
Abstract
The purpose of the present study was to investigate parents’ profile, both at personal and familial levels, who live with and raise children with blindness or visual impairment. Twenty families participated in this study. Data were collected through semistructured interviews, while its analysis was based on qualitative methods focusing on terms of tracing categories and subcategories. The findings highlighted that the great number of parents’ responsibilities had a negative impact on their emotional state. This outcome may be reasonably attributed either to lack of effective management of their negative emotions or to recorded difficulties in obtaining all substantial information regarding their child’s life prospective well as in devoting too much effort to keep a balance in their family environment. In addition, parents underscored the vital role that professionals, friends, and unions play in their family cohesion and wellbeing. In conclusion, the results can add to the content of existing or future family support programs enriching them with even more constructive theoretical background from the field of counseling and inclusive practices.
Keywords
Introduction
It is evident that parents occupy a significant role in people’s lives, especially in young children (National Academies of Sciences, Engineering, and Medicine, 2016). Parents are entitled to provide their children a safe place to grow up and live to develop in the best possible way. However, parenting role may be very challenging for parents who have children with complex needs or disabilities. Relevant literature on parenting style and parenting stress has reported that highly stressed parents tend to engage in parenting behaviors that are more conducive to a child’s negative development (Baker et al., 2003; Hastings, 2009). In this case, parents usually fail to develop effective parenting strategies, regarding implementation of structured programs for their children, provision of opportunities for positive parent–child interactions, and usage of positive reinforcement (e.g., praise) to encourage social and behavioral competence (Brotman et al., 2011).
Specifically, when parents are informed that their child is visually impaired or blind, they get overwhelmed with stress and anxiety concerning their child’s future steps in all sectors of life. Such negative feelings occur because usually parents want to ensure their children’s quality of life and, in most cases, excessive anxiety leads to opposite outcomes (Christensen & James, 2017; Ha et al., 2011). The typical procedure for parents who have a child with blindness or visual impairment (from now on BVI) is to refer to experts to find out more information about the cause of their child’s visual impairment, to investigate any potential measures to restore degrees of their child’s sight, as well as to learn strategies and apply practices that improve the quality of their child’s life.
Relevant research support that families which have a child with BVI undergo stressed and pressurized situations which are multilayered and have profound effects mainly on three aspects of their life, such as: (a) social, which refers to the consequences of this situation in their relations with others (e.g., their friends do not have time to see them or the parents are not available to hang around with them); (b) psychological, such as shock, denial of the problem, sadness, depression, re-evaluation, overprotection and ambiguous tendencies with the ultimate goal of accepting the problem by the family members themselves (Palmer & Glass, 2003); and (c) financial, which relates to big amounts of money that need to be spent to provide the best support for their children at all aspects of their life (Bruce et al., 2007; Elliott & Shewchuk, 2003).
More analytically, regarding the first aspect – as mentioned above – the social dimension, parents feel the need to change their lifestyle and focus more on social support for their child. Social support, according to relevant literature review, contributes a lot to the members of families who have children with BVI, given that through supportive and constant interactions, the wellbeing of the whole family, can be stabilized and promoted by ensuring health, safety, and chances to participate in social and cultural events (Cimarolli & Boerner, 2005; Cimarolli & Wang, 2006; Reinhardt, 2001; Singletary et al., 2009). In addition, when parents become members of a parental network then they have the chance to share experience, knowledge, and worries with other families who have children with BVI. This involvement turns to be very therapeutic for the parents because through interaction, they are capable to exchange experience, and share knowledge helping them in this way to release their tension (Johnson, 2010; Lupón et al., 2018; Mackintosh et al., 2005).
Another dimension, relevant to social support, refers to effective cooperation between school and family. It seems that an appropriate school context may help the family members to cooperate smoothly and effectively. However, this kind of cooperation functions well provided that teachers have adopted an inclusive attitude toward students with BVI or toward students with disabilities in general (Elsman et al., 2016).
Regarding the second aspect, the emotional one, parents strive to deal effectively with all aspects of their child’s visual impairment, but this effort is usually accompanied with frustration, low self-esteem, and embarrassment. According to Lupón et al. (2018), parents undergo considerable stress due to certain internal factors such as personal expectations, assumptions, perceptions, and attitudes. Most often, parents seem unaware of how to cope with such stressful circumstances and moreover how to raise realistic expectations easily met by their children. In many cases, parents also tend to overlook their personal needs and desires believing that in this way they are fully devoted to their children. As a result, significant changes take place in the family dynamics and its members often feel incapable of taking care of their child’s needs. These situations may lead to depression and anxiety, jeopardizing quality of life for all family members (Scherer et al., 2019; Seltzer et al., 2001).
In addition, relevant research highlights the imbalance which usually takes place between the couple (i.e., father and mother). It is stated that mothers who have children with BVI spend more time in child care activities compared to fathers and consequently they are more frequently engaged in their children’s life matters (Riga & Andreou, 2018). According to researchers, mothers’ responsibility when raising a child with disabilities increases significantly compared to that of fathers’ who are usually more detached and for this reason mothers are very emotionally involved and worried about whether they can sufficiently meet their children’s real needs. In addition, because of this emotionally overloaded attachment, which has been developed between mothers and their children, mothers are more easily prone to depression, making them gradually distant from the couple’s interpersonal relationships (Bambara, 2009; Bambara et al., 2009; Rees et al., 2007; Vu et al., 2005; Zeng et al., 2012 On the other hand, fathers seem to be less anxious than mothers, less emotionally involved in the child’s everyday difficulties, while they usually focus primarily on issues related to financial security as well as social acceptance (Hanson, 2002).
Regarding the financial aspect, a relevant study conducted by Calvo & González, (2004) found that the presence of a child with BVI in a family requires extra economic resources to cover its additional personal needs. Usually, these personal needs refer to health care expenses and the members of the family need to dedicate a great amount of time in taking care and support their child who has disabilities. Thus, in many cases, the father or the mother – usually mothers – take the decision to reject job opportunities, focus on their child’s needs and put aside their personal ambitions or even their everyday needs. In other cases, families are forced to employ support personnel so that their child can receive specialized educational or therapeutic services, which are usually offered by state medical administrations or/and private specialized health organizations (Calvo & González, 2004).
To sum up, it turns out that parents who have children with BVI are subjected to a series of unprecedented, stressful and thus frustrating situations during the demanding upbringing of their child (Zheng, 2014). Also, it is worth mentioning that parents’ emotional state and behavior, particularly in cases of children with BVI, depend on specific variables such as the child’s degree of vision loss, the presence of siblings, close friends, and relatives (Hanson & Lynch, 2004; Sakkalou et al., 2018; Zeng et al., 2012). In addition, the variety of families’ emotional state varies a lot because it depends on the support and experience, they get from other therapeutic services (Liebermann et al., 2017). Finally, some risks that nearly all researchers stress out and according to them jeopardize the balance and homogeneity of families who have children with BVI are issues relevant to daily fatigue as well as to many practical accommodations and arrangements that need to be sorted out daily (Britner et al., 2003; Kandel & Merrick, 2007).
The general objective of this study was to investigate parents’ basic needs, both at personal and familial levels, while raising children with BVI. Thus, the following research questions were formulated:
(a) What are the needs of parents who have children with BVI regarding their role in the parenting process?
(b) What are the sources of support that parents of children with BVI are looking for, so they can establish and reinforce their role in the parenting process?
(c) What are the personal needs of parents who have children with BVI during the parenting process?
Methodology
Participants
Twenty families who had a child with BVI participated in the present study. The mean age of the children with BVI was 12.05 years and their age range was from 5 to 18 years old (70% was the percentage of those with congenital BVI, whereas 30% was the percentage of those with acquired BVI).
Although, both members from each family were invited to participate, in the end only one member of each family took part. In specific, 14 mothers and 6 fathers accepted to share their needs and experience with the authors (mothers were much more willing to participate in the research). Eight mothers out of 14 in total were not working; they were exclusively engaged in taking care of their children who had BVI. Also, two of the fathers had retired early to better assist their children. The educational level of the participants ranged from postgraduate studies to primary (elementary) school education.
The local community of the blind (LCB), brought in contact the authors and potential families to participate in the present study. Convenience sampling was chosen as opposed to random sampling, which is the most popular sampling method, in terms of providing useful information to answer research questions (Creswell, 2011).
Materials
The study is classified as qualitative, and the data were obtained through interviews. The type of semistructured interview was used as a tool for the data selection and the interview guide was organized around three main axes: (a) parents’ needs in relation to their children, (b) search for help, and (c) parents’ personal needs. The structure of the semi-structured interviews was based on the Family Needs Survey (FNS) Family Questionnaires (Dunst et al., 1988; Hanley et al., 2003) and the Family Support Scale (FSS) (Hanley et al., 1998). The FNS scale has been used to investigate the needs of parents with children with disabilities, in conjunction with the family environment and consists of 33 questions. Likewise, the FSS includes 11 questions and aims to describe the type of support that each family member receives from the other family members.
Because the topic of the interviews was very sensitive and perhaps the interviewees wanted to talk about negative emotional experiences, the authors decided – although there was an interview guide – to provide the participants some sort of flexibility to express themselves freely if they wanted. In particular, the basic themes of the FNS and FSS scales (as described above) were used as the starting point of the interview. A digital recorder was used for the interviews after the participants’ consent. The average duration of the interviews was around 60 min each.
Research design
In carrying out this study, a specific structure was followed, comprising the following steps: a. contact the LCB to find potential families, b. design the interview guide according to the objectives and the research questions of the study, c. conduct two pilot interviews to improve clarity and coherence in the interview guide and its potential questions. The first contact was initially done by phone informing the families about the research and assuring their anonymity (Guanglun et al., 2017). The authors spoke with 32 families and in the end 20 accepted to participate. The ethical principles of the Declaration of Helsinki were followed and signed consent were obtained from the participants using the appropriate forms and procedures suggested by the World Medical Association. In turn, the authors went to the families’ homes based on the latter’s availability and all interviews were recorded with the consent of family members.
Data analysis
A qualitative descriptive design was adopted for this study and an inductive thematic analysis was carried out (Fereday & Muir-Cochrane, 2006). Based on relevant literature, there are two approaches that could be applied to process and analyze the obtained data. The first approach refers to the “bit-by-bit” method in which the data are analyzed at sentence (or word) level (i.e., very small units) and then categorized into broader categories based on their thematic relevance. The second approach treats the data as a whole and the elaboration of data is based on wider thematic units. In the present study, the data processing and analysis was based on the development of categories and subcategories; that is, a combination of the two approaches (Creswell, 2011; Dey, 1993). Also, according to Rice and Ezzy (1999), the tracing process of categories, themes or/and sub-categories required from the authors “careful reading and re-reading of the data” (p. 258) to arrive at a consensus regarding thematic patterns within the obtained data.
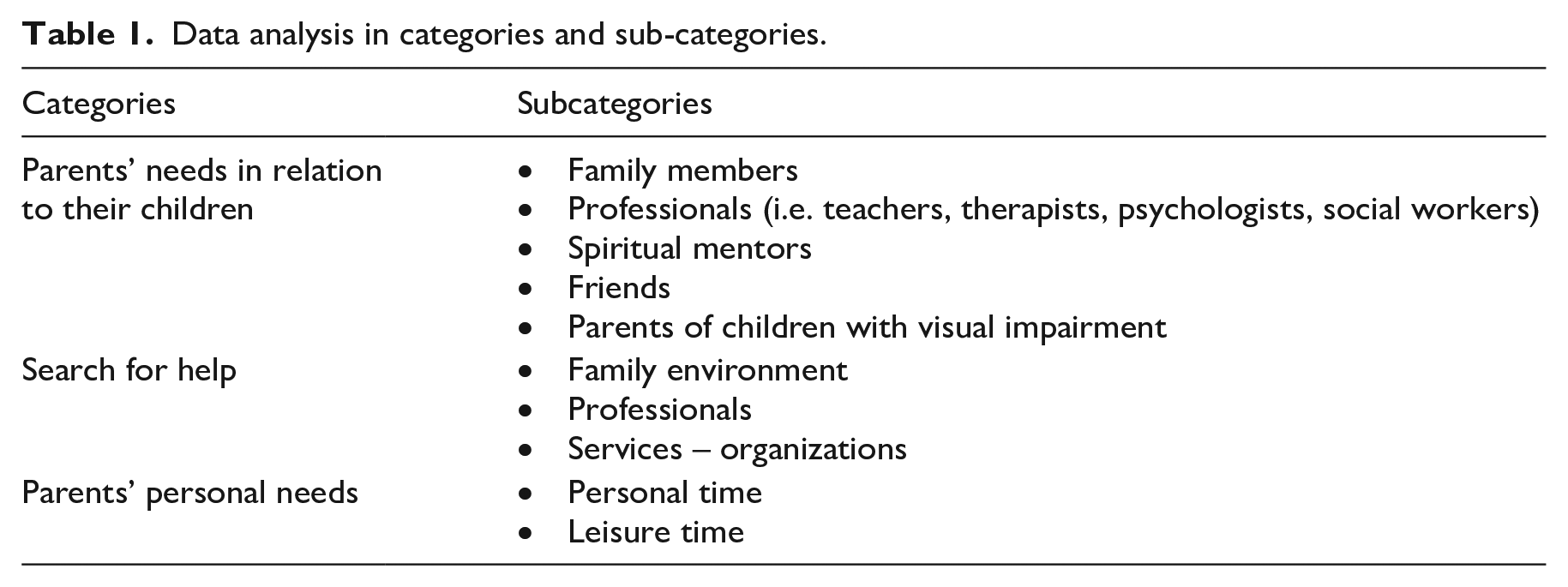
Hence, for each key issue, categories were developed in conjunction with corresponding sub-categories in accordance with each research question. In total, the analysis revealed three broad categories with 10 corresponding subcategories (see Table 1). In the “Results” section, many quotations are provided, and all children are referred to with the initials of their names, to assure anonymity.
Data analysis in categories and sub-categories.
Results
The results were organized and presented according to the three main axes which composed the semistructured interviews (see above) providing data upon (a) the family environment, (b) the school environment, (c) club unions, and (d) the personal context of the participants. The authors elaborated the data and finally concluded to three broad categories which: (a) “parents’ needs in relation to their children,” (b) “search for help,” and (c) “parents’ personal needs.”
Parents’ needs regarding their children
The analysis of the data revealed the category “Parents’ needs in relation to their children” and five subcategories seemed to compose it. The participants referred to several people with different occupations they felt they would talk to about their fears, challenges, responsibilities, and effective management of negative emotions and stressful situations. These people were members of the family, members from the school environment, professionals, persons from church as well as other parents with children with BVI. Some subcategories and extracts are provided below.
Discussion with family members
Most of the participating parents mentioned that to overcome their worries about their children’s vision problems, they would like to discuss it primarily with persons from the family environment, then with professionals, and last with friends or members from church. In total, 17 out of 20 participants (85%) had this strong feeling to discuss and share their worries about their children’s needs with family members, because according to them “family members show real interest and can feel you better than anyone else.” Based on the obtained data, fathers put great emphasis on the process of sharing through discussions with their wives and other relatives, whereas mothers reported that they needed constant psychological support and advice regarding practical issues to enhance the quality of their children’s everyday life. Fathers seemed to worry about issues related to finance and home management and highlighted the significant support and understanding they received from their wives. Some relevant extracts are provided below: We are husband and wife but at the same time we are friends, . . ., soulmates. . . (Father 3) We manage to deal with all this stuff through conversation and good communication. . . my wife helps me a lot and I believe I help her too . . . (Father 6) We both take care of the household. (Father 4) I discuss everything with my husband and my siblings . . . my mother, my father stood by me very much when they were alive . . . unfortunately they have passed away. (Mother 3)
Discussion with professionals
Almost all participating parents stated that they would like to talk with their child’s teacher or therapist, because they strongly believed that this communication would help a lot the social and academic progress of their child (Nourian & Namvar, 2016). Similarly, because of their need for counseling, they wanted to interact with various professionals such as psychologists, social workers, and in some cases psychiatrists, to get feedback and support on regular basis. Some relevant extracts are provided below: Maria’s [pseudonym] teachers are very helpful, and I’d like to talk with them more often . . . I’d be very happy though if I could discuss more with a social worker . . . dunno . . . I feel that discussions with experts regarding the issues that my child is facing right now, would help me a lot to understand Maria, to be there for her . . . (Mother 6) Yes, they help me a lot because I find it difficult to cope with . . . I spent hours and hours with all these responsibilities, and I definitely need somebody to count on. (Mother 7) I’d like to talk to a psychologist on regular basis. It is important . . . it is crucial . . . the presence of an expert, the advice of a specialist. (Mother 9) For now, I believe a social worker would be just fine . . . later on? Well . . . we’ll see . . . perhaps we may need a psychologist to understand our child’s problems and then support him more efficiently. (Father 3)
Discussion with spiritual mentors
Furthermore, according to the parents’ perception, church could also play a vital role in supporting emotionally and psychologically their children, through their spiritual mentors. Nevertheless, a lot of the participating interviewees (more than 10), had second thoughts regarding the appropriateness of this support on behalf of the church due to unpleasant experiences they had in the past. We went to the church, but they cannot really help you. They told us to have faith in God . . . what we really need is proper meetings on regular basis with a social worker or a psychologist . . . once a month or once every fortnight, here or in their place. . . whatever . . . it doesn’t really matter. (Father 4) I believe that priests in church understand you very much. They seem to understand the situation but, in the end, it turns out, that they cannot really help you . . . (Father 1) Yes, why not? There are spiritual mentors in church that can help a lot. . .if my child wants to get some advice from the church, I don’t have any kind of objections or reservations to go for it. (Father 5) Yes, I would like the help of a priest to support me spiritually, but I do also need the support from a specialist such a social worker or a psychologist. (Mother 6)
Discussion with friends
All participating parents mentioned that they like to talk and share their worries with friends, but on the other hand, they did realize in the end that friends cannot have genuine empathy because they have their own families and concerns about them. In general, parents did appreciate their talks with friends, but it seemed they did not expect something that would soothe away their pain and worries (Dehghani & Nazari, 2014). Yes, we have friends, and we talk a lot but not family issues. (Mother 4) My opinion? [. . .], friends cannot not offer substantial help in this matter. Usually, we just sit down and have a cup of tea or coffee, and this is it; nothing more. . .nothing less. . . (Mother 2) Friends is an extremely important chapter in life but you have to dedicate some time to see them, to talk with them. . .when the vision problems started in our family we weren’t, you know, the ideal company. . .so it turned out that our friends didn’t have enough time to visit us. (Mother 7)
Discussion with other parents of children with visual impairment
Finally, most parents (14 out of 20, 70%) stated that it was nice to have contacts with other parents of children with BVI, but it was quite clear to them that they cannot – or they do not want – to be in their shoes. Well, maybe it is kind of relief to talk and share your problem with other families who have a child with visual impairment . . . but I think it’s completely different in each case. I mean every family has its own rules and ways to deal with this kind of problem and to my experience most of time these ways differ from family to family. (Mother 1) I used to meet with other families who have children with visual impairment, but not anymore. My boy is much involved now in activities; and to be honest, I try to keep it in this way, nobody can really understand you. (Father 2)
Search for help
The next broad category “search for help,” referred to families’ actions, when they looked for something specific in terms of their needs. Table 1 depicts the subcategories that the “search for help” category consists of; that is, family environment, professionals, as well as organized services and associations/organizations (in total three subcategories).
Family environment
Seven parents out of 20 (35%), put a great emphasis on the assistance which was provided by other family members, and they underscored the quality and effectiveness of this assistance. Some representative extracts are provided below: My daughter has a great understanding about her brother’s difficulties and helps us a lot. I believe she has great empathy, and we are very happy. (Mother 6) No, there is no need to remind or explain all this stuff every day. The vision problem is part of our everyday life so there is no point to mention it every day . . . we live with it. . . (Mother 8)
On the other hand, some issues were also mentioned which did not accord with empathy, support, or understanding. My husband is kind of . . . how can I put it? . . . it is difficult for him to accept it. You see initially my boy was sighted but because of an accident he lost his sight. . .it is 7 years now. . .and still he is quite distant from him. (Mother 2) We are apart right now with my wife. The only thing we discuss is about the child, how does he feel, what does he want to do, stuff like that. (Father 2)
In addition, grandparents seemed to have a role and a “voice” in the family network since they supported the family financially and emotionally. My mother. . .she is always on my side. . .great support! I love her so much!. (Mother 3) When I was in despair my parents were there . . . there are no words to express my gratitude to them. (Mother 10) My parents help me a lot, but you know, at the same time they are very concerned,. . . whether they’re doing the right thing when they take care of their grandchild. (Mother 11)
Professionals
Fourteen parents out of 20 (70%) highlighted the great support they had from professionals. According to their statements, they much appreciated professionals’ tips and advice for alternative means to enhance their communication with their children. Most parents referred to different professionals’ occupations such as psychologists, child psychologists, social workers, speech therapists, child psychiatrists, and physiotherapists. We need professionals and to be honest we are desperate for any kind of information that comes from people who know very well their job. (Father 3) Well, the major problem is the lack of a very good ophthalmologist. I have to confess that it was quite an adventure for us to find a good doctor, a person that we can count on for our child. . .anyway . . . We are ok now but we paid the price for others’ mistakes. . . (Mother 3)
Parents also mentioned the need to have carers on a regular basis for their children provided by the government or by the local authority. However, they stressed the need to have carers who have been trained on special needs and disabilities because it seemed that regarding this matter there were many drawbacks. As a result, family members, especially mothers, took care of their child who had BVI. It would be very helpful for me and for D [the name of the child] to have a person with professional knowledge and patience to play with D, walk around, to have fun and stuff. Unfortunately, it was very hard to find such person, so we decided to handle it by ourselves, but as you understand it’s different to play with your mother and different to play with a person who doesn’t belong to the family. (Mother 6)
Services and organizations
The majority of the participating parents (14 out of 20) commented in a very positive way the support they received by associations of and for the blind. They underscored the fact that they had almost every single day contact with members of the associations and received support and assistance on a regular basis. Oh yes, the association helps a lot! It is an asset for us. (Father 6) I don’t know if I could make it without the precious support I got from the association. They are excellent people with great experience. (Mother 7)
On the other hand, six parents (30%) stated that they did not need any assistance from any association for the blind. They preferred to take all appropriate measures and manage family issues on their own. They also mentioned the indifference on behalf of the state services, every time they refer to them, for an assistance or information regarding special programs for children with BVI. My child is never looked after by others. I don’t need help from others. I can manage it by myself. What I have realized so far is that we have to take matters into our own hands . . . (Mother 4) The truth is that from ordinary people I don’t expect anything. . .they look at us with compassion; but I do expect readiness and professionalism from state services, but again the frustration and disappointment is big . . . I don’t want to discuss it anymore. (Mother 1)
Parents’ personal needs
The third broad category, “Parents’ personal needs” included subcategories related to parents’ personal time with a great emphasis on leisure activities.
Personal/leisure time
This category includes data which reflected the parents’ needs for free time to do something which would release their stress and tensions. In specific, 15 parents (75%) seemed to need time for personal peace and calmness in everyday life. In general, they had very little time at their disposal for themselves and almost all their activities were strongly linked with the activities of their children. Some extracts are provided below: Free time in our home? You know something . . . Having a blind child is like a full-time job. (Mother 4) There is no free time. I really need it, but don’t have it . . . (Mother 8)
Parents expressed the need to do leisure activities. Parents felt that they need some time for themselves. I really need some time for myself, but it looks impossible . . . I have the full responsibility for my child. (Mother 7) Unfortunately, there is no free time for me. . .never stop working, from the office to home to take care F [. . .her blind child] and vice versa . . . (Mother 3) The truth is that I have very limited free time; only when B [his blind child] is at school, then I can have some time for me but still I feel it is not enough. (Father 2)
Only five parents (25%), mostly fathers, stated that they had enough free time to do things with their family. Yeah, there is time to do stuff as a person; it’s important for me. (Father 5) There are ways to find free time. My child [he meant his child with BVI] plays the guitar, swims in the winter, has English, French lessons . . . There are many activities, so there is some time for me as well. (Father 6)
Discussion
The first research question deals with parents’ needs regarding their role in the parenting process. Relevant research holds that parents who have children with disabilities need to discuss and share their needs and anxieties with members of social networks; this may be due to their need to effectively manage their tensions or their grief or frustration (Arshad & Lodhi, 2015). Similarly, it was revealed in the present research that there were few families which did not feel the need to communicate with others. They stated that they preferred to deal on their own, the issues which were relevant to their child’s visual impairment because – as they argued – they know better than their friends their child’s needs and all the effective ways for support and communication (Donaldson, 2017). This finding is also in line with the findings of Bailey et al. (1999), who supported that this specific parental behavior perhaps constitutes a reflection of a compulsive overprotection which in the end excludes them from many social activities such as meeting with friends, traveling, and so on (also, Donaldson, 2017).
With regard to the second research question and the quest for help from the family environment, what was highlighted from all parents, was the support among spouses. This support was described as financial, physical, and emotional (Dehghani & Nazari, 2014). As parents have pointed out, they did not need to explain their child’s situation to the rest of the extended family since there is understanding and mutual help between spouses (Arshad & Lodhi, 2015). It seems that mostly mothers are those who feel more vulnerable to their child’s situation and for them the support from their spouses is valuable and irreplaceable. This finding has been highlighted in various surveys. According to relevant literature review, mothers of children with BVI usually experience more anxiety and feel sadness, and their social and professional lives as well as their family relationships are seriously affected (Sen & Yurtsever, 2007; Tröster, 2001).
Accordingly, mothers, because they usually dedicate more time for their children with BVI compared to their husbands, are much more involved in their child’s daily care and as a result they are led to increased symptoms of depression and anxiety (Neely-Barnes & Dia, 2008). A similar outcome was also found in the research conducted by Oelofsen and Richardson (2006) regarding mothers of children with developmental disorders which, according to the researchers, had increased anxiety and their physical condition was negatively affected compared to fathers’ physical condition (Bailey et al., 1999; Fewell, 1986; Heiman, 2002; Lustig, 2002; Zeng et al., 2012).
Regarding the help and assistance of grandparents, the participating parents reported that grandparents proved to be great carers and assistants at many levels (i.e., emotionally, financially, etc.) (Chang & McConkey, 2008; Fewell, 1986). However, despite the great help they received from grandparents, parents also stressed the fact that grandparents are often afraid to take on the responsibility of their child who had the visual impairment (Dehghani & Nazari, 2014).
An important support factor for parents and their children who have visual impairments is the help they receive from the rest of the kids, their siblings, with typical development (Ravenscroft, 2016). As the parents have mentioned, the siblings of the children with BVI are valuable helpers and supporters for them as they make a decisive contribution to the care and upbringing of their brothers or sisters who have BVI. Similar results have been found in research conducted in children with intellectual disability (Dehghani & Nazari, 2014). In addition, as observed in relevant literature review, even when parents get older, retired, or have passed away, the siblings are in charge to take care of their brother or sister who have a disability (Heller & Arnold, 2010).
Regarding family friends, they seemed to be compassionate and were involved without feeling sorry for the child who had the visual impairment; instead, they helped the children with BVI to join the social community, but not to a large extent. Similar results may be found in research which dealt with families of children with disabilities (Dovigo & Janssen, 2017; Dunst et al., 1994; Hong et al., 2014).
Moreover, school, church, state, and other organizations such as unions, based on the present study, contributed positively, and constituted an important source of help and support by strengthening the resilience of the participating families (Figueiras & Arcavi, 2015). In the present study, 70% of the participating families said that it helps a lot to discuss the problem of their child with doctors, psychologists, teachers, priests, and so on (Christensen & James, 2017). Nevertheless, each family had a different hierarchy regarding the support and help they received (i.e. spouses, relatives and friends, church, parents of other children with similar problems, government agencies, unions, and so on), and this may be due to different parents’ network, expectations, and culture (Oktorina & Wahyu, 2015).
Finally, with regard to the personal-individual needs of the participating parents (third research question), 75% stated they would like more free time for them. More specifically, parents reported that they generally do not have free time and that was something that concerned them a lot and felt quite unhappy. According to relevant research, this situation is partly responsible for parents’ depression because creative leisure centers or day centers allow parents to relax and have a break from the intensive care of their child (Burton-Smith et al., 2009).
The case of parents who have children with disabilities or even professionals who work for years with children with disabilities, may constitute a case of the “burn out” phenomenon. Burnout is an important and complex situation, and the WHO included it in the International Classification of Disorders ICD-11. In the relevant literature, burnout has become an area of research and intervention in the fields of work psychology and health and deals with issues of emotional exhaustion, depersonalization, and reduction of personal performance that can occur in individuals who are involved in stressful situations too often and too long (Sadziak et al., 2019). Hence, it is important for professionals and parents to recognize the signs of burnout and in turn develop intervention programs, such as mindfulness programs, reducing stress, and burnout situations (Anclair et al., 2018).
In total, data collection as well as the analysis carried out revealed many and interesting elements regarding the emotional “landscape” of families who had children with BVI (Elsman et al., 2016). It may be argued that the participants in the present research experienced many stressful situations regarding the “burden” of many responsibilities which most of them had to do with their children who had BVI. It seems that all these responsibilities had a negative impact on their emotional state (Davis, 2009). These responsibilities or obligations included: management of negative emotions, struggle to get all the information that they needed regarding the condition of their child and the opportunities for their child, as well as struggle to keep a balance in the family among others (Donaldson, 2017). Parents often mentioned that they had to make very often difficult decisions and felt very lonely during these situations. According to relevant research, this kind of situations constitutes high-risk factors that can affect parental psychological resilience and family harmony (Kandel & Merrick, 2007).
The majority of the participating parents stated that they had positive emotions from the process of externalizing their feelings to people they are familiar with, discussing their positive and negative experiences and interacting with people with whom they feel emotional proximity (Donaldson, 2017). This finding indirectly confirms the findings of other surveys according to which the families of children with BVI and the children themselves feel content and emotional support by other members of their close environment (Chang & Schaller, 2000; Lupón et al., 2018; Reinhardt, 2001).
Restrictions and suggestions
In the present study, the sample was small indeed, but it is numerically satisfactory if one considers that the percentage of people with BVI is small compared to people who are sighted (Ravenscroft, 2015). Nevertheless, we strongly believe that the above limitations do not reduce the dynamics and effectiveness of this research; on the contrary, it highlights the complexity of the needs and the mental and emotional state of families which raise a child with BVI. Issues of future investigation can be placed in the effectiveness of family support programs – such as counseling programs – which will be based on spouses’ needs, emotions, and desires, in terms of their child with disabilities increasing the quality of their lives (Parween, 2015; Selikowitz, 2006). Torreno (2012) especially argued that when parents behave and react in an overprotective way, their children are more likely to become either passive and introvert (i.e., lack of interest at a personal and social level, too relied upon their parents, etc.), or excessively independent and involved in dangerous activities. Therefore, it can be assumed that every single parent represents a unique case, each one of them carrying their own beliefs and maintaining their individual prospects of life (Hashemi et al., 2017).
Finally, it would be important to investigate in detail the categories of support structures that exist for families who have children with disabilities, and whether and to what extent they contribute to a more effective coverage of their needs and thus to the emergence of a more optimistic attitude toward disability. For example, researchers indicate that what matters most for parents is the quality of support services compared to the number of specialists they work with (Perry, 2004; Yesilkaya et al., 2021). Hence, it may be a good suggestion to put under the microscope of the “burn out” phenomenon parents’ situation, who raise children with BVI, or children with disabilities in general.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.