
Abstract
Abstract
Objectives
To calculate the dynamic stiffness index (DSI) of 18 different brands of medical elastic compression stockings (MECS).
Methods
In all, 18 different brands of MECS that were divided into five categories (class II round-knitted, class II flat-knitted, class III round-knitted, class III flat-knitted and class IV flat-knitted MECS) were tested. The static pressure and dynamic pressure pulsations at the B1 level were measured with a newly developed dynamic pressure-determining device. The DSI was calculated.
Results
The DSI of all 18 brands of MECS showed higher values compared with the static stiffness. A wide range of dynamic stiffness indices was observed not only between all brands of MECS, but also within the five categories.
Conclusions
The DSI of MECS is independent of the compression class and the type of knit. The variation in the DSIs between MECS is not because of any measurement error and would indicate that different therapeutic effectiveness may be expected within one compression class. Therefore, a refinement in the current classification system for MECS with other characteristics such as the DSI is warranted.
Keywords
Introduction
Medical elastic compression stockings (MECS) have been used to treat venous disorders since the granting of the patent number 12294 to William Brown on 26 October 1848, the day which has been regarded as the birthday of the ‘rubber’ stocking. 1 From that day on lots of different types of MECS have been developed leading up to the MECS as we know them today. One of the important clinical applications of MECS is the prevention of oedema. This is achieved by the physical characteristics of the materials used in the manufacture of MECS. Three main characteristics of MECS are important for their effectiveness: elasticity, stiffness and hysteresis. Hysteresis is due to internal friction between the stitches and is defined as the loss in recovered linear length of an elastic product after it has been subjected to repeated stretching and relaxation. 2 Pressure is exerted on the leg because of the elasticity of MECS. The pressure is related to the extension of the MECS. When the circumference increases, as during walking or oedema formation, the pressure will also increase. This phenomenon is known as stiffness which is medically important. 3 The stiffness, which is also known as slope or elasticity coefficient, is defined according to the European Committee of Normalization (CEN), as the increase in pressure at the B level, if the circumference increases by 1 cm. 4 Stiffness of MECS not only plays a role in oedema prevention, but was also reported to affect the venous haemodynamics particularly in dynamic condition. 5,6 The higher the stiffness, the better the oedema preventive effect. To date, this parameter is measured under semi-static conditions in a laboratory. Different devices and methods are used to determine the stiffness and in general are as follows: the MECS is positioned in a relaxed condition and is then elongated/stretched to the circumference of the B level. This procedure is repeated several times and the stretching increased by 1 cm. The difference in force required to elongate the MECS is used to calculate the stiffness. We recently published the widely ranging static stiffness of nine different brands of class II MECS, and concluded the static stiffness is an additional important characteristic for distinguishing between MECS from different brands. 7 However, the static stiffness does not reflect the dynamic condition, and the differences between the therapeutic effectiveness of MECS belonging to the same compression class cannot be explained on the basis of static stiffness alone. Compression therapy is mainly effective during walking and MECS behave differently under dynamic conditions as illustrated in Figure 1. As already mentioned, under static conditions MECS are relaxed (0% elongation) and then stretched to a certain extent. In reality, MECS are not relaxed on the leg and changes in circumference or percentage of stretch are much less than in a laboratory setting. As is shown in Figure 1, the smaller the change in circumference, the steeper the slope. The slope represents the stiffness. We assumed that during walking, because of the smaller changes in circumference, the dynamic stiffness index (DSI) would be higher.

Static and dynamic force elongation curves of MECS. The slope of the curve resembles the stiffness. (a) Under semi-static conditions the MECS is elongated from a state of total relaxation to the stretch that is required at the B1 level. (b) Under dynamic conditions as during walking the circumference changes of the leg are small. This curve shows the smaller the elongation increments, the steeper the curve meaning a higher dynamic stiffness index
Thereby, we expected the differences between the DSI of the different brands of MECS larger compared with the differences we found earlier between the static stiffness. 7 A variety in therapeutic effectiveness can be expected on the basis of the differences between the DSI, which is very important in selecting the most suitable MECS for the patient.
The aim of the study was to calculate the dynamic stiffness of 18 different brands of MECS belonging to three different compression classes.
Materials and methods
Medical elastic compression stockings
We arbitrarily chose MECS of 18 different brands, 11 brands belonging to compression class II, five brands belonging to compression class III and two brands belonging to class IV. All brands from various manufacturers, as shown in Table 1, were divided into five categories based on the type of the knit: class II round-knitted MECS; class II flat-knitted MECS; class III round-knitted MECS; class III flat-knitted MECS; and class IV flat-knitted MECS. There was no specific reason for choosing different numbers in the three compression classes. Generally, there is more choice in class II and class III MECS. In all experiments B1 leg-size of 22 cm was used. The manufacturers were not aware that the MECS were being tested.
Brands and manufacturers of medical elastic compression stockings (MECS)
Test procedure
Before testing, all MECS were washed according to the European guidelines, followed by hydro-extraction (maximum for 2 min) and flat drying. The MECS were conditioned at least 12 h prior to the measurements.
Measuring point
Measurements were performed at the B1 level; this is the point at which the Achilles tendon changes into the calf muscles. We chose the B1 level because the results of our earlier study showed that the largest differences in the circumference during walking occurred at this level. 8 The results reported in that study corroborate those reported by Blättler et al. 9 A device was used to mark the measuring positions. This consisted of a marking-board on which an adjustable clamp was mounted. This clamp enabled to fix the lower end of the round-knitted MECS to a system of clamps, or for flat-knitted MECS to a metal foot frame. The device is shown in Figure 2.

Device for marking the measuring points according to the CEN. In this case a round-knitted MECS is clamped
Dynamic leg-segment model
The new dynamic leg-segment model was described in details elsewhere, but the method is discussed briefly.
8
An artificial leg-segment model based on an air-filled drum was developed to investigate the dynamic behaviour of MECS.
10
The dynamic leg-segment model simulates the walking speed and walking pattern of the real leg during walking and consists of four components:
A form wheel for simulating walking patterns. The circumference of the leg changes during walking, primarily as a result of the movement of the calf muscles; An air-pressure generator (Figure 3). This air-pressure generator (Posthumus Products, Haarlem, the Netherlands) is connected to the form wheel, can be adjusted for the frequency and the amplitude of the signal and provides the air-filled drum of the artificial leg-segment with precise pressure in such a way that the dynamic variation in circumference of the MECS equals 1 cm; An artificial leg-segment consisting of an air-filled drum covered with a rubber skin (Figure 4). We used an air-filled drum with the same circumference as the leg-circumference at the B1 level. The MECS is put over the leg-segment. Changes in the circumference are registered with strain-gauge plethysmography. The pressure in the air-filled drum was recorded with a TruWave pressure-transducer (Baxter Healthcare Corporation, Irvine, CA, USA).
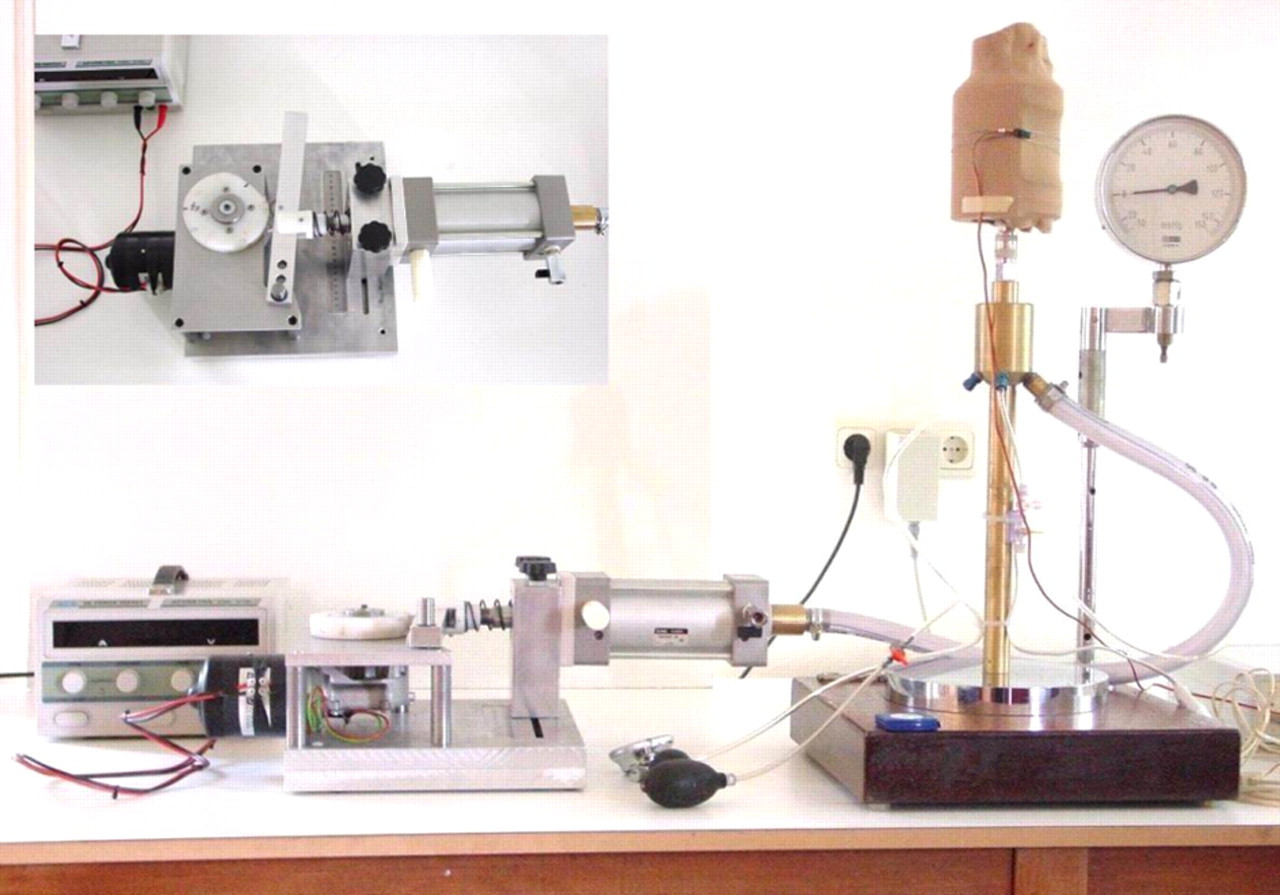
Measuring instrument with the dynamic leg-segment model. Inset: adjustable air pressure generator

Artificial leg-segment model without (a) and with (b) MECS. The dynamic changes of the MECS are determined with strain-gauge plethysmography
The pressure and the changes in circumference were measured simultaneously and fed into a computer system: the Fysio Flex system, built at the instrumentation service unit of the University of Nijmegen, The Netherlands. A registration curve of a dynamic measurement is shown in Figure 5.
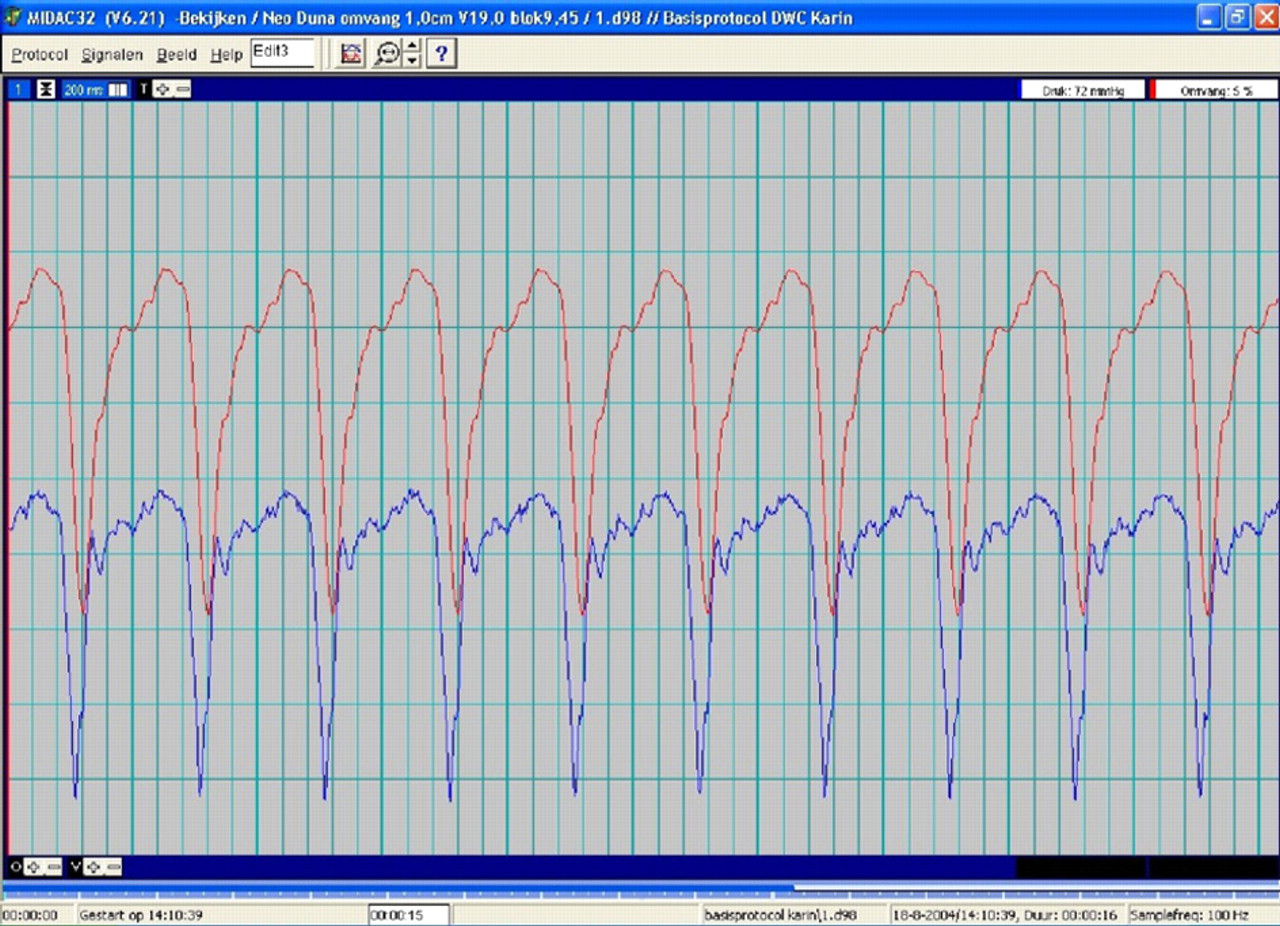
Registration curve of a dynamic measurement. The red signal represents the circumference variation. The amplitude of this signal equals 1 cm. The blue signal represents the pressure variation in the air-filled drum
Dynamic stiffness
A new definition for DSI, based on the current definition of stiffness as mentioned by the CEN, is introduced. DSI is defined as the increase in pressure when the variation of circumference equals to 1 cm at a frequency of 1 Hz* (mmHg/cm measured at 1 Hz).
The DSI was then calculated.
*1 Hz = 1 gait cycle/s. Three repeated measurements were conducted per MECS.
Statistics
The mean pressure with standard deviation (SD) and DSI with SD were calculated from these three replicate measurements per brand of MECS.
A components of variance analysis was used to judge the reliability and the reproducibility of the DSI. The reliability (Rel) of the measurements was calculated using the following formula:
Results
Pressure at the B1 level
According to the CEN, the exerted pressure at the B level for a class II MECS ranges from 23 to 32 mmHg, for a class III MECS from 34 to 46 mmHg, and for a class IV MECS 49 mmHg and higher. These values indicate a hypothetical cylindrical ankle of 20 cm. With regard to the pressure profile, the CEN defines a residual pressure at the B1 level as 70 to 100% compression at the ankle. 4 This means that the value for class II MECS varies from 16 to 32 mmHg, for class III MECS from 24 to 46 mmHg, and for class IV MECS 34 mmHg and higher. The mean pressure and the SDs of the 18 brands of MECS at the B1 level are shown in Table 2. It can be seen that almost all, but the class III Mediven® Forte stocking, exert pressures within the accepted range. The overall tendency in both class II and III MECS is that flat-knitted MECS exerted higher pressures compared with round-knitted MECS. Furthermore, it is notable that three class II MECS (Neo Duna, Juzo® 3022 and Juzo® 3052) exerted pressures, which are similar to those exerted by several class III MECS.
Mean pressures at B1 level of 18 different brands of medical elastic compression stockings (MECS)
*Figures are the means ± SD calculated from three replicate measurements per brand.
Dynamic stiffness index
The mean DSI and SDs of 18 different brands of MECS are shown in Table 3 and a graphical representation is shown in Figure 6. It can be seen in Figure 6 that there is a large variation in DSI irrespective of the compression class or the type of knit. The DSI in the 11 different brands of class II MECS ranged from 16.1 ± 0.27 mmHg (Venotrain® Soft) to 32.2 ± 1.19 mmHg (Mediven® 550). The DSI in the five different brands of class III MECS ranged from 19.1 ± 0.53 (Luxovar Prestige) to 30.0 ± 0.92 mmHg (mediven® 550). The DSI in the two brands of class IV MECS ranged from 22.2 ± 0.59 (Neo Durelna Speciaal) to 26.0 ± 0.59 (Euroform Speciaal). The variation in the range of DSI in the five categories of MECS is shown in Table 4. Although there is a large variation in all five categories of MECS, it can be seen that the SDs in the two categories of class II and class III flat-knitted MECS are higher compared with the other groups. Results of the statistical analysis showed that the reliability index was high for all five categories of MECS and the reproducibility of the measurements was excellent (Table 4).
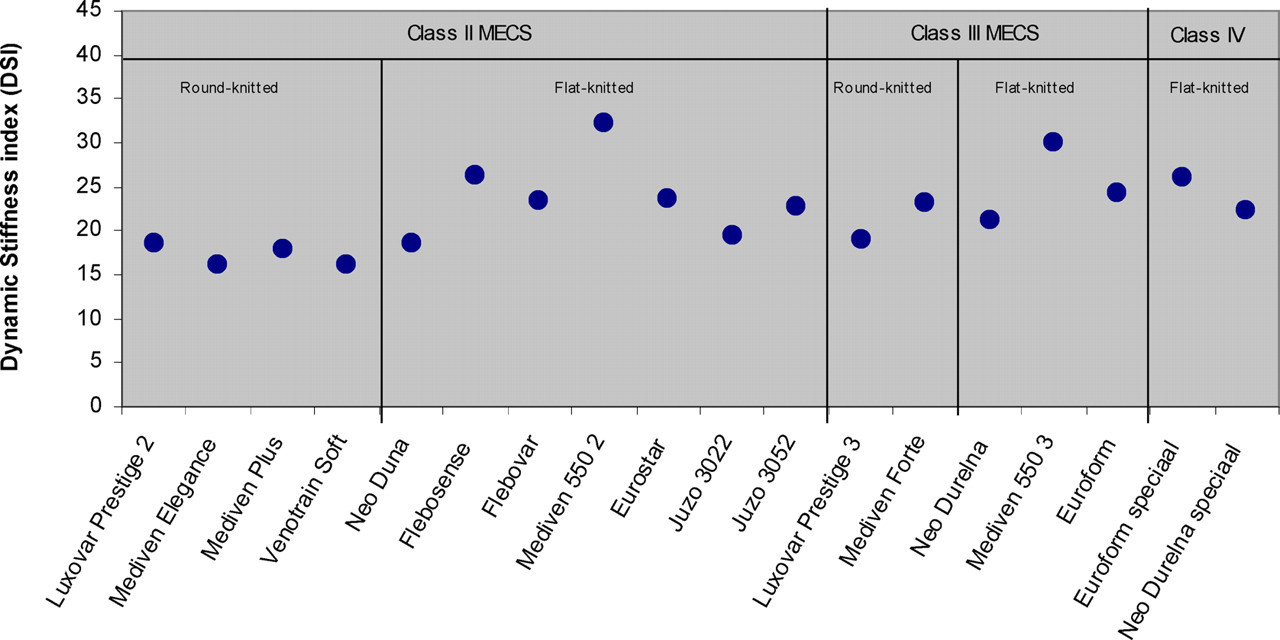
Distribution of dynamic stiffness index of 18 different brands of class II, class III MECS. Each dot represents one MECS
Mean dynamic stiffness index of 18 different brands of medical elastic compression stockings (MECS)
The dynamic stiffness index was calculated as follows: DSI = Δp/Δo (where Δp is the change in pressure and Δo the difference in circumference (equals 1 cm) at a frequency of 1 Hz
*Figures are the means ± SD calculated from three replicate measurements per brand
Variation in the range of dynamic stiffness index (DSI) of 18 different brands of medical elastic compression stockings (MECS) with reliability and reproducibility of the measurements
*SD of a single measurement of DSI
†95th percentile of the absolute difference between duplicate measurements
Discussion
We recently introduced a new parameter for MECS, the DSI and showed that the values of DSI were much higher than those of the static stiffness. 8 In addition, the results of the present study showed that there was considerable variation in the DSIs between various brands of MECS and within the five categories, irrespective of the compression class and type of knit (round-knitted or flat-knitted). Does this large variation in the DSIs of MECS belonging to the same compression class explain the differences in their therapeutic effectiveness? The results of our investigations reported here would indicate that the answer is yes and that the differences between DSIs are as important if not more important than the differences between the compression classes, which would vary according to the clinical indication. Häfner and Jünger showed in their randomized study that MECS of the same compression class do have different acute effects on venous haemodynamics. 11 The explanation for these different effects was the stiffness, which was defined as the ratio between maximum pressure exerted during exercise and the resting pressure when standing. A positive correlation between this ratio and the improvement in venous refilling time was found. However, the current differences between MECS of the same compression class cannot be explained on the basis of static stiffness, because these differences are within the tolerance limits of manufacturing. Perhaps, the DSI would enable a more accurate classification for MECS. Generally, MECS may be divided into four categories according to their DSI: (a) MECS with low compression and low DSI; (b) MECS with low compression and high DSI; (c) MECS with high compression and low DSI and (d) MECS with high compression and high DSI as shown by the four different types of registration curves in Figure 7. Each category has its own specific medical indication for treating venous disorders. 12 In general, the choice for a certain MECS is only based on the compression class. Adding the DSI to the compression class may allow a wider choice of MECS for the particular clinical indication of the patient. For example, for a deep venous reflux, a class III MECS is generally prescribed. However, there are patients with deep venous reflux who will have the same beneficial effect from a class II MECS with high stiffness as compared with a class III MECS with medium or even low stiffness. Moreover, MECS of a lower compression class are generally more appreciated by the patient. MECS that are acceptable to the patient should have a correct balance between comfort and effectiveness. On the one hand, the higher the stiffness of the MECS, the more they resemble inelastic material and the more effective they are in preventing oedema, decreasing venous refluxes and improving calf muscle pump function. 5,6 On the other hand, they are less patient friendly because they are more difficult to put on and pull off.
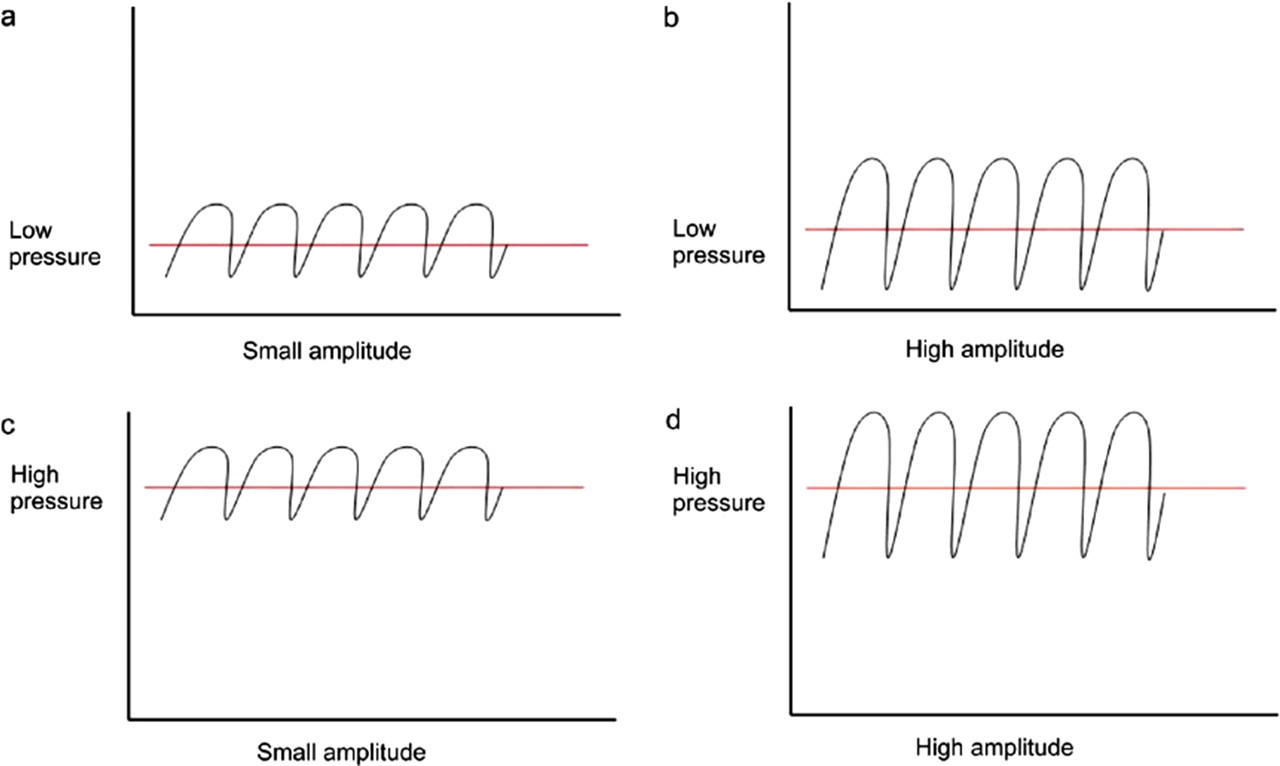
Four types of registration curves: (a) MECS with low compression and low DSI; (b) MECS with low compression and high DSI; (c) MECS with high compression and low DST; (d) MECS with high compression and high DSI
However, the question still remains whether the exertion of high pressure is necessary or will exertion of lower pressure be sufficient to achieve the desired therapeutic effect? The compression class of MECS has proven to be important in the prevention of recurrence of venous ulceration. 13 Moreover, it is known from studies on compression bandages that the so-called massaging effect, which is directly related to the elasticity and the stiffness, is important for optimizing venous return. 6,14 The massaging effect will increase and the effectiveness of MECS will improve by increasing the pressure and the stiffness. We have developed an in vitro method, which simulates the behaviour of MECS during walking as closely as possible. However, we do realize that the method is time-consuming and not easy to implement in daily practice. Nonetheless, the manufacturers can easily conduct such measurements. Advantages of the dynamic leg-segment model are that the model is based on a method that was approved by the CEN. Measurements can be easily adjusted with regard to the frequency, changes in circumference and amplitude. Pressure is measured under the MECS within the air-filled drum and the pressure-sensor remains unaffected. In contrast, pressure-sensors used for interface pressure measurements (this is the pressure between the MECS and the skin) are affected by test location, interface conditions and anatomic leg shape. Liu et al. investigated the objective skin pressure distribution of MECS and reported on the various factors that influenced the skin pressure. 15
The leg-segment model used in the present study is an air-filled closed system. Since air can be compressed, measurements should be conducted under standardized conditions. Nonetheless, the leg-segment model still requires further refinements and validation for routine use. At present, the pressure cannot be read directly. Partsch recently introduced a simple in vivo method to assess the static stiffness index (SSI), which is defined as the pressure difference between active standing and lying. 16 However, pressure differences were divided by 1 cm for reasons of simplicity, assuming that the increase in the circumference was 1 cm. Unlike the calculation reported by Partsch, we conducted our measurements with an actual increase in circumference of 1 cm. In our opinion the change in circumference is very important because a small increase in circumference results in higher stiffness (Figure 1). Our measurements were in vitro. However, it would be desirable also to conduct such measurements in vivo in order to be able to compare such measurements with those reported in other studies. Mosti and Mattaliano studied simultaneous changes of leg circumference and interface pressure under compression bandages in vivo. 17 They used the modified SSI as the pressure difference between the standing and the lying condition corrected for the actual increase of leg circumference. In a recent study by Partsch et al., it was clearly shown that in vivo measurements of the interface pressure and the SSI correlated well with in vitro laboratory measurements of static stiffness. 18 Benigni et al. proposed to define a DSI as the difference between the high and the low pressures recorded during walking. 19 Measurements were performed on a treadmill using a pressure transducer with two sensors. The measured interface pressures were the mean pressures of both sensors. However, they did not take into consideration the change in circumference during walking and measurements were not conducted at the B1 level. This meant that the results of their study could not be compared with those reported in other studies.
There is little or no evidence-based literature for evaluating the role of stiffness of MECS in patients with chronic venous insufficiency. The reported clinical trials were of poor design and confusing. The compression that was used was often not clearly defined, which made the comparison of results difficult if not impossible. As a direct result, considerable interest has arisen in the physical properties of MECS and their relationship with the therapeutic effectiveness. In our opinion, it is essential to pursue well-designed clinical trials and investigations concerning MECS and compression therapy in general. Insight into the differences between the different types of MECS that are commercially available is required in order to develop or refine a more accurate classification that would clearly reflect the therapeutic effectiveness of MECS for treating chronic venous insufficiency.
Acknowledgements
We would like to thank Mr R Stolk at the Research and Development Department, Varitex NV and Mr R Bot, of Varitex NV in Haarlem, for their contribution.