
Abstract
Objective
We aimed to determine the incidence of and associated risk factors for endovenous heat-induced thrombosis (EHIT) after endovenous radiofrequency ablation (RFA).
Methods
We retrospectively reviewed the medical records of 82 patients with 97 great saphenous veins undergoing RFA from 2012 to 2014.
Results
The incidence of EHIT was 10.3%. Class 1, 2, and 3 EHIT was found in 50%, 30%, and 20% of legs, respectively. No class 4 EHIT, deep vein thrombosis, or pulmonary emboli occurred. Univariate analysis revealed that the associated risk factors for EHIT were a vein diameter of >10 mm, operative time of >40 min, and Caprini score of >6. Multivariate analysis revealed that the independent risk factors associated with EHIT were a vein diameter of >10 mm and operative time of >40 min.
Conclusions
A vein diameter of >10 mm and operative time of >40 min might be predictive factors for EHIT following RFA.
Keywords
Introduction
Endovenous thermal ablation has been shown to be effective for the treatment of superficial venous reflux.1,2 Endovenous radiofrequency ablation (RFA) and endovenous laser ablation have become the first-choice treatments for valvular reflux of the great saphenous vein (GSV) and have almost replaced high ligation and venous stripping.3–5 Deep venous thrombosis is a known complication of endovenous ablation ranging from 0% to 16%.6,7 Male gender, larger vein diameter, increased severity of venous disease, increased Caprini risk assessment score, and obesity were identified as risk factors for EHIT.6,7 Thrombus formation may occur from a proximal GSV into the common femoral vein following GSV thermal ablation; this phenomenon is termed endovenous heat-induced thrombosis (EHIT).6,7 EHIT was classified by Kabnick et al.
8
based on the extent of propagation into the deep venous system. According to Kabnick et al.,
8
EHIT is categorized as class 1 to 4. Class 1 is defined as a thrombus that extends to the SFJ, class 2 is defined as extension into the venous system with a cross-sectional area of <50%, class 3 is defined as femoral vein extension of >50%, and class 4 is defined as occlusion of the femoral vein (Figure 1). Class 1 EHIT is regarded as a benign condition because it does not propagate into the deep veins. Class 2 and 3 EHIT are clinically significant because they may lead to deep vein thrombosis (DVT); however, the effects of treatment with anticoagulation therapy, treatment duration, and treatment outcome have yet to be clearly defined. Class 4 EHIT is a form of DVT that requires treatment with an anticoagulant.6,8 The objective of this study was to identify the incidence of, possible risk factors for, and treatment and outcomes of EHIT after RFA.
Endovenous heat-induced thrombosis (EHIT) classification.
Methods
A retrospective review of patients with GSV incompetence treated by endovenous RFA was performed over a 2-year period from 1 July 2012 to 31 August 2014. This research is a retrospective of cohort data. All RFA procedures were recorded into a protocol form. All patients had undergone duplex ultrasound scanning (DUS) prior to GSV ablation. Evaluation of the lower limb veins was performed using a GE LOGIC 9 system (GE Healthcare, USA) using 5 to 10 MHz linear transducers. GSV reflux was defined as retrograde flow of >0.5 s. Ablation of the GSV was performed using a VNUS ClosureFast catheter (VNUS Medical Technologies/Covidien, Mansfield, MA, USA). Our RFA technique has been previously described. 5 Venous access was obtained with a micropuncture sheath using ultrasound guidance. A 0.035-in guidewire was inserted through the GSV and exchanged for a sheath. The RFA catheter was placed 2.0 or 2.5 cm from the saphenofemoral junction (SFJ). Tumescent anesthesia (450 mL of normal saline, 10 mL of sodium bicarbonate, and 40 mL of 1% lidocaine with epinephrine) was injected into the perivenous space. The proximal 7 cm segment of the GSV was treated with two 20 s energy cycles. The other segments of the GSV were treated with either one or two 20 s energy cycles. 5 Adjunctive procedures including phlebectomy or ultrasound-guided foam sclerotherapy (USGFS) were often performed in the same setting as ablation of the GSV. If concomitant phlebectomy was performed, the standard microphlebectomy technique was employed. 5 USGFS using 1% or 3% polidocanol was performed to treat tributaries and incompetent perforators. 5
DUS was performed immediately postprocedure to confirm closure of the GSV and patency of the deep vein system. Postoperatively, the limb was compressed with an elastic bandage for 24 h, then with a graduated compression stocking for 1 week. No patient was given an anticoagulant for DVT prophylaxis. Postoperative DUS was performed 7 days, 1 month, and 3 months after the procedure. The examination focused on detection of EHIT or DVT and evaluation of the ablated veins for closure. The position of any thrombi in the GSV in relation to the SFJ was noted. The entity of EHIT along with a classification system was described by Kabnick et al. 6 Class 1 is defined as a thrombus extending up to the SFJ, class 2 is defined as a thrombus extending into the femoral vein and occupying <50% of the cross-sectional diameter, class 3 is defined as a thrombus occupying >50% of the cross-sectional diameter of the femoral vein, and class 4 is defined as complete occlusion of the femoral vein. If DUS showed EHIT, treatment of EHIT was based on the surgeon’s preference; e.g. serial DUS with surveillance with DUS repeated weekly only or full anticoagulation until the thrombus retracted into the SFJ.
All clinical data and DUS images were reviewed by a surgeon who did not participate in any of the procedures. Demographic data and clinical information including age, sex, height, weight, body mass index (BMI), symptoms of chronic venous disease, and history of DVT were recorded. The patients’ symptoms and signs were recorded using the Clinical, Etiologic, Anatomic, Pathologic (CEAP) clinical classification system. 9 The CEAP classification of venous disease at the time of the procedure was used to compare the severity of disease. The GSV diameter was recorded. The distance between the tip of the RFA catheter and the SFJ was recorded at the time of ablation. The length of the ablated vein and total RFA energy were also recorded. Patients who underwent concomitant phlebectomy or USGFS with 1% or 3% polidocanol of the varicose veins below the knee level were identified. Risk factors for thrombophilia were reviewed, including the Caprini score (which has been used to predict the likelihood of VTE in surgical patients 10 ), procedural factors, and follow-up ultrasound. Ten medical records with missing data were excluded.
Qualitative demographic data are presented as frequencies and percentages, and quantitative data are presented as means and standard deviations. For univariate analysis, qualitative data were analyzed using either the chi-squared test or Fisher’s exact test as appropriate. For quantitative data, the unpaired t-test was used for normally distributed data, and the Mann–Whitney U-test was used for data that did not fit a normal distribution pattern. Multivariate analysis of determinants of EHIT was performed using a multiple logistic regression model. Statistical significance was achieved at a p-value of <0.05. Data were prepared and analyzed using PASW statistics 18.0 (SPSS, Inc., Chicago, IL, USA). The ethics committee of the Siriraj Institutional Review Board approved this study (No. 641/2557 (EC4)).
Results
In total, 97 veins in 82 patients were treated with RFA. There were 15 cases of bilateral disease. The average age of the patients was 59.0 ± 9.5 years. The maximum CEAP clinical class among all patients was CEAP C2 and C3–6 in 38 (39.1%) and 59 (60.9%) patients, respectively. General anesthesia, regional anesthesia, and intravenous sedation were performed in 10 (12.1%), 2 (2.4%), and 70 (85.5%) patients. Treated patients demonstrated a vein diameter ranging from 4 to 25 mm (average, 8.7 ± 3.1 mm). The average energy delivered among all patients was 10.94 ± 3.26 W, and the mean RFA time was 2.56 ± 0.80 min. Concomitant additional procedures were varicose vein phlebectomy (23 procedures, 23.7%) and USGFS (18 procedures, 18.5%). All incompetent GSVs in all patients were successfully treated by RFA. EHIT was identified in 10 legs with an incidence of 10.3%. Class 1, 2, and 3 EHIT was found in 50%, 30%, and 20% of legs, respectively. No class 4 EHIT, DVT, or pulmonary emboli occurred in these patients.
Univariate analysis of procedural factors influencing EHIT.
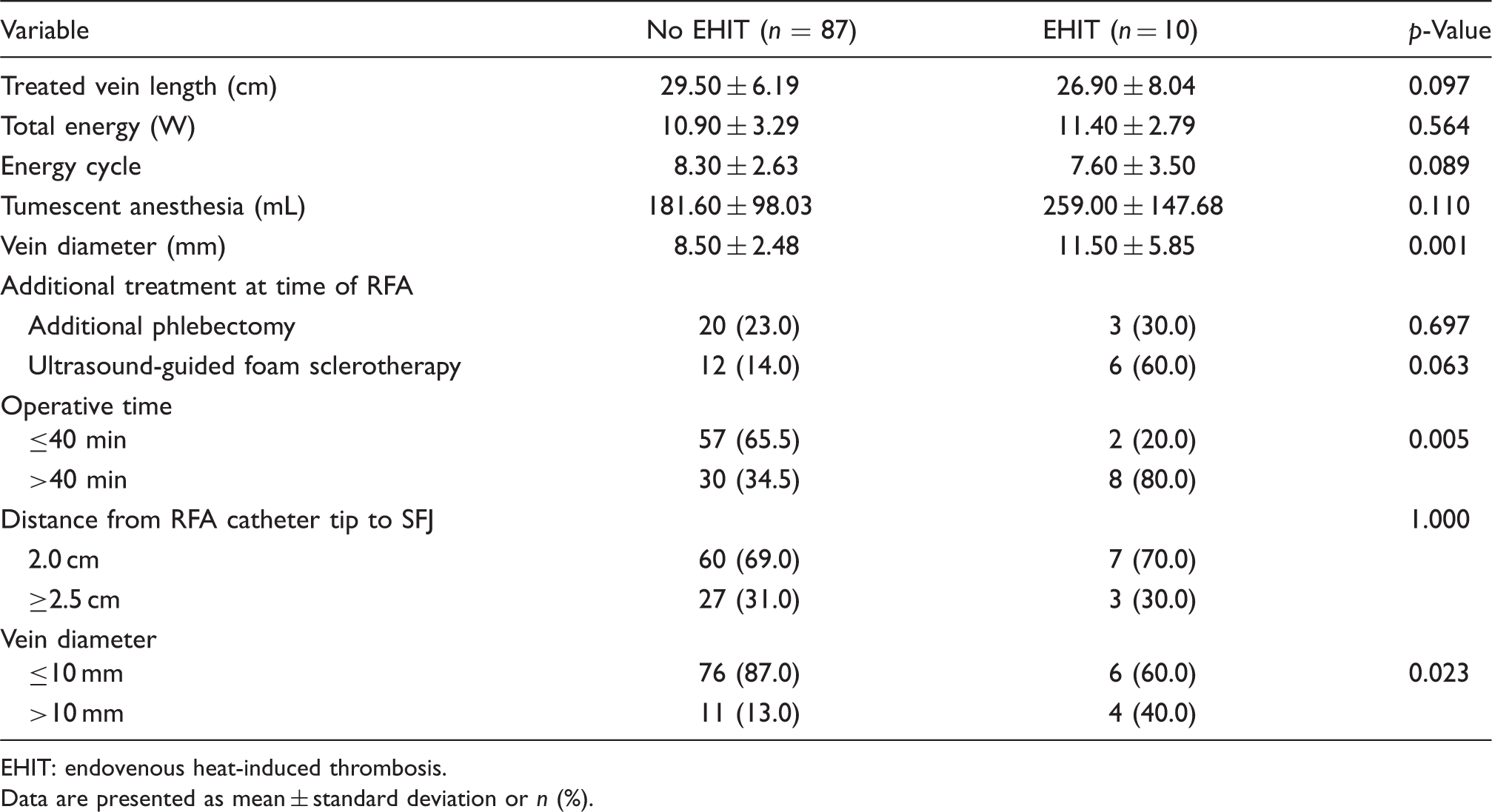
EHIT: endovenous heat-induced thrombosis.
Data are presented as mean ± standard deviation or n (%).
Univariate analysis of clinical factors influencing EHIT.

EHIT: endovenous heat-induced thrombosis.
Data are presented as mean ± standard deviation or n (%).
Multivariate analysis revealed that a vein diameter of >10 mm (odds ratio [OR], 5.97; 95% confidence interval [95% CI], 1.161–30.716; p < 0.05) and an operative time of >40 min (OR, 12.05; 95% CI, 1.36–26.41; p < 0.05) were independent risk factors for EHIT. We found that a Caprini risk assessment score of >6 was not an independent risk factor for EHIT.
Of the 10 patients with EHIT, 5 (50%) had class 1 EHIT, 3 (30%) had class 2 EHIT, and 2 (20%) had class 3 EHIT. None of the patients with class 1 EHIT received an anticoagulant, and their EHIT resolved in 7 days. There were three cases of EHIT class 2. We observed the two patients and performed ultrasonography every 7 days after EHIT was detected. All thrombus retracted above SFJ without any anticoagulant administration. One patient with class 2 EHIT received rivaroxaban for 2 weeks until the EHIT disappeared. Both patients with class 3 EHIT received an anticoagulant for 14 days, and their EHIT resolved in 6 weeks. No symptomatic pulmonary embolism was detected in any patients with EHIT.
Discussion
Management and outcomes of patients with EHIT after RFA.

EHIT: endovenous heat-induced thrombosis; RFA: radiofrequency ablation; BMI: body mass index; GSV: great saphenous vein; SFJ: saphenofemoral junction; USGFS: ultrasound-guided foam sclerotherapy; LMWH: low-molecular-weight heparin; VKA: vitamin K antagonist.
There is a consensus that antithrombotic treatment is not necessary for class 1 EHIT and that anticoagulation is mandatory for class 3 and 4 EHIT. 6 However, uncertainty and disagreement exist regarding class 2 EHIT. Based on our experience and previous reports, class 2 EHIT could be observed because two of three cases of class 2 EHIT resolved within 2 weeks without any treatment. No symptomatic PE was detected. Only 1 case received anticoagulant because the patient could not come to hospital to serial US at 7 days after EHIT was detected. We decided to give rivaroxaban to her and serial US at 14 days. At 14 days after EHIT was detected, the thrombus disappeared. In our point of view, we think that EHIT 2 might be a benign condition as well as EHIT 1; however, we should confirm in the larger cohort study. Patients with class 3 EHIT received anticoagulants, and their EHIT resolved in 2 to 6 weeks.
We found that RFA in patients with a vein diameter of ≥10 mm increased the risk of EHIT. Our result is similar to that of a previous report showing that the diameter of the saphenous vein is a risk factor for EHIT after RFA, especially a vein diameter of ≥8 mm. 13
A prolonged operative time of >40 min increased the risk of EHIT. This may have occurred because of the difficulty in cannulation of the RFA catheter secondary to the tortuosity of the GSV, leading to repetitive trauma of the GSV near the SFJ. Operative time is not only depended on bilateral disease but also adjunct multiple phlebectomy in some cases; however, bilateral disease and additional multiple phlebectomy are not associated with EHIT in our series.
Other reported risk factors for EHIT include age, sex, adjunctive phlebectomy, CEAP class, ablation distance from the SFJ, and Caprini score.6,11,14 Our analysis did not identify any effect of age, sex, or CEAP class for the risk of EHIT. The incidence of EHIT did not increase with the addition of phlebectomy or USGFS.
In our previous practice before 2013, the RFA catheter tip was placed 2 cm from the SFJ. A recent report noted a reduction in EHIT if the RFA tip was positioned at a distance of 2.5 cm from the SFJ. We have placed the RFA tip 2.5 cm from the SFJ since 2013. We found no difference in the occurrence of EHIT between a catheter tip distance of 2.0 and 2.5 cm. 15
The Caprini risk assessment model has been used to predict the occurrence of DVT and pulmonary embolism in medical and surgical patients. 10 We do not routinely give anticoagulant in varicose vein surgery in Thailand. In Thailand, there is lower incidence of DVT than in the Western countries. This research was the first to evaluate the relationship of Caprini score and incidence of EHIT or DVT in Thailand. An increased Caprini risk assessment score was a significant risk factor for EHIT in our univariate analysis, especially in patients with score of >6; however, it was not an independent risk factor in the multivariate analysis, which showed that the independent risk factors for EHIT after RFA were a vein diameter of >10 mm and a prolonged operative time of >40 min. Prophylaxis anticoagulant in case of high risk for EHIT especially in case of larger diameter and expected prolonged operative time should be considered.
The small number of patients with EHIT limits the statistical power of this study. Larger series are needed to clarify which risk factors influence the rate of EHIT following RFA. In addition, further study is required for the role of DVT prophylaxis in high-risk group for EHIT.
Conclusions
The principal risk factors for EHIT after RFA were a vein diameter of >10 mm and operative time of >40 min. Most cases of EHIT appear to be benign and can be treated with observation and serial ultrasound, except class 3 & 4 EHIT, which requires anticoagulant therapy. Additional larger studies are required to confirm these findings and determine whether they are applicable to different populations.
Footnotes
Contributorship
NS researched the literature and conceived the study. NS and TV were involved in protocol development, gaining ethical approval, patient recruitment, and data analysis. NS wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The ethics committee of the Siriraj Institutional Review Board approved this study (No. 641/2557 (EC4)).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Faculty of Medicine, Siriraj Hospital, Mahidol University.