
Abstract
Objectives
There is no data available at present on the changes in the exerted pressure together with the dynamic stiffness index (DSI) of medical elastic compression stockings (MECS). The objective of this pilot study was to measure the pressure and calculate the DSI of 12 different brands of MECS before and after having been worn for eight hours.
Methods
In all, 12 different commercially available brands of MECS that were divided into two categories (class I round-knitted and class II flat-knitted MECS) were tested. The pressure was measured, and the DSI of the MECS was first calculated at the B1 level before wearing in the morning and again eight hours after they had been worn. All laboratory measurements were performed using a newly developed dynamic leg-segment model.
Results
The pressure at the B1 level dropped significantly in all 12 brands of MECS after having been worn for eight hours, whereas the DSI remained unchanged.
Conclusion
The DSI of MECS reflects an important and particularly consistent therapeutic effect. As the pressure drops during the day, the pressure amplitude or pulsations remain the same. The pressure drop may be due to fatigue of the elastic material. The DSI would therefore form a valuable indicator for prescribing the most effective MECS for the patient.
Introduction
The dynamic stiffness index (DSI) of medical elastic compression stockings (MECS) is an important parameter in understanding the efficacy of compression therapy. MECS with a low interface pressure may be more effective than expected only by the pressure they exert. This can be explained by the fact that a high DSI induces high-pressure amplitudes during walking. 1 The effectiveness of ambulatory compression therapy mainly depends on the pressure peaks during walking. Due to these pressure peaks, venous drainage is ameliorated and oedema is reduced. 2–4 Non-ambulatory patients do not have the benefit of the extra effect of compression, such as a high DSI. A well-known observation is the difficulties encountered in the treatment of dependency oedema in patients confined to wheelchair with compression therapy despite the high interface pressure. This can be explained by the absence of pressure peaks because of immobility.
Manufacturers of MECS generally mention the pressure exerted at the ankle (B level), according to the CEN, but the DSI is not mentioned on the package. This lack of information hampers the prescriber in choosing the most effective MECS and in providing the most appropriate information to the patient. The quality of compression therapy is expected to improve when prescribers can base their choice on both the important characteristics of MECS; the interface pressure and the DSI.
It is known from the literature that interface pressure decreases with time. 5–8 For example, the interface pressure underneath short stretch bandage drops by 46% at the B level during the first three hours of wearing and with 37% of the original pressure remaining after seven days. 9 This can be explained by a reduction in oedema and the resulting loosening of the bandage. To our knowledge, no data are available on the behaviour of the DSI or stiffness of MECS over a period of time. The aim of this study was to measure the pressure and calculate the DSI of 12 different commercially available brands of MECS before and after having been worn for eight hours. To clarify, it was not the intention of this study to evaluate the wear-and-tear of MECS after eight hours wear.
Materials and methods
Medical elastic compression stockings
We randomly chose MECS of 12 different commercially available brands. All MECS belonged to compression class II (pressure at the ankle, 23–32 mmHg). All the brands from the various manufacturers are shown in Table 1. They were divided into two categories based on the type of knit: class II round-knitted MECS and class II flat-knitted MECS. In all experiments B1 leg-size of 22 cm was used. The manufacturers were not aware that the MECS were being tested.
Brands and manufacturers of medical elastic compression stockings (MECS)
Measuring point
Measurements were performed at the B1 level, the point at which the Achilles tendon changes into the calf muscles. We chose the B1 level because the results of our previous study showed that the largest differences in the circumference during walking occurred at this level. 10
Measurements
Of the 12 brands of MECS, the static pressure of each MECS was measured twice. The MECS were prepared in accordance with the European Committee of Standardization. 11 Prior to putting on the MECS in the morning, the pressure and the DSI were measured and calculated, respectively. Both these measurements were performed using a new dynamic leg-segment model. Subsequently, the MECS were worn for eight hours during normal daily activity and the measurements were repeated within 10 minutes after taking off the MECS. Each of the MECS was worn by the same investigator (CvdW).
Dynamic leg-segment model
A new dynamic leg-segment model based on a method with an air-filled drum approved by the CEN was developed to investigate the dynamic behaviour of MECS.
10,11
The dynamic leg-segment model simulates the walking speed and walking pattern of the real leg during walking, which denotes the circumferential changes during walking and the amplitude of these changes (Figure 1). The model consists of four components:
A form wheel for simulating walking patterns. The circumference of the leg changes during walking, primarily as a result of the movement of the calf muscles. We previously analysed these movements with regard to the gait cycle, amplitude and form of the signal. For this purpose healthy volunteers walked on a treadmill with mercury-filled rubber gauges around the leg at the B1 level. Changes in circumference were determined using strain-gauge plethysmography. In order to imitate these changes for our model, a form wheel was designed. An air-pressure generator (Figure 1). This air-pressure generator (Posthumus Products, Haarlem, The Netherlands) is connected to the form wheel, can be adjusted for the frequency and amplitude of the signal, and provides the air-filled drum of the artificial leg-segment with precise pressure in such a way that the dynamic variation in circumference of the MECS equals 1 cm. An artificial leg-segment consisting of an air-filled drum covered with a rubber skin (Figure 2). We used an air-filled drum with the same circumference as the leg-circumference at the B1 level (22 cm). The MECS is put over the leg-segment. The air-filled drum is connected with a TruWave pressure-transducer (Baxter Healthcare Corporation, Irvine, CA, USA) to determine the air-pressure in the drum and, thus, the pressure exerted by the MECS. Changes in the circumference are registered with strain-gauge plethysmography. The pressure and the changes in circumference were measured simultaneously and entered into a computer system: the Fysio Flex system, built at the instrumentation service unit of the University of Nijmegen, The Netherlands. A registration curve of a dynamic measurement is shown in Figure 3.

Measuring instrument with the dynamic leg-segment model. Inset: Adjustable air pressure generator
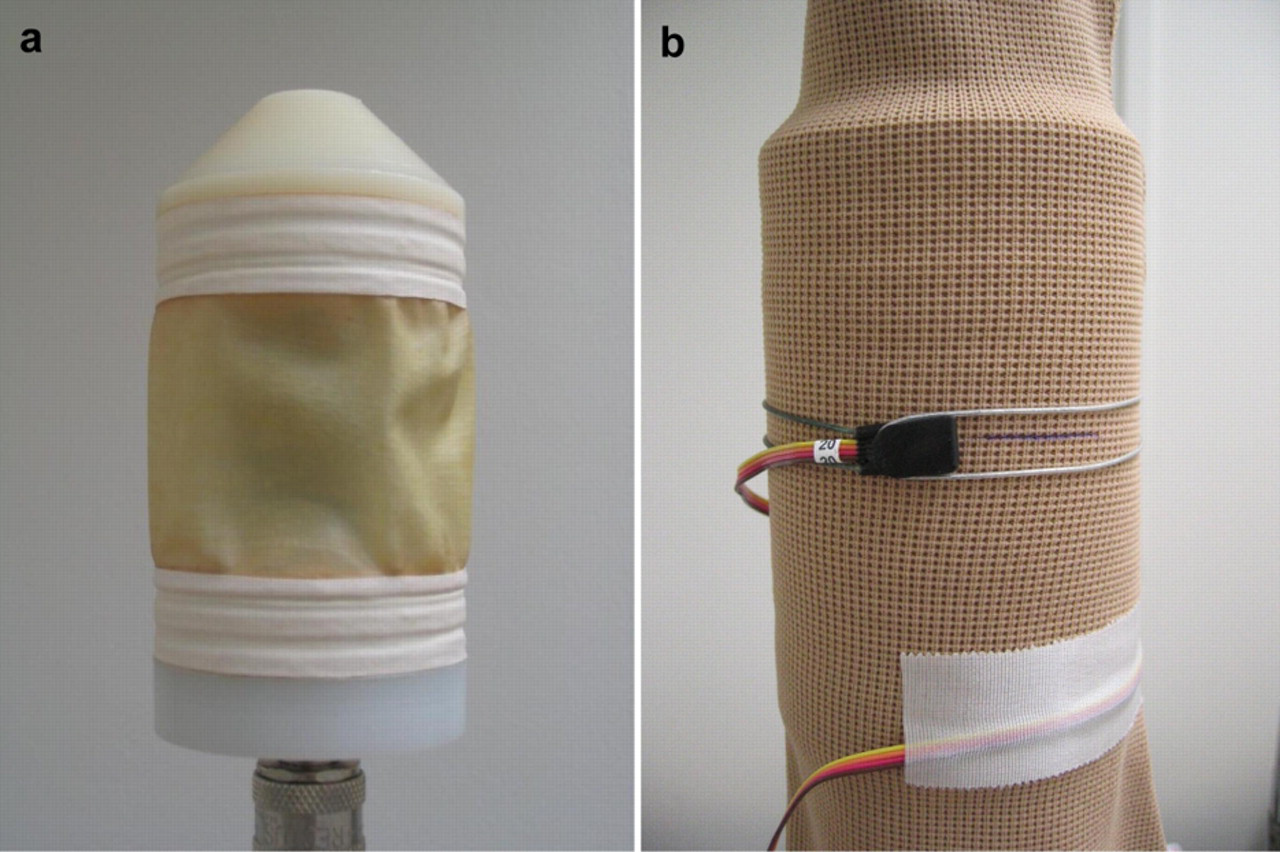
Artificial leg-segment model without (a) and with (b) medical elastic compression stockings (MECS). The dynamic changes of the MECS are determined with strain-gauge plethysmography

Registration curve of a dynamic measurement. The upper signal represents the circumference variation. The amplitude of this signal equals 1 cm. The lower signal represents the pressure variation in the air-filled drum
Dynamic stiffness index
A new definition for DSI, based on the current definition of stiffness as mentioned by the CEN, is introduced. DSI (mmHg/cm measured at 1 Hz) is defined as the increase in pressure when the variation of circumference equals 1 cm at a frequency of 1 Hz (equals one gait cycle per second).
DSI was then calculated. The variation in the DSI was 4% based on repeating the DSI measurement of the same MECS on 10 consecutive days.
Statistics
To test for statistically significant differences in the continuous pressure and DSI data, a paired Student's t-test was used. A two-sided P value <0.05 was considered as significant. SPSS software 12.0.1 for Windows was used. To assess the variability of the pressure and DSI measurements, one MECS was measured 10 times on 10 consecutive days to determine the variation in both measurements.
Results
Pressure at the B1 level
According to the CEN, the exerted pressure at the B level for a class II MECS ranges from 23–32 mmHg. With regard to the pressure profile, the CEN defines residual pressure at the B1 level as 70–100% compression at the ankle. 11 This means that the value for class II MECS varies from 16 mmHg to 32 mmHg.
Of the 12 MECS studied, four MECS did not fulfil the CEN criteria of a class II MECS (one stocking was <70% of 23 mmHg and three MECS showed pressures above 32 mmHg; Table 2 and Figure 4). A statistically significant decrease in the pressure exerted by the MECS was noted after having been worn for eight hours (mean 26.4 mmHg [SD 7.8] versus 20.9 mmHg [SD 8.0]; P < 0.0001). All MECS showed a pressure decrease after eight hours wear. The majority of the MECS (8/12) demonstrated a loss of 20% or more of pressure measured prior to use. Of the eight MECS that were eligible for class II stockings, four MECS demonstrated pressures below 18.4 mmHg after having been worn for eight hours. Two out of three MECS that showed high initial pressures were considered to show pressures within the limits of class II stockings. The variation in the pressure of the Mediven Plus was 4% (mean 20.52 [SD 0.91]).
Pressures at B1 level of 12 different brands of class II medical elastic compression stockings (MECS) measured in the morning and after having been worn for eight hours

Change in pressure of 12 different brands of class II medical elastic compression stockings after having been worn for eight hours. The shaded area in the graph shows the pressure range of a class II MECS according to the CEN at the B1 level
Dynamic stiffness index
There was no significant difference between the DSI of MECS before and after having been worn for eight hours (mean 20.4 [SD 4.5] vs. 21.0 [SD 5.7]; P = 0.31) (Table 3 and Figure 5). The mean difference in change in DSI is 0.54 [SD 1.74] and 9/12 showed <5% change after eight hours wear. The variation in the calculated DSI of the Mediven Plus was 4% (mean 17.3 [SD 0.65]). Although, there was a wide variation in the DSI of the round-knitted MECS as well as the flat-knitted MECS, the mean DSI of the flat-knitted MECS was higher than the mean DSI of the round-knitted MECS (mean 18.6 [SD 5.0] versus 22.2 [SD 3.5] in the morning and mean 19.6 [SD 7.0] versus 22.3 [SD 4.4] after eight hours).
Dynamic stiffness index of 12 different brands class II medical elastic compression stockings (MECS) calculated in the morning and after eight hours
*Measured at a frequency of 1 Hz
† The variability of the DSI measurement was 4%. This was determined by measuring one brand of MECS 10 times on 10 consecutive days
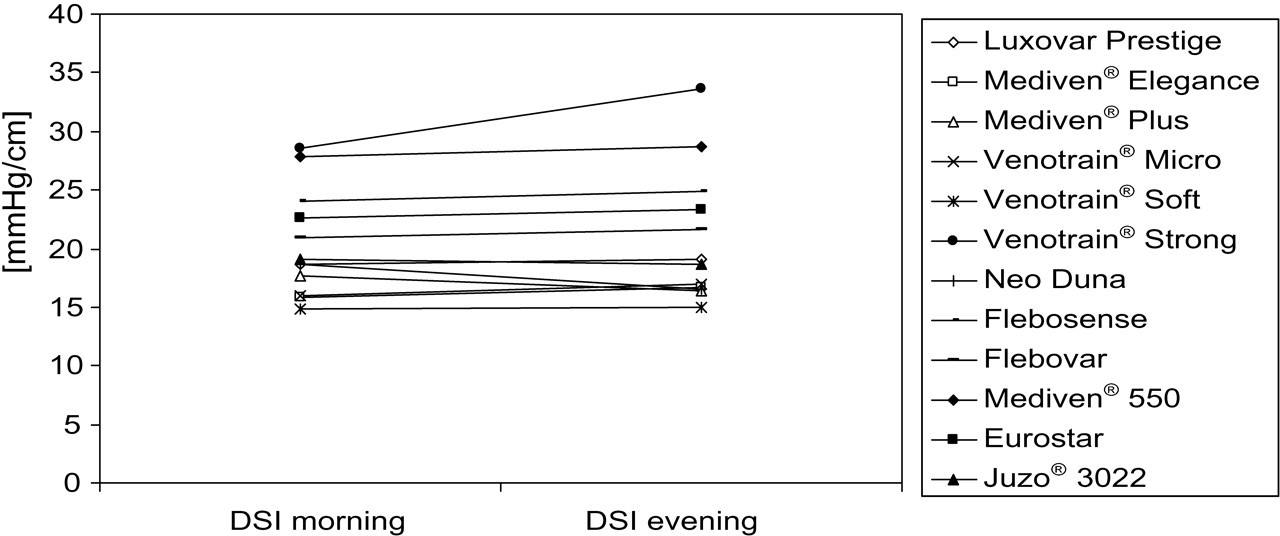
Change in dynamic stiffness index of 12 different brands of class II medical elastic compression stockings after having been worn for eight hours
Discussion
MECS are designed to be worn during the daytime and especially during walking. They are most effective in combination with motion. The combination of compression and walking is known as ‘ambulatory compression therapy’. Ibegbuna et al. were the first authors who studied the haemodynamic effects of elastic compression during walking on a treadmill using air-plethysmography in order to reflect more accurately the daily physiological conditions. 12 They showed that MECS significantly improved venous haemodynamics in patients with chronic venous insufficiency at different walking speeds.
Previous studies reported that the interface pressure under compression bandages decreased in time. 7 In recent years, more information on the influence of stiffness with regard to compression therapy has become available. The stiffness of MECS is responsible for pressure changes during walking. The higher the stiffness, the higher the pressure-amplitude. 10 This so-called massaging effect due to these pressure pulsations is extremely important in the treatment of leg oedema, for blocking reflux and in reducing ambulatory venous hypertension. In the study by Partsch et al., 13 stiffness was measured in vivo to assess the elasticity of compression material. A clear distinction was shown between elastic, long stretch material and inelastic, short-stretch material. Inelastic bandages showed higher pressure peaks compared with elastic bandages and stockings. This means that the massaging effect for inelastic bandages is higher. In the present study only MECS were used to measure pressure and calculate the DSI.
Treatment or prevention of leg oedema is considered to be the main aim of compression therapy in venous diseases. MECS with a high DSI are more effective in the treatment of venous diseases than those with a low DSI. 2–4
To our knowledge, unlike studies on interface pressure, there are no reported studies in the literature on the changes in DSI of MECS after they have been worn for a period of time. It was the objective of this study, to assess the change(s) in the characteristics of MECS and not to determine the wear-and-tear of MECS after eight hours wear. We are aware that the elastic material of the MECS may return to the baseline (as is the case before wearing the MECS) after relaxation of the knit.
The results of the present pilot study showed that the pressure of all tested MECS had dropped significantly after having been worn for eight hours. Moreover, it has to be remarked that only one stocking per brand was measured. This was based on the results of our previous studies in which the same brands of MECS were investigated. 1 However, it is noticeable that eight of the 12 brands of MECS do not fulfil the criteria of a class II stocking at a certain point during the day. What does this mean in daily practice? In our opinion it is not the pressure but the pressure pulsations created by the stiffness of the MECS that is important. In contrast to the pressure alterations, the changes in DSI are not significant and are likely to be due to the variation in the measurement. This is also confirmed by the observation that the changes in DSI were noted to be either positive or negative. Interestingly, there were no differences between the round-knitted and the flat-knitted MECS as far as the change in DSI was concerned. We can explain the pressure drop on the basis of fatigue of the elastic materials. Since stiffness is a characteristic of all the materials and particularly of elastic materials, its role can best be explained as the result of internal friction between the threads, stitches and the resistance against deformation. Since neither friction nor resistance is related to elasticity, stiffness will not alter during the eight hours of wear (day).
This information on the stiffness of MECS is essential in daily practice. A correct combination of interface pressure, as indicated by the CEN compression classes and the DSI is essential for prescribing optimal ambulatory compression therapy with MECS. On the one hand, MECS with low DSI will not only lose the pressure they exert during daytime, but will also have a low walking pressure-amplitude. Patients who wear such MECS have a risk of developing oedema during the day. Formation of oedema is related to the severity of venous insufficiency. On the other hand, MECS with a medium pressure and high stiffness are perfectly able to prevent oedema because of the high pressure amplitudes during walking.
The results reported here clearly shows that the DSI is highly important for sufficient compression during daytime. The natural decrease in interface pressure can be compensated with an appropriate DSI. An example of this is shown in Figure 6. Although the pressure drops at the and of the day below the minimum pressure allowed at the B1 level of a class II stocking, under ambulatory conditions, the pressure pulsations provide adequate pressures during most part of the day. Therefore, we recommend prescribing MECS with a high DSI and high pressure to all patients with a strong tendency towards the formation of oedema and in whom a constant high pressure is necessary, for instance in patients suffering from a post-thrombotic syndrome. In patients with mild venous problems, such as patients suffering from mild venous symptoms (C0–C1), prescription of MECS with a lower DSI and lower pressure will be sufficient. Thus, a physician can choose an appropriate MECS by choosing a higher stiffness for treating severe chronic venous insufficiency, without increasing the pressure. Further well-designed clinical studies are warranted to establish whether this in fact is the case.
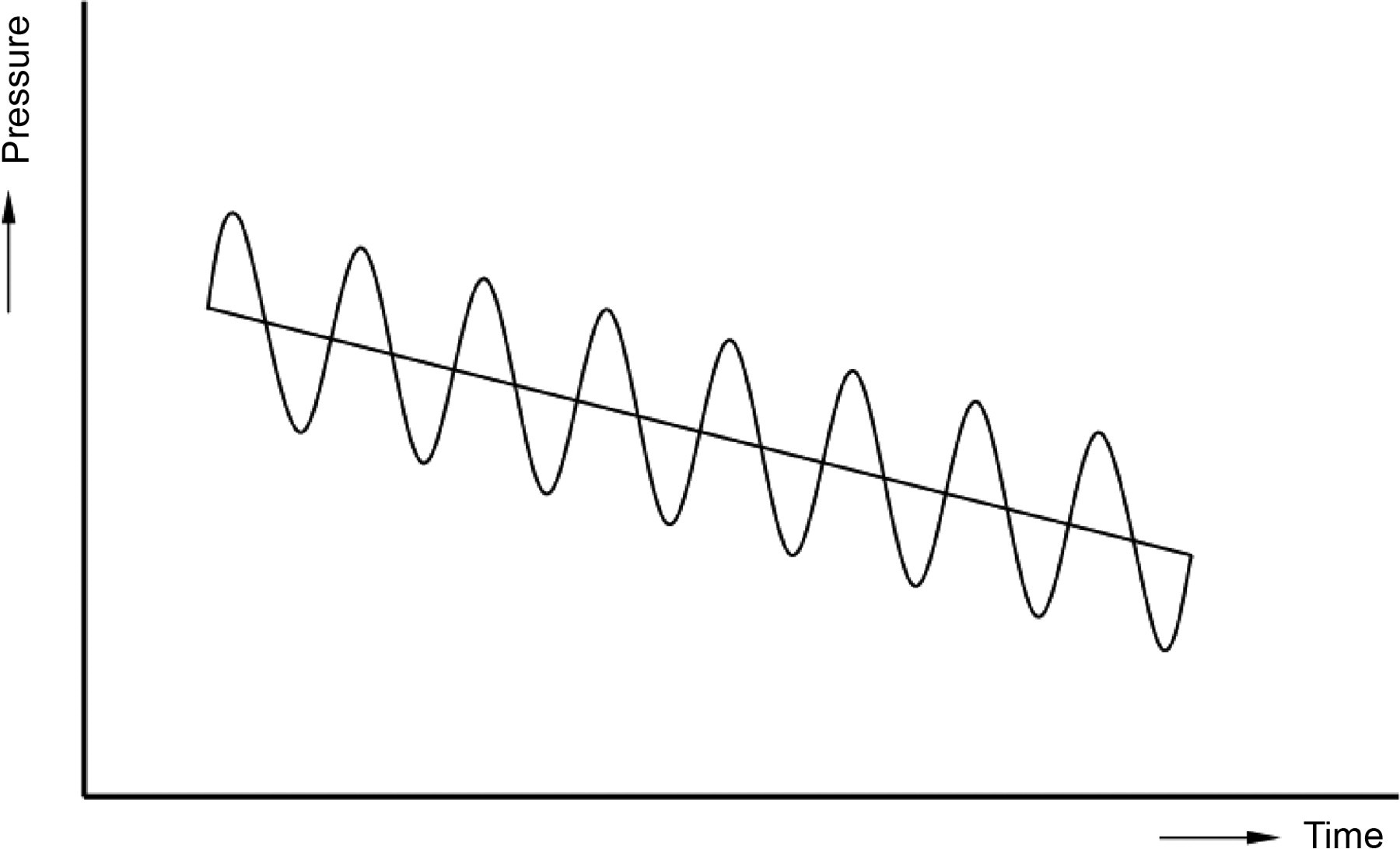
Example of a stocking that shows a decrease in pressure and continuous pressure pulsations (dynamic stiffness index) during the day