
Abstract
Compression therapy is still the cornerstone in the treatment of PTS. The therapy is primarily focused on the decrease of the AVP, enhancement of the microcirculation and reduction of the edema. In our practice, most patients are initially treated with short stretch bandage to reduce the edema. Medical Elastic Compression Stockings (MECS) class II (CEN 23–32 mm Hg)or class III (CEN 34–46 mm Hg) with a high stiffness index are prescribed after the edema is disappeared. The prescription will be for a lifelong usage of stockings. Correction of saphenous reflux, deobstructing and stenting might be considered in certain patients with PTS.
The post-thrombotic syndrome
The post-thrombotic syndrome (PTS) is a frequently (23–60%) reported complication in patients with a previous deep vein thrombosis (DVT). 1 The incidence of PTS is 10% one year after an episode of DVT, increasing to 50% over a period of 5 to 8 years. 2
When treating the acute deep vein thrombosis, not only the anticoagulant therapy is important for the prevention of PTS, but also the compression therapy. Brandjes et al. showed the importance of medical elastic compression stockings (MECS) after acute DVT. In this randomized study, the use of a sized-to-fit graded MECS applied within 2 to 3 weeks of the initial diagnosis, reduced the rate of mild-to-moderate and severe PTS by about 50%. 3 The rationale behind the use of MECS for the prevention of PTS is derived from the increased venous flow velocity during MECS therapy. High velocity will result in more rapid thrombus resolution. After acute DVT, fibrinolysis, thrombus organization, neovascularization and recanalization will consecutively occur in the deep venous system. The recanalization and the inflammatory response to acute thrombosis directly damages the vein wall and venous valves in the deep venous system. Therefore, a quick resolution of the thrombus is essential for limiting the damage to the valves.
The heart is a pressure pump and not a suction pump. Therefore, other mechanisms are required for the venous return under the influence of gravitation. The physiological return of venous blood from the legs is dependent on vis a tergo, vis ab fronte, the muscles in the legs in combination with the venous valves, the venous tonus and the arteriovenous pulse pump. Out of all these mechanisms, the calf muscle pump (CMP) is by far the most important contributor to the transport of the venous blood. The number of sufficient valves is essential in order to keep balance between the output (venous return) and reflux volume of the CMP. If reflux is present, the capacity of the CMP is essential for a sufficient reduction of venous pressure. However, the function of the CMP is dependent on the ability of the vein to collapse. The ability decreases when the vein wall becomes more stiff or when the elasticity of the vein is lost which is the case in patients with PTS. When this occurs, the veins are unable to push the blood cranially which could lead to CMP dysfunction. Finally, venous hypertension will occur when the venous volume exceeds the capacity of the calf muscle.
As a result of the venous hypertension, the vein will distend further, leading to more vulvar incompetence. Eventually, progression of the venous dysfunction occurs and the superficial venous system is affected. This will results in an increase of venous resistance and subsequently a progression of ambulatory venous hypertension
The venous hypertension causes a disturbance of normal flow in small capillaries and increases capillary filtration. This will lead to interstitial edema, trapping of enzymes and finally a decreased cutaneous oxygen concentration (Figure 1). As a result of this, patients develop signs of venous stasis including pre-tibial edema, redness, induration of the skin, hyperpigmentation, venous ectasia, collateral veins (which in some patients are formed across the lower abdomen, known as de Palma vein), atrophie blanche, lipodermatosclerosis and finally venous ulceration. Patients with PTS experience symptoms such as leg pain, heaviness, cramps, itching, fatigue, paresthesia and venous claudication. These symptoms can affect the quality of life tremendously and therefore have considerable socioeconomic consequences.
4
Pathophysiology of chronic venous insufficiency.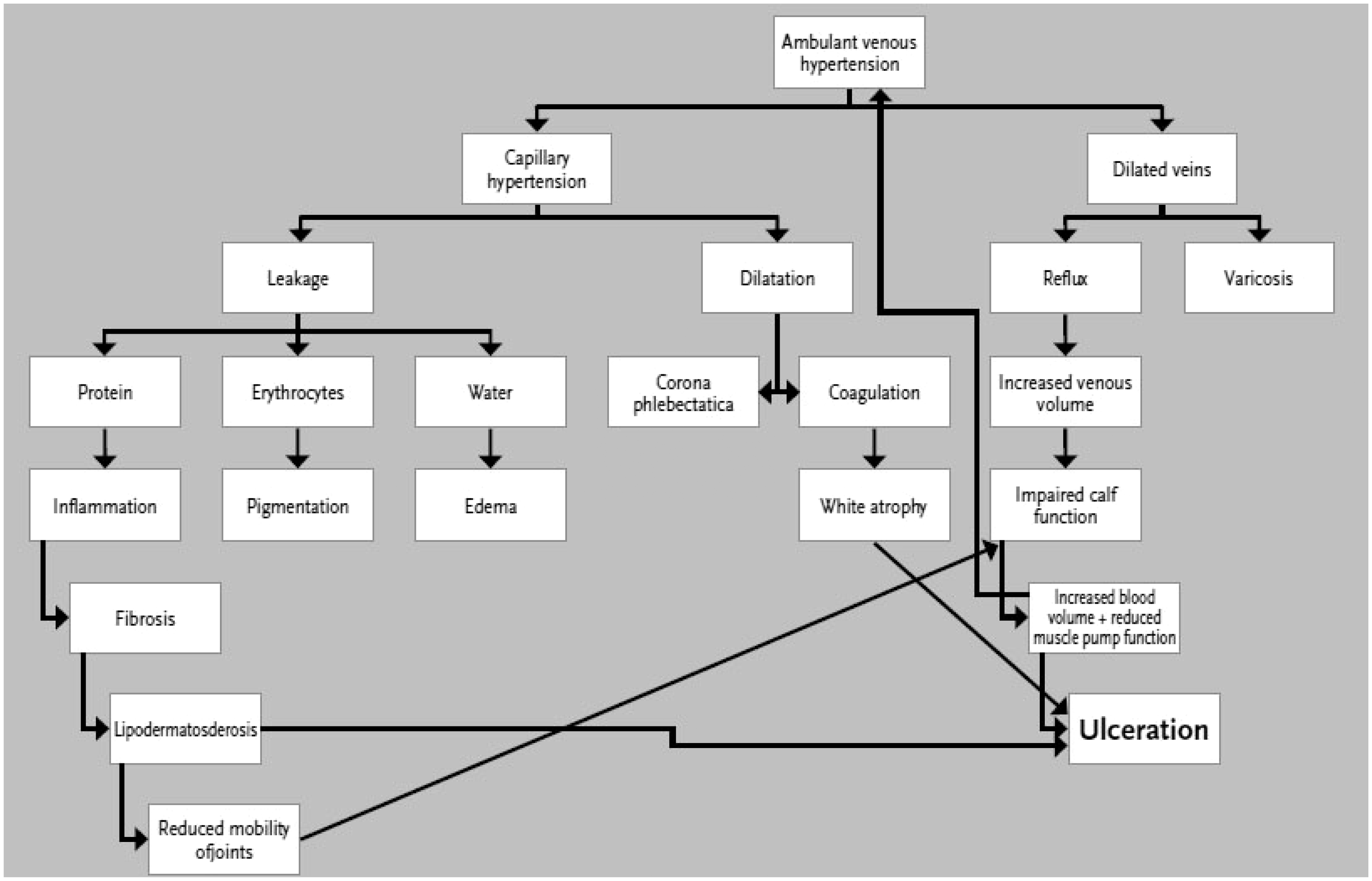
Villalta scale.
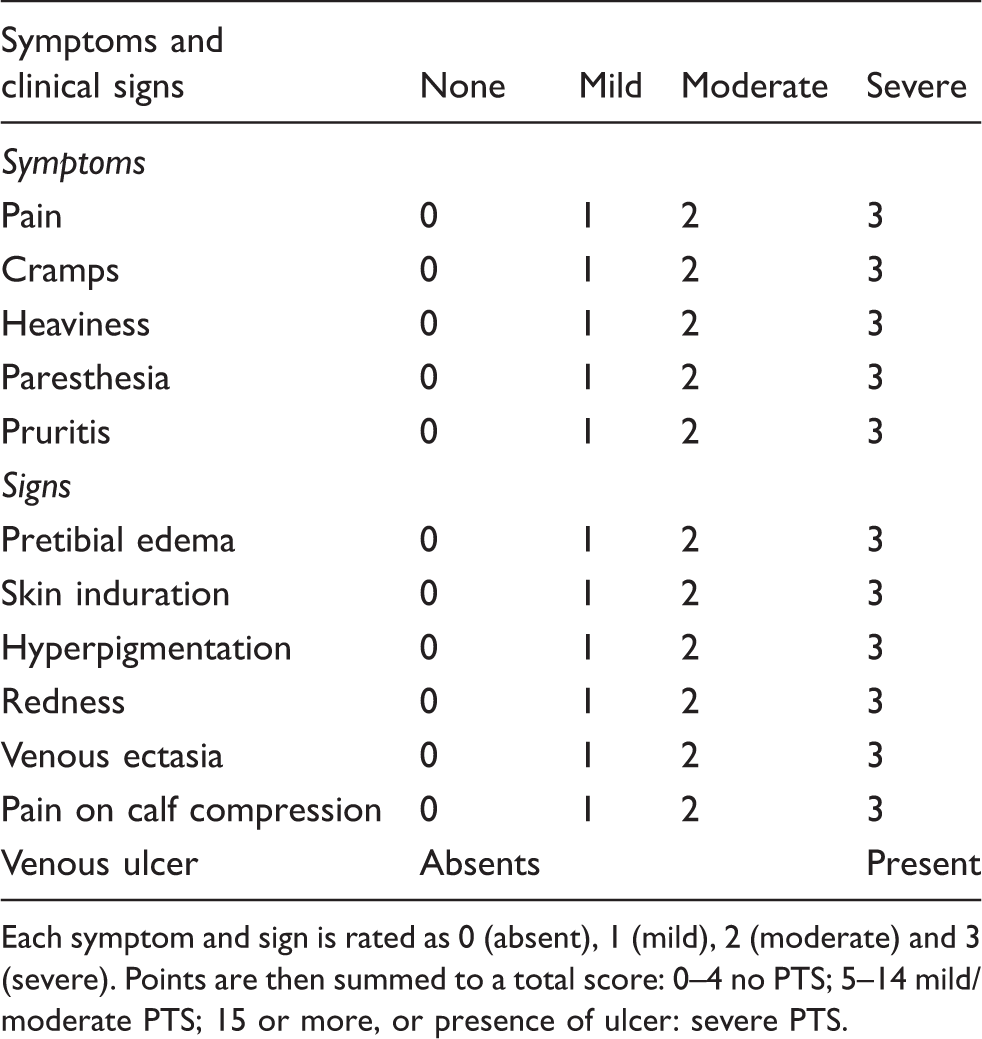
Each symptom and sign is rated as 0 (absent), 1 (mild), 2 (moderate) and 3 (severe). Points are then summed to a total score: 0–4 no PTS; 5–14 mild/moderate PTS; 15 or more, or presence of ulcer: severe PTS.
Diagnosis of PTS is based on both symptoms and clinical signs in a patient with previous DVT, independently from the presence of anatomic of hemodynamic abnormalities on duplex ultrasound. Nevertheless, the duplex ultrasound (DUS) investigation is an essential and often forgotten investigation in these patients.
The DUS investigation can clarify the degree of venous valve incompetence, residual obstruction, recanalized veins and collateral channels. Based on the DUS findings, the PTS can be classified according to the pathophysiologic condition (reflux, obstruction or both). In some patients, additional investigations are needed, such as plethysmography, phlebography, invasive ambulatory venous pressure measurements, MRI or CT scans.
In daily practice, the Villalta score, the CEAP classification, the leg circumference and the DUS investigation are important tools in the follow up of PTS.
Compression therapy
Today, compression therapy is still the cornerstone in the treatment of PTS. Compression therapy is divided in elastic and non-elastic compression materials. Technically, it is very important to distinguish between elastic compression (e.g Medical Elastic Compression Stocking ( MECS), short- and long stretch bandages) and non-elastic compression (e.g. non-elastic zinc oxide plaster and flannel bandages). Several compression methods may be used in the treatment of PTS. However, most patients are initially treated with adhesive or non-adhesive short stretch bandages to reduce the edema. For this therapy it is important to remove the elastic bandages at night to prevent arterial inflow problems in supine position. 6
Compression therapy with elastic bandages is contraindicated in patients with peripheral neuropathy (diabetes mellitus), severe peripheral arterial disease (PAD), totally occluded deep venous system, severe congestive heart failure (CHF), contact allergies or undefined ulcers. In these patients, intermittent pneumatic compression (IPC) therapy may be a good alternative. However, the treatment of patients with PTS and comorbidities should not only be focused on the reduction of edema but also on the comorbidity itself.
Once the edema is disappeared with compression or IPC, MECS can be prescribed.
The beneficial positive effects of compression therapy on the function of the venous system of the leg are improvement of the function of the CMP, reduction of the venous diameter, increase of venous flow velocity, reduction of reflux, increase arterial perfusion and increase of interstitial pressure. This leads to a lower ambulatory venous pressure (AVP), prevention and reduction of edema and enhancement of the microcirculation. 7 Eventually, it will result in the alleviation of leg swelling and limits the progression of PTS. Besides the therapeutic effects on chronic venous diseases (CVD) and PTS, it has been demonstrated that healthy individuals (e.g. athletes and passengers on long flights) also benefit from compression therapy.8–11
Background knowledge on compression is essential for understanding the compression therapy mechanism. A compression device creates pressure on the surface of the leg and thus on the skin. This pressure is defined as the interface pressure. The interface pressure is transmitted to the dermis, veins and muscles. However, liquid (in the leg also known as edema) has an incompressible nature. Therefore, the circumference of the leg is decreased by the compression of the soft tissue and muscles only.
In standing position, venous pressure is defined by the hydrostatic pressure. Because of this, standing venous pressure (SVP) depends on the person's height and will be between 80–100 mm Hg in the average European. The SVP of patients with CVD is equal to the SVP of healthy individuals. However, the difference between the healthy and the affected legs lies in the drop of venous pressure to 20–25 mm Hg versus <20 mm Hg during ambulation. The insufficient drop of venous pressure will result in an increased AVP, also known as venous hypertension. Compression therapy aims to compensate for the deficit of venous pressure drop during ambulatory. In case the AVP does not drop below 40 mm Hg, the CEN
*
compression class II MECS should compensate the difference between the venous hypertension and the AVP in healthy legs (Figure 2). The interface pressure alone (+/− 27 mm Hg) is not sufficient to compensate for the venous hypertension. However, effective compression is not only determined by interface pressure, but also by the characteristics of the used materials such as hysteresis, elasticity and stiffness. For a long time these latter three characteristics were measured in static condition only. Nevertheless, compression therapy is mainly effective during ambulatory and the behavior of compression materials should be investigated under dynamic conditions. Stolk et al. introduced this idea and developed a dynamic leg-segment model to measure the dynamic stiffness index (DSI) of MECS.
12
They showed that the amplitude of the interface pressure is highly correlated with the stiffness of the MECS during walking. The stiffness is the result of the internal friction between the threads, stiches and the resistance against deformation. According to the CEN (Table 2), the stiffness is defined as the increase in pressure at the B-level (i.e. the ankle at the point of its minimum girth), when the circumference at the B level increases by 1 cm.
13
A correct combination of interface pressure and the DSI is essential for prescribing optimal MECS.
The interface and venous pressures (mm Hg) in a patient with healthy or CVD legs, with or without high or low stiffness MECS, during supine position, standing and walking. The stiffness classification according to the CEN. Source: CEN8188:2010adnexB.5.4stiffness.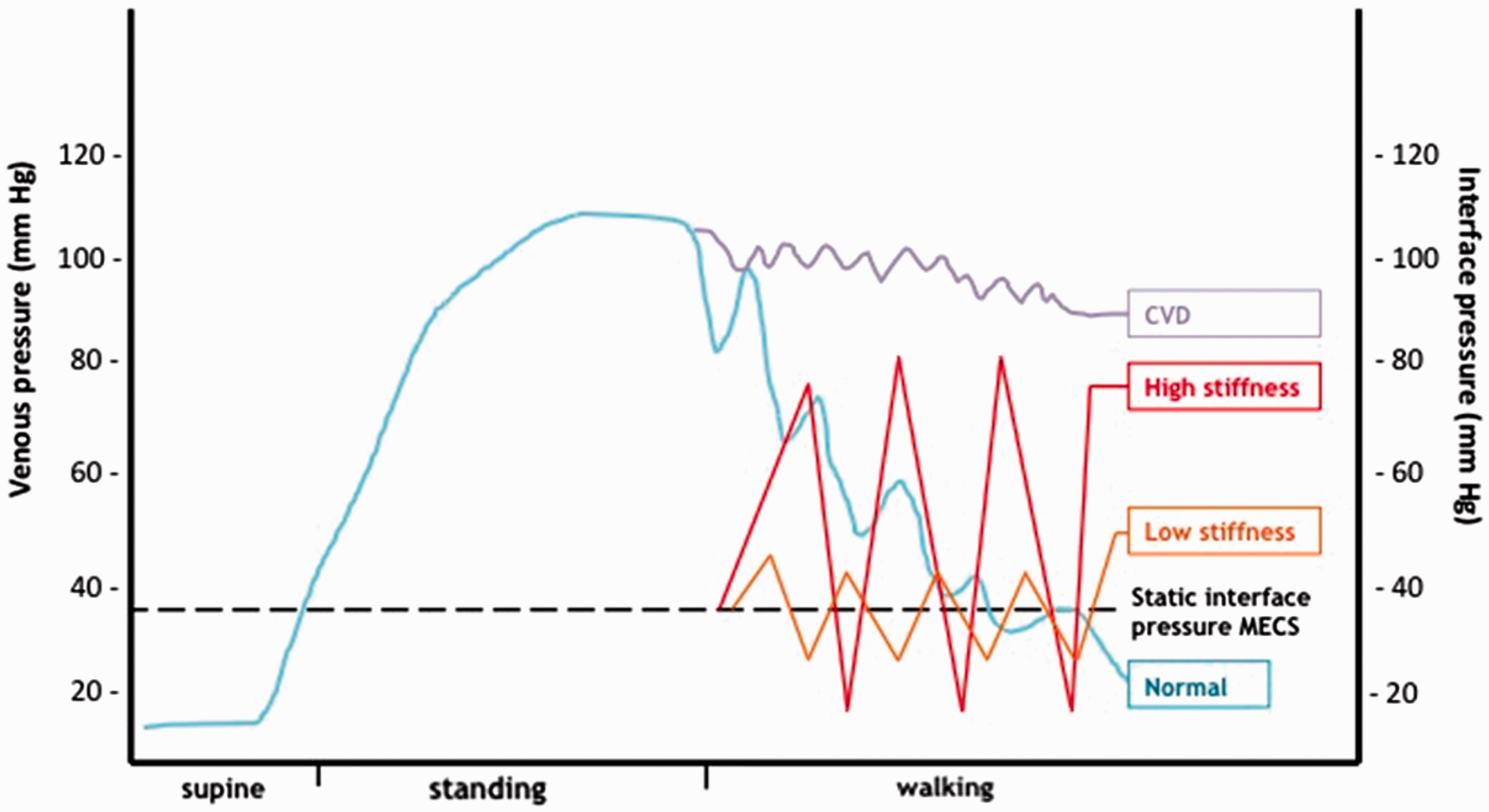

In static conditions, the rise of venous pressure by this elongation is quite low, between 1–5 mm Hg. However in ambulation this pressure dramatically increases to 60 mm Hg and more. This can be explained by the phenomenon of hysteresis, the loss in recovered linear length of an elastic product when it recoils after exposure to repeated stretch-relaxation operations. The circumference of the legs, especially in the B1 region, changes continuously during walking (normally a frequency of 1 Hz = 1 gait cycle per second). If the material of the MECS contains a high hysteresis, the elastic elongation of the MECS is unable to keep up with the circumferential changes of the leg during a normal walking speed. Depending on the stiffness of the MECS, the pressure will more or less rise when the circumference increases. In the opposite direction, when the circumference of the leg is decreasing, the interface pressure drops. This phenomenon is known as the massaging effect of MECS.
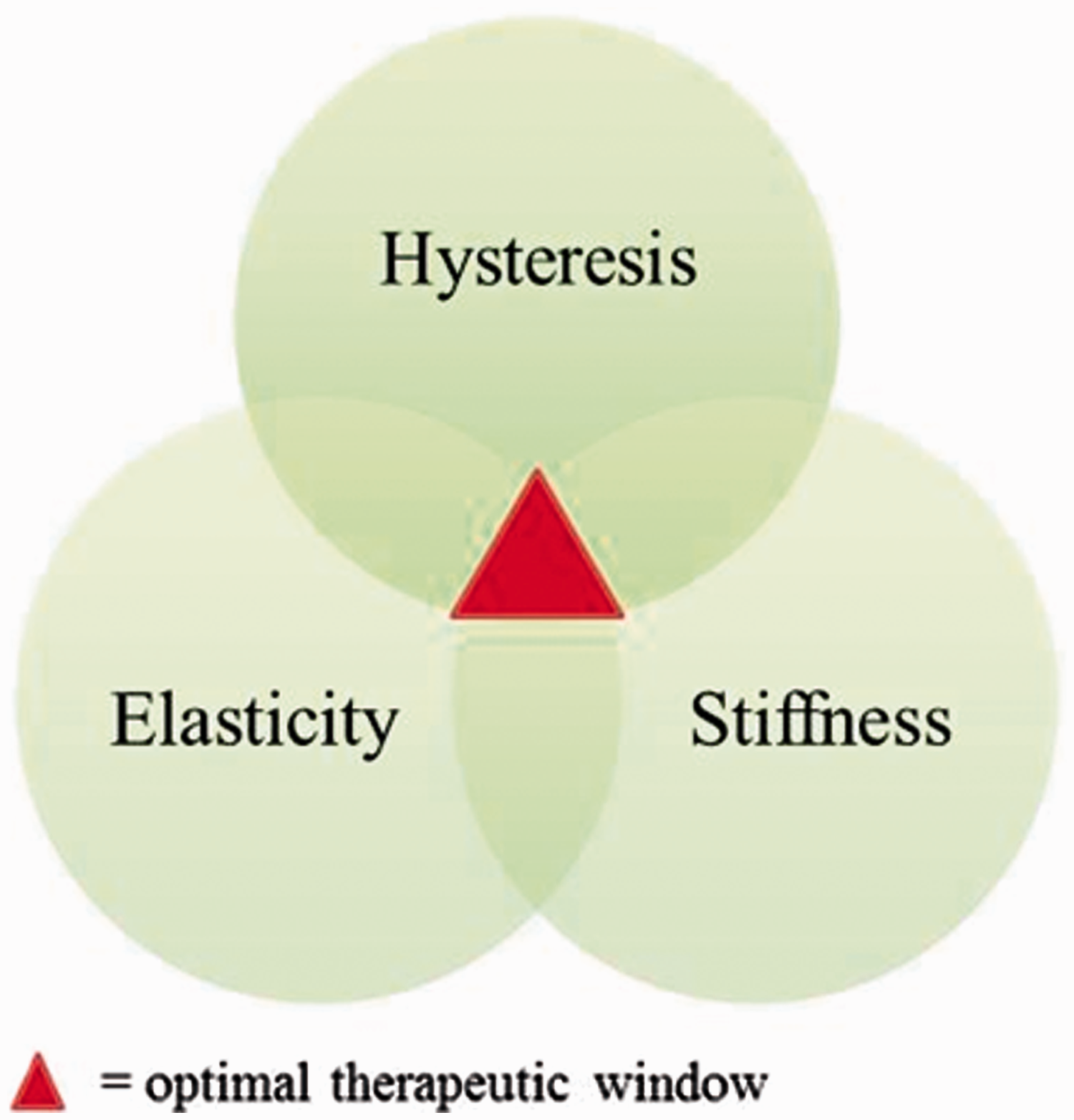
The relation between hysteresis and stiffness is illustrated in Figure 3. This process is speed-dependent. The elongation of the material is only possible if the material is elastic. This brings all three physical characteristics of the compression devices together (Figure 4).
Force- elongation curves of MECS with high and low stiffness. The curves were performed with the same speed of elongation. The area of the graph resembles the hysteresis, whereas the slope resembles stiffness. Relation between elasticity, stiffness and hysteresis.
van der Wegen performed several studies on the effects of DSI of MECS and their behavior. They concluded that MECS belonging to the same static interface pressure had widely ranging stiffness. 14 In addition, it was shown that DSI correlated well with the static stiffness index and the textile density 15 . Based on these findings, they concluded that it is sufficient for the manufacturers to only determine the static stiffness of the MECS. To make sure that the consumers are well informed about the performance of the MECS, both the stiffness and interface pressures should be labeled on the MECS. Further investigations in the field of compression therapy should take the different characteristics of the compression devices into account.
Compression and PTS
To date, two prospective studies and two randomized controlled studies (one trial used a cross-over design) evaluated the effectiveness of MECS in patients with PTS in reducing symptoms. O' Donnell et al. evaluated the venous hemodynamics between eleven limbs with deep venous damage on ascending phlebography and eight control limbs. They found similar amplitudes of the pressure swing between the PTS subjects with MECS and the control subjects. In addition, MECS significantly reduced the maximum systolic pressure during exercise in the PTS subjects, but control levels were not reached. Compression had neither effect on the resting venous pressure nor on the venous return time. 16
Recently, Lattimer et al. conducted a prospective study on the hemodynamic performance of MECS. They randomly assigned 40 limbs with PTS to four different stockings (class I or class II, below or above knee level). The venous filling index (VFI), venous filling time (VFT90) and the venous volume (VV) significantly improved with all four stockings compared with no compression. The extent of improvement correlated with the initial magnitude of reflux, irrespective of the class or length of stocking. However, only 18%–30% of the legs showed a normal VFI with stockings. 17 One has to realize that this study was performed under static conditions. Therefore, the amplitude of the interface pressure, also known as the massaging effect of the MECS, could not be demonstrated. In addition, the results were registered with an air plethysmography that uses a polyurethane pouch which is not calibrated for hysteresis. Therefore, the results of this study are debatable.
The positive hemodynamic effects that were found in the study of Lattimer et al. are not in line with the results of the clinical study of Ginsberg et al. In this study, 35 patients with PTS were equally randomized to MECS with an ankle pressure of 30 to 40 mmHg or to placebo stockings (one or two sizes to large). After three months of follow up, no substantial benefit of MECS in the reduction of symptoms was demonstrated. 18
Kahn et al. found similar results in their crossover study. They evaluated the effect of MECS on symptoms during treadmill exercise between 19 subjects with and 21 subjects without PTS. Most symptoms worsened slightly with exercise, whether or not MECS were worn, and whether or not PTS was present. The leg volume and leg circumference increased with exercise despite the fact that the PTS patients wear stockings. 19
Besides these four studies that evaluated the effect of MECS in patients with PTS, there are two studies that assessed the IPC. The venous velocity response to high pressure, rapid-infiltration compression devices versus standard, low-pressure, slow-infiltration compression devices, was evaluated in the study of Malone et al. 22 healthy limbs and 11 post-thrombotic limbs received five different IPC devices in a random sequence. A five-minute compression time for each device was chosen based on the findings of a preliminary evaluation. Standard and high-pressure rapid-infiltration compression significantly (p<.005) increased the popliteal and femoral vein velocities in healthy (16–37 mm Hg) and PTS patients (13–22 mm Hg). However, the PTS patients had a significantly attenuated velocity response (13–22 mm Hg) to all compression devices when compared to healthy subjects (16–37 mm Hg). 20
Ginsberg et al. randomized 15 patients with severe PTS to a low (15 mm Hg) pressure and changed to a high therapeutic (50 mm Hg) pressure or vice versa after one month. After two months, the placebo group had a mean symptom score of 14 which was significantly lower (p = .0007) than the mean score in the pressure group (17). Finally, 75% of the participants decided to continue the IPC between pressures of 40 and 50 mm Hg. 21
Although the results of Ginsberg et al. are promising, IPC is rarely used because it is time-consuming and expensive. Therefore, O'Donnell et al. evaluated a new portable device ‘Venowave’ that assists the venous return by a wave- form motion on the calf. In this blinded randomized crossover study, 26 patients with PTS received Venowave for eight weeks and a control device for another eight weeks. The mean VEINES-Qol score at the end of the study period was significantly higher (p = .004) for Venowave (53) than for the control device (50). The mean Villalta score was significantly decreased (p = .004) for Venowave (12) compared to the control group (15). 22 Nevertheless, further studies are required to determine the longer-term benefits and safety of Venowave.
There is a paucity of studies that evaluated compression therapy in PTS. In addition, the few existing studies are of poor methodological quality. Clinical studies that evaluate the treatment in PTS should use primary outcome parameters, such as edema (circumference of the leg) and progression of the disease. Unfortunately, there are several studies that report the importance of MECS in deep venous incompetence. For instance, Stolk et al. showed that a high stiffness provides high resting and high-pressure pulses during walking. 12 Therefore, it is more effective in preventing edema, reducing refluxes and improving ambulatory venous hypertension.
The clinical efficacy of compression therapy depends on the stiffness, hysteresis and the elasticity of the bandages. However, when prescribing MECS, not only these characteristics must be taken into consideration, patient's preference is also important.
In our practice, we recommend MECS class II (CEN 23–32 mm Hg) with a high stiffness index for mild-moderate PTS and MECS class III (CEN 34–46 mm Hg) with a high stiffness index for severe PTS. Normally, MECS with a low stiffness are not advised. However, if patients find the MECS constricting, difficult to apply or when severe obstructive PTS is present, a MECS with a lower stiffness can be suggested. In these cases, a MECS with a low stiffness and a high interface pressure can be worn together with a MECS with a high stiffness and a low interface pressure. Patients with severe edema or congestion may have benefit from additional IPC therapy or walking exercises.
In case the saphenous reflux takes a significant share in the total reflux, the physician may consider to treat the saphenous incompetence. 23 However, the correction of saphenous reflux is contraindicated in case of severe deep venous obstruction, because the saphenous veins function as collaterals of the deep venous system.
In our practice, patients with high iliac-femoral obstructions are desobstructed and stented. However, these procedures should be reserved for patients with severe signs and symptoms of PTS. In addition, long-term studies on the effectives of these procedures are lacking.
Footnotes
*
Comité Europé en de Normalisation.