulnerability to internalizing problems as children navigate increasingly complex cognitive and social worlds (Moilanen, Shaw, & Maxwell, 2010). Some previous research suggests that internalizing symptoms gradually increase across this period (Lee & Bukowski, 2012; Reynolds, Sander, & Invin, 2010; Riina, Martin, & Brooks-Gunn, 2014), although other research indicates either stability in internalizing problems (Galambos, Barker, & Almeida, 2003), or that this increase may be exclusive to girls (Bongers, Koot, Van der Ende, & Verhulst, 2003; Leve, Kim, & Pears, 2005). Mixture modelling approaches support individual-level variation in trajectories of internalizing problems (e.g., Sterba, Prinstein, & Cox, 2007), and underscore the importance of identifying risk factors associated with the variation of internalizing symptoms. These trajectories, however, have focused on children drawn from typical populations, and may not provide insight into the trajectories of internalizing problems among children with histories of conduct problems.
Central to developmental perspectives of psychopathology is understanding how comorbidities, and the factors that contribute to these comorbidities vary over the course of development (Cicchetti & Sroufe, 2000). Longitudinal research has established the prospective link between externalizing problems and future internalizing problems within both general populations (e.g., Blain-Arcaro & Vaillancourt, 2017) and among youth at risk for conduct problems (Moilanen et al., 2010). A broader developmental psychopathology perspective, however, underlines the importance of identifying risk and protective factors central to variation in these developmental trajectories (Cicchetti & Rogosch, 2002). Several theoretical models have been proposed to explain why children with conduct problems are more vulnerable to internalizing problems compared to their peers (Lilienfeld, 2003). Notable among these explanations is the dual failure model (Patterson & Stoolmiller, 1991). This model proposes that conduct problems in particular, by way of their aggressive and disruptive symptoms, lead to failure across social and academic domains, which, in turn increase the risk for negative emotional affect and internalizing problems (Ward, Sylva, & Gresham, 2010). Academic failure and peer rejection are higher among youth with conduct problems (Patterson & Stoolmiller, 1991), and increase the likelihood of both internalizing and externalizing problems among typically developing children (Bornstein, Hahn, & Haynes, 2010; Fussner, Luebbe, Mancini, & Becker, 2016; Kiur, Leskinen, Nurmi, & Salmela-Aro, 2011; Herman, Lambert, Ialongo, & Ostrander, 2007). These dual failure variables may explain the elevated vulnerability for internalizing problems among youth with conduct problems, and may become particularly salient during the transition to adolescence (Fussner et al., 2016).
A second explanation of why youth with conduct problems are more likely to develop internalizing symptoms compared with other youth is the common-cause hypothesis (Lilienfeld, 2003). Children with conduct problems are thought to be more likely to report internalizing problems because the same genetic and environmental factors contribute to the development of both outcomes (Bornstein et al., 2010; Wertz et al., 2015). Indeed, following from multiformity theories of comorbidity (Krueger & Markon, 2006), the confluence of these risk factors would explain higher risk for comorbidity generally, and would not be exclusive to the link between conduct and internalizing problems. Four frequently proposed mechanisms for this common-cause framework are low family socioeconomic status, problematic parenting behaviors, difficult temperament and low levels of cognitive functioning. Adverse socioeconomic factors such as low levels of maternal education and low family income increase the likelihood of conduct problems (Bradley & Corwyn, 2002; Burke, Loeber, & Birmaher, 2002; Veenstra et al., 2006), and are associated with a greater vulnerability for internalizing problems (Slopen, Fitzmaurice, Wiliams, & Gilman, 2010). Similarly, parent-level variables such as higher maternal distress and lower parental warmth are associated with both greater risk for conduct and internalizing problems (Mazza et al., 2016; Slopen et al., 2010). Difficult temperament, and in particular negative emotionality, may also be an important mechanism for explaining the association between conduct and internalizing problems (Davis, Votruba-Drzal, & Silk, 2015; Eisenberg et al., 2009). Finally, children with lower levels of cognitive functioning are more vulnerable to both conduct and internalizing problems, suggesting that cognitive functioning may also serve as a common-cause variable (Benasich, Curtiss, & Tallal, 1993; Lynam, Moffitt, & Stouthamer-Loeber, 1993).
Context may shape the efficacy with which these two theoretical frameworks explain increased vulnerability to internalizing problems among children with conduct problems. Indeed, the moderate concordance of parent–teacher ratings of internalizing problems has been suggested to reflect in part the likelihood that these behaviors manifest differently across context (De Los Reyes & Kazdin, 2005). In other words, differences in rater-evaluations of children’s internalizing problems may reflect meaningful differences in the presence of these problems depending on the environment in which they are observed (De Los Reyes et al., 2015). In understanding how conduct problems are associated with the development of internalizing problems, dual failure variables may be anticipated to exert more of an influence in a classroom context, where teachers can directly observe the negative impact of academic failure or peer rejection. The impact of common cause variables may have more consequences within the home, where parents may be more aware of the emotional consequences of negative temperament or maternal distress.
Within a larger developmental psychopathology framework, common-cause and dual-failure variables provide two plausible theories by which childhood conduct problems augment the risk of later internalizing problems. From a practical perspective, however, common-cause and dual-failure variables are not always independent of each other. Indeed, higher rates of peer rejection and lower levels of academic achievement are associated with many of the common-cause variables such as cognitive functioning, family socioeconomic status, temperament, and parental practices (Clark & Ladd, 2000; Godleski, Kamper, Ostrov, Hart, & Blakely-McClure, 2015; Sirin, 2005). The interdependent nature of these variables underscores the importance of considering a complex array of dual failure and common cause variables simultaneously when exploring the link between conduct and internalizing problems.
The present study sought to identify the mechanisms explaining higher levels of internalizing problems among children with conduct problems compared to children without conduct problems. From a clinical perspective, we were particularly interested in understanding how these trajectories differed according to the presence or absence of clinically-significant levels of conduct problems. The conceptual model tested is presented in Figure 1. Both dual-failure (e.g., peer rejection and academic achievement) and common cause variables (e.g., family socioeconomic status, maternal distress, maternal warmth, child temperament, and child receptive vocabulary) were anticipated to mediate differences observed between children with and without conduct problems with regards to internalizing problems. It was hypothesized that dual failure variables would explain more of the variance in the disparities with regards to teacher-rated internalizing problems, while common-cause variables would explain more of the variance for mother-reported internalizing problems.
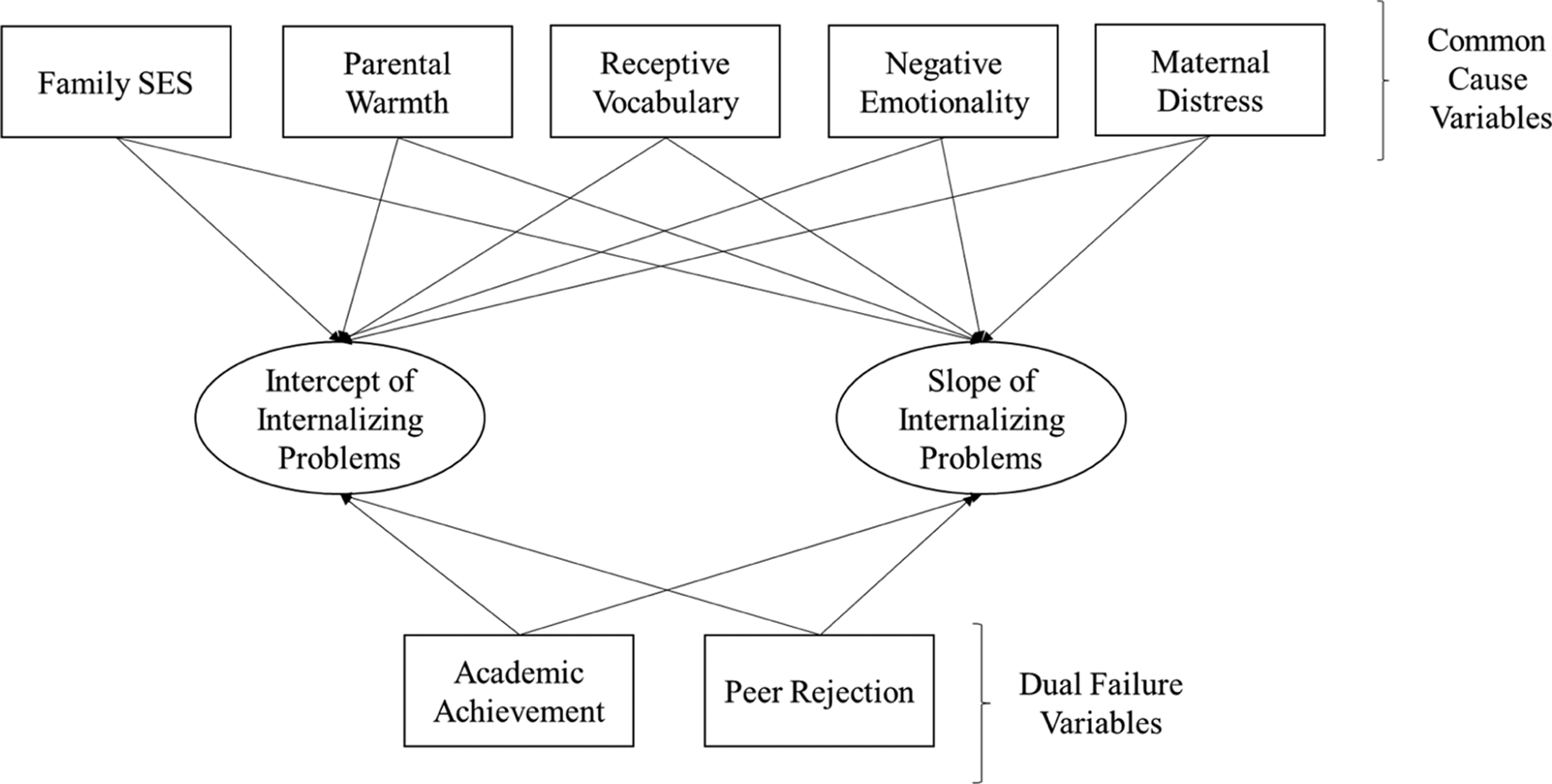
Conceptual model.
Finally, research generally suggests higher levels of internalizing problems among girls and higher rates of externalizing problems among boys (Costello, Mustillo, Erkanli, Keeler, & Angold, 2003; Galambos, Leadbeater, & Barker, 2004; Hankin, Mermelstein, & Roesch, 2007). Existing research is mixed, however, as to whether gender differences occur with regards to the association between internalizing and externalizing problems (Blain-Arcaro & Vaillancourt, 2017; Gooren et al., 2011; Klostermann et al., 2014). For this reason, gender was tested as a moderator in the current study.
Method
Participants
Following ethics review board approval, participants from in and around major population centers in Quebec, Canada were recruited from 155 francophone schools based on having conduct problems (N = 434, 44.7% girls) or the absence of these problems (comparison group; N = 310, 49.8% girls). Exclusion criteria for participating in this study were having an intellectual or sensory disability, having a pervasive developmental disorder, or living in a foster family. The children in the current sample were francophone, and of European descent. A multi-gated method of screening was used to detect children with conduct problems (Severson, Walker, Hope-Doolittle, Kratochwill, & Gresham, 2007). This multi-gated approach was used to maximize the number of children with conduct problems identified, while addressing potential limitations in relying exclusively on school-based referrals to identify all children with conduct problems (Eklund & Dowdy, 2014; Wehmeyer & Schwartz, 2001). Children were recruited based on being less than 10 years of age and receiving in-school services for conduct problems in schools with elevated deprivation indices, and were subsequently evaluated using the ASEBA in order to classify their conduct problem status. Children were included in the conduct problem group if they were scored as above the threshold (T score ≥ 65) on the DSM-oriented scales for conduct problems and oppositional problems of the ASEBA (Achenbach & Rescorla, 2000) as rated by either mothers or teachers. In addition, a total of 881 students (first to third grade), from schools with elevated deprivation indices who were not receiving services, were screened for conduct problems also using the same criteria on the ASEBA (participation rate = 71.5%). To obtain roughly equal numbers of boys and girls, all girls and approximately one out of four boys who was above the threshold on the ASEBA were invited to participate in the study
Participants in the comparison group were recruited from elementary schools with similarly high indices of deprivation to reduce their socioeconomic differences from the children in the conduct problems group. They were proportionally matched by sex and grade level to the children in the group with conduct problems, and were evaluated by parents and teachers to ensure that their scores on the ASEBA were below the threshold for conduct problems or oppositional defiant problems (i.e., that their t scores were below 65 according to both parents and teachers). The analytic sample of the current study was restricted to children between 7.0 and 9.9 years of age to narrow the age range used, and included 687 children (328 girls).
Procedure
Between 2008 and 2010, parents and children were met at home by two trained research assistants to complete questionnaires, following parental consent and verbal assent from the child. Teachers completed questionnaires over the telephone. The initial assessment (T1) was followed by assessments every 12 months for the three subsequent years (T2 to T4). Parents, children, and teachers received financial compensation for participating.
Measures
Conduct problems
Conduct problems at study inception were evaluated using the DSM-oriented scales for conduct problems and oppositional problems from the parent and teacher versions of the ASEBA (Achenbach & Rescorla, 2000). These scales included behavior problems consistent with symptoms of conduct disorder and oppositional defiant disorder listed in the DSM-IV (APA, 1994) with items such as “(shows) cruelty, bullying or meanness to others”. The conduct problems scale totaled between 13 items (teacher version) and 17 items (parent version) and the oppositional problems scale totaled 5 items for both versions. Items were scored on a 3-point scale ranging from 0 (not true) to 2 (very true or often true). Cronbach’s alphas varied from .85 to .93 in this sample. Youth with T scores of ≥ 65, as reported by either mothers or teachers were included in the conduct problem group.
Internalizing problems
Internalizing problems from Wave 1 to Wave 4 were assessed using the ASEBA mother and teacher report (Achenbach & Rescorla, 2000). The internalizing problems scale included questions on symptoms of anxiety/depression, social withdrawal, and somatic complaints, again using a 3-point scale (e.g., child cries a lot). T scores computed for teacher and mother reports were used in this study. Higher T scores indicated higher levels of internalizing problems. Descriptive statistics for these and other variables are presented in Table 1. The scale demonstrated good internal consistency (α = .87 to .89).
Descriptive statistics for the sample divided by gender and conduct problems.
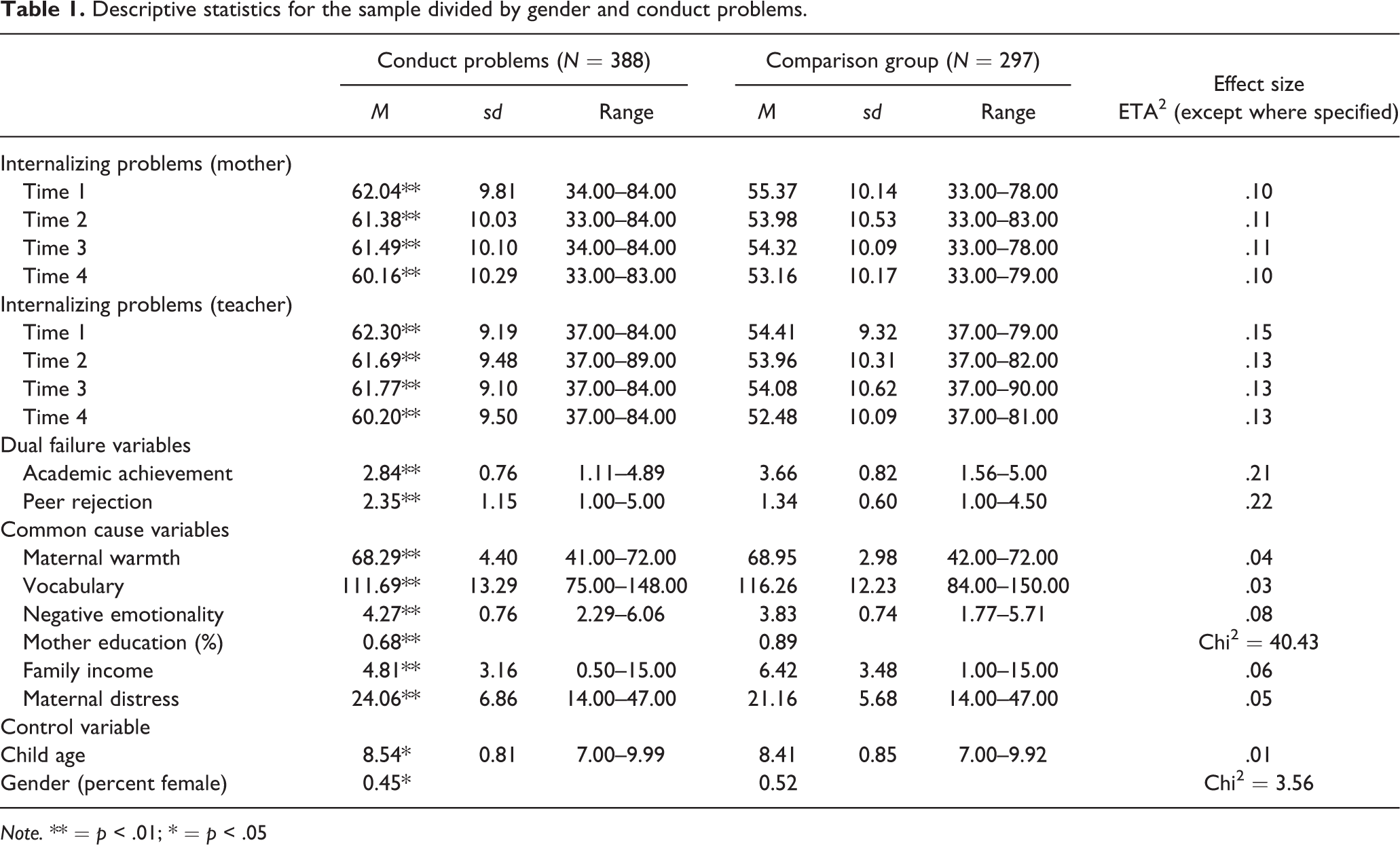
Note. ** = p < .01; * = p < .05
Dual failure variables
Academic achievement
Academic achievement was assessed by teachers during the initial testing period by using items drawn from the Academic Performance Rating Scale (DuPaul, Rapport, & Perriello, 1991). This scale was used as opposed to report card grades due to the highly qualitative nature of report cards among children of this age group in Quebec. Teachers replied to two questions in which they were asked to “evaluate the quality of the child’s work in mathematics” and “evaluate the quality of the child’s work in French (language arts)”. Children were evaluated using a 5-point scale (1 = between 0 and 64; 5 = scores between 90 and 100). Math and language arts scores were significantly correlated (r = .79, p < .01), and were combined for the current analyses.
Peer rejection
Peer rejection in the initial testing period was assessed using three items from the Teacher Peer Social Skills questionnaire (Dishion & Kavanagh, 2003). Teachers were asked to rate the child’s social acceptance and rejection by their peers on a 5-point scale ranging from 1 (very few) to 5 (almost all) with items such as “what percent of the child peers reject the child”. Higher scores on this measure indicated higher levels of peer rejection, and the measure showed acceptable reliability (alpha = .77).
Common cause variables
Maternal distress
Maternal distress was assessed in the initial testing period using the Psychological Distress Index-Short Form (Préville, Boyer, Potvin, Perrault & Légaré, 1992). Mothers were asked to describe their level of distress over the past week using 14 items on a 4-point scale ranging from 1 (never) to 4 (very often) (e.g., have you felt your heart beating fast in the absence of physical exercise), with higher scores indicating higher levels of distress. The scale showed reliability (alpha = .90) similar to those observed with validated norms (alpha = .91).
Maternal warmth
Maternal warmth was assessed in the initial testing period using the warmth subscale of the Perceived Parental Acceptance-Rejection Questionnaire (Rohner, 1984), as completed by mothers. This subscale included 18 items assessing parent’s perception of their warm and accepting behavior on a 4-point scale (e.g., I like to have my child with me), with higher scores indicating higher levels of warmth (alpha = .84).
Child temperament
Child temperament was assessed during the initial testing period by mothers using the negative emotionality subscale of the Child Behavior Questionnaire Short Form (Putnam & Rothbart, 2006). This scale contains 31 items assessing diverse aspects of negative emotionality (alpha = .87) (e.g., gets angry when asked to go to bed, cries when a favorite toy is broken or lost), with higher scores indicating higher levels negative emotionality.
Child receptive vocabulary
Child receptive vocabulary was measured in the initial testing period with the Peabody Picture Vocabulary Test-Revised (Dunn & Dunn, 1981), a measure of receptive vocabulary that is highly correlated with other measures of cognitive functioning (Hodapp & Gerken, 1999). A research assistant administered this test, which consists of 170 multiple-choice cards where children are asked to identify the image associated with the word. The test ends when the child obtains six wrong answers on eight consecutive cards. A higher score denotes a larger vocabulary.
Family SES
Family SES was assessed in the initial testing period using both maternal education and family income. Maternal education was assessed based on maternal self-report, and mothers were dummy coded based on having completed high school or not. Family annual income was assessed using an ordinal scale from the Quebec Child Mental Health Survey (Valla et al., 1997). This is a one item scale that asked families about their income in categories starting at less than C$6,000 (US$5,296.55) to more than C$150,000 (US$132,432). This variable was weighted to create a normal distribution. The median family annual income was between C$50,000 and C$59,999.
Control variables
Finally, child age was controlled using maternal report of the child’s birth date, which were subtracted from the date at which the evaluations were completed. Child gender was assessed based on reports by the parent at the initial testing period.
Analytic plan
Latent growth curve models (LGM) were used to explore trajectories of internalizing problems across the transition to adolescence using MPlus 7.11 (Muthén & Muthén, 1998–2013). This method permits for the identification of initial levels of and the rate of change for internalizing problems over time, and how different variables (e.g., the dual failure or common cause variables) are associated with these trajectories. Finally, Mplus addresses concerns regarding missing data employing Full Information Maximum Likelihood. Since inception, less than 6% of families initially recruited for this study have become untraceable or have refused participation in the study. Furthermore, although 5% of the data was missing from the analytic sample, listwise deletion would have resulted in a loss of 37% of the participants. In total, 91% of the sample completed measures at all four waves of data collection, 5% of the sample completed measures at three waves of data collection, 2% completed two waves of data collection and 2% completed only one wave of data collection. Little’s missing at random test was not significant (χ2 = 818.03, df = 882, n.s.), indicating that the data was missing at random.
Modelling was done in three steps. The first step modelled the shape of the curve for internalizing problems, with both linear and non-linear curves being tested. The next step added conduct problem status along with control variables (age and gender) to these models. The third step added dual failure variables (e.g., academic achievement and peer rejection) and common cause variables (e.g., receptive vocabulary, family SES, temperament, parenting practices, and maternal distress) to the models. In cases in which dual failure or common cause variables were significantly associated with the intercept or slope of internalizing problems, indirect effects were added to assess if these specific variables mediated between conduct problem status and internalizing problems. Indirect effects were calculated using the product of the coefficient approach (Preacher & Hayes, 2008). To test the indirect effects, bootstrapping (done 1000 times) was employed (Bollen & Stine, 1990; Shrout & Bolger, 2002). This bootstrapping approach relies on fewer normality assumptions within the data and can be used to identify which variables are serving as mediators (Hayes & Preacher, 2010). To assess if the association between conduct problem status and internalizing problems differed across gender, an interaction term for gender and conduct problem status was included in the second and third steps.
Results
Descriptive statistics (shown in Table 1) show that as suggested, a number of significant differences were observed across the conduct problems and non-conduct problems groups. In the next step of analyses, differences in the trajectories of internalizing problems were explored. Starting with teacher ratings, in the first step, a baseline model assessed trajectories of internalizing problems. A linear model fit the data best (χ2 = 9.93, df = 5, n.s., RMSEA = .04, CFI = .99). The mean for the intercept (B = 58.83) and slope (B = −.54, p < .01) was significant, indicating a slight decrease in internalizing problems across time. Significant variance was also observed around the intercept (B = 53.01, p = .05) and the slope (B = 3.79, p < .05), suggesting variation in initial levels of internalizing problems as well as in change over time. In the next model, intercept and the slope were regressed on conduct problems as well as the control variables (age and gender), and is presented as model 1 in Table 2. Having conduct problems was associated with higher levels of internalizing problems, but was not significantly associated with the slope (i.e., change over time) in these problems. No significant interaction was observed between gender and conduct problem status.
Trajectories of internalizing problems (N = 685).
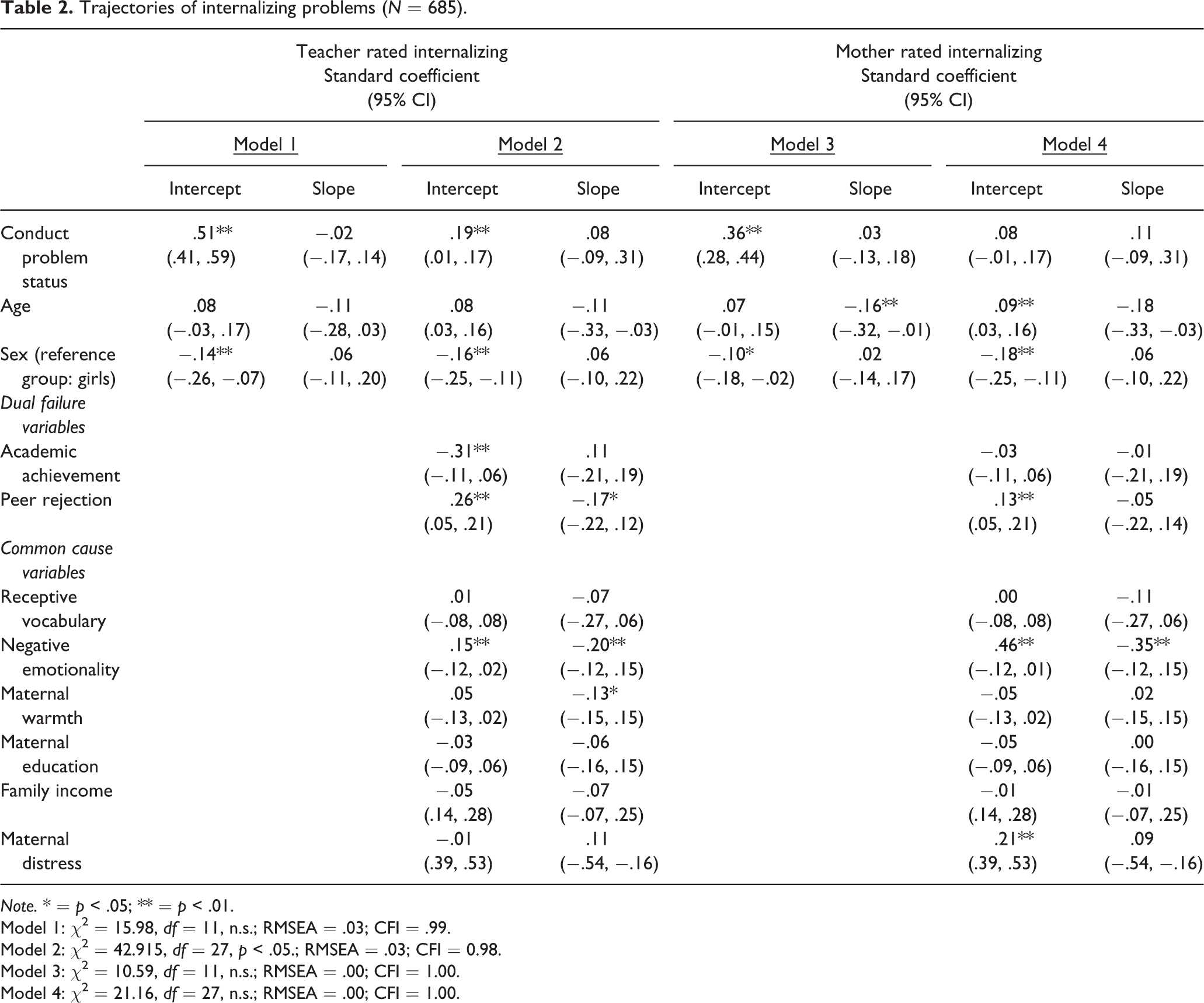
Note. * = p < .05; ** = p < .01.
Model 1: χ2 = 15.98, df = 11, n.s.; RMSEA = .03; CFI = .99.
Model 2: χ2 = 42.915, df = 27, p < .05.; RMSEA = .03; CFI = 0.98.
Model 3: χ2 = 10.59, df = 11, n.s.; RMSEA = .00; CFI = 1.00.
Model 4: χ2 = 21.16, df = 27, n.s.; RMSEA = .00; CFI = 1.00.
The third model included the dual failure (peer rejection, academic achievement) and common cause (family SES, receptive vocabulary, temperament, parenting, and maternal distress) variables, along with age. As can be seen in model 2 of Table 2, being in the conduct problems group continued to be associated with higher levels of internalizing problems. In addition, higher rates of peer rejection, and lower levels of academic achievement were associated with higher levels of internalizing problems. Negative emotionality was also associated with higher levels of internalizing problems. None of the other common-cause variables were associated with initial levels of internalizing. Higher levels of peer rejection and negative emotionality were also associated with greater decreases over time in internalizing problems. Higher maternal warmth, while not associated with initial levels of internalizing problems, was associated with greater decreases in internalizing problems over time.
The possible explanatory role of variables significantly associated with the intercept (i.e., peer rejection, academic achievement, and negative emotionality) and slope (i.e., peer rejection, maternal warmth, and negative emotionality) were subsequently tested using indirect effects. When indirect effects were modelled, conduct disorder status was significantly associated with lower school achievement (β = −.46, p < .01), lower parental warmth (β = −.21, p < .01), higher peer rejection (β = .47, p < .01), and higher negative emotionality (β = .28, p < .01). For the intercept, significant indirect effects were found for academic achievement (β = .15, p < .05 CI 99% .08, .20), peer rejection (β = .12, p < .05, CI 99% .07, .17), and negative emotionality (β = .19, p < .05, CI 99% .04, .30). While conduct problem status continued to be associated with the intercept, these findings suggest that this effect may be partially explained by both these dual-failure variables, as well as negative emotionality. No significant indirect effects were observed for the slope.
The same analyses were then conducted with maternal ratings of internalizing problems. Again, in the first step, the best fitting baseline model was a linear model (χ2 = 8.02, df = 5, p < .05, RMSEA = .03, CFI = .99). The means for the intercept (B = 59.12, p < .05) and slope (B = −.61, p < .05) were significant, as were the variance for the intercept (B = 85.51, p < .05) and the slope (B = 2.66, p < .05). This suggests that mother-reported internalizing problems decreased over time, but that significant variance was observed around both the intercept and the slope. The second step regressed the intercept and the slope of internalizing problems on conduct problems, while controlling for age and gender, and is presented as model 3 in Table 2. As was the case for teacher reported internalizing problems, conduct problems were associated with higher rates of internalizing problems, but were not associated with change in internalizing problems across time. The moderating role of gender was tested, and the interaction term was not significant.
In the third step, dual-failure and common cause variables were added onto the intercept and slope of internalizing problems (model 4, Table 2). Model fit continued to be good, but the association between conduct problem status and the intercept of internalizing was no longer significant. Higher levels of peer rejection, maternal depression and negative emotionality were all significantly associated with higher levels of internalizing problems, but only age and higher levels of negative emotionality were associated with decreases in internalizing across time. When indirect effects were tested, being in the conduct problems group was associated with significantly higher levels of negative emotionality (β = .28, p < .05), peer rejection (β = .47, p < .01) and maternal depression (β = .22, p < .05). Significant indirect effects between conduct problems and the intercept of internalizing problems via negative emotionality (β = .13, p < .01 CI 99%: .08, .18), peer rejection (β = .06, p < .01 CI 99%: .01, .11) and maternal depression (β = .05, p < .01, CI 99%: .02, .08) were observed.
A significant interaction emerged between gender and conduct problem status (β = −.33, p < .05). For boys, the association between conduct problems and mother-rated internalizing problems remained significant, even when controlling for dual failure and common cause variables. For girls, the association between conduct problems and initial levels of internalizing problems were no longer significant once other variables were included in the model. No other significant interactions were observed across gender in this model.
Discussion
In line with the existing literature, children with conduct problems had higher levels of internalizing problems from the first testing-period onward, according to both mothers and teachers (Wolff & Ollendick, 2006). The current findings add to this literature by suggesting that some (e.g., academic achievement, maternal distress) but not all (e.g., negative emotionality, peer rejection) of the mechanisms explaining greater vulnerability for internalizing problems among youth with conduct problems varied across parent and teacher ratings. These findings may indicate that context plays a role in conditioning the importance of dual failure and common cause models in explaining the disparities in internalizing problems observed across conduct problem status.
More specifically, when teacher ratings were used to assess youth’s internalizing problems, dual failure variables along with negative emotionality, partially explained higher levels of internalizing problems among youth with conduct problems. These findings support a substantive body of work suggesting the importance of dual failure variables for understanding risk for internalizing problems among adolescents with conduct problems (Patterson & Stoolmiller, 1991; Klostermann et al., 2014; Verboom et al., 2014), and may specifically underscore the importance of these dual failure variables for explaining internalizing problems within the school environment.
For mother’s ratings of internalizing problems, however, negative emotionality, along with maternal distress and peer rejection accounted (or in the case of boys, partially accounted for) the link between conduct and internalizing problems over time. The importance of negative emotionality, both for mother’s and teacher’s ratings of internalizing problems may highlight the role of a general “psychopathology factor” in understanding co-occurrence of internalizing and externalizing problems during childhood and adolescence (Lahey et al., 2015; Tackett et al., 2013). These findings support the importance of negative emotionality for understanding the association between conduct problem status and internalizing problems in general, and highlight the importance of early interventions and additional support for youth with higher levels of negative emotionality. Similarly, maternal distress was also associated with higher levels of mother-reported internalizing problems, and partially accounted for differences in internalizing among youth with and without conduct problems. The importance of maternal distress may reflect a larger literature indicating possible genetic factors associated with the development of internalizing problems (Wertz et al., 2015). These findings may also reflect how mother’s evaluations of their children’s internalizing problems are influenced by their own internalizing problems (Briggs-Gowan, Carter, & Schwab-Stone, 1996), and may explain why distress mattered more for maternal vs. teacher ratings.
The models showed some significant gender differences in terms of how conduct problems were associated with internalizing problems according to mothers, but not teachers. These findings reflect some (e.g., Blan-Arcaro & Vaillancourt, 2017; Gooren et al., 2011), but not all (e.g., Klostermann et al., 2014) of the existing research. Among girls, the link between conduct problems and internalizing problems (as rated by mothers) was no longer significant when dual failure and common cause variables were included in the analyses. Among boys, these factors partially accounted for differences between conduct problem and non-conduct problem groups for mother and teacher ratings of internalizing problems. The fact that conduct problems were no longer significantly associated with initial levels of internalizing once peer rejection and common cause variables were included among girls, while only partial mediation was observed among boys, may reflect the greater disruptive effect of aggressive behaviors among girls generally (Martin-Storey et al., 2011), particularly with regards to how their social failure is associated with the development of internalizing problems (Rose & Rudolph, 2006).
Although rates of internalizing problems did generally decrease slightly across time, conduct problem status was not associated with this change. Peer rejection, negative emotionality and maternal warmth for teacher-rated internalizing problems, and negative emotionality for mother-reported internalizing problems, however, were associated with decreases in internalizing problems over time. Negative emotionality and peer rejection were both associated with the intercept and slope of internalizing problems, most likely reflecting regression towards the mean. Conversely, maternal warmth was only associated with decreases in internalizing problems over time, reflecting previous findings that parenting practices are protective for children’s internalizing problems (Scaramella, Conger, & Simons, 1999).
A number of reasons may explain why the majority of variables, including conduct problems, were not associated with change in internalizing problems across time. According to both dual-failure and common-cause frameworks, the majority of the proposed mechanisms linking conduct problems to higher levels of internalizing problems would already be in place by late childhood. Indeed, previous work suggests links between conduct problems and internalizing problems can be observed during the initial years of formal education (Gooren et al., 2011; van Lier & Koot, 2011). This may explain why conduct problems were associated with general disparities in internalizing problems, but not with change over time (Edwards & Hanes, 2015; Gilliom & Shaw, 2004; Lilienfeld, 2003). While identifying clinically significant conduct problems prior to middle childhood is difficult, recruiting a younger sample may clarify the role of common cause and dual failure variables with regards to the initial onset of internalizing problems among youth with conduct problems.
Finally, while some of the proposed common-cause variables were associated with internalizing problems (e.g., negative emotionality, maternal distress) family socioeconomic status and cognitive functioning were not. Indeed, some previous work exploring these specific common-cause variables also found that they played a minimal role in the development of internalizing symptoms in children at risk for externalizing problems (Moilanen et al., 2010). These findings may also reflect previous work suggesting that common cause variables may be more relevant for trajectories of internalizing problems earlier in development (Leve et al., 2005). Again, a longer longitudinal study may highlight the role of common cause variables in explaining vulnerability to internalizing problems among youth with and without conduct problems earlier in development. Finally, with regards to receptive vocabulary, the exclusion of the children who met criteria for a diagnosis of intellectual disability may have reduced the variance, limiting the likelihood that this kind of vocabulary would be associated with trajectories of internalizing problems
Limitations and future directions
This study provided a unique opportunity to understand disparities in internalizing problems among children with and without clinically significant conduct problems over time. Some limitations, however, should be noted. First, while the current study benefited from the inclusion of both parent and teacher assessments of childhood behavior problems, youth perceptions were only available later on in the study. The lack of youth report is a specific limitation of the current study, and future work exploring trajectories of internalizing problems, particularly studies with older participants, may benefit from adding youth-reported internalizing problems. Including youth self-reports of internalizing problems would provide a useful avenue for future research. Second, the current findings are correlational. Similarly, assessments of conduct problem status, initial levels of internalizing problems, and the dual failure and common cause variables occurred at the same wave of data collection. This question of directionality needs to be taken into consideration in the interpretation of the findings, particularly with regards to factors such as negative emotionality, with may predate conduct problem status. The current sample consisted of white, francophone children recruited in and around urban areas in Quebec, and findings need to be replicated in other populations. An additional concern has to do with the possible nonindependence of teacher ratings. While over 3,000 teachers participated in this study, records were not kept of which teachers evaluated which students, and we estimate that a small number of teachers may have evaluated more than one student. Finally, it would be interesting to understand how the association between conduct problems and internalizing problems varies according to service usage. Understanding how conduct problem status is associated with change in internalizing problems within the context of service access may be particularly useful for understanding the mechanisms that explain this association.
Despite these limitations, the current findings have important clinical implications for understanding internalizing problems among youth with a history of conduct problems. The findings highlight how comparing parent- and teacher-reports may underline potential differences in the ways in which internalizing problems can be seen across context, particularly with regards to why children with conduct problems display internalizing problems. They also suggest several directions for future research. In particular, they support the universal importance of addressing negative emotionality among youth with conduct problems. In the school context, the findings also suggest the importance of supporting both the development of positive social relationships, and helping youth with conduct problems avoid academic failure. Finally, despite the relative stability of internalizing problems during the transition to adolescence, these findings support the importance of exploring disparities among children with and without conduct problems over time, as youth with conduct problems showed similar, albeit elevated trajectories of internalizing problems compared to their typically developing peers.
Footnotes
Funding
The author(s) declared receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the Canadian Institutes of Health Research (82694) and the Social Sciences and Humanities Research Council (37890 and 32 326706).