
Abstract
This article begins by considering how current models of vulnerability do not adequately capture situations arising from physical, cognitive and behavioral impairment. Using specific examples and prior studies, three dimensions – ability to remediate, duration, and stability of the underlying challenge – are suggested to enhance our understanding of situations that lead to vulnerability. As these dimensions are explored, four categories are proposed for such situations: Straightforward Resolvable, Complex Resolvable, Straightforward Unresolvable, and Complex, Dynamic Unresolvable. These categories are leveraged in the discussion of the embodied consumer to develop propositions related to the likelihood someone will experience vulnerability in a given situation. We also address how the experienced vulnerability of one person ripples outward to create secondary vulnerability in his/her social network. After using these categories to understand how various impairments may lead to vulnerability, we then focus closely on how specific physical, cognitive and behavioral impairments limit market choice and market flexibility. Normative market expectations regarding the body and its cognitive capacity present fertile ground for exploring consumer agency and how actors relate to one another in the market. Theoretical propositions, as well as broader areas of inquiry, are developed to help identify areas for future research.
The existing marketing literature on vulnerable consumers is wide-ranging in the settings in which it explores vulnerability. For example, vulnerability in the marketing literature includes people in a community hit by a natural disaster (Baker, Hunt, and Rittenburg 2007), cognitively normal but low literacy adults (Adkins and Jae 2010; Adkins and Ozanne 2005; Ringold 2005), new mothers (The VOICE Group 2010), consumers in multicultural marketplaces (Broderick et al. 2011), those grieving the loss of a loved one (Gentry et al. 1995), and refugees, orphans, the elderly, and citizens of impoverished third world countries (Shultz and Holbrook 2009). Policy makers, social activists, and marketers desire a coherent framework to understand the range of situations leading to consumer vulnerability so they may better understand how policies and procedures impact aspects of vulnerability in the market. However, the marketing literature on vulnerability often overlooks people with significant chronic or progressive disability although many people live with these challenges.
The United States Census Bureau (Brault 2012) reports 31% of the U.S. population as having a disability with 13% of these classified as severe; approximately 4.5% of U.S. citizens over 6 years old require assistance in activities of daily living. A different survey estimated there are 65.7 million adults in the United States who provide unpaid, informal caregiving to someone with special needs (National Alliance for Caregiving and AARP 2009). This same survey estimates that more than 30% of all U.S. households provide care to someone with special needs. The number of consumers with a disability, or those in relationship with such people, dwarfs those in other situations leading to vulnerability in the U.S. and other developed countries. The United Nations estimates about 720 million people worldwide have some level of disability and about 100 million experience “very significant difficulties” (World Health Organization 2011). Overall, this suggests that, on a worldwide basis, attention to disability and its impact on able-bodied consumers is warranted.
Disability as a forum for exploring vulnerability is interesting for several reasons: in the case of significant disability, dependency on others for physical and communication needs extends the potential for vulnerability into the group of caregivers; embodied challenges clarify dimensions of vulnerability related to duration and ability to remediate; and a close inspection of cognitive, behavioral and physical disability helps reveal where current market approaches to impairment-related vulnerability may fail their intended targets. This article advances understanding in each of these areas, adding dimensions that can be applied to all situations leading to vulnerability, as well as a more targeted analysis of the vulnerability that comes from inhabiting a body that fails normative expectations.
How Do We Think about Vulnerability and What Do Current Models Overlook?
In response to a literature that uses the term vulnerability in many different settings, Baker, Gentry, and Rittenburg (2005) propose boundaries for what is and is not real (as opposed to perceived) consumer vulnerability. Among the characteristics associated with potential vulnerability they delineate are individual characteristics (e.g., cognitive capacity), individual states (e.g., grief), and external conditions (e.g., stigma). Central to their consumer-driven definition of vulnerability is the question of control, with less control (over interactions, outcomes) being associated with higher vulnerability. Succinctly, they define vulnerability as “a state of powerlessness that arises from an imbalance in marketplace interactions [deriving] … from the interaction of individual states, individual characteristics, and external conditions” (p. 129) (emphasis in original). In this definition, while everyone has the potential to be vulnerable, vulnerability is not an automatic by-product of an individual state, characteristic, or external condition; it must include an experiential element of the consumer being powerless to achieve a market goal. With regard to groups often painted with a broad brush as vulnerable, such as the homeless, they conclude that, “although some classes of people are more likely to experience vulnerability, that does not mean that people in those classes are always vulnerable” (p. 137) and with appropriate support and market systems they may transition out of vulnerability. Baker, Gentry, and Rittenburg (2005) call for policies to “empower consumers and facilitate the movement away from vulnerability,” but remain silent on consumers who are unlikely to move from vulnerability and who may become increasingly vulnerable (e.g., progressive neuromuscular disease such as ALS). This issue is one of the concerns of this research.
Baker (2009) and Baker and Mason (2012) describe the approach as detailed in Baker, Gentry, and Rittenburg’s (2005) and Shultz and Holbrook (2009) (explored in more detail in the next paragraph) as a situational definition of vulnerability. The 2009 and 2012 studies hold that the situational approach is more accurate for assessing any one person’s vulnerability, but acknowledge the situational approach lacks generalizability. Commuri and Ekici (2008) suggest using the terms class-based (for the demographic descriptions of someone likely to be vulnerable, e.g. visually impaired) and state-based (the personalized resources and experiences this person brings to the class situation rendering him/her personally vulnerable or not). Commuri and Ekici also acknowledge the theoretical and policy hurdles to a state-based approach (there are potentially as many states as there are people), but support its use in conjunction with the class-based approach. Nested within the discussion of situational vulnerability, or state-based versus class-based vulnerability, is the notion that vulnerability can be lessened or ameliorated with the right combination of resources and support. Of interest herein are people for whom the situation leading to vulnerability will likely never disappear. For people in this situation, a degree of dependency on others (often family and friends) is necessary. As a result of this on-going dependency, we are also interested in the secondary level of vulnerability that may be engendered in the support group. That is, we are also interested in people who may otherwise not be in a class considered vulnerable except through relationship.
Shultz and Holbrook (2009) propose a model to help organize the “evolving and emerging articulation of consumer vulnerability.” Their model provides a macro perspective that identifies powerlessness in an interaction as flowing from two sources: knowledge of how to solve a problem and access to the means of solving the problem. In this typology, people who do not know how to solve their problem and who have no means to solve it are deemed doubly vulnerable; people are economically vulnerable if they know what to do but do not have the resources (i.e., money, geographic location, transportation); people are deemed culturally vulnerable if they have resources, but do not know how to solve the problem; and the invulnerable are defined to have both the knowledge and the means to address the challenge they face. Following their model, vulnerability is fluid, situational and experienced at some point by everyone. Interventions and education may reduce vulnerability, but reversals of fortune, less-than-forthright marketing, even personal idiosyncrasies (such as an inability to navigate a website for information), can move one from invulnerability to one of the other states. The Shultz and Holbrook (2009) model implies that the situation leading to vulnerability can be solved in some manner, raising the issue of what this means for someone with a significant or progressive physical, cognitive, or behavioral impairment.
For example, in Shultz and Holbrook’s (2009) model, the description of cultural vulnerability says, “People are culturally vulnerable if they have plenty of resources to acquire what they need but just do not know what is good for them” (p. 125), and economically vulnerable if “they know what is good for them but do not have the abilities, skills, funds, or other resources needed to acquire it” (p. 125). But, how would one place someone with intractable addiction in this paradigm? Most addicts do know what is good for them; some even have plenty of resources. Sometimes, knowledge and resources are not enough. Or, consider the case of anosognosia (a condition in which a person who has an impairment seems unaware of the existence of his/her disability). Someone may agree that a person with dementia should not handle his/her own finances, but may be unable to recognize his/her own dementia. This person knows what is good for a particular condition but is not capable of seeing himself/herself as having that condition. No amount of education can overcome the anosognosia. Both these examples point to the idea that some vulnerability is tied to a failing organic system and may not be captured fully in current theoretical models. Further, when someone has a failing body, it is common for someone else to support/make these decisions for the person, potentially extending the potential for vulnerability to others.
For example, a working adult in the U.S. with a steady income stream, who is healthy, literate, and so forth, may be vulnerable as she tries to manage the day-to-day needs of an ailing parent who lives at a distance. To use the distinction outlined by Commuri and Ekici (2008), the parent is in the class of ailing elderly (with some degree of physical, cognitive or behavioral impairment), and then, through relationship, the adult child is in the vulnerable class of adult-children-trying-to-help-at-a-distance. Both the parent and the child are in vulnerable states, albeit different ones. The parent may never leave the vulnerable state; the child may cycle in and out of vulnerability as circumstances change.
The notion that the consumer vulnerability of a group may flow from the vulnerability of one of its members is an extension of the idea of stigma by association (Goffman 1963). Stigma by association occurs when the stigmatizing attribute of one member of the group spreads to everyone with him/her. Stigma by association has been documented in many settings, such as obesity (Hebl and Mannix 2003) or sexual orientation (Neuberg et al. 1994). We enhance to vulnerability theory by considering the vulnerability others experience as a by-product of being in a relationship with someone who has a physical, cognitive and/or behavioral impairment (see also Burke 2007; Burke and Parker 2007; Goldstein and Johnson 1997; Mason and Pavia 2006; Pavia and Mason 2012; Werner and Heinik 2008).
Vulnerability as a Function of Ability to Remediate, Duration and Dynamism
Turning to the embodied consumer, an inspection of situations related to physical, cognitive, and behavioral impairment raises three dimensions that can be used to further organize vulnerability research in marketing. The first dimension is whether the situation leading to vulnerability can be remediated (e.g., illiteracy) or not (e.g., dementia). The second is dimension whether the situation leading to vulnerability has a clear end point in the near future or not (e.g., a broken arm versus an amputated arm). These first two dimensions are intertwined, of course; if the situation leading to vulnerability cannot be remediated, then it is not going to resolve in the near future. On the other hand, if the situation leading to vulnerability can be remediated, this does not necessarily mean it will be remediated. The third dimension is whether the situation leading to vulnerability is static in its challenges (e.g., loss of an eye) or dynamic (e.g., progressive vision loss).
Regarding the dimension of whether the situation leading to vulnerability can be remediated (the first part of Table 1), so far, neither policy making nor health advances can reverse dementia, eliminate traumatic brain injury, remove autism spectrum disorder, or stop pulmonary fibrosis. Other situations leading to vulnerability, such as illiteracy, can be improved but only through significant effort on someone else’s part. Still other situations leading to vulnerability, such as a broken arm, can resolve after an initial intervention with the passage of time. Forward thinking societies make a large effort to provide the quick fixes (like setting a broken bone) that bring members out of vulnerability given sufficient time. Most societies make an effort to remediate poverty, inequality, and illiteracy, but exceedingly complex problems often suffer from resource constraints. Social marketing and macromarketing often focus on vulnerabilities that might be remediated with tactical or sustained coordinated efforts. In situations of vulnerability whereby the underlying cause cannot be remediated, policies for the vulnerable person are oriented to ensuring some autonomy, safety and providing access to care. But the underlying class of vulnerability is not treated itself. And then there is a secondary vulnerability that comes from being part of the support group for the impaired individual, which may not be addressed by policies at all.
Ability to Remediate, Duration and Dynamism as Dimensions of Situations Leading to Vulnerability.
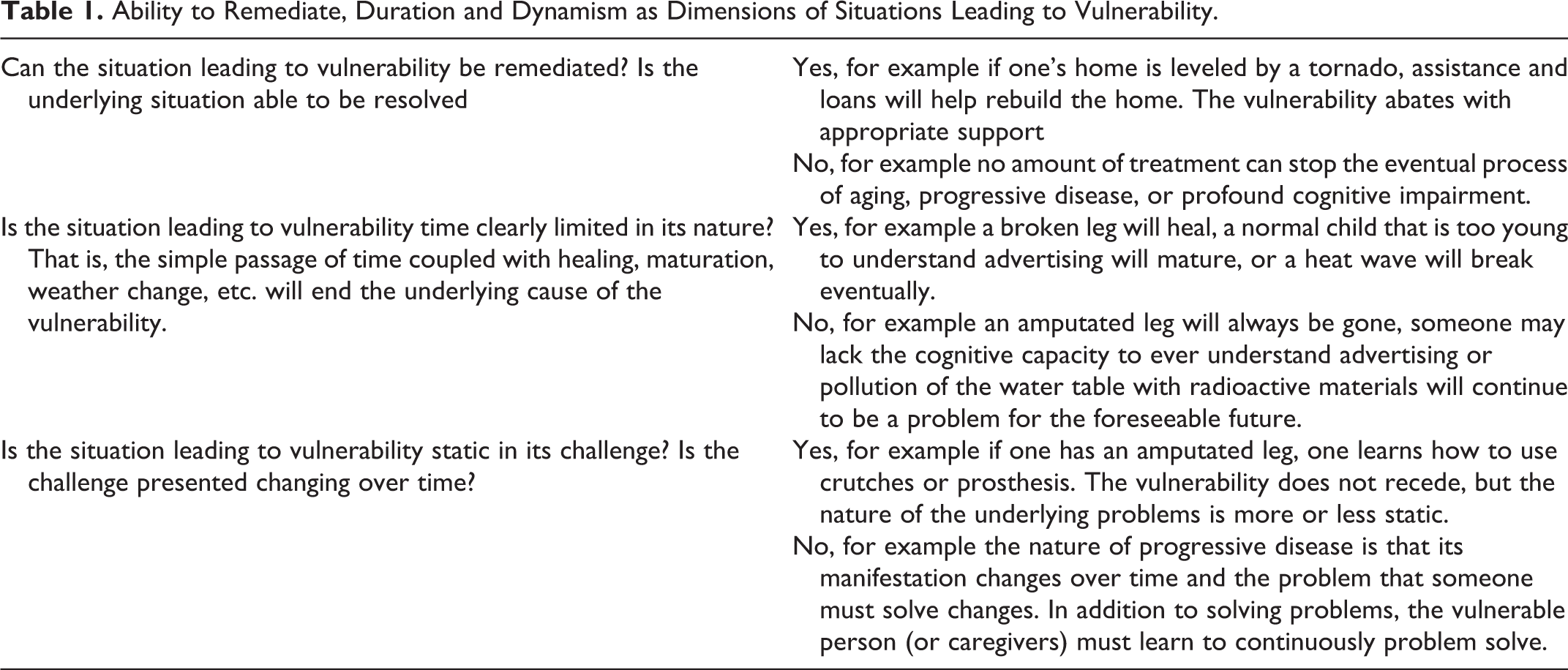
Regarding the time dimension (the second part of Table 1), macromarketing challenges increase as the duration of the situation drags on. A notable amount of the marketing literature on vulnerability focuses on time-limited vulnerabilities (e.g., natural disaster, see Baker, Hunt, and Rittenburg 2007). These vulnerabilities require coping skills and support to help the person “get through” the challenge. Policies, community support, and education are often geared towards information on how to fix what is broken, how to tread water until things resolve, or temporary accommodations until things are back to normal (e.g., a time-limited handicap parking pass). On the other hand, when a situation leading to vulnerability stretches on indefinitely, the individual, and those in a support relationship with him/her, look at market challenges differently. If someone is in a wheelchair for a matter of weeks, she may be willing to forgo driving and delegate tasks to those who support her. But if the wheelchair is permanent, coping may mean permanent changes to her physical environment, such as moving to accessible housing near accessible mass transit. Policies, community support and information for people with permanent impairment are geared toward how to regain one’s life given these limitations, but the monetary support for enacting many adaptations is slim and most individuals rely on an informal extended support system.
Regarding the dynamism dimension (the last part of Table 1), the dynamic component of the underlying vulnerability increases the need for problem-solving, information-seeking, self-reliance, accommodation, and negotiation (Duhacheck and Oakley 2007). For example, if one has eye damage that is stable, then investing in magnifiers, specialized software, and electronic readers not only solves the problem, it solves the problem in a long term way. However, if the challenges are constantly changing, then the motivation moves away from just finding a way to address the immediate challenges and becomes one of finding a way to solve problems. That is, instead of seeking information on a particular problem, people begin to seek information on how to seek information. From a macromarketing perspective it is more straightforward to address vulnerability when the need is static. For example, if lack of transportation prevents children in a particular district from attending school, this problem could be addressed with free bus service. But suppose transportation is a problem, a part of the town is flooded, and a local manufacturing plant closes, laying off some parents. It is more difficult to design a safety net of policies and support for the school children that is effective for an idiosyncratic, changing set of needs.
As shown in Figure 1, these three dimensions (ability to remediate, duration, and stability of the underlying challenge) can be combined in four ways to classify situations leading to vulnerability and to see how disability fits into this mix.

Situations leading to vulnerability as a function of ability to remediate, duration, and dynamism.
Straightforward Resolvable
These are situations leading to vulnerability that can be remediated with a targeted fix, resolving in the near term. These situations present a largely static challenge, such as a broken bone, stolen wallet, or flooded home. The macromarketing challenge is to provide adequate communications so that when someone experiences this situation, he/she understands and locates the needed intervention and moves back to his/her normal state of non-vulnerability in a timely manner. Short term support may be needed while the necessary time passes until non-vulnerability emerges.
Complex Resolvable
These are situations leading to vulnerability that can be remediated although it takes ongoing effort. The resolution may occur in the future, but the remediation effort will have to endure to assure resolution. The challenge is fairly static, for example, illiteracy or bankruptcy. The macromarketing challenge is to help identify the vulnerable and develop enticing programs that can sustain interest and provide desired outcomes. For some of these situations, the challenge is complex and multifaceted, for example, breaking the cycle of multi-generational poverty. The macromarketing challenge in these cases is to understand the broader system and its interrelated parts, to identify the elements with the greatest leverage to help change the system;,to help develop effective programs, and to help ease transitions.
Straightforward Unresolvable
These are situations leading to vulnerability that cannot be remediated and as a result are likely to endure without an endpoint, although the challenge that is presented is static. An example of this is hearing impairment or being unusually short or tall. The macromarketing challenge is to foster systems, technologies and structures that allow people with these challenges to seek and choose the adaptations that provide as full an experience of the market as possible, and, ideally, move into non-vulnerability.
Complex, Dynamic Unresolvable
These are situations leading to vulnerability that cannot be remediated and as a result will endure, but the challenge they present is changing, frequently in a way that increases the likelihood of vulnerability. For example, one may have increasing drug addiction, dementia, or progressive disease. This category is dominated by vulnerabilities that are associated with the body. The macromarketing challenge is largely one of protecting the increasingly vulnerable person while maintaining his or her rights, and finding ways to support the cast who, in turn, provides support to the vulnerable member.
Integrating These Categories in Existing Vulnerability Theory
Considering these four types of vulnerability from the perspective of Shultz and Holbrook (2009), the macromarketing challenge raised by vulnerability in most cases is to increase cultural knowledge (e.g., access to someone who can set a bone, information regarding how to repair flood damage, who to contact for a reading program) and to coordinate economic support (e.g., health insurance, disaster relief, welfare, or child care). Broadly speaking, economic and cultural vulnerability are higher when the underlying situation is more complex and enduring. From the perspective of Commuri and Ekici (2008), various classes sit within the four different categories. The extent to which any individual experiences vulnerability within a category depends on individual resources or, in Commuri and Ekici’s terms, the individual’s state. However, scarce individual resources are often part of the attributes of Complex Resolvable (outside funding is needed to help the person eventually develop his/her own resources) and Complex, Dynamic Unresolvable (ongoing outside funding is needed as vulnerability persists/increases). This suggests that some categories are more likely to be associated with experienced vulnerability. Using Baker, Gentry, and Rittenburg’s (2005), Baker’s (2009), and Baker and Mason’s (2012) work, experienced vulnerability will depend on the individual’s resources and background. But, many forms of Complex Resolvable and Complex, Dynamic Unresolvable situations leading to vulnerability are characterized by lower individual resources, suggesting high levels of experienced vulnerability in these categories.
This analysis leads to the first two propositions. The first proposition recognizes that not everyone facing a particular situation experiences vulnerability, but that certain situations are more likely to result this state. The second recognizes that quick fixes are appealing and, as a result, the likelihood of someone receiving assistance to remediate the vulnerability is higher if the means for delivering the assistance is straightforward.
Proposition 1: As the degree of complexity in the underlying situation increases, the probability that the individual facing the situation experiences vulnerability increases.
Proposition 2: If an individual experiences vulnerability, he/she is more likely to receive the necessary support to move back to a non-vulnerable state if the underlying situation has a straightforward remediation.
Many of the settings in which vulnerability is explored in the marketing literature fall into one of the first three categories. In these settings there is some hope of either remediation or finding an accommodation to allow the individual to resume his or her life. Less research is set in the fourth situation leading to vulnerability (Complex, Dynamic Unresolvable). Why less macromarketing research focuses on topics such as systems to support people facing Complex, Dynamic Unresolvable situations (e.g., the frail elderly or the severely disabled) is an open question. One possibility is that the individuals in this category are not very visible in most societies, so people living with these vulnerabilities attract less attention from the media and from researchers than, say, tornado victims. A second possibility is that the dependent measures one should use to assess the success of a system addressing Complex, Dynamic Unresolvable situations are unclear, especially if the vulnerability is idiosyncratic and increasing. Whatever the cause, the result is little marketing or macromarketing research in this area. But, the motivation to understand this particular type of situation leading to vulnerability is high because the problem of the embodied consumer, in an organic body that eventually succumbs to the progressive indignities of age, accident, disease and disability, is going to face everyone who does not die prematurely.
Vulnerability and Social Ties
Solutions for different situations leading to vulnerability may not be neutral or beneficial to everyone else. For example, the U.S. has a requirement that households can only have one car if a child in the household receives federal disability benefits. This demonstrates how the families who are committed to providing assistance to the chronically vulnerable person may find their control lessened and their likelihood of vulnerability increased. Similarly, in places like the U.S., the U.K., and Australia, schools have implemented “nut free” policies to protect the well-being of children with nut allergies. However, while such policies protect specific individuals, they also constrain the choices of many others. Sometimes individuals who face reduced choice are directly related to a vulnerable person, and sometimes the restrictions or costs are more broadly felt.
To further explore how vulnerability expands through the social network, suppose one’s mother’s home is leveled by a tornado. One might help her access community resources or even take the parent under one’s own roof while her home is being repaired. In this scenario, the freedoms and choices of the extended family may be limited by the tornado disruption, but the effect is muted and short term. Resources of the community are used, but the demand is time-limited. On the other hand, if one’s mother is diagnosed with dementia, someone, usually a family member, has to start to coordinate any community resources that are available, and organize finances, medical appointments, and other tasks of daily living. In the case of a parent with dementia, as demands on both family and community grow over time, the potential for vulnerability spreads. The family members experience a reduction in freedoms/choice and the cost for public services continues indefinitely as everyone tries to support the person with dementia. Layton and Grossbart (2006, p. 202) point to this tradeoff when they ask, “How may marketplace viability and community life and development be mutually reinforcing or at odds? What are the public policy implications of these interdependencies and tensions?”
Supporting all members of the community may only happen when the choices and resources for some, perhaps a majority, of the community are curtailed. Thus, efforts to mitigate or resolve vulnerability may actually extend constraints beyond the original vulnerable person. The point here is not that this leaking of vulnerability into the surrounding community is negative. Indeed, at the core of community is the notion of social ties and reciprocal well-being. However, effectively addressing Complex, Dynamic Unresolvable situations requires addressing the secondary vulnerability it engenders.
Layton and Grossbart (2006) suggest the notion that quality of life is actually a trade-off among generations and that “QOL issues are often framed in terms of individuals, but life may be socially embedded and not isolated. Thus, consumers’ QOL levels and social ties are related” (p. 207). We suggest that the tradeoff in QOL may not only be between generations, but also between the people who are touched by a situation that leads to vulnerability (e.g., the family of the ill person or the neighbors of the family whose home is destroyed). For example, in a study of parents of adults with intellectual disabilities (Yoong and Koritsas 2012), parents reported a reduction in their own opportunities for leisure. As one parent said, “We can’t go anywhere…the QOL that most other people our age have, we don’t have” (p. 613). Similarly, a study of individuals living with mild to moderate Alzheimer’s Disease and their families (Kurz et al. 2008) reports a discrepancy between the importance caregivers assign to their “ability to enjoy life” (100% of the American respondents deem this important) and their achieved ability to enjoy life (about 75% of the caregivers achieve this in U.S.). In contrast, the people with Alzheimer’s disease in the U.S. also reported 100% for the importance of enjoying life, but about 95% reported achieving enjoyment of life. It is possible the criteria for achieving enjoyment of life differ significantly between these two groups, but it is also possible that a tradeoff in QOL occurs with the caregiving task.
The takeaway is that long lasting, complicated, dynamic vulnerabilities, like those associated with severe disability and impairment, often lead to secondary vulnerabilities in the support group of the vulnerable person. The secondary vulnerability is not the same as the initial vulnerability, but it is directly related to it. This is captured in our third proposition.
Proposition 3: When someone experiences vulnerability from a Complex, Dynamic Unresolvable situation, his/her social network is exposed to the potential of a secondary vulnerability as a direct result of their ties to the vulnerable person.
An implication of spreading vulnerability, especially in the Complex, Dynamic Unresolvable category, is that systems designed to support the initial vulnerability may be called upon to address secondary vulnerabilities, even though the secondary vulnerabilities are not part of the system’s designated domain. For example, the public school system is required to provide a free and appropriate education for all students in the U.S. For complex, hard to manage students, this fortuitously provides hours of respite care for their home provider. If school were available five days a week, all year long, the provider could conceivably even work part time. However, because school are not charged with providing respite care, school closings, such as holidays and summer break, make employment very difficult for the primary home care provider. This observation leads to the final two propositions of this section.
Proposition 4: There are more resources for individuals who experience vulnerability due to Complex, Dynamic Unresolvable situations than there are for the support group members who experience secondary vulnerability.
Proposition 5: Because they see no other alternative, people with secondary vulnerabilities (that derive from their close social ties to individuals who experience vulnerability due to Complex, Dynamic Unresolvable situations) seek relief from their secondary vulnerability from systems that that are designed instead to provide services to the initially vulnerable individual.
Three Broad Topics Related to Secondary Vulnerability Associated with Physical, Cognitive, and Behavioral Impairment
Often people with vulnerability, say from a natural disaster, learn from others who share the same vulnerability. Disability is unusual in this regard because, in general, the more severe the disability, the more it plays out in the individual body in a personalized way. For example, one person’s profound seizure disorder is often quite different from another’s, limiting the opportunity for even finding people with identical vulnerabilities. As Thomson (1997) notes, “Disability unites a highly marked, heterogeneous group whose only commonality is being considered abnormal” (p. 24). Individuals with disability may have very little in common with each other except that they deviate from proscribed norms, and the more severe the disability, the more this hold true. The Kessler Foundation/NOD survey (2010, p. 148) supports this with 40% of the respondents with a very severe disability indicating that they have only “some sense” or “no sense” of “commonality with other people with disability.” The caregivers of someone with a severe disability have the shared experience of living with these challenges but, since the challenges themselves are idiosyncratic, so is the experience of living with them.
The first topic we relate to secondary vulnerability is the support available to caregivers. Idiosyncrasies of the underling disability notwithstanding, secondary vulnerability may be reduced by reaching out to other support providers. Support groups, online or face-to-face, reduce the sense that the individual or his/her support group is single-handedly facing an unending set of challenges and supports coping (Duhachek and Oakley 2007). For example, in a study of caregivers of individuals with Alzheimer’s Disease (Millán-Calenti et al. 2000), after one year of participating in a support group, caregivers reported more knowledge of available resources, a better sense of where to turn in times of stress, increased attempts to regain their own social life, and a greater sense of well-being as a direct result of better problem-solving skills. As this particular study shows, the day-to-day problem for individuals, or their support groups, who face dynamic or progressively worsening vulnerability is often to learn the system, as opposed to addressing a particular challenge. The role of online support groups is especially important as a different survey found (Kurz et al. 2008), “The single most common reason given by family members or other carers not using AD [Alzheimer’s Disease] organizations in France, Canada, and the USA was that they were too far away or too inconvenient to get to” (p. 351). Theoretical contributions can be made in understanding how to build and maintain extended support groups, and how to maintain clear and accurate information in a free-wheeling online forum.
The second topic we relate to secondary vulnerability is the role of the support group as a market intermediary. Specific issues related to interaction in the market are addressed further on. Here we begin the discussion of how support can be provided in a manner that helps maintain autonomy (see also Meneely, Strugnell, and Burns 2009). For example, in a short biography included in Thomas (1999) a woman who had been largely house-bound for 23 years finally received enough home health support to allow her to do both self and home care and to do four hours of shopping per week (largely for food). She says, “I was able to choose exactly what I wanted, instead of having to look delighted and not show that what was bought was not want I wanted” (p. 90). As this quote demonstrates, the role of the support group is laden with power negotiations, social roles and meaning. A similar issue can be seen in the reflections of a 50 year old male with a recent spinal cord injury (Van de Velde et al. 2012). He was willing to accept certain help from the nurses while he was in the hospital, because “they were supposed to help me … that was their job” (p. 495). But, upon returning home, while acknowledging his girlfriend could do these tasks faster, decided “she can do other things for me, and I intentionally had to tell her what she can do and what I want to do” (p. 495). Relevant topics for future research could include understanding the dynamics of support groups for the vulnerable, the difference between paid and unpaid support givers, and how market systems impact group dynamics (e.g., the legality of sharing one’s credit card).
The third topic we relate to secondary vulnerability rests on structural changes in the last 50 to 70 years regarding who provides services to people with disabilities or other embodied vulnerabilities. Is it exclusively family or local community (what occurred for millennia); large institutions (e.g., madhouses, tuberculosis sanatoriums); government support for local delivery (e.g., group homes); government support for government approved services in the home or local delivery (e.g., the care described in the previous paragraph or a nursing home); or private insurance support for approved services (e.g., long term care insurance coverage)? How can services be provided in a way that maximizes overall benefit (to society, community, family and individual), while remaining cost-efficient, high-quality, and personalized? In a detailed discussion of these trends as they related to intellectual disabilities in the UK and Australia, Dowse (2009) notes that efficient use of state funds has the effect of “bringing market relationships into what had once been regarded as non-market spheres” (p. 575) and that, “people with intellectual disability do not have the power of choice in purchasing services and that they and their families, friends and allies have a diminished role in determining support service needs” (p. 579). Macromarketing may be able to help explore the balance between individual rights, family needs, resource constraints, autonomy in the market and consistency in service provision.
This concludes our analysis of the four categories in which current thinking on vulnerability is expanded and clarified by considering bodily impairment. By organizing vulnerability into four categories reflecting ability to remediate, duration and dynamism, the often overlooked category of Complex, Dynamic Unresolvable situations emerges. In addition to being of interest in its own right, this type of situation often triggers vulnerability in the individual’s family/support group. The likelihood of secondary vulnerability is high when one is in relationship with the individual who experiences vulnerability due to a Complex, Dynamic Unresolvable situation.
We now look beyond the four categories to focus closely on how specific embodied challenges limit market choice and market flexibility (e.g., cannot speak or cannot walk without crutches). Normative expectations regarding the body and its cognitive capacity present fertile ground for exploring consumer agency and how actors relate to one another in the market. We begin with updated data on the Americans with Disabilities Act, but similar legislation exists in other developed countries. This discussion acts as a foundation for considering the environment in which individuals with disabilities operate. The article then considers specific types of impairments as they relate to the market, explores how current remediation works or falls short, and considers what this means about experienced vulnerability.
Consumer Vulnerability and the Americans with Disabilities Act
Laws and regulations impact the experienced vulnerability associated with disability. In 1990 the U.S. enacted the Americans with Disabilities Act as part of a larger social movement that increased opportunities for people who had been disadvantaged in the market. Similar legislation has been passed in other developed nations. The goal of this sort of legislation is to increase access to a wide range of retail, entertainment, and travel opportunities for individuals with disabilities. Kaufman-Scarborough and Baker (2005) provide a detailed background on ADA and report on a 1998 survey related to disabled individuals’ assessment of how well ADA meets its stated goals. Among other findings these authors report that respondents understand access to mean different things but that, in general, when access is difficult, individuals report lower marketplace interaction.
The survey was conducted again recently (Kessler Foundation/NOD 2010), this time including 1001 disabled respondents (56% with very or somewhat severe disabilities and 42% with slight or moderate disabilities, 2% did not provide a response) and 788 non-disabled respondents. Again the survey was done by phone. If the person with a disability were unavailable or unable to answer, a proxy from the household responded for the disabled person. Approximately 10% of the disabled “respondents” were proxies. Harris Interactive included a screening question on other surveys that it ran in the weeks preceding the Kessler Foundation/NOD survey to estimate the incidence of adults with disabilities in the U.S. and calculated that the prevalence is between 13% and 16%. This is slightly below the Bureau of the Census figure that places disability in people 21 and older at 22.5% (Brault 2012).
In general, the Kessler Foundation/NOD surveys in 1998 and 2010 (as well as ones in 2000 and 2004) show that only about a quarter to a third of the respondents with disabilities believe that ADA has made life better for them. People with severe disabilities are slightly more likely to report that ADA has made their lives better, but the numbers are still very low (26% for the severely disabled as opposed to 14% for the slightly disabled) (Kessler Foundation/NOD 2010, p. 145).
So, the question of what ADA has done for respondents and what it cannot, or has not done, is an intriguing one. A key insight emerges from the questions related to specific consumer activities. In comparing adults with and without disabilities in the Kessler Foundation/NOD surveys, adults with disabilities report greater problems with transportation (34% vs. 16%), lower likelihood of going to a restaurant at least twice a month (48% vs. 75%), a greater likelihood of needing medical care in the last 12 months but not getting it (19% vs. 10%), lower access to the internet (54% vs. 85%), a higher rate of being dissatisfied with life in general (20% vs. 6%), and greater financial vulnerability (58% vs. 34%). While about 83% of adults with slight disabilities report being “treated the same as other people,” the number drops to 58% for those with severe disabilities.
ADA mandates environmental changes such as ramps and wider doorways. It says that business cannot discriminate on the basis of disability, but laws cannot realistically mandate that stigmatization of disability disappear. It says that the service provider must make it possible for the person with a disability to engage in consumption at the service provider’s place of business, but it does not ensure that the disabled person can arrange transportation, have enough financial resources, or have someone with whom to dine. It can require that retail website sites have voice-overs to help the visually impaired but cannot mandate that everyone have a computer and Internet access. It can ensure movement through a health facility, but it cannot guarantee that the sort of specialist that someone desires is available in her geographic region. Legislation like the ADA is proscriptive in way that reduces environmental barriers. But, in terms of actually improving the day-to-day lived experience of people with disabilities, especially severe disabilities, it is limited. What this means is that current efforts focused on access have improved access, but they have not eliminated all market impediments associated with physical, behavioral, or cognitive impairment.
The Market and Specific Types of Impairments
In the field of disability studies a number of models are used to explore disability. Two of the most basic are the medical model of disability and the social model of disability (DePoy and Gilson 2011; Kaufman-Scarborough and Baker 2005; Oliver 1996). In the medical model, the impairment is seen as the root of the problem, and if the impairment were eliminated, it would allow the individual to enjoy surroundings that were designed for the able-bodied. In the medical model, if someone has severe osteoarthritis and cannot go up and down stairs, a knee replacement and month of rehab therapy should enable them to enjoy the marketplace just like everyone else. In contrast, the social model says that the rigid application of normative expectations is what makes an impairment disabling. In the social model of disability, the incorporation of stairs in public places relies on the expectation that everyone can go up and down stairs. It is this expectation that makes advanced osteoarthritis of the knee a disability. If there were elevators or ramped floors, then the social model would suggest that being unable to use stairs ceases to be a disability.
Scholars, especially those with a disability or living with someone with a disability, have spoken out against the perspective in which disability is solely a social construct (Anastasiou and Kauffman 2013; Gottlieb 2002; Reindal 2010; Ware 2002). These writers contend that the embodied reality of disability, such as chronic pain or requiring over an hour to get dressed in the morning, extends much further than a social construct. As Anastasiou and Kauffman (2013) describe, the social model draws “a vertical line between biological properties and the social dimensions of disabilities” (p. 445), continuing to say that the subject of the social model “is not an individual with a full set of properties (biological, psychological, social) but, at best, a ‘half-person’ with only social properties” (p. 445). That is, these authors hold the social model is inadequate because the body itself has limitations or differences that make daily functioning and activities more difficult or time-consuming, regardless of the environment. These differences fundamentally change the experience of life. Our research is stationed in this latter perspective as it considers the lived experiences of individuals, their caregivers, and their activities in the market, acknowledging both the social construction and the experience of a non-normative body.
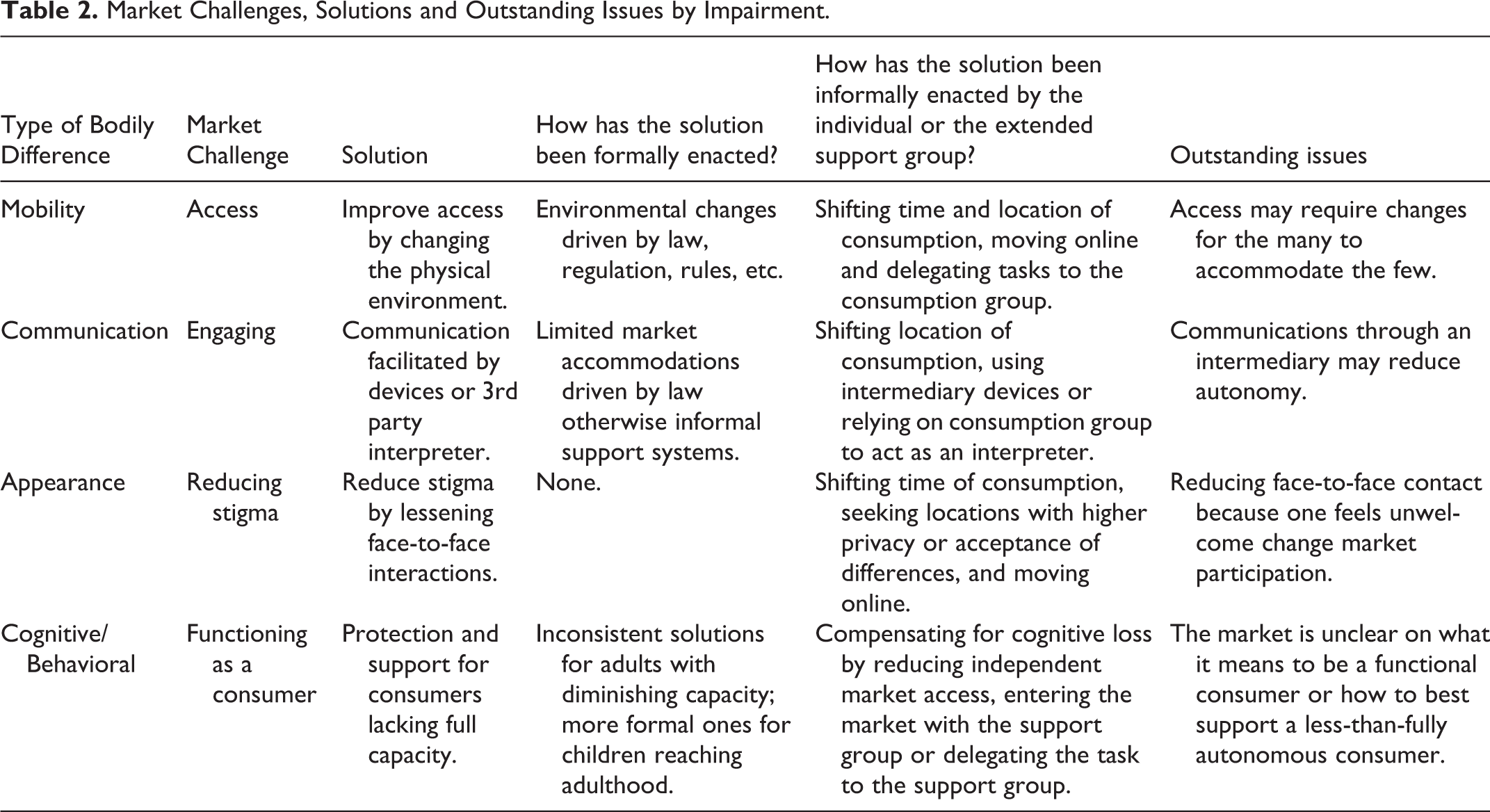
Table 2 captures many of the ideas that are developed more fully in the four sections below. The left hand column this Table has the four types of bodily difference that are discussed here in detail, section by section. Each type of bodily difference presents a market challenge to the individual and this is succinctly described in the second column. Various ways of addressing these challenges appears in the third column. Some of these solutions have been formally enacted, for example through laws, and others have been developed informally by individuals or their support groups. These are identified in the fourth and fifth columns, respectively. Issues related to macromarketing surface in the discussion below and are summarized in the table’s last column.
Market Challenges, Solutions and Outstanding Issues by Impairment.
Impairment that Limits Mobility
The type of disability in this category, such as using crutches /wheelchair, gait disorders, and visual impairment, are precisely the sorts of impairments that ADA addresses in its focus on access to the market. Access has been an important focus elsewhere such as the Council of Canadians with Disabilities and the Union of the Physically Impaired Against Segregation in the UK (Withers 2012). The issue for mobility limiting impairments is getting to/from the marketplace, moving through the marketplace and being physically present for exchange. Impairments leading to mobility restrictions can be any of the four categories discussed earlier. Mobility challenges are highly visible and touch many in the population, ranging from a broken leg (Straightforward Resolvable), club foot (Complex Resolvable), amputations (Straightforward Unresolvable) and progressive neuromuscular disease (Complex, Dynamic Unresolvable).
Because mobility limitation (especially Straightforward Resolvable) is so common, and because many of the challenges in this category of disability are amenable remediation, accommodation rules have been written for retail/service settings. Stairs have been complemented with ramps and elevators, bathrooms have been made accessible, seats are set aside in classrooms and theaters for wheelchairs, retail locations must have some wide parking spots, and stores have a variety of heights for check-out counters.
Although access has been addressed at the policy level to allow the individual to enter the market, the lived reality of mobility impairment is somewhat different. Proxemics is the term that is used to capture the cultural and social norms associated with the space and the people inhabiting the space (Hall 1966; Yanow 2006). Building on proxemic expectations of how close individuals should stand to each other, designers work with these notions and ADA regulations to lay out stores. But access legislation does not address variations in speed, surges in demand (e.g., limited number of reserved handicap spaces), or all the idiosyncratic needs of a physical impairment that limits mobility. As a result, individuals or their caregivers shift physical locations (e.g., to a restaurant with a bigger parking lot), change time of consumption (e.g., to a Wal-Mart only on a quieter day), move consumption online, or delegate the task to someone without the mobility impairment (Mason and Pavia 2006; Meneely, Strugnell, and Burns 2009; Pavia and Mason 2012).
From a theoretical perspective, it is useful to consider mobility as both the movement (from here to there) and the speed of the movement. Much of the regulation regarding access for those with mobility impairment relates to the movement but not speed. One topic that may be of interest to macromarketing is the extent to which time/speed expectations constrain people with mobility impairments. That is, structural solutions like a curb-cut may not be enough if one’s transit time across the street is too slow to be safe. One solution is ready-to-use modifications such as stoplights with a “slow down” button for pedestrians who require much longer crossing the street. Another is segmenting service provision by speed, such as changes in airport security screening where travelers can self-select into lines with norms of faster/slower transit times. The broad question is, in a world where speed is revered, how does one build support for modifications that accommodate slow movement? This leads us to propose the following.
Proposition 6: Mobility impairment adaptations that relate to movement at a slower speed are accepted by the population only when slow movement is an option, not a requirement.
Impairment that Limits Communication
The second category of impairment includes hearing loss, speech impediments, aphasia, and other disabilities that limit communication. This category of disability is less about access than about the ability to engage. While there are a few instances of temporary hearing/speech loss (Straightforward Resolvable in the earlier discussion), most instances of this impairment have the potential to be longer lasting, such as newborn hearing impairment amenable to Cochlear implant (Complex Resolvable), permanent damage to speech centers after stroke (Straightforward Unresolvable), and progressive hearing loss associated with aging (Complex, Dynamic Unresolvable).
Some of these impairments, such as hearing loss, are addressed in ADA wherein sign language interpreters are required at various public events and educational settings or closed captioning is required for public broadcast. However, market experiences such as overhead announcements, sirens, talking to a physician, asking for a variation to an item on a menu in a restaurant, even needing a wake-up assist from the front desk in a hotel, remain and these are difficult to negotiate on one’s own. As a result what often occurs is that an intermediary, a hired interpreter or a part of the consumption group, helps facilitate communication.
One of the problems with using an intermediary for communication is that it is easy for the person with the communication impairment to lose his/her autonomy. For example, a study of deaf users of medical care identified a neutral third party professional sign language translator as an optimal arrangement (Steinberg et al. 2006). But professionals are not always available and when family members were the intermediary, “participants reported that they were frequently inadequate as communication facilitators and participants still felt excluded from the health care conversation. Working with family members as interpreters also compromised privacy” (p. 262).
In addition, the role of a third party intermediary is particularly complex if the cognitive capacity of the individual is unclear, as demonstrated in two contrasting studies of elderly patients who have family/friends that attend doctor visits with them. When the aging individual is cognitively intact, in a controlled randomized experiment no differences were measured between individuals and individuals accompanied by a family member in terms of the physician’s focus on the patient’s concerns, number of words spoken, on measures of patient centered communication, or in the level of participatory decision making (Shields et al. 2005). However, in aging adults with increasing dementia, “the doctor-patient relationship changed dramatically as others became involved in care often with attendant ethical dilemmas related to patient autonomy and the locus of decision making” (Adams et al. 2005, p. 231).
As shown in Table 2, for communication impairment, the problem of engagement is usually addressed with a device that provides a communication interface (e.g., a speech machine, cochlear implant, or Braille text) or a human who provides the interface. Both of these can have an impact on the experience of the market for the individual with a communications disability. He or she may only go to certain places that have the devices (e.g., Braille markers) or who are willing to work with the devices (e.g., placing a special order at a restaurant with a speech machine). Or the individual must coordinate his/her market experience with the time that the human interpreter is available and negotiate any concomitant issues of autonomy.
From a theoretical perspective, macromarketing is concerned with how the individual’s voice is accurately retained as he/she uses intermediaries to engage in the market. Although this is clearly an issue for individuals who have communication impairments, it is also present when anyone requires someone to speak in his/her stead. All of the issues raised here for people with organic impediments to communication also exist for people who do not speak English in the U.S. or the home language in the country where they are engaging (see also Broderick et al. 2011).
Proposition 7: As the complexity of the topic of communication increases (e.g., medical care, advanced finances), the autonomy of an individual with communication impairment decreases.
Impairment that Makes One Look Different
The third category of impairment includes facial disfigurement, missing limbs, being very tall or very short, and other dysmorphisms. These impairments limit the individual’s experience of permission to participate in the market. Impairments that make one look different can fall in any of the categories discussed earlier. Almost everyone experiences some form of Complex Resolvable impairment whereby an accident, surgery, or even something as trivial as a bad hair day makes being in public uncomfortable until he/she looks more like everyone else. Straightforward Unresolvable and Complex, Dynamic Unresolvable impairments that make one look different can also have mobility or communications components (e.g., limb amputation or severe facial burns). But sometimes the “impairment” is not really much of an impairment beyond looking different. Someone with a significant port wine birthmark or vitiligo (Straightforward Unresolvable) should be able to function normally, but the literature is replete with instances of public discrimination against non-normative bodies.
The problem for this type of impairment is that the market is experienced as a hostile environment with whispering, pointing, staring, and other stigmatizing behaviors. The difficulty of sharing public space and drawing the gaze of others has been widely noted in the disability literature (Hughes 1999). For example, Hawkesworth (2001) describes how people living with facial differences seek the spatial-temporal combinations that minimize their exposure and maximize control (e.g., opting for email over an in-person meeting or choosing to work in a darkened cinema). Looking different can motivate individuals or their consumption groups to choose locations where the critical gaze of others is lessened (e.g., shopping at quiet times), can be obscured (e.g., a restaurant with alcoves), or can be eliminated (e.g., shopping online) (Pavia and Mason 2012). It is also common to seek places where non-normative looks and behavior are more accepted (e.g., burn camp, costume party) or other environments that can be thought of as a diluted version of Foucault’s (1967) heterotopias of deviation. These places are spaces away from home where many of the constraints of normal society are loosened, such as swimming pools, ice skating rinks, zoos, and campgrounds. Places that stand outside everyday culture by being more formal or with stated inclusiveness-norms, such as religious services, are also locations where the stigmatizing gaze is attenuated. The most effective means of avoid the gaze of others, of course, is to consume online.
Normative appearance is a very complicated topic. To date, humans continue to be critical of visible difference, although what constitute difference is quite fluid (e.g., tattoos were a marked difference at one point). So, the prognosis for remediating this particular market impediment at a macro-level is open to debate. While media has an undeniable impact in setting expectations for appearance, and in mocking those who do not meet minimal norms (e.g., the TV show, What Not to Wear), it is not clear what can or should be done. From a system perspective, the role of the Internet as a means for avoiding the critical gaze from an in-person encounter raises questions about what it means to consume online because one does not feel welcome in person. Then, once the person chooses to consume primarily online, questions are begged about the body images used online, both those that support an idealized normative body and those that, in aggregate, are even more negative than usual about a non-normative body (Heuer, McClure, and Puhl 2011).
Cognitive and Behavioral Impairment
The fourth category of impairment in Table 2 is cognitive impairment and/or behavioral disorders including forms of mental illness that interfere with decision making, dementia, autism, sensory overload, traumatic brain injury, poor impulse control, and a long list of other disabilities. Some situations lead to Straightforward Resolvable cognitive/behavioral impairments (a bad reaction to prescription drugs) or Complex Resolvable (treatable depression). More common are Straightforward Unresolvable (dyslexia) and Complex, Dynamic Unresolvable (Alzheimer’s disease). A complicating factor in classifying various cognitive/behavioral impairments is that, for some, the etiology is unclear and the efficacy of various prevention/treatment options is not agreed upon (e.g., autism).
Cognitive and behavioral impairments can lead a person to have difficulty making good choices; to use unacceptable touch, sounds, or language; to violate social norms for greeting, waiting, and queuing; and to find new environments, packaging, or products completely overwhelming (Meneely, Strugnell, and Burns 2009). Mostpeople accept that young children do not have the capacity be fully independent agents in the marketplace, but a point comes where a person is deemed adult enough to make certain decisions. That is, for different types of transactions there is an age at which most people, or the law, or social norms, believe that someone is capable of making a particular consumer decision. In the U.S. for example, a person can join the military without parental consent at 18 years of age, buy alcohol at 21, and vote at 18.
In the same way, there are marketplace behavioral expectations that come with age. An infant crying at McDonald’s is very different than a large middle aged man crying at McDonald’s. If a four year old has a temper tantrum on an airplane the other passengers react differently than if a woman aged 25 starts screaming, hitting, and stamping her feet in the aisle. A five year old that puts candy in her pocket without paying is seen differently than a 70 year old that does the same thing. And a mother changing an infant’s diaper in the restroom is very different from a mother changing a 12 year old’s diaper.
As these examples show, cognitive/behavioral impairment raises two issues: the first is the cognitive ability of the individual to engage independently in the market, and second is the ability of the person to follow accepted social norms for market engagement. Many of the market mechanisms for addressing cognitive/behavioral impairment focus on the first issue (cognitive capacity) and come down to questions of the individual’s legal ability to make a decision. For example, if an adult has previously been cognitively/behaviorally normal but now has increasing dementia, until she voluntarily gives up her rights or until the court takes rights away from the person, she retains full consumer autonomy. This means she has the right to buy a car, assuming a loan if necessary, even if she has lost the ability to route-find while in the car. Until the person is shown to be a threat to himself or others, for the most part, in the U.S., policy and the law seems to have an implicit expectation of an informal support network to help someone with cognitive impairment.
With regard to the second issue, ability to follow accepted social norms, few regulations address this beyond basic health and safety issues. It is not illegal to walk along the sidewalk muttering or waving one’s arms, but it is illegal to do this in the aisle of a plane taxiing on the runway. However, if the person walking along the sidewalk is not a young child and if he/she is part of group, the rest of the group may feel enough stigma by association to choose to consume without the cognitively/behaviorally impaired person (Pavia and Mason 2012). When this happens, the person with impairment is often kept out of the market and someone else consumes for them raising issues of autonomy.
As shown in Table 2, challenges associated with cognitive/behavioral impairment are complex and much less amenable to regulatory remediation. Substantial confusion surrounds issues such as dementia and voting (Karlawish et al. 2004), mental retardation and consent laws (Pollack 2005), and intellectual disability and banking (Hayes and Martin 2007). Especially when a previously functioning consumer begins to slip into cognitive/behavioral decline, it is common for his/her support group to act as an intermediary. This intermediary may find environments that are less challenging (e.g., quieter, calmer), buffer the individual from some decisions (e.g., take over bill paying), provide moment-to-moment support in decision making, or may enter the market as a proxy for the individual (Barnhart and Peñaloza 2013).
From a theoretical perspective, the topic of cognitive capacity and behavioral impairment raises many macromarketing questions. First among these is what does it mean to be a functional consumer? How do we provide opportunities for individual choice while protecting those who cannot make decisions (see also Dowse 2009; Pilgrim and Tomasini 2012)? How do we support consumption groups that enable a person to be present in the market who no longer has the capacity to act independently (Barnhart and Peñaloza 2013)? What does it mean to have a marketplace that is increasingly complex if it excludes more and more people who cannot function in a complex market? Most these issues require more investigation before propositions can be made, but we have captured two below.
Proposition 8: Increasing market complexity increases the number of adults with cognitive/behavioral impairments that require intermediaries.
Proposition 9: Intermediaries for people with cognitive/behavioral impairments limit market interactions undertaken with the impaired person to maintain compliance with behavioral market norms.
This completes our detailed look at how specific forms of bodily impairment impact market interaction. Speaking broadly, bodily impairment can fall in any of the four categories identified earlier. But, setting aside Straightforward, Remediable problems like a broken leg, mobility and communication impediments are generally more amenable to remediation and have received more attention in the literature. Many complicated and meaningful issues remain though, particularly those associated with visible difference and cognitive/behavioral impairment. Among these issues are how normative appearance expectations are reinforced by the marketing mix, the nature of secondary vulnerability, what it means to be an autonomous consumer, and the implications of increasing market complexity.
Discussion
We began by exploring existing vulnerability research in marketing and related fields to consider how this literature addresses, or fails to address, issues related to disability and bodily impairment. Scholarly work in vulnerability has frequently been analogous to the medical model. That is, illiterate consumers will no longer be vulnerable if they are taught to read; or the flooded homeowners will no longer be vulnerable once their homes are rebuilt. Much less attention has been given to situations leading to vulnerability that cannot be remediated. If the equivalent of the social model of disability is brought to vulnerability theory, instead of trying to remediate illiteracy, the market could be changed to no longer require reading. This is a much more challenging position and is not realistic. Especially from the perspective of significant cognitive impairment, neither the medical model (in which cognitive ability is restored), nor the social model (redesigning the market to require less cognitive ability) holds much promise (Dowse 2009; Pilgrim and Tomasini 2012). In actuality, many aspects of the marketplace are becoming more complex and the expectations on consumers for cognitive processing have increased. This suggests that the environment is more likely to cause someone with cognitive impairment to experience problems. That is, the marketplace de facto renders more people impaired, and potentially vulnerable, as it becomes more complex.
Following more recent theory in disability studies, our approach has moved beyond the medical/social model debate to use the body itself as a lens to understand how impairment impacts one’s ability to consume. This work has unpacked the nature of the bodily-related impairment and ways one might reduce its vulnerability. We have approached the issue of disability as a situation that leads to vulnerability from a practical day-to-day perspective. Following other writers in the marketing field, we have used the term vulnerability to capture a complex array of factors that, for a variety of reasons, puts someone as less than an equal footing in the market.
There are aspects of modern life that leave someone with physical, cognitive or behavioral differences at a disadvantage in the market, such as the “need for speed” in movement or speech that is assumed in much of today’s world. Similarly, fragmentation of experience privileges flexibility over routine, adding to the demands on someone who finds engaging with the market difficult from the outset (e.g., Meneely, Strugnell, and Burns 2009). In addition, the primacy of visual images in much of contemporary marketing also places increased pressure on those with non-normative bodies (DePoy and Gilson 2011). And, neo-liberal notions of individual value arising from production and work lead many with limited ability (for one reason or another) to be less than fully productive workers to question their worth as people (Kumar, Sonpal, and Hiranandani 2012).
On the positive side, market changes, such as ramps, designated parking, sign language interpreters and the growth of the internet have opened more of the market to people with impairments. The marketing system has vastly improved the lives of people with disabilities through changes in education, access to health care, inclusion of people with disabilities in TV shows, and advances in biomedical engineering. As medical advances allow people to live longer, and survive trauma and premature birth, more families are touched at some level with engaging in the market with someone who faces physical, cognitive or behavioral challenges. At the same time, many consumers cannot believe the statistics regarding the extent of disability or impairment in the population because they do not actually see, or think they do not see, many disabled consumers themselves on a day-to-day basis in public. The more that people with disabilities consume in private, by proxy, at not peak times, and/or online, the less visible they are in the market and the less likely it is that someone sees this as pressing social issue.
Finally, drawing on recent work by Burghardt (2013) and Withers (2012), we would also like to raise the provocative question of whether the label of vulnerability may itself be a social category that oppresses those classified vulnerable. Most marketing literature on vulnerability has as an end the coordination of resources to improve individual’s lives (e.g., emergency relief), programs to reduce social injustices (e.g., literacy program), or changes in the macromarket to remove unnecessary structural barriers to consumption, education, and recreation. However, some in the disability field have questioned whether, in the case of enduring embodied difference, classifying someone with persistent market imbalances as vulnerable sets those with disabilities in position of inherent powerlessness. As Burghardt notes, “Vulnerability is thus a relative state: the normative social structures against which it is compared sketch out its parameters of defenselessness and passivity, or conversely, integrity and agency” (p. 559). On the other hand, the lived experience of a body that requires additional support and care, causes other theorists to “posit that the notion of vulnerability is more complex, and that a full understanding of disability requires a broad discussion of the human condition, including vulnerability and human frailty and their inherent meanings” (p. 557). The question these scholars raise regarding vulnerability’s role in identity and marginalization is beyond the scope of this article, although we note that even within vulnerability theory, the lack of attention to Complex, Dynamic Unresolvable situations is a form of marginalization itself.
Acknowledging the role of the body on consumption and the interplay of the body and the marketplace provides fruitful venues for additional research and a means for improving lives worldwide. We have identified a number of theoretical macromarketing issues that that have applications well beyond just the part of the population living with impairment. Autonomy, what it means to be a fully functional member of the market, the experience of secondary vulnerability, and how trade-offs are made between the more and less able remain important global macromarketing issues.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.