
Abstract
Background
Stiffness is an independent determinant of compression therapy efficacy, beyond compression pressure alone. Three indices — static stiffness index (SSI), dynamic stiffness index (DSI), and walking pressure amplitude (WPA) — quantify stiffness. This study evaluated in vivo stiffness in eight compression stocking models to assess whether those marketed as “strong-elastic” differ significantly from those marketed as “light-elastic”.
Methods
In a prospective, open-label pilot study, 10 healthy participants were each fitted with eight off-the-shelf AG II compression stocking models (4 “strong-elastic”, 4 “light-elastic”). Continuous pressure monitoring was conducted at four standardized anatomical sites (B, B1, C, D) of the right lower extremity using the Picopress® system. A total of 320 measurement cycles were completed. Data were analyzed by comparing grouped results for “strong” vs. “elastic” stockings.
Results
The SSI did not differ significantly between “strong-elastic” (stMCS) and “light-elastic” (elMCS) stockings at any site (p > .05). However, stMCS showed significantly higher DSI at sites B (4.55 ± 2.00 mmHg vs 3.90 ± 1.63 mmHg; p = .028), C (5.83 ± 2.28 mmHg vs 5.10 ± 1.82 mmHg; p = .015), and D (2.33 ± 1.16 mmHg vs 1.58 ± 0.87 mmHg; p < .001). For WPA, stMCS exhibited significantly higher stiffness at B1 (6.75 ± 2.26 mmHg vs 6.03 ± 2.27 mmHg; p = .018), C (4.33 ± 2.31 mmHg vs 3.73 ± 2.24 mmHg; p = .020), and D (6.25 ± 2.07 mmHg vs 4.23 ± 1.59 mmHg; p < .001). Mean lower leg circumference increased from 0.50 cm (D) to 1.05 cm (C), depending on movement.
Conclusion
At B1, no significant differences in SSI or DSI were found between “strong-elastic” and “light-elastic” stockings, whereas WPA significantly differentiated both groups. Overall stiffness values exceeded previous reports, indicating both stMCS and elMCS possess substantial stiffness and likely improve venous hemodynamics.
Keywords
Introduction
Medical compression therapy represents a fundamental component of conservative management for venous and lymphatic disorders, including chronic venous insufficiency, acute deep vein thrombosis, and acute and chronic lymphedema.1,2
The compression class is a well-established parameter for classifying compression stockings and is defined according to compression classes I–IV, which in Germany are regulated by the RAL-GZ 387 standard (Reichs-Ausschuss für Lieferbedingungen, Deutsches Institut für Gütesicherung und Kennzeichnung e.V. [German Institute for Quality Assurance and Labeling]) with pressure ranges as follows: Class I (18–21 mmHg), Class II (23–32 mmHg), Class III (34–46 mmHg), and Class IV (≥49 mmHg).3,4
In contrast, stiffness — reflecting the dynamic material properties (i.e., rigidity) of compression garments — is currently less commonly used as a predictor of therapeutic efficacy and is rarely reported by manufacturers. The stiffness of compression garments directly influences the increase in working pressure generated between the compression stocking and the lower limb as the leg circumference expands during muscular activity.5–12
Several indices are available to quantify stiffness in vivo, including the static stiffness index (SSI), dynamic stiffness index (DSI), and walking pressure amplitude (WPA). The SSI is defined as the pressure difference measured between the limb and compression garment when transitioning from a supine to standing position.2,4–6,9,10,13–19 The DSI represents the difference between maximum and minimum pressures recorded during repeated dorsal extension of the ankle joint, 2 while the WPA corresponds to the pressure difference measured during repeated tiptoe-exercises, simulating physiological walking movements in place. 2
The dynamic mechanical behavior of medical compression stockings is crucial during movement and plays a significant role in the hemodynamic benefits of compression therapy. This dynamic action, often described as the “massage effect” occurring during muscle systole and diastole, leads to reduction of vessel diameter, improved venous return, decreased ambulatory venous hypertension and reflux, enhanced filtration/resorption balance, and consequently reduction of tissue edema.3,13,14,20,21
Patients, materials, and methods
Study aim
This exploratory study aimed to investigate and compare the in vivo pressure characteristics of eight different, currently commercially available models of circular-knit medical compression stockings, all classified as compression class AG II, in subjects with healthy venous systems. To this end, the study stockings were compared in terms of their static stiffness index (SSI), dynamic stiffness index (DSI), and walking pressure amplitude (WPA) in order to determine the extent to which the marketing terms “strong-elastic” and “light-elastic” used by manufacturers correspond to the data collected in vivo.
Study design
This prospective, open-label pilot study included 10 participants with healthy veins (4 males, 6 females), examined between July and December 2024. Each participant attended two study visits. At the initial visit, eligibility was confirmed by assessing inclusion and exclusion criteria, including duplex and doppler ultrasound examination of the lower limb venous system and evaluation of arterial blood flow via ankle-brachial index (ABI) measurement. The legs of the test subjects were then measured in a specialized medical supply facility and subsequently, four “light-elastic” and four “strong-elastic” off-the-shelf circular-knit medical compression stockings (class AG II, 23–32 mmHg) were custom-ordered for each participant. Leg circumference measurements at points B, B1, C, and D were further obtained during standardized movement sequences (Figure 1) to access the changes in circumference during motion. At the second visit, SSI, DSI, and WPA were measured for each of the eight stocking models using the PicoPress® system (Microlab Elettronica SAS, Padua, Italy). Measurements were conducted at the B, B1, C, and D anatomical landmarks on the right lower limb of each participant. The sequence in which the compression stockings were tested was randomized for each study participant using https://www.randomizer.org/. In addition to compression pressure data, participant demographics (age, sex, weight, height, BMI), environmental parameters (room temperature), and time of day were recorded for each measurement session. To minimize potential confounding effects due to ambient temperature variation, all measurements were performed between late October and early November 2024. Study protocol for one of a total of eight measurement cycles per test subject to determine the pressure curves under the respective medical compression stockings applied.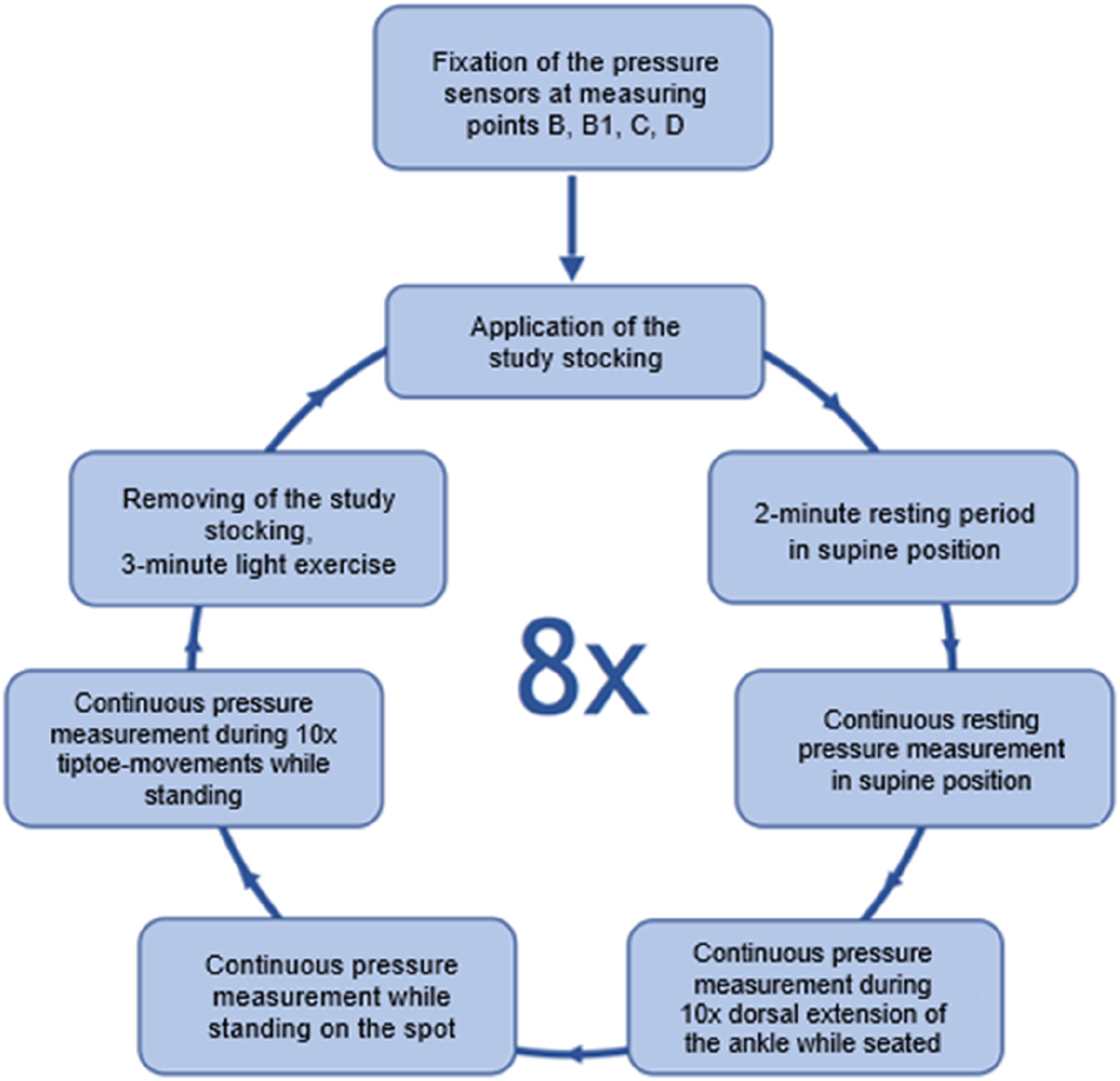
Ethics
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. All participants provided written informed consent prior to enrollment. The study protocol received approval from the Westfalen-Lippe Ethics Committee (approval number: 2024-370-f-S, dated 12 September 2024).
Inclusion and exclusion criteria
Eligible participants were adults aged 18 to 80 years who provided informed consent and were physically able to perform the movements required for compression pressure measurements. Exclusion criteria comprised lack of consent or inability to provide consent, medical contraindications to compression therapy (including chronic heart failure NYHA class III, severe peripheral arterial disease with ankle artery pressure <50 mmHg, and cardiovascular events within the past 6 months), pregnancy or breastfeeding, symptoms of dizziness or unsteadiness, and pre-existing conditions affecting the lower extremities such as chronic venous insufficiency, lipedema, or lymphedema.
Study products
Stocking manufacturers with the corresponding models of selected medical compression stockings.

Pressure measurement procedure
A total of 320 measurement cycles were conducted according to a standardized sequence of movements. For each compression stocking and participant, pressure values were recorded at measuring sites B, B1, C, and D under the following conditions: at rest in the supine position, at rest in the standing position, during active dorsal extension of the ankle while seated, and while performing toe-stands in the upright position (Figure 1).
All measurements and the application of the compression stockings were performed by the same trained investigator to ensure consistency. Participants were blinded to the specific compression stocking model being tested in each cycle. Pressure data were collected using the PicoPress® system (Microlab, Padova, Italy). At the beginning of the measurement series, pressure sensors were affixed once to the right lower extremity of each participant at measurement points B, B1, C, and D. The sensors remained in place throughout all eight measurement cycles to maintain positional accuracy and avoid variability. To don and doff the stockings, the “Doff'N'Donner” aid (Sigvaris, Memmingen, Germany) was used, as its rolling mechanism minimized disturbance of the attached pressure sensors. After each new stocking was applied, probe placement was verified, and care was taken to ensure the fabric was evenly applied without folds or creases.
Each measurement cycle commenced with a two-minute rest period in the supine position. Resting pressure was then recorded once a steady-state pressure curve was reached. To avoid artificially elevated readings due to compression of the calf against the examination surface, a foam roll (15 cm diameter) was placed beneath the distal thigh, as previously described. 2
Subsequently, participants were instructed to sit upright and perform 10 active dorsal extensions of the ankle while continuous pressure data were recorded. This was followed by a transition to a standing position, where pressure was continuously monitored until a steady-state curve was again achieved. Finally, participants performed ten toe-stands while standing, with continuous pressure monitoring throughout.
All measurements were carried out following a predefined Picopress protocol to ensure standardized conditions across participants and trials. After completion of each cycle, the stocking was removed, and participants engaged in light walking for 3 minutes before the next stocking was applied.
Statistical analysis
Statistical analyses were conducted using Microsoft Excel (Office 2019, Microsoft Corp., Redmond, WA, USA) and IBM SPSS Statistics (version 30, IBM Corp., Armonk, NY, USA).
Depending on the nature of the data, comparisons were made using the Wilcoxon signed-rank test for paired samples and the Mann–Whitney U test for independent samples. Grouped data from compression stockings marketed as “strong-elastic” (stMCS) were compared with those marketed as “light-elastic” (elMCS). A significance level of 5% (p < .05) was defined a priori for all statistical evaluations.
Results
Participant characteristics
Ten participants (6 female, 4 male) with clinically healthy venous systems of the lower extremities were enrolled and examined over a 6-month period (July 2024 to December 2024). Descriptive analysis yielded the following means ± standard deviations: age 29.5 ± 3.44 years, height 173.3 ± 5.95 cm, weight 68 ± 9.91 kg, body mass index (BMI) 22.57 ± 2.66 kg/m2, and ankle-brachial index (ABI) 1.05 ± 0.08 bilaterally.
Comparison of stiffness indices: SSI, DSI, and WPA
Mean values and standard deviations for the grouped data of the “strong-elastic” (stMCS) and “light-elastic” (elMCS) medical compression stockings.

* indicates statistical significance (p < 0.05).
In contrast, significant differences were observed in the dynamic indices — the dynamic stiffness index (DSI) and the walking pressure amplitude (WPA) — at various measurement points during movement. For the DSI, the comparison between stMCS and elMCS revealed statistically significant increases in mean dynamic stiffness at measurement points B (0.65 mmHg), C (0.73 mmHg), and D (0.75 mmHg). At B1, however, the mean difference in DSI was only 0.10 mmHg and did not reach statistical significance. Regarding the WPA, significant differences between stMCS and elMCS were observed at measurement points B1, C, and D, with mean increases in stiffness of 0.72 mmHg at B1, 0.60 mmHg at C, and 2.02 mmHg at D.
Circumferential changes of the lower extremity
Changes in body position — standing, dorsal extension of the ankle, and tiptoe stance — resulted in significant increases in mean lower leg circumference at various measurement points compared to the base circumference at rest. During standing, significant circumferential increases were observed at measuring points B (0.65 cm; p = .006), B1 (0.85 cm; p = .041), and C (0.50 cm; p = .020). Ankle dorsiflexion produced significant increases at points B (0.60 cm; p = .006) and C (0.85 cm; p = .007). During tiptoe stance, significant increases were recorded at points B (0.95 cm; p = .005), B1 (1.00 cm; p = .041), C (1.05 cm; p = .007), and D (0.50 cm; p = .026).
Circumferences (mean ± standard deviation) in cm at measurement points B, B1, C, and D comparing the resting condition in supine position with measurements taken during standing, ankle dorsiflexion, and tiptoe stance.

Discussion
Although the significance of stiffness for the efficacy of compression therapy has been extensively documented,5–9,11–13,15–17,20,22,23 there remains a limited number of studies addressing its in vivo measurement.2,3,5,10,17,24,25 Among these, published between 2000 and 2009, five specifically investigated stiffness in medical compression stockings.3,5,10,24,25 However, to our knowledge, only one study published in 2006 directly compared the stiffness of individual compression stockings. 5 At present, no studies exist that provide an in vivo comparison of stiffness among currently commercially available compression stocking models, particularly between those marketed as “strong-elastic” and “light-elastic”.
In vivo determination of stiffness
Medical compression therapy is known to enhance venous hemodynamics and reduce venous reflux. 3 A critical factor in this therapeutic effect is the elasticity of the compression material, which acts as a counterforce against the expanding calf circumference during muscle contraction, thereby facilitating improved venous return. 3
The elasticity of compression materials can be assessed through its stiffness, defined in vitro as the increase in compression pressure per 1 cm increase in leg circumference or stretch of the material at the respective measurement site.2,5–8,10,11,13,15,26 Stiffness thus represents a product characteristic reflecting the dynamic and elastic properties of the material, which are particularly relevant during standing and movement,6,9–11,15,16,22,23,26 making in vivo assessment essential for understanding real-world performance.
However, standardized determination of stiffness in vivo is challenging due to natural anatomical variability. Human leg circumference changes do not uniformly approximate 1 cm, with literature reporting the greatest changes at the B1 measurement point.5–8,13,15,22,24,26 In previous studies, an average circumference increase of approximately 8 mm has been documented when transitioning from supine to standing positions, 5 which corresponds closely to the 8.5 mm average increase at B1 observed in the present study (Table 3).
Interestingly, the data presented in this study also demonstrate significant circumference increases at the C measurement point, averaging 8.5 mm during dorsal extension of the ankle and 10.5 mm during tiptoe stance—values comparable to those recorded at B1. Contrary to previous reports, in this study the maximum circumference increase was thus observed at the C measurement point rather than B1.
Stiffness indices
Static stiffness index (SSI)
The static stiffness index (SSI) in vivo, defined as the pressure difference between the applied pressure during standing on the spot and the resting pressure in the supine position measured between the compression material and the lower leg 2,4–6,9,10,13–19, represents the primarily recommended parameter for stiffness analysis of compression materials. 13 This preference is attributed to its ease of measurement 13 and the well-documented strong correlation with the dynamic stiffness index reported in the literature.5,6,10,13,14
Dynamic stiffness index (DSI) and walking pressure amplitude (WPA)
To more accurately assess the massage effect13,14,21 of medical compression stockings, influenced by circumference changes of the legs occurring predominantly during movement—and the consequent stretching and relaxation of the elastic fibers in compression materials—dynamic indices have been defined alongside the SSI. The dynamic stiffness index (DSI) quantifies the difference between the minimum and maximum pressures during ankle joint movements,1,2,9,14,26 while the walking pressure amplitude (WPA) reflects the pressure difference between maximum and minimum values recorded during physiological walking movements in standing position. 2 Both indices aim to better characterize the effects of dynamic movement on compression materials. Importantly, they account for the hysteresis of the compression fabric—that is, the loss of elastic fiber length recovery following repetitive stretching and relaxation 7 —thereby providing a more realistic representation of in vivo conditions. However, previous studies have shown that the SSI and DSI correlate well with each other.5,6,10,13,14
Stiffness of “strong-elastic” and “light-elastic” compression stockings
In alignment with the commonly accepted definition of stiffness, the present study primarily focused on pressure measurements obtained at the B1 anatomical site. In the literature, the stiffness of medical compression stockings is generally described as low, with a static stiffness index (SSI) typically below 5 mmHg, 13 thereby classifying them as elastic compression materials.10,20,27,28
The data from the present study demonstrated for measurements taken at the B1 site a mean SSI of 5.65 ± 3.14 mmHg versus 5.78 ± 2.55 mmHg, a dynamic stiffness index (DSI) of 7.63 ± 2.67 mmHg versus 7.53 ± 2.55 mmHg, and a walking pressure amplitude (WPA) of 6.75 ± 2.26 mmHg versus 6.03 ± 2.27 mmHg for the stMCS vs. elMCS, respectively (Figure 2). SSI, DSI, and WPA at measuring point B1 for the group of “strong-elastic” (stMCS) and “light-elastic” (elMCS) compression stockings, showing the mean value [x] and median [-].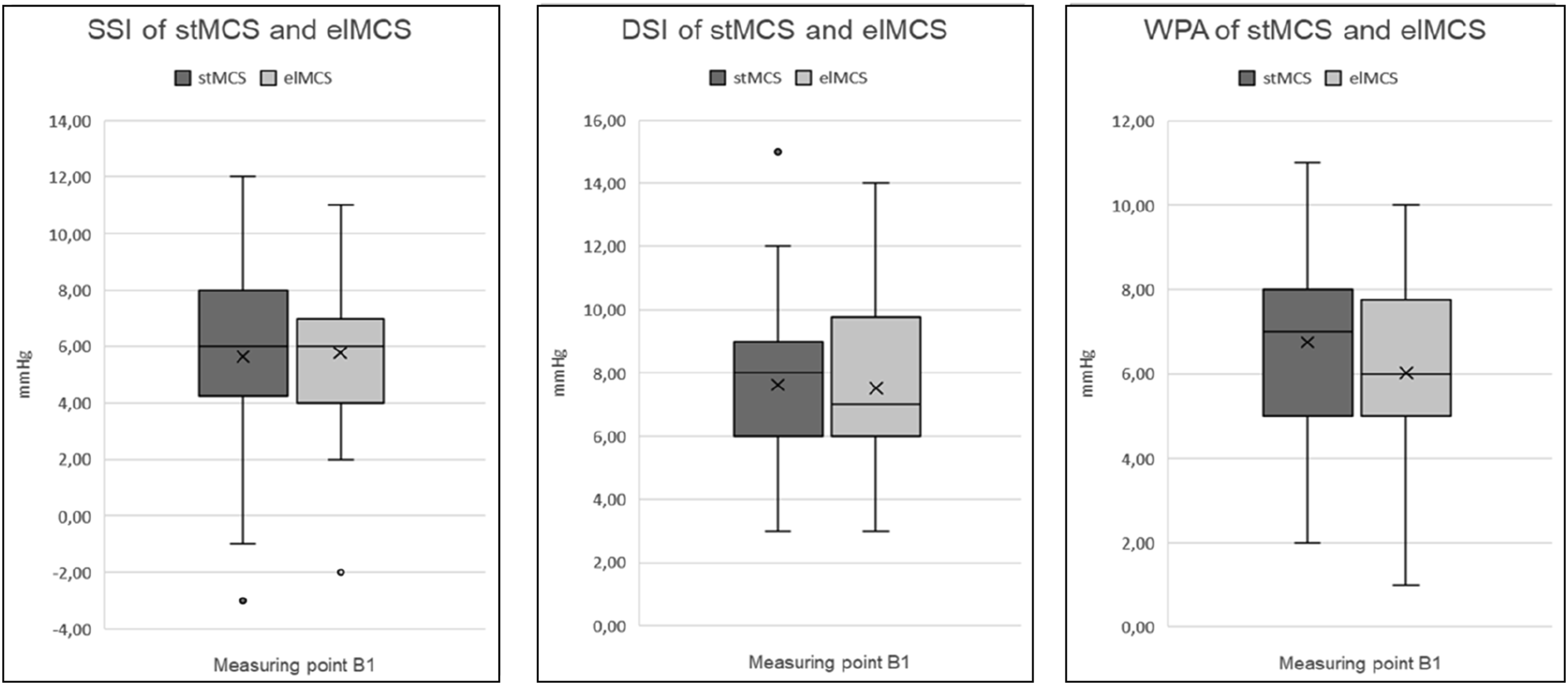
A statistically significant difference between stMCS and elMCS was found only for the WPA, while no such difference was observed for the SSI or DSI at the B1 site. Notably, the stiffness values observed for both groups exceeded those previously reported in the literature. 13
This outcome is favorable in so far, as the hemodynamic benefits associated with compression therapy—such as the reduction of venous reflux and the mobilization of edema 3 —can reasonably be expected for both “strong-elastic” and “light-elastic” stocking models. However, the absence of significant differences in SSI and DSI values at the B1 site between the two stocking types remains surprising. One possible explanation may be that the average circumference increase of only 0.85 cm at B1 falls short of the 1 cm increase typically defined in the determination of stiffness.
This possible explanation is backed by the significant changes recorded for the WPA at B1, in which the average circumferential differences of the lower extremity reached the required 1,0 cm.
Stiffness assessment at alternative measurement sites
The significant differences in stiffness observed between stMCS and elMCS at the C and D measurement sites (Table 2) should be interpreted with caution. This is particularly relevant for the DSI values at the C and D measuring sites, as the required 1 cm increase in lower leg circumference—representing the defined stretch of the compression material necessary for stiffness calculation—was not achieved (Table 3).
By contrast, the WPA data appear more clinically relevant. At the C measurement site, significant differences in WPA between stMCS and elMCS (4,33 ± 2,31mmHg vs 3,73 ± 2,24mmHg; p = 0,20) were observed at a circumference increase close to 1 cm (Table 3). However, the significantly elevated WPA values for the group of stMCS vs. elMCS at the D site occurred alongside only a modest increase in circumference of 0.5 cm and must therefore be questioned in relevance.
Consequently, in addition to the B1 site, the C measurement point may warrant consideration in future studies investigating in vivo stiffness properties of medical compression stockings.
Limitations
This study has several limitations. Most notably, the small sample size may restrict the generalizability of the findings; however, this limitation was partially offset by the high number of measurement cycles conducted. Moreover, the study population consisted exclusively of participants with healthy venous systems. Future investigations should include individuals with venous and lymphatic pathologies to evaluate whether the findings are transferable to clinical populations.
Additionally, individual anatomical differences in leg contours may have influenced the fit of the off-the-shelf compression stockings, potentially introducing variability in the results. Nonetheless, this variability reflects the real-world application of medical compression stockings in routine care, where individual differences in fit must be anticipated and accounted for. Following completion of this study, an additional document was published, 29 in which the definitions of the DSI and the WPA differ slightly from the definitions used in this study. For improved comparability, future studies may therefore consider adopting these standardized definitions.
Conclusion
This study investigated the in vivo behavior of off-the-shelf medical compression stockings of compression class AG II. No significant differences were observed between compression stockings marketed as “strong-elastic” and those marketed as “light-elastic” at the B1 measurement site for the commonly applied stiffness indices SSI and DSI. In contrast, a significant difference was detected for the WPA at B1. Notably, both groups (stMCS and elMCS) demonstrated stiffness values exceeding those previously reported in the literature, indicating a generally favorable impact of medical compression stockings on venous hemodynamics, regardless of their marketing as “strong-elastic” or “light-elastic”.
Footnotes
Acknowledgements
The authors would like to express their sincere gratitude to Maren Hoffmann, Sonja Feldmann-Plum and Marion Erdt for their dedicated assistance throughout the study. The authors also wish to thank Peggy Schneider for her insightful and constructive comments on the manuscript.
Ethical considerations
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. All participants provided written informed consent prior to enrollment. The study protocol received approval from the Westfalen-Lippe Ethics Committee (approval number: 2024-370-f-S, dated 12 September 2024).
Author contributions
Conceptualisation: M.S., D.B.
Methodology: D.B., M.S.
Data acquisition: D.B.
Formal analysis: D.B., M.S., N.A.R
Investigation: D.B.
Writing – original draft: D.B.
Writing – review & editing: D.B., M.S., N.A.R
Supervision: M.S.
Guarantor: D.B.
All authors have read and approved the final version of the manuscript and accept responsibility for the integrity of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Stifterverband für die Deutsche Wissenschaft e.V. (Donors’ Association for the Promotion of Sciences and Humanities in Germany).
Declaration of conflicting interests
Dennis Braß (D.B.) received travel grants from AbbVie Inc.
Nessr Abu Rached (N.A.R) received funding from Novartis Pharma, Janssen-Cilag GmbH, Recordati Rare Diseases Germany GmbH, UCB Pharma, Almirall Hermal GmbH, Bristol-Myers Squibb (BMS), and Johnson & Johnson for financial support, travel grants, and/or personal honoraria for lectures unrelated to the submitted work.
Markus Stücker (M.S.) received consulting fees from Bauerfeind AG, URGO GmbH, and eurocom e.V., speaker fees from Julius Zorn GmbH, URGO GmbH, and Viatris, and research funding from Mölnlycke Health Care AG, medi GmbH & Co. KG, URGO GmbH, Huntleigh GmbH, Rheacell, and eurocom e.V.