
Abstract
China is expected to have a rapid growth in specialized early intervention (EI) services for young children ages birth to 6 and their families. A major barrier in the provision of EI services in China is the shortage of well-trained EI personnel. In 2013, a Home-Based Early Intervention Program (HBEIP) was started at South China Normal University (SCNU) in Guangzhou, China to prepare future professionals to use family-centered EI practices adapted from similar programs in the United States. During the first year of implementation, HBEIP collected data from a self-efficacy survey and a needs assessment. Results from the evaluation showed that Chinese trainees perceived the family-centered approach to EI as relevant and valuable, and indicated needs for improving supervision and coaching supports in future implementation of HBEIP. The research team discussed implications for cross-cultural adaptation and implementation of personnel training practices.
Keywords
In China, the number of children from birth to 6 years old with disabilities has been increasing. According to the most recent national sampling survey, the estimation was 1.68 million (China Disabled Persons’ Federation, 2006). However, most were not diagnosed. For example, in 2015, only 48,000 children within this age range were diagnosed with some disabilities (China Disabled Person’s Federation, 2016). On the contrary, public early intervention services are not accessible without an official diagnosis of disability (Hu & Yang, 2013). As a result, even fewer children of this age have received public services. According to results from the most recent survey in 2003, only 67% of this population received public medical rehabilitation or intervention services, most of which were hearing and physical therapies (China Disabled Persons’ Federation, 2003). This status of public services probably remains the same today, as early intervention (EI) from birth to 6 is still not mandated in any legislation in China. The discrepancy between children identified as needing such support and those receiving help might be due to lack of well-trained special education personnel. As the importance of early development gained more attention, the State Council of China and several local governments, including the government of Guangdong province, announced a new administrative plan in 2010. The plan calls for expanding the age range for public special education services from its current span of 6–15 years to 3–18 years by 2016.
Guangdong is a province in southeast China with the largest population of any province (i.e., 104 million). To work as a licensed educator for preschoolers with or without disabilities in Guangdong, a pre-service teacher must complete core coursework in a licensure program for early childhood or Grades 1 through 3. The coursework is designed to equip pre-service teachers with essential knowledge and skills; nonetheless, at this point there is no province- or nationwide licensure for special education professionals across all ages, except in the city of Shanghai, which is outside the Guangdong province. Results from a survey study conducted by Xie and colleagues (2014) showed that 75% of professionals working in special education schools and classrooms in Guangdong were trained under other disciplines, such as early childhood education, educational science, psychology, and medical science, with very limited preparation in addressing the needs of students with disabilities. Therefore, an effective personnel preparation program in special education is a significant need.
As mentioned, both national and local administrative plans have emphasized the importance of training competent special education teachers as one of the foundational building blocks to support the development of special education services. South China Normal University (SCNU), a major teacher-education university located in the capital city Guangzhou, Guangdong, has a long history of preparing educators in the greater South China region. In 2013, a new department was established at SCNU to prepare special education personnel; however, a solid teacher training model was not developed at that time. Concurrently, several initiatives called for increasing the number of qualified professionals for serving young children with disabilities. Researchers also emphasized the need to transition from a traditional, child-centered service model to a more family-centered approach in EI (Hu & Yang, 2013). Thus, an experimental pre-service and in-service training program was developed at SCNU as the first initiative in China to focus on preparing future early childhood interventionists in carrying out family-centered, naturalistic, environmentally based services with young children who have developmental delays (Bruder, 2000; Johnson, Rahn, & Bricker, 2015; McWilliam, 2010; Swanson, Raab, Roper, & Dunst, 2006). This Home-Based Early Intervention Program (HBEIP) adapted a family-centered model (Dunst, Trivette, & Hamby, 2007) to provide contextually relevant experiences for students.
Conceptual Framework of HBEIP
Implementation Science Framework
With careful cultural consideration, program designers adopted an implementation science framework (Sloboda, Dusenbury, & Petras, 2014) as the underlying conceptual model for developing HBEIP. This framework serves as the foundation for adapting the delivery of family-centered practices so that (a) the practices are culturally responsive, (b) accurate implementation of effective personnel training practices can be ensured, and (c) improved outcomes will be observed. The implementation science framework (Sloboda et al., 2014) provides a roadmap for successful implementation of a new program in sequential stages: dissemination and diffusion, adoption, implementation, and sustainability.
In the dissemination stage, program developers review the published work of researchers who have developed effective practices and of practitioners searching for innovative practices. In the adoption stage, the program team analyzes each innovative practice to determine whether it or an alternative solution will be implemented. After a practice has been selected, the third or implementation stage explores how this new practice including evidence-based strategies will be integrated into the existing service system in the community. The team also examines initial evaluations of the effectiveness and the “fit” of the new practice. This evaluation informs the fourth stage devoted to sustainability, in which community personnel deliver the installed practice across an extended period of time with high procedural fidelity. All four stages in this implementation science schema are influenced by the context, and are characterized by the program, the intervention, the organization and community, and the people who implement the practice. As a result, adaptations occur in every stage to resolve the conflicts observed between the newly implemented practice and culturally specific, contextual factors.
Family-Centered EI Practices
Family-centered EI practices include fulfilling family needs and respecting the involvement of Chinese families in the raising of their children. The concept of “family-centered EI practices” has been widely adopted in health care, human services, education, and related fields in the United States, defined by Dunst et al. (2007) as “an approach to working with families that honors and respects their values and choices and which includes the provision of supports necessary to strengthen family functioning” (p. 370). This approach is grounded on the values and beliefs that (a) the professional–family partnership is an equal-power relationship with respect, dignity, and active collaboration; (b) constant, transparent yet caregiver-friendly information sharing supports families in making informed decisions; and (c) empathetic understanding of family choices, as well as individualized, responsive services based on the strengths, needs, and priorities of families and their children will help promote positive outcomes (Bruder, 2000; Dunst et al., 2007; Dunst, Trivette, & Hamby, 2008).
In China, from the traditional cultural perspective, parents often view teachers as the experts in instruction and as authorities who should take full responsibility for the learning of their children. With this philosophical mind-set, the existing body of research literature and practices in special education primarily address school-age students; thus, service models for early childhood intervention (ECI) have mirrored school-age special education and services centered on the child rather than the family (e.g., child, parents, and siblings). Given the nature of providing services to the birth-to-five population, as well as the fact that families are the primary caregiving units during the early years, an ecological approach encompassing active family involvement has been strongly encouraged in ECI (Chiang & Hadadian, 2010; Jiang & Huang, 2005; Yang, 2003).
Currently, there is increasing attention and advocacy for supporting and educating families of young children with special needs, making the adoption of family-centered practices particularly timely. Researchers (e.g., Jiang & Huang, 2005; Yang, 2003) have indicated that a lack of empirical findings and often ineffective current practices for supporting families remain as major challenges. Due to a scarcity of research and practices in China for delivering family-centered EI in a natural environment (e.g., home), implementing evidence-based, well-studied practices from other countries with ongoing careful adaptation and evaluation is a feasible and necessary strategy.
Program Development
HBEIP is an experimental personnel training program aimed at providing Chinese early interventionists the knowledge, skills, and experiences necessary for serving young children below 6 years old and their families in a home setting. The purposes of HBEIP included the following: to (a) adapt evidence-based EI practices from the United States and Europe, (b) develop a solid infrastructure for HBEIP, (c) create informative and explicit training materials, (d) implement HBEIP with an effective training format, and (e) review the cultural appropriateness of the adapted practices. HBEIP was developed by a team of researchers who adapted home-based, family-centered, evidence-based practices (EBPs) from the United States. This two-phase training program consisted of a 3-week on-site training session as the first phase, followed by a 15-week supervised practicum as the second. An overview on the development and implementation of HBEIP is summarized next.
International Teaming
The project established a team of seven researchers for the development of HBEIP. Team members consisted of three local researchers from the SCNU and four from universities in United States. All team members, except for the local parent consultant, had or were working on doctorates in special education. Among them, five were native Chinese speakers who were fluent in English. Supported by the other U.S. researchers, the lead researcher (i.e., the first author) took the lead in planning for the timeline of implementation and the roles of other team members, provided core training sessions and online support sessions, as well as conducted the evaluation of training outcomes. The two local researchers were responsible for recruitment of students and families, planning and delivering prerequisite training sessions, and supervising practicum experiences. The parent consultant provided feedback on the design of training topics and practicum experiences.
Stages of Development and Implementation
The research team selected and adapted three intervention practices as the core of HBEIP based on activities, routines, and efforts to build capacity. As mentioned above, according to the implementation science framework, the team introduced HBEIP in four stages: dissemination and diffusion, adoption, implementation, and sustainability (Sloboda et al., 2014). Adaptations took place across stages to acknowledge the cultural differences between China and the original contexts in which the practices were developed. At present, HBEIP is in the third stage, implementation.
Stage 1: Dissemination and diffusion
The three intervention practices chosen for HBEIP were disseminated in a “user-pull” model in which researchers identify needs for discussions with users. Here, the specific needs at SCNU motivated and initiated the process (Thigpen, Puddy, Singer, & Hall, 2012). In an initial meeting, the lead researcher, research consultant, and local researchers discussed the current system, services, and needs for ECI in Guangzhou, and realized the need and urgency for the HBEIP initiative. Several international meetings were held using online video-conferencing technology to allow deliberations among research team members regarding local needs and evidence-based EI practices in the United States. These discussions helped researchers draft an implementation plan and specify the scope for HBEIP.
Stage 2: Adoption
During this second stage, additional members joined the research team to expand the group’s knowledge and skill repertoire. Team members review the literature in both Chinese and English to identify potential EI practices, discuss advantages and barriers of each, and rate each of them (see Table 1). Three approaches or models of EI service were selected: activity-based intervention (ABI; Pretti-Frontczak & Bricker, 2004), routines-based intervention (RBI; McWilliam, 2010), and a capacity-building approach (Swanson et al., 2006). The team selected these practices to meet the needs of the community and to match the capacity and practices of the special education program at SCNU.
Considerations for the Selection of Practices.
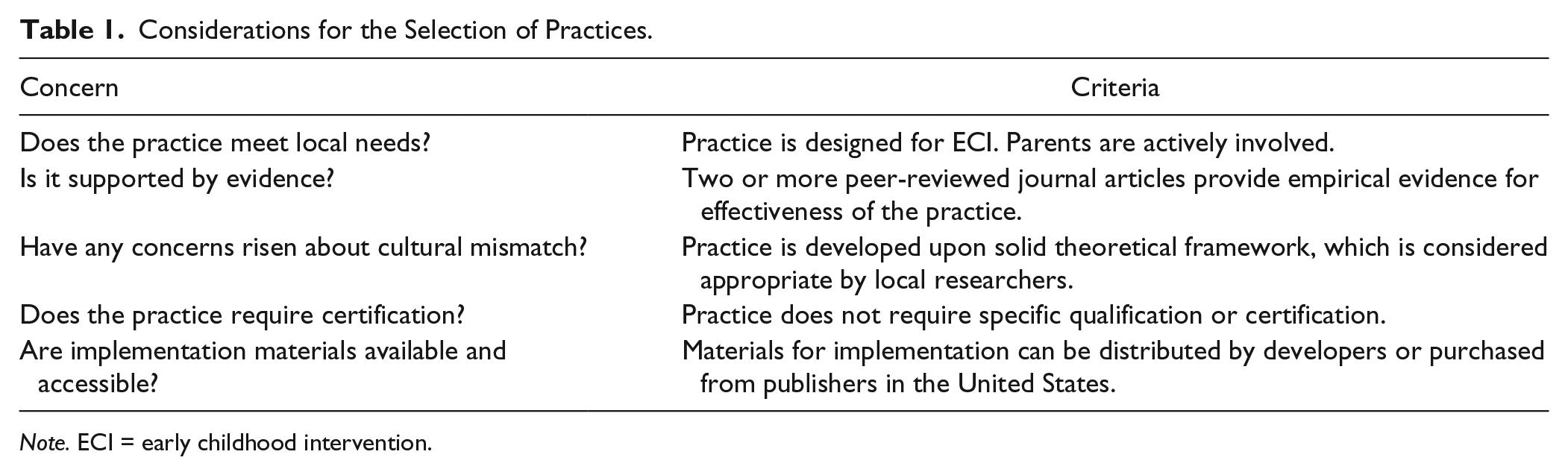
Note. ECI = early childhood intervention.
Stage 3: Implementation
Adopting these three research-based practices led to the next stage, implementation, in which the project “installed” the selected practices in the teacher training program as a supervised practicum. This critical stage of implementation originally includes six steps as suggested by Fixsen, Naoom, Blase, and Friedman (2005): selection, pre-service training, consultation and coaching, staff evaluation, program evaluation, and facilitative administrative supports. Results from evaluating the implementation outcomes will inform innovations at the system’s level. Given the language differences between the local community and the communities in which the practices were developed, the team added an additional step, language translation and content adaptation, as the first step. The training structure and procedures of the HBEIP program will be delineated later in the program description section. In addition, a detailed explanation of the seven steps of implementation and the current state of HBEIP can be found at http://hbeip.blogspot.com.
Stage 4: Sustainability
To date, the first cohort of HBEIP has completed the 3-week intensive training and has practiced providing family-centered services to young children with disabilities and their families. The project has recruited and begun training a second cohort. With support from the administrators, the local researchers at SCNU have decided to continue offering HBEIP at the beginning of every school year to promote the awareness and usage of family-centered practices in Guangzhou.
Program Description
Participants
In June, 2013, a recruitment announcement was made to undergraduate students, graduate students, and staff in the Department of Special Education at SCNU, as well as to in-service special educators from five special education schools in Guangzhou. Forty-four participants, including 27 students (i.e., undergraduate and graduate levels), four faculty members, and 13 special educators, were enrolled. The mean age of participants was 29 years, with two males and 42 females. In terms of educational attainment, two participants had earned doctorates, 13 had or were working toward master’s degrees, and the rest had or were working toward bachelor’s degrees. All participants had a background in school-age special education, from either degree-related programs or in-service professional development. Regarding years of experiences serving children aged birth to 5 with special needs and their families, 21 participants (47%) reported no experience at all, six (14%) indicated less than 2 years, and 17 participants (39%) indicated 3 to 16 years’ experience.
Attendance and attrition
Thirty-two participants attended all 47 hr of in-class learning activities; 12 in-service professionals attended only portions of the training in segments ranging from 3 to 8 hr, depending on their availability from work. After training, 23 undergraduate student participants began supervised practicum experiences. Twenty (87%) attended all 15 weeks of home visits and supervisor meetings. The other three students missed one to two visits or meetings, due to health issues. All four online support sessions had an attendance rate of 90% or above. Five students missed one of the online sessions due to technical reasons (e.g., the Internet speed was not sufficient for using the online conferencing platform). Two of the four faculty members, who are the local researchers in this study, participated fully in all the in-class training, and supervised practicum meetings and online sessions. Table 2 shows the attendance record of HBEIP participants.
Attendance of Participants by Groups (n = 44).

Training Structure
HBEIP consisted of in-class training and supervised practicum, which were conducted sequentially in two semesters. All components of HBEIP were offered at no cost to participants.
In-class training
The local researcher provided seven prerequisite training sessions in a total of 10 hr, focusing on theories about typical/atypical development, behavioral management, family, and individualized instruction. These sessions were embedded into the regular coursework provided at SCNU in 1 week. After that, the lead researcher visited SCNU for 2 weeks and provided 13 core training sessions in a total of 37 hr, focusing on specific strategies in providing family-centered intervention services in a home setting. The topic and length of each training session are listed in Table 3.
Training Topics and Length of Time.
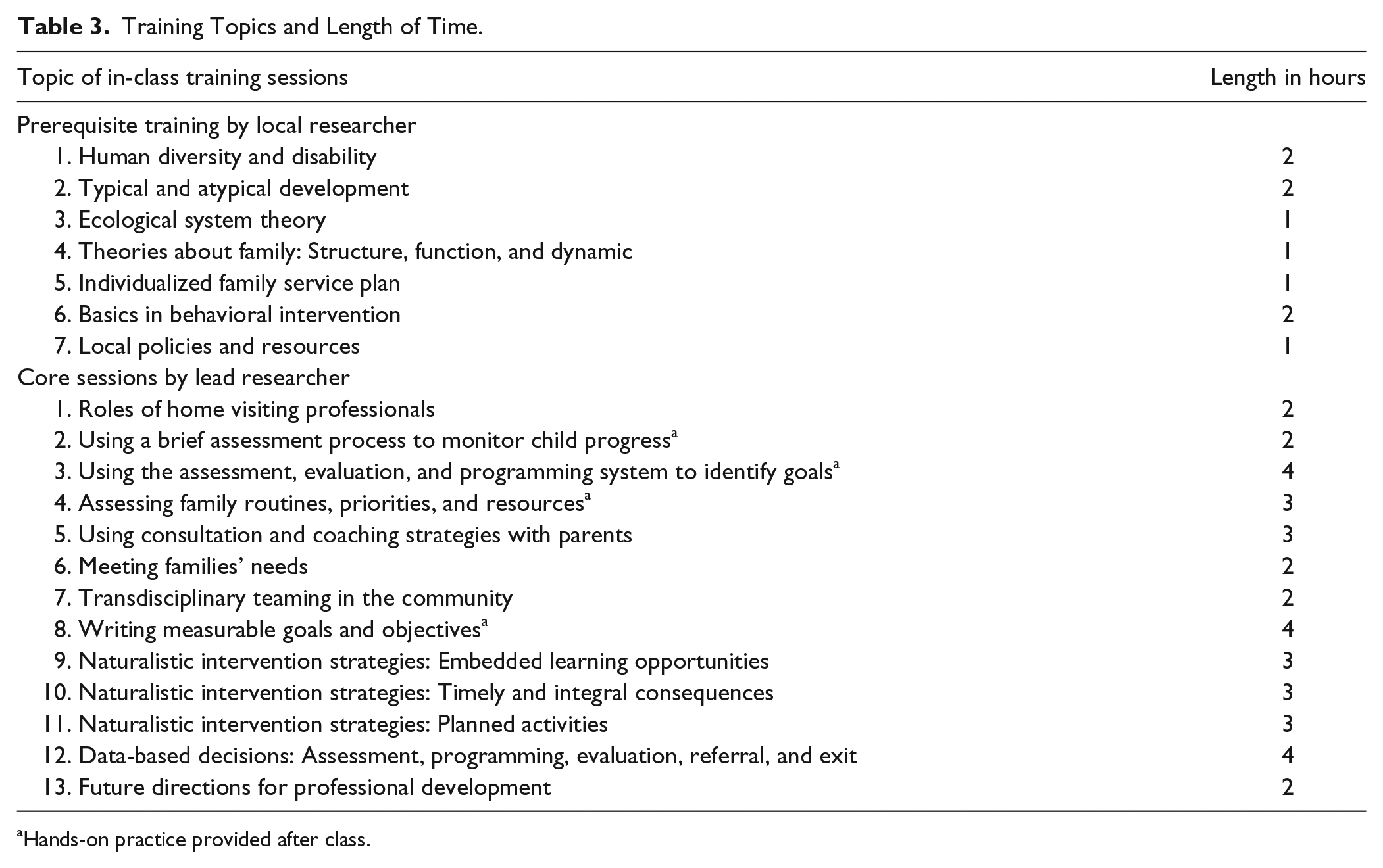
Hands-on practice provided after class.
The format of in-class training included large group lectures and small group discussions. As shown in Table 3, some in-class training sessions were followed by hands-on practice. For example, after training the students on using the assessment, evaluation, and programming system (AEPS; Bricker, 1993/2000; Bricker, 1996/2005), they formed small groups of three to visit a volunteer family with a child with developmental disabilities to practice using the tool during the weekend. When they came back the following week, the whole class shared and reflected on their experiences with hands-on practice. All in-class training sessions (not including the hands-on practice) were video-recorded for future review by trainees.
Supervised practicum
Subsequent to in-class training, there were 15 school weeks for practicum experiences. Twenty-three undergraduate-level student participants participated in these practicum experiences and were divided into six small groups. Each group was assigned to a family of a child aged from birth to 4, who had a diagnosed developmental delay. During the practicum phase, each group conducted a weekly, 1-hr home visit with the assigned family to practice the strategies they learned from in-class training. Meanwhile, the students used consultation and coaching strategies to work with the family in assessing the child’s development, identifying goals, developing plans for home-based intervention, and practicing the skills needed for implementation. Two faculty members and four graduate students were assigned as supervisors to lead the weekly 1-hr reflection and planning meetings with all members of the focal practicum group. The structure of the weekly meeting consisted of a 15-min description of how the home visit plan was implemented in the previous week, a 30-min reflection on the perceived challenges and accomplishments, and ended with a 15-min collaborative planning time for the next home visit.
Based on the practicum students’ needs, the lead researcher provided four additional online support sessions during the 15-week practicum to strengthen specific skills (e.g., naturalistic strategies to support communication development, identifying goals for intervention, developing a data collection system, and using strength-based language). Online support sessions were conducted using a free online conferencing platform provided by Tencent (http://www.tencent.com/en-us/ps/imservice.shtml). Each session contained three components: a 60-min lecture on the topic, a 30-min presentation of examples on how to apply the skills, and a 30-min question and answer discussion. The lead researcher also provided individualized feedback on practicum students’ assignments, including assessment reports, individualized family service plans, parent handouts, data collection forms, and service summaries. Furthermore, the 13 local in-service special educator participants served as consultants to provide information regarding available resources in the community. Some consultants also participated in the online sessions, though not required to, to help answer students’ questions.
Evaluation Procedures
Evaluation Questions
After the first year of implementation, evaluation was conducted to examine the effectiveness of HBEIP. Figure 1 presents the timeline of each training and evaluation procedure. Program evaluation efforts focused on addressing the following questions and informing future development of the program:
How does HBEIP affect the readiness of Chinese participants in delivering home-based EI services?
What kind of supports and resources are helpful to participants in the program?
Which supports and resources are needed for improvement in HBEIP?
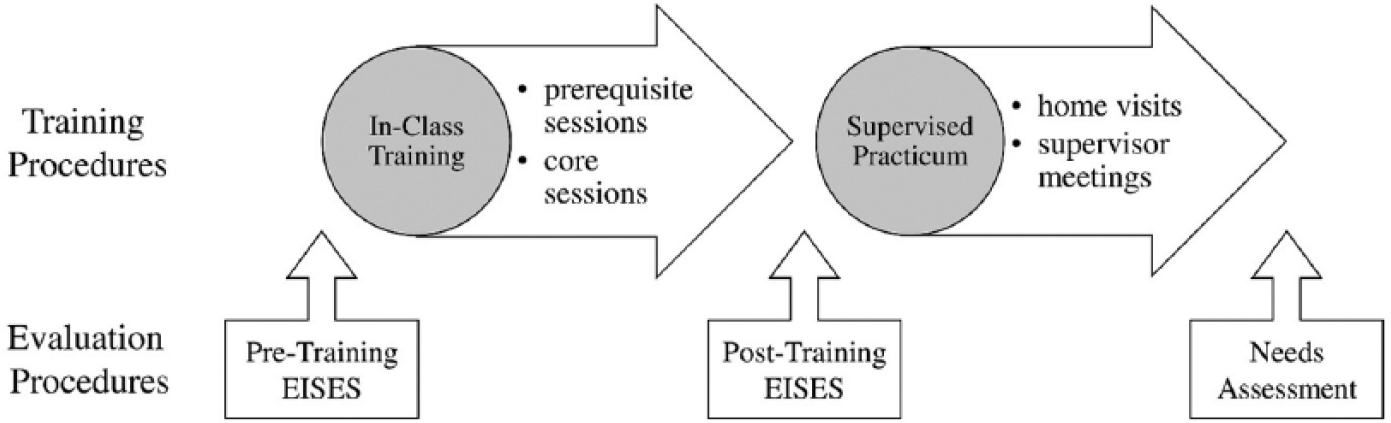
Timeline of the training and evaluation procedures in the first year of HBEIP.
Measures
Early interventionist self-efficacy survey
The project employed the Early Interventionist Self-Efficacy Scale (EISES; Lamorey & Wilcox, 2005) to measure the participants’ self-perceived efficacy as an early interventionist 2 times: a pre-training administration before the prerequisite sessions and a post-training administration after the in-class training and before commencement of the supervised practicum. The EISES is a 15-item questionnaire grouped into two major components that measure the participants’ perception of their personal efficacy (e.g., abilities to offer beneficial services to children and families) and general efficacy (e.g., the sense of the general effectiveness of family-centered EI). Among the 15 items, 10 focus on personal efficacy and the other five focus on general efficacy. The lead researcher translated the survey, and local researchers reviewed it for translation equivalence. A 5-point Likert-type scale was used for rating, ranging from 1 point as strongly disagree to 5 points as strongly agree. Preliminary evidence indicated that the EISES demonstrated sufficient technical adequacy (Lamorey & Wilcox, 2005).
Needs assessment
After the 15-week supervised practicum, the project team developed and implemented a needs assessment to identify needs of HBEIP graduates and to garner suggestions for future HBEIP improvements. The assessment was comprised of three major sections: motivation and gain, support/competency, and areas for improvement. The first section contained a multiple-choice question that asked participants’ purpose in joining HBEIP and an open-ended question asking what they learned during their time in the program. A 5-point Likert-type scale allowed trainees to evaluate the level and type of support received (e.g., week/strong), personal competencies (e.g., prepared/unprepared), and program needs (e.g., not needed/in great need). The survey also included an open-ended question inviting participants to raise other challenges and suggestions not mentioned elsewhere in the assessment.
Data Analysis
Descriptive statistics were computed for the EISES and the needs assessment results. Next, a paired-samples t test of the pre- and post-HBEIP EISES was calculated to evaluate the effects of this intensive workshop. A one-way within-subjects analysis of variance (ANOVA) was used to help interpret the assessment results, as well as items under each category in the “support/competency” and “needs improvement” sections, respectively, to investigate whether statically significant differences would be presented. Finally, answers from the open-ended questions were classified into several thematic categories.
Evaluation Results
Early Interventionist Self-Efficacy Survey
Thirty-eight of 44 participants completed the EISES. Results of descriptive statistics and the comparison between pre- and post-training appear in Table 4. The t-test results indicated that there was a statistically significant difference between total scores of EISES before training (M = 49.97, SD = 5.35) and after (M = 54.24, SD = 6.68), t(37) = −5.47, p < .001. Furthermore, item-level examination showed that eight of 15 items demonstrate statistically significant increases after these trainees completed the HBEIP in-class training. However, when dividing items into the two major components—personal efficacy and general efficacy—all eight of these items pertain to personal efficacy. Pre- and post-training scores of general efficacy and each of the five items under this component were not significantly different. A full list of EISES items can be obtained from http://hbeip.blogspot.com.
Descriptive Statistics and Paired-Samples t Tests of the EISES (n = 38).
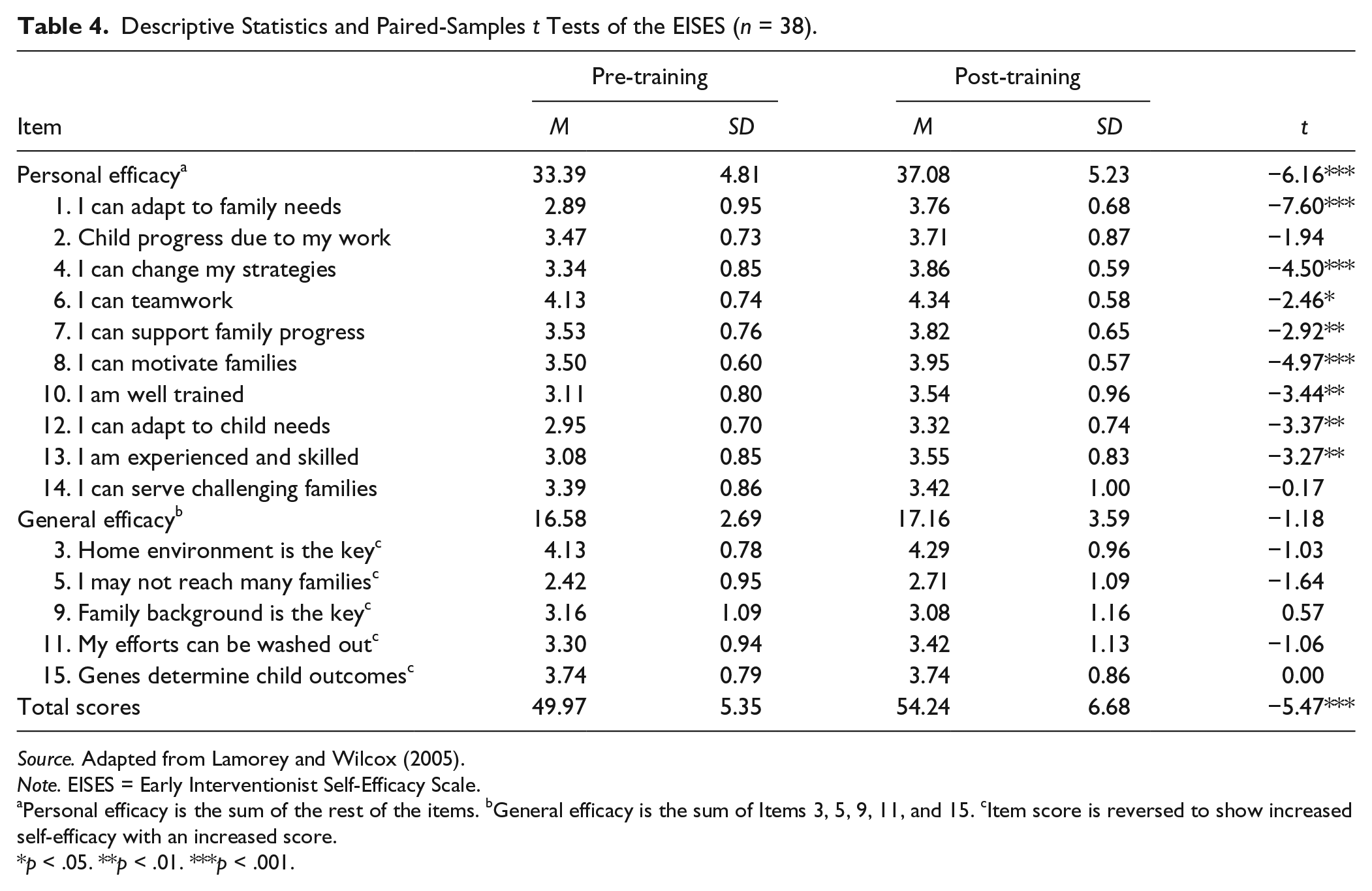
Source. Adapted from Lamorey and Wilcox (2005).
Note. EISES = Early Interventionist Self-Efficacy Scale.
Personal efficacy is the sum of the rest of the items. bGeneral efficacy is the sum of Items 3, 5, 9, 11, and 15. cItem score is reversed to show increased self-efficacy with an increased score.
p < .05. **p < .01. ***p < .001.
Needs Assessment
Motivation and gain
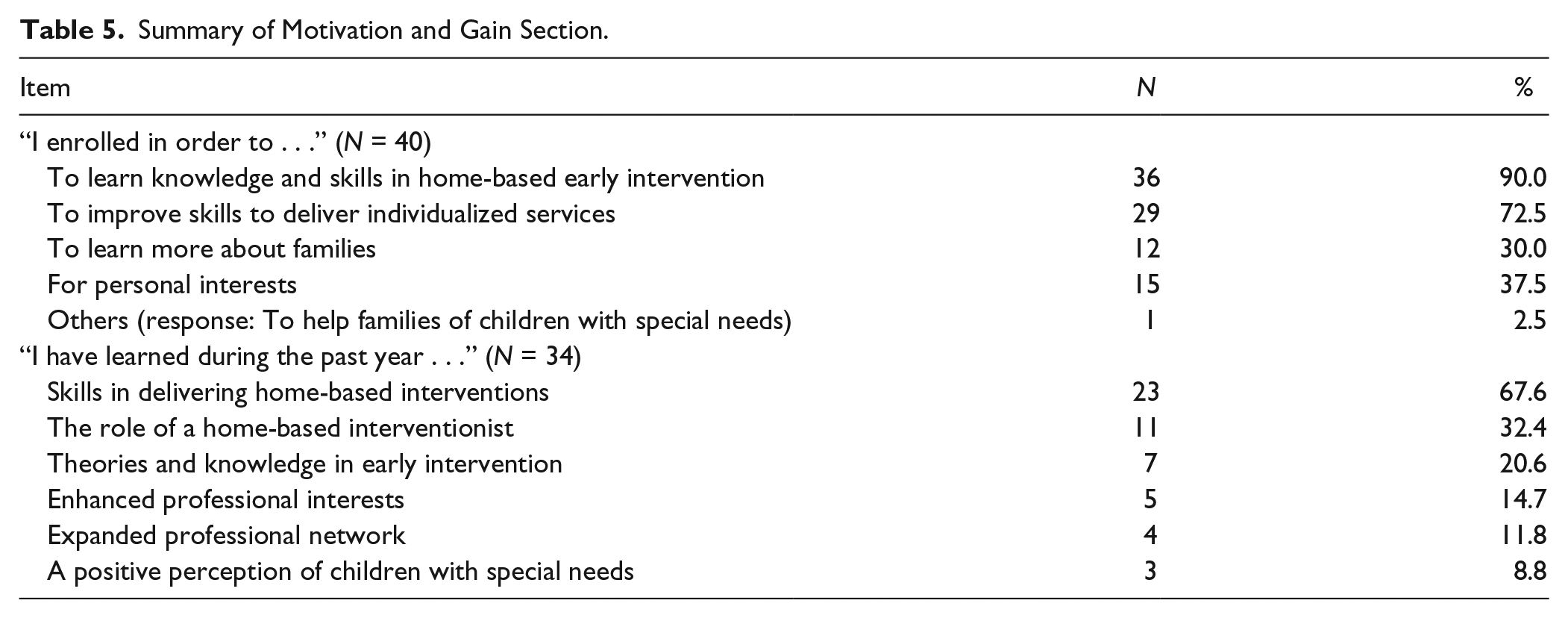
Forty of the 44 participants completed this three-part needs assessment. Results of the motivation and gain section are summarized in Table 5. Thirty-six (90.0%) participants reported that they enrolled in HBEIP to learn knowledge and skills in home-based EI. Twenty-three (67.6%) participants responded to the open-ended question about their gains, reporting that they have learned the skills in delivering home-based interventions in the first year of HBEIP. Interestingly, only 8.8% participants wrote that they have gained a positive perception of children with special needs.
Summary of Motivation and Gain Section.
Perceived supports and needs
The descriptive statistics and ANOVA results of the support/competency section are presented in the middle column in Table 6, with the results of the needs improvement section shown in the column on the right.
Descriptive Statistics and One-Way ANOVA Results for Needs Assessment in HBEIP (N = 40).
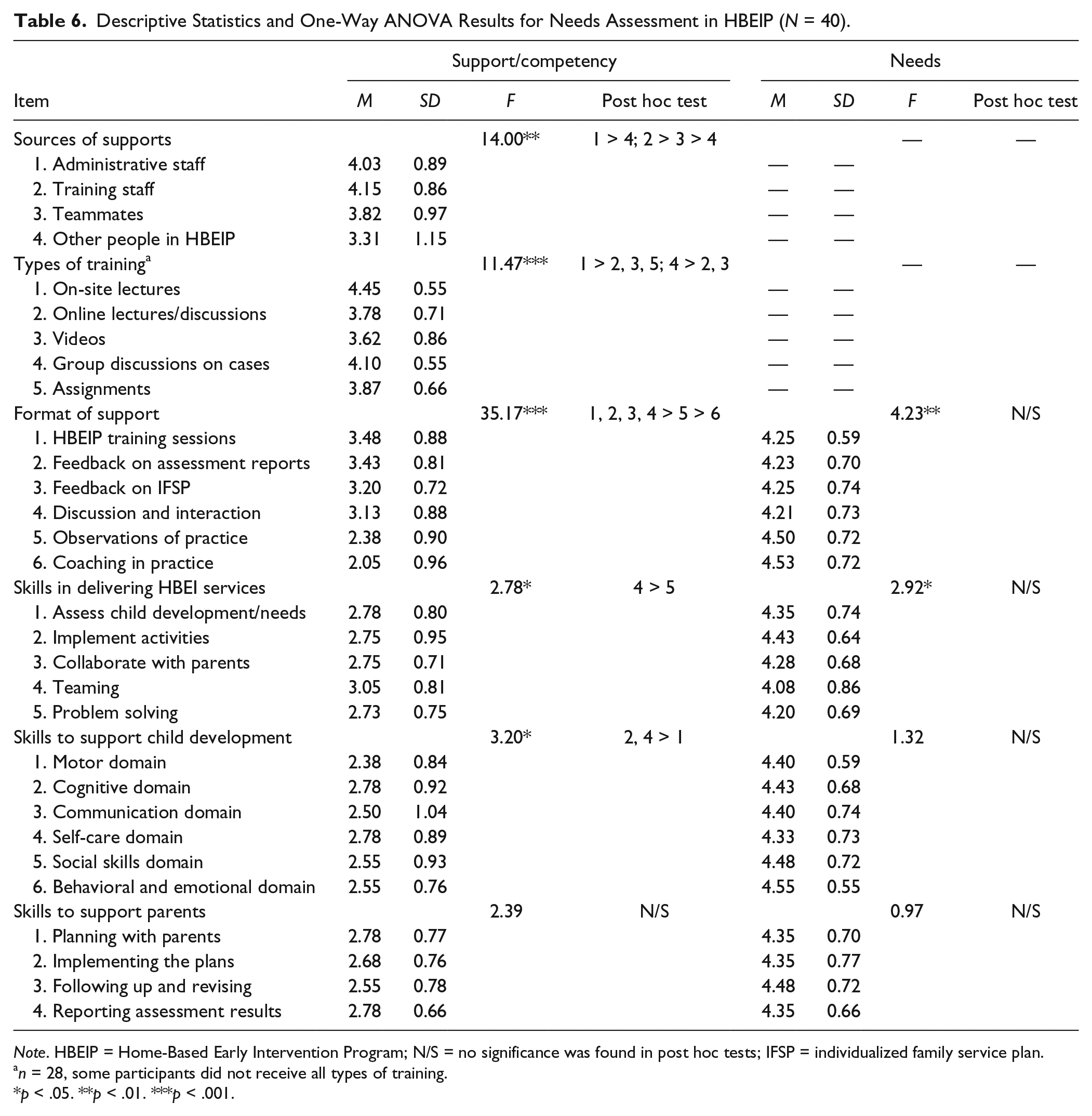
Note. HBEIP = Home-Based Early Intervention Program; N/S = no significance was found in post hoc tests; IFSP = individualized family service plan.
n = 28, some participants did not receive all types of training.
p < .05. **p < .01. ***p < .001.
Overall, participants reported having received strong to very strong support from the training staff (M = 4.15), including the lead researcher, the local researcher, and supervisors, as well as from the administrative staff (M = 4.03). Results from post hoc tests indicated significantly stronger supports from administrative staff than from teammates, and that the perceived supports from training staff were significantly stronger than supports from teammates and other people in HBEIP (e.g., the consultation panel of in-service professionals).
Participants rated on-site lectures as the most effective (M = 4.45) out of five types of training, followed by group discussions based on cases (M = 4.10). Post hoc tests indicated that the perceived effectiveness of on-site lectures was significantly higher than that of online lectures/discussion, videos, and completing assignments, and that group discussions on their practicum experiences was significantly more helpful than online lectures/discussions and videos.
Among six major formats of support, training sessions were rated as the most helpful to participants (M = 3.48). In post hoc tests, observations of modeled practice and coaching were found significantly weaker than other formats. These two formats were also rated to have the highest needs for improvement, although no significant results came up from post hoc tests.
Participants reported being most skillful in teaming with other group members (M = 3.05), which is significantly stronger than their perceived problem-solving skills (M = 2.73). They generally reported high needs to improve their skills (M = 4.08–4.35); no significant result came up from post hoc tests.
In terms of skills to support child development, again, participants reported generally low level of perceived competency (M = 2.38–2.78). Specifically, motor area was rated as having received less support (M = 2.38) than cognitive domain (M = 2.78) and self-care (M = 2.78). Needs for improvement were also high across all skills (M = 4.33–4.55), although no one area was found significantly higher than others.
Similarly, all four categories of skills to support parents were reported low in competency (M =2.55–2.78) and high in needs for improvement (M = 4.35–4.48). No significant difference was found in post hoc tests.
Open-ended question
Thirty-four participants provided 41 comments to the open-ended questions on other challenges and suggestions not mentioned above. Time limitation was reported by 13 participants as a barrier to meaningful participation in the program. Lacking supports in practicum was identified by 12 participants. Five participants commented on challenges in implementing intervention plans (e.g., collaborating with the focal family, monitoring child progress), and another four participants reported specific challenges collaborating with the focal family (e.g., in scheduling a visit and identifying practical intervention goals). Five participants reported difficulties in teaming (e.g., scheduling a team meeting); two other participants wrote about needing more training on the theoretical foundations for the intervention skills that they learned and practiced.
Discussion
With the intention of introducing family-centered practices to China as a pioneering international project, HBEIP aimed to teach EBP to current pre-service and in-service teachers who serve young children with special needs and their families. During the first year of implementation, the research team adopted and translated several Western-developed intervention practices for use in Guangzhou, China. The infrastructure of HBEIP was established at SCNU, including recruitment criteria and procedures, training lessons and materials, supervised practicum system, and the role of program coordinators. The research team implemented HBEIP and evaluated it for the first cohort of participants. Feedback from participants provided preliminary evidence for the cultural responsiveness and utility of the program. Results from formative evaluations informed future directions for improvement and sustainability.
Question 1: How Does HBEIP Affect the Readiness of Chinese Participants in Delivering HBEI Services?
Results from the EISES surveys showed a statistically significant gain in the overall level of self-efficacy after participants completed HBEIP in-class training; participants felt that they had the knowledge and skills necessary to provide needed supports to young children and their families. This finding indicated that the 3-week in-class training had a positive effect on participants’ confidence in their ability to produce desired outcomes for children and families. It is interesting that although significant increases were found in eight targeted skills and the total score of the EISES, no significant differences were found in two personal efficacy items and for all five general efficacy items. As defined by the developers of the EISES (Lamorey & Wilcox, 2005), general efficacy items measure early interventionists’ perception of how children’s individual and ecological risk factors affect outcomes after receiving EI. The lack of improvement on general efficacy items may be explained by the low percentage of reported gains (3, 8.8%) in “a positive perception of children with special needs.”
Besides the general efficacy items, two personal efficacy items did not show significant improvement. The first one describes, “When a child shows improvement, it is because I have been effective in facilitating the family’s ability to support their child’s development.” By the time the participants completed the post-training EISES survey, they had not had experience applying the skills in practice and evaluating the effectiveness of their practice. It is reasonable that their confidence level on this item remained the same before and after training. The other item, Item 14, states, “If I really try, I can get through to even the most challenging families.” As newly trained early interventionists with very limited in-field exposure, even though the participants were introduced to children and families with a wide range of needs during the training, they might still not feel confident working with “the most challenging families.”
After completing a supervised practicum, results from the needs assessment indicated not only some level of gains for participants but also needs for improvement. Most participants who responded to the open-ended question reported that they learned knowledge and skills for delivering home-based EI, which matched with their initial purpose of enrolling in HBEIP. However, results from the other sections in the needs assessment showed that participants generally felt they had insufficient skills and knowledge for supporting children and families. One interesting finding was that the participants reflected anecdotally on their gains in other non-targeted areas, such as their expanded professional network connections and their increasingly positive perception of children with special needs.
It is noteworthy that only 8.8% participants mentioned having developed a positive perception of children with special needs. As an early interventionist, it is important to develop a positive and healthy attitude about disability and an understanding of diversity in child development. This low percentage of reported gain may be explained by the fact that most training topics in HBEIP focused on teaching and learning practical intervention strategies (e.g., “Assessing Family Routines, Priorities and Resources”), with relatively less efforts to challenge and question the stigma that traditionally related to disability.
Even though HBEIP seemed to produce positive effects on the trainees’ competencies in delivering family-centered practices, the trainees appeared to be more conservative in self-ratings of their knowledge and skills for working with young children with disabilities and their families. Although the two surveys asked different questions about ECI competencies, the lower ratings of the needs assessment results could be viewed as an indication of trainees’ realizations about the types of skills and knowledge they needed to improve having real-life experiences. This finding also informed the research team about the importance of providing continuous support (e.g., building a community of practice, helping trainees develop a positive view about disability, and coaching in practice) to the trainees to produce a high-quality home-based EI workforce (Dunst, 2015).
Question 2: What Kind of Supports and Resources Are Helpful to Participants in HBEIP?
HBEIP participants positively rated supports from trainers, administrators, teammates, and other related professionals (e.g., in-service consultants). Students gave higher ratings to on-site, large group lectures than to more individualized training approaches, such as assignments (with individualized feedback provided by the trainer), small group discussions (focusing on specific cases with which the participants were working), and online training (small groups focusing on student-chosen topics). Similar results appeared in the ratings of different formats of support: Large group training worked better than more individualized supports (e.g., observations and coaching). Participants may have given higher ratings for the on-site lectures and the large group training sessions because these were provided by the lead researcher, who is a licensed early interventionist with extensive knowledge, skills, and experiences in home-based EI. Local faculty members and in-service special education teachers who had little background or experience serving young children in a home setting provided other sessions, such as observations and coaching sessions. Given that home-based EI services have been instigated in China, perhaps it is necessary to adopt a “train-the-trainer” approach to ensure dissemination and sustainability of HBEIP (Green, 2005).
Question 3: What Kind of Supports and Resources Are in Need of Improvement in HBEIP?
The major needs for improvement reported by participants in HBEIP were the lack of opportunities to observe how the learned strategies are applied in real settings and the chance to receive feedback in their practice settings. The low ratings might be attributed to limited personnel, time, and system support. Practicum participants were supervised by professionals who, though experts in school-age special education, had very little or no experience working with young children and their families. Recruitment of supervisors for HBEIP practicum experiences was a challenging task because ECI services are typically provided by medical professionals in clinical settings, and the special education professionals were not familiar with an innovative model such as HBEIP.
It is also noteworthy that only 8.8% of participants reported gaining a positive perspective about children with special needs. As HBEIP was a new initiative and the first-year training topics primarily focused on practical intervention strategies, it was likely that the participants had limited understanding of influential genetic and environmental factors in child development, and remained skeptical about the effects of EI due to social stigma and stereotypes of disability. In the future development of HBEIP, it would be beneficial to add new topics that addressed the need for participants to acquire accurate knowledge about disability and evidence for the effectiveness of EI, as well as to help them develop a positive image of children with disabilities.
In addition, some participants, especially those who were in-service professionals, had limited time for practicing learned skills and strategies due to the existing workload required in their programs. After the in-class training, in-service professionals were not able to continue to fully participate in practicum experiences. Instead, they indirectly participated by providing occasional consultations for college students. Limitation of time was also reported as one of the major barriers by college students. In addition to their daily responsibilities as full-time students, they voluntarily spent their spare time participating in HBEIP practicum experiences. Overall, as a pilot project, HBEIP had not been integrated as part of the teacher training program at SCNU or in local special education schools, a situation that might have resulted in inconsistent implementation of practices. Significant amount of efforts will be needed at the administrative level to ensure and allocate the resources and supports required for a sustainable implementation of HBEIP, as defined as “systems innovations” in the implementation framework (Fixsen et al., 2005). For example, if HBEIP training could be listed officially as an in-service professional development course of the Special Education Department at SCNU, in-service professionals would register for credit hours, and this will help ensure their full program attendance.
In light of the positive reviews received from HBEIP participants, as well as their need for more in-practice supports, the research team has already made minor changes to the program, including providing specific training for supervisors, applying for more funding resources, and developing supervision routines for practicum experiences. The team has also planned follow-up workshops that will focus on specific topics of interest for the first cohort of graduates. This first-year implementation has provided firsthand experience of effective practices and directions for improvement for the program. The following section provides implications to the field, especially for other researchers who are also interested in introducing and implementing high-quality intervention models to countries and areas with limited resources.
Limitations
This preliminary study had several limitations. First, the sample size was small. The number of participants in each group (undergraduate students, graduate students, faculty members, and in-service professionals) was not sufficient to examine the differences in responses between groups. In addition, trainees volunteered to participate in the study, and this self-selection could have compromised generalizing the findings to other populations. Second, varying amounts of practicum time for each participant might have affected their perceived experiences and needs. Third, the challenge of finding highly qualified supervisors may have affected trainee learning. Finally, there is no technically adequate assessment tool currently available in China that could be used to measure the outcomes of EI practices for children with special needs and their families, and as a result, such outcomes were not measured in this study. Future research should focus on examining the relation between improved competency of interventionists and positive child and family outcomes.
Implications
The findings from this study, although preliminary and on a small scale, do provide four invaluable implications for future practice and research. First, trainees rated the current training model highly, which echoed previous findings that a combination of lectures, fieldwork, and ongoing support can effectively prepare these professionals to carry out EBP (Dunst, 2015). Likewise, besides equipping the trainees with core competencies for working with young children with special needs and their families, additional opportunities with different types of practices should be provided for trainees to observe, implement, and be observed. Second, further training on supervision and coaching should be developed to ensure that the supervisors and coaches are content experts, and to maximize their use of effective strategies and high-quality, constructive performance feedback to trainees. Third, system changes in China are needed. The integration of the training program into a personnel development system will increase participation as well as the program’s sustainability. Most important of all, such integration will help pre-service and in-service professionals receive adequate training to work in ECI and should promote positive outcomes for young children with special needs and their families. For HBEIP, the next step will be advocacy for its integration into the curriculum framework of the Special Education program at SCNU and the teacher training requirements of local special education schools. These changes will eventually lead to a full implementation in Guangzhou as well as other cities in China.
For researchers focusing on international implementation of personnel preparation projects, this study provides an example of the process and potential challenges that arise when introducing a new service model in a different country. Findings from the present study suggest that an implementation science framework may be applied in an international context, with additional attention to language and cultural adaptations. Under each stage of implementation, international researchers should evaluate the needs and supports required in each stage of implementation, embed collaborative efforts from international and local researchers to address cultural responsiveness, as well as apply a data-driven model to guide decisions for the next steps.
Conclusion
The purpose of HBEIP was to develop a model for preparing early interventionists in using family-centered strategies to support young children and their families in China. As the findings of this study indicated, HBEIP increased trainees’ self-efficacy as an early interventionist, as well as needs for improvement on their knowledge and skills. Even though further scale-up investigations on child and family outcomes are needed, the evaluation results of HBEIP provide evidence for effective adaptation and successful introduction of family-centered practices in China, and enlighten the possibility of continuing and expanding such training program. Subsequently, the goal is to build a high-quality, competent workforce in ECI that promotes positive outcomes of young children and their families.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.