
Abstract
Consumers increasingly turn to online health communities for health information and social support. Yet, the type of value consumers derive from online health communities is not well understood. This study examines social support as the mechanism through which consumers co-create and experience different types of value. Cutrona and Russell’s typology of social support and Holbrook’s consumer value typology are applied to posts and threads obtained from two online communities for people with Parkinson’s Disease and ALS. Results demonstrate that online health communities give consumers the opportunity to create and experience forms of consumer value that would not otherwise be available in a traditional health delivery system. The results lend support to a re-conceptualisation of medical practice and health delivery for consumers with chronic conditions.
Introduction
Health is an important social and economic issue with significant ramifications for macromarketing. Access to quality medical information and to efficient, affordable, and safe healthcare practices are critical to consumer quality of life (QOL) and provide a foundation for distributive justice (Brennan, Eagle, and Rice 2009; Layton 2009; Rahtz and Syzykman 2008; Sirgy, Lee, and Rahtz 2007; Varman and Vikas 2007). Issues of inequity, consumer vulnerability and disempowerment are concerns for health systems globally, both in developed economies such as the United States (Mascarenhas, Kesavan, and Bernacchi 2013) and Europe (Stakišaitis et al. 2007) and in developing economies like India (Varman and Vikas 2007). Internet technology has enabled the development of patient-centered websites and consumer forums that add to consumer knowledge and potentially improve the efficiency and effectiveness of healthcare delivery. Such peer-to-peer online health forums are especially valued by patients who suffer from rare, chronic or debilitating conditions, assisting these individuals to connect with others, share information and experiences and gain support leading to better health outcomes (Edlin 2002).
The value placed by consumers on peer-to-peer networks is an important factor in understanding whether such networks supplement or challenge traditional macromarketing systems of health delivery. To date, little research examines how consumers co-create value within online health communities. Our goal is to contribute to the macromarketing debate regarding online aspects of health systems by examining the exchange of social support as a mechanism for consumer value co-creation within online health communities for people suffering from degenerative neurological diseases. We use Cutrona and Russell’s (1990) social support typology and Holbrook’s (1999) typology of consumer value as a theoretical basis upon which to inform our observations and analyses (Hunt 1993).
We begin with scholarship relating to online communities, co-creation of value, consumer value, and social support. We then extend the findings of earlier studies through observational research to demonstrate how participants of online health communities experience co-created value through social support. We conclude with a discussion of the macromarketing implications, with consideration of health service providers and policy makers. In particular, we argue that peer-to-peer online discussion forums provide patients and care givers with much more than simply information on treatment and lifestyle options. These peer-to-peer discussion forums give consumers the opportunity to create and experience forms of consumer value that would not otherwise be available in a traditional health delivery system. The results lend support to a re-conceptualization of medical practice and health delivery for consumers with chronic conditions.
Theoretical Background
Marketing scholarship in the field of online socially-based consumption focuses on both brand communities (Hollebeek and Chen 2013; Schau, Muniz, and Arnould 2009) and social communities (Brown, Broderick, and Lee 2007; Peters, Bodkin, and Fitzgerald 2012; Seraj 2012), recognizing that these online communities are vital spaces for the exchange and diffusion of consumption messages. Recent attention has shifted from online communities as spaces where word-of-mouth marketing proliferates, creating or damaging brand value, to the creation of peer-to-peer consumer value within these communities. This shift, from considering the impact of online community life for firms to the value for consumers has occurred in parallel with renewed interest in the concept of value co-creation.
Value Co-creation
Value co-creation is the notion that consumers come together with suppliers, service providers or other consumers to generate benefits realized by the user in the consumption process (Lusch, Vargo, and O’Brien 2007; Nambisan and Nambisan 2009; Vargo and Lusch 2004). Within online communities value co-creation occurs between consumers or peers in a process variably known as peer production (Tapscott and Williams 2006), co-production (Peters, Bodkin, and Fitzgerald 2012), or social production (Arvidsson 2008) amongst other terms. The idea that consumers can work together with firms as part of the value-creation cycle rather than operating as passive targets of value is not new (Cova, Dalli, and Zwick 2011; von Hippel 2005). The internet, however, gives consumers the ability to self-organize and collaborate online as part of a “socially-embedded consumption experience” (Mathwick, Wiertz, and de Ruyter 2008, p. 833).
Misra, Mukherjee and Peterson (2008) examine value created within an online support group for patients suffering from depression. The study identifies areas of discussion among participants (e.g. disease information, credibility of internet sources) and level of activity (e.g. number of postings per day, duration of time spent on site), but without developing the concept of consumer value. Another study focuses on value captured by the firm (Nambisan and Nambisan 2009) and considers the potential for co-creation of value across four categories of online communities: communities led by consumers, communities led by healthcare firms, communities that share knowledge, and communities that create new knowledge, including discussion of specific online health communities. Once again, consumers are acknowledged in the value-creation process, but value experienced by consumers is not considered in any depth. Of some relevance is McColl-Kennedy et al.’s (2012) study of value co-creation within a face-to-face health service encounter. The study aims to understand exactly what consumers do when co-creating value. One of the eight value co-creation practices identified as “Connecting with Others” directly relates to the use of online health communities, the function of which is to enable people experiencing a particular health condition to connect with others for the purpose of information sharing and support. The study identifies quality of life (QOL) as the value experienced by consumers, but does not go into the concept further. Other scholars explore the motivation for consumers to form online collectives and cooperate in value-creating consumption experiences using concepts such as the nature of community (Fischer, Bristor, and Gainer 1996), social capital (Mathwick, Wiertz, and de Ruyter 2008), and collective action (McLure Wasko and Faraj 2005). None of these studies directly relate these various constructs to consideration of consumer value.
Early work examining online environments (Hoffman and Novak 1996) and studies in the brand community literature provide some direction with regards to consumer value. Most brand community research looks at the processes involved in co-creation, what consumers do, the activities and practices they perform (Kozinets 1999; Leigh, Peters, and Shelton 2006; Schau, Muniz, and Arnould 2009), or the types of communities that foster co-creation (Fischer, Bristor, and Gainer 1996; Muniz and O’Guinn 2001). For example, Hoffman and Novak (1996) identify types of online consumption behavior such as providing information and emotional support, showing appreciation for the community, sharing jokes and personal stories, expressing a spiritual bond between participants, and intervening to ensure posts remain within the guidelines and misleading information is corrected. Although not the main focus, many of these studies discuss consumer value at some level, finding that through the process of sharing information and experiences, a sense of belonging, self-identity, and obligation develop. Group members value being appreciated and accepted by others. They value being useful, providing help to solve practical problems or emotional support. This research also notes that group members actively compete with one another displaying their individual and cultural competencies to gain recognition and establish their status in the social hierarchy. Above all, as aptly put by Muniz and O’Guinn (2001) group members enjoy “…the relatively hedonistic and liberatory ethos, where pleasure is more sanctioned than restricted” (p. 427).
Seraj’s (2012) work on an online aviation community is one of the few that explicitly looks at co-created consumer value. Results identify three general types: intellectual, social, and cultural value. Intellectual value is the quality content and knowledge and functional information created by and available to community members. Social value comes from the interactive, playful environment that is “enthusiastic and fun” resulting in the development of social ties giving members a sense of belonging. Finally, cultural value provides norms of behavior allowing members to take on roles and moral responsibility leading to feelings of pride and respect and ensuring accepted practices are followed. A comparison of intellectual, social and cultural value with previous brand community studies reveals a number of similarities with regards to consumer value. Consumers experience pure pleasure, learn practical knowledge, gain status, recognition, morality, a sense of belonging and acceptance. Our study aims to further research on how consumers experience co-created value within online health communities through one of the primary functions of an online health community: social support.
Social Support
“Social support refers to verbal and nonverbal communication between recipients and providers that reduces uncertainty about the situation, the self, the other, or the relationship, and functions to enhance a perception of personal control in one’s experience” (Albrecht and Adelman 1987, p. 19).
Of considerable interest is the availability of social support within online environments populated by strangers, using only text-based communication. Studies conclude that despite the impoverished nature of the environment, social support flourishes and contributes to feelings of self-esteem and empowerment (Coulson 2005; Coulson, Buchanan, and Aubeeluck 2007; Coulson and Kniff 2007; Drentea and Moren-Cross 2005; Farnham et al. 2002; Fischer, Bristor, and Gainer 1996; Lieberman et al. 2005; Malik and Coulson 2008). Access to face-to-face social support may be difficult for people who are chronically ill or disabled, due to rationing of services as well as transport and other logistical challenges. Online health communities provide a mechanism through which regular and ongoing text-based interaction is available to those who find external face-to-face interaction difficult due to a disability or other health condition (Braithwaite, Waldron, and Finn 1999). Online communities can also contribute to feelings of belonging, empowerment and independence through actively connecting with others (Sandjaja 2011).
Recognizing the multi-dimensional nature of social support and building on previous research, Cutrona and Russell (1990, see p. 321 for a summary of different models) advance a five-dimension typology of social support that includes: information, emotional, network, esteem, and instrumental support. Cutrona and Russell’s (1990) typology is not reliant on identification of non-verbal or physical forms of support and is readily utilized in a text-based environment, so more suitable for use in an online community than some other social support typologies (Braithwaite, Waldron, and Finn 1999). Table 1 provides a brief description of each type of support with examples from Cutrona and Russell’s work and additional examples sourced from studies of online health communities.
Typology of Social Support {Cutrona & Russell, 1990 p. 322, paraphrased}.
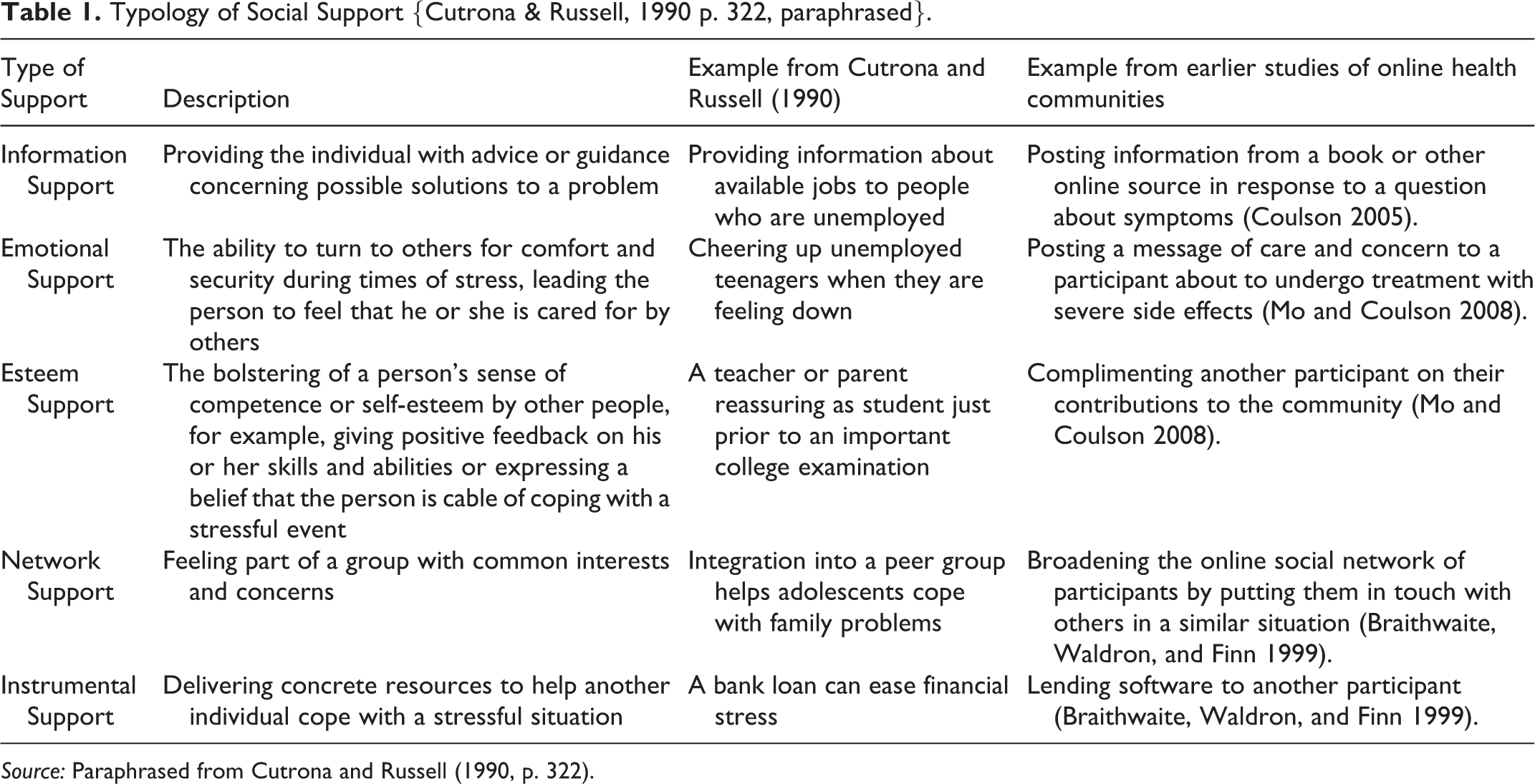
Source: Paraphrased from Cutrona and Russell (1990, p. 322).
Prior studies demonstrate the provision of all five forms of social support in online health communities, although few opportunities for instrumental support present themselves (Coulson 2005). Within an online context instrumental support or tangible assistance might include writing a protest letter on behalf of other participants or sending a gift (Mo and Coulson 2008), but these expressions of support are less common than the provision of information or esteem-building messages. Cutrona and Russell’s (1990) typology is a useful framework for identifying different types of social support, but it does not address consumer value as a function of both costs and benefits perceived in exchange (Zeithaml 1988). To consider the relationship between social support and consumer value, we turn to an existing marketing framework, Holbrook’s typology of consumer value (Holbrook 1999b).
Holbrooks’s Typology of Consumer Value
Holbrook’s (1999b) typology considers consumer value along three continuous dimensions, the first of which is described as an intrinsic-extrinsic continuum. Extrinsic value relates to the function of some item which is valued not for itself, but for its ability to perform a task. Holbrook provides an example of hammers and screwdrivers, valued for their functional ability to hammer a nail or screw in a screw. Intrinsic value by comparison is related to a consumption experience that is appreciated for itself, such as an excellent performance of a symphony orchestra. The second of Holbrook’s dimensions is that of self- or other-orientation. Self-oriented value is experienced directly by the consumer, whereas other-oriented value is captured only when some other person is also involved in the consumption experience. For example, an individual might participate in a charity bicycle ride in which the enjoyment and camaraderie of the ride are examples of self-oriented value captured by the participant whilst the recognition the individual receives from the charitable organization due to their fundraising effort is an example of other-oriented value. The third of Holbrook’s dimensions considers value as either active or reactive. Active value is created when a consumer does something, either physically or mentally, as part of a consumption experience. For example, a consumer reads a newspaper, actively enjoying their consumption of journalistic content. Reactive value is created when a good or service being consumed does something to or with the consumer, such as a beauty salon providing a visually pleasing manicure.
Holbrook’s typology uses these three dimensions to classify eight types of consumer value: efficiency, excellence, status, esteem, play, aesthetics, ethics and spirituality, each of which is described more fully in Holbrook’s own work (Holbrook 1999b). In a later study Holbrook (2006) organizes these eight types into four general value categories. Economic value encompasses efficiency and excellence while hedonic value includes play and aesthetics. Social value covers status and esteem whereas altruistic value includes ethics and spirituality. These general categories capture much of the same content in other typologies that refer to social, emotional and functional value (Sánchez-Fernández and Iniesta-Bonilla 2007; Sheth, Newman, and Gross 1991). For reference, Figure 1 shows Holbrook’s consumer value typology incorporating the eight value types and four general categories.
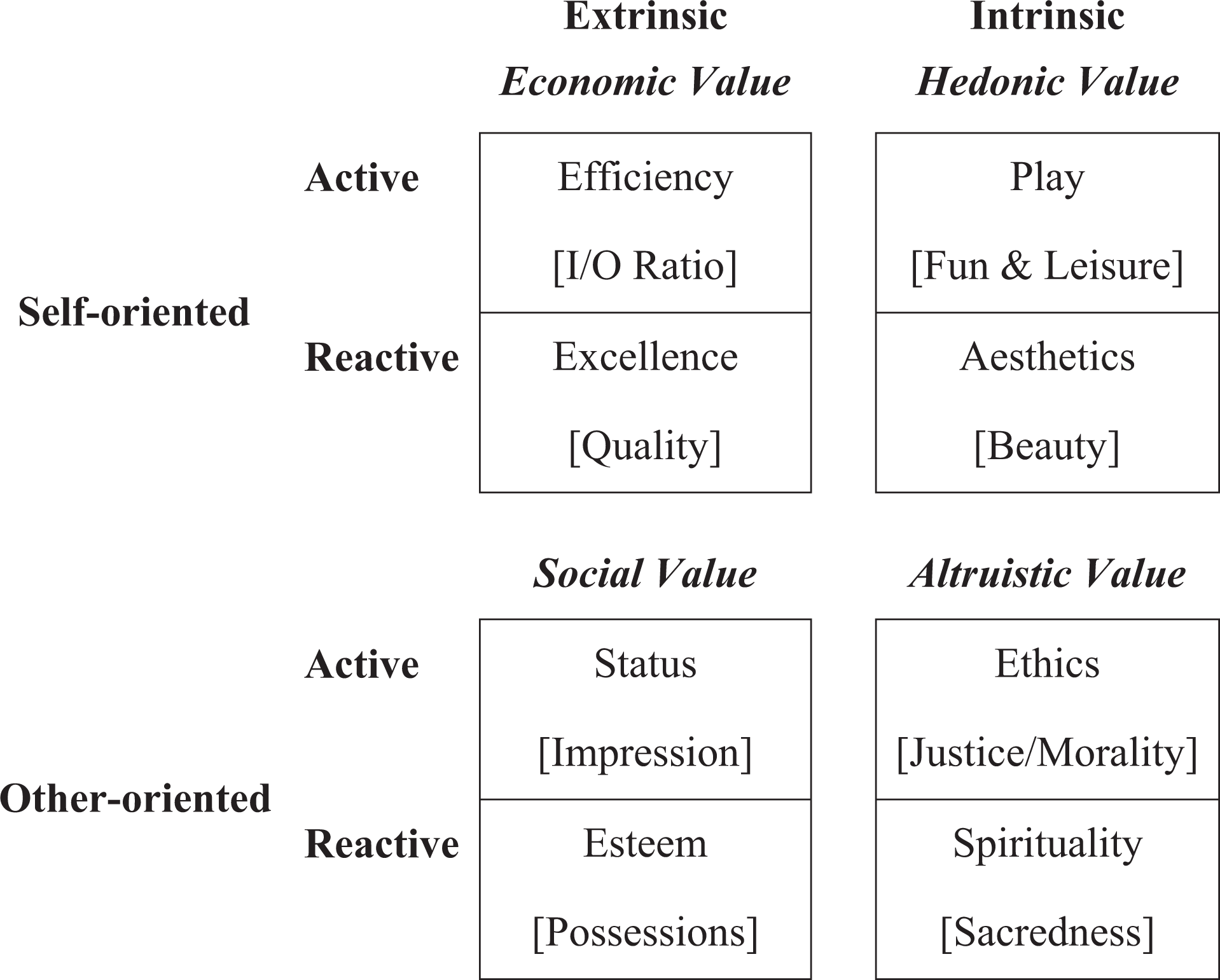
Holbrook’s typology of consumer value (adapted from Holbrook 2005, 2006).
Although much of Holbrook’s typology is consistent with the way in which consumer value is discussed in other research, the classification of consumer value into eight “types” has proved problematic. Critics complain that the eight types do not adequately address consumer value identified in their own research. For example, Richins (1999) has difficulty aligning benefits such as “personal growth” and “freedom” with any of Holbrook’s eight value types and Smith (1999) finds Holbrook’s description of ethics value too restrictive. Certainly many of the value types are evident in the brand community literature with a number of the studies touching on social, hedonic, economic and altruistic value (Muniz and O’Guinn 2001; Muniz and Schau 2005; Schau, Muniz, and Arnould 2009; Seraj 2012). These studies also distinguish additional consumer value types, ones that do not easily fit within Holbrook’s typology, the most noticeable being a sense of community with belonging and acceptance.
Holbrook’s eight types are not intended to be exclusive or exhaustive. The types are instead a guide as to how consumers might experience value. Additionally, the three dimensions of intrinsic-extrinsic, self-other orientation, active-reactive are each a continuum, meaning that value derived from a particular experience can be recognized in multiple ways (for examples see Holbrook 1999a, pp. 186–187) and can therefore fit into several of Holbrook’s “types” at one time. For example, a joke about symptoms shared between two online health community participants can cheer up both participants (esteem), demonstrate intelligence and wit (status), and entice participants into repeat visits in order to extend the enjoyable exchange (aesthetics and play). Thus, the experience may have some relevance to all of Holbrook’s “types”, although some are more relevant than others (play, esteem, status, aesthetics) depending where on each continuum the experience lies.
Holbrook’s (1999b) typology recognizes that value may be experienced differently by individuals participating in parallel consumption experiences and thus provides a suitable basis for guiding the exploration of value experienced in online communities that are used by participants in different ways and for different purposes (Kozinets, Hemetsberger, and Schau 2008). For example, Mathwick, Malhotra, and Rigdon (2002), assessing Holbrook’s “self-oriented” dimension of value, find that consumer value experienced in an online retail environment varies depending on whether the consumer is undertaking a goal-directed shopping task or an experiential shopping task. Their study examines four of Holbrook’s value types, paving the way for further research into other dimensions of consumer value. With the exception of the few studies already discussed (Misra, Mukherjee, and Peterson 2008; Nambisan and Nambisan 2009), there does not appear to be any recent published scholarship specifically exploring the concept of value within online health communities.
We argue that participants in online health communities both create and obtain value through one of the most widely recognized practices of online health communities, the generalized exchange of social support among peers (Ballantine and Stephenson 2011; Beaudoin and Tao 2007; Eichhorn 2008; Turner, Grube, and Myers 2001). The analytical model in Figure 2 illustrates the investigative process undertaken to identify the different types of social support produced within online health communities and discover how community members experience the value co-created. We apply our proposed model within two online health communities to examine the interplay of social support and consumer experiences of co-created value.
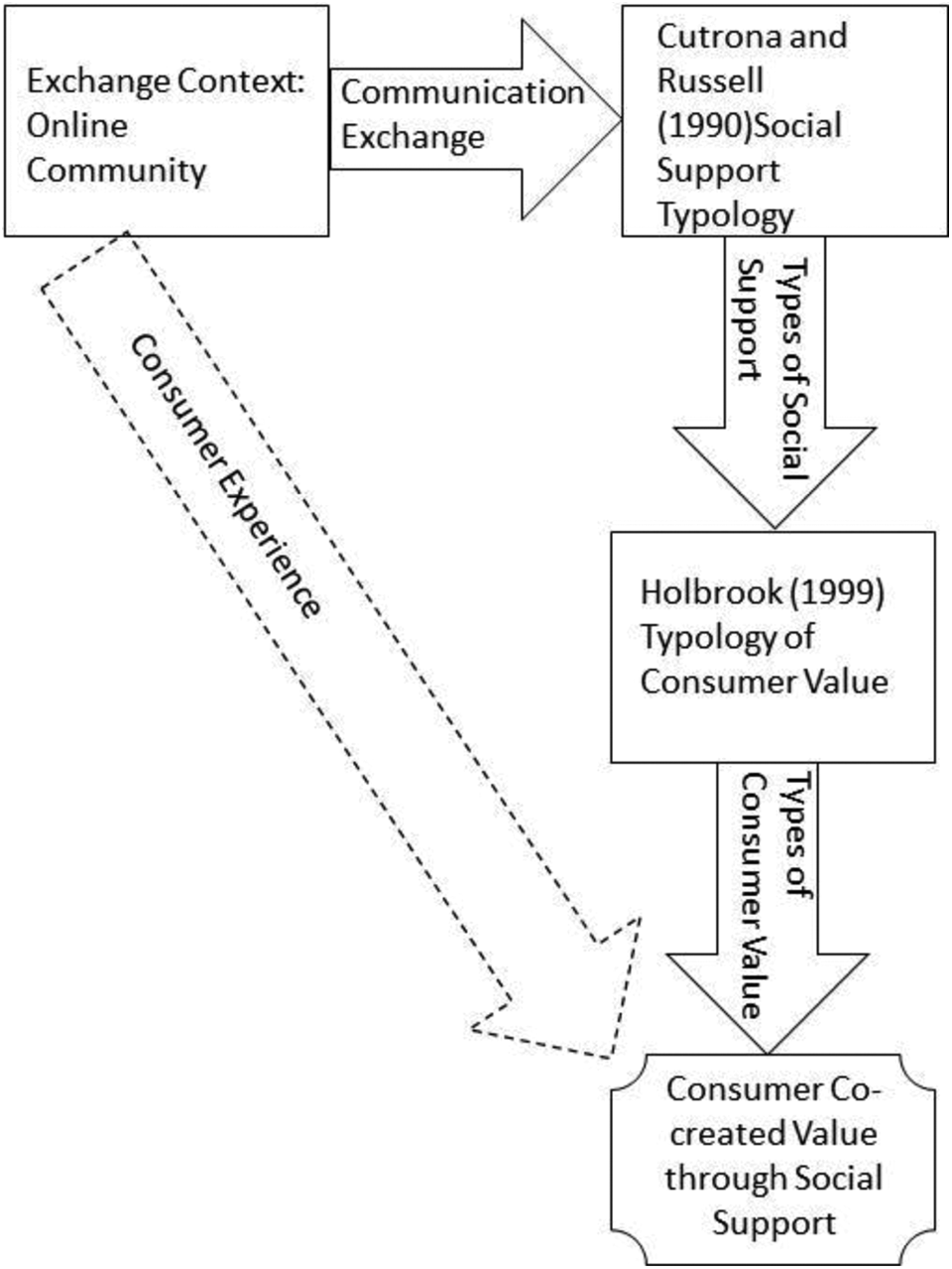
Analytical model.
Method
This qualitative study uses posts and full conversation threads collected from two online health communities to investigate the practice of social support as generating various types of co-created consumer value within the online community experience. In contrast to a grounded theory approach (Strauss and Corbin 1990), our consideration of consumer value is guided by, but not limited to, Holbrook’s value typology (Holbrook 1999b). Philosophers of science (Feyerabend 1975; Kuhn 1962) recognize all human understanding is inherently subjective, being informed either explicitly or implicitly by our experiences, beliefs, and theoretical perspectives. As such, the use of a theoretical framework as a guide to recognizing and identifying new phenomenon does not necessarily limit discovery, but in fact can actually encourage a more complete understanding (Hunt 1993; Kuhn 1962). Holbrook’s typology is used as its multiple dimensions provide for greater analytical granularity, prompting an exploration of some forms of consumer value that may otherwise be overlooked.
Context
The two online communities selected are for people with degenerative neurological diseases. One community is for Parkinson’s disease (PD) with around 2000 members and the other is for Motor Neuron Disease, also known as Amyotrophic Lateral Sclerosis (ALS), involving about 15,000 members. Both diseases are incurable and lead to severe disability and dependence. These online communities, characterized by patients with limited capacity for involvement in typical neighborhood community life, were selected as ideal demonstration sites for the importance of social support in creating value.
PD affects about 1% of the population over the age of 60 and 4%-5% by age 85. Between 5-10% of all cases present before the age of 40 (Rodrigues 2008). PD causes tremors, rigidity, decreased limb movement and postural instability, symptoms that may be accompanied by others such as pain, dementia, speech, and swallowing difficulties and depression (Lieberman and Williams 1993). The estimated cost of PD is more than $6 billion per year in the U.S. While PD has no known cause or cure, pharmaceutical treatments are available that retard or delay the progression of the disease by four to five years (National Institute of Neurological Disorders and Stroke 2003).
ALS affects neurons that control muscles relating to speech, breathing, swallowing and movement. Damaged neurons fail to activate these muscles, which gradually waste. Life with ALS is characterized by high levels of disability, and the disease is terminal (Ray and Street 2005). ALS has no known cause or cure (O’Brien, Kelly, and Saunders 1992). The average age of diagnosis is 55 years with most cases being diagnosed in people aged 40-70 (Ray and Street 2005). Typical life expectancy is three to five years following diagnosis (Buckley et al. 1983). The precise incidence of ALS is uncertain due to reporting differences between countries, but is considered to affect around one person per 100,000 (Chancellor and Warlow 1992).
Daily living is an immense challenge for patients and their care providers affected by these diseases. Participation in local community life, even medical appointments and face-to-face support groups, can be difficult as both mobility and communication are impaired. Research shows access to support through online health communities significantly benefits sufferers of these diseases, their care givers and their family members (Braithwaite, Waldron, and Finn 1999).
Procedure
Following Kozinets’ (2010, Chapter 8) discussion of ethical internet research, the research team made no contact with the members of the online communities. Accordingly, the names of the online communities are not published and pseudonyms used by participants are disguised with generic participant codes such as PD006 and ALS023. In addition, all quoted material is paraphrased and tested using Google search to ensure that the quotes cannot be traced back to the online community through an internet search. Care has been taken to ensure that the paraphrased quotes reflect the content and sentiment of the original post whilst using synonyms and altered phrasing to avoid tracing. This approach is consistent with that suggested by the British Psychological Society (2007).
Consistent with Liang and Scammon’s (2011) recent study of an online health community, data consist of full threads and individual posts to the online communities during an observation period of one month. Two separate units of analysis are required since individual posts, whilst suitable for identifying the solicitation and provision of social support, do not distinguish co-created value. To claim that value has been co-created, the researcher must examine the entire conversation threads containing multiple posts that include the provision of social support, acknowledgement of receipt and the resulting effect. The need for two separate units of analysis is best explained with a hypothetical example. Consider a post that would be familiar on almost any online health forum, a request for information about a drug treatment. Participant 1 posts a request for information about how side effects of a PD drug might be offset through dietary change. Participant 2 responds with dietary suggestions as well as empathy for Participant 1’s situation. The receipt of value (i.e. the information requested coupled with additional, unrequested emotional support) by Participant 1 is dependent on whether those suggestions are taken up and whether what the researcher believes to be emotional support is received as such. Only when Participant 1 reports back that the dietary changes have been successful, or that the emotional support offered has had a positive effect on his mood or ability to cope, is it apparent that value has been created.
Within the ALS community 133 members posted 499 times during the study period, initiating 61 threads with an average of 8.2 posts per thread. Thirty-five members of the PD community initiated 30 threads during the study period, comprising 137 posts with an average of 4.6 posts per thread. Both communities are characterized by participants posting detailed medical information regarding the management of symptoms. Concern has been expressed by doctors that consumer-initiated medical information posted on the internet may be inaccurate and even cause harm (Hardey 2001). To ensure the medical information collected as part of this study is valuable at a macro-level, a leading neurosurgeon assessed the medical information for inaccuracies. The medical assessment indicates that these two online health communities are able to self-monitor misleading information and the medical information shared is accurate. This approach responds to calls within the health literature for treatment and diagnostic information shared between participants of online health communities to be assessed by medical professionals (Coulson 2005; Finn 1999).
Data, along with any demographic information available, were loaded into Nvivo 9.2 (QSR International Pty LTD 2011) for coding and analysis. Consistent with Spiggle’s (1994) method for qualitative analysis, posts were first coded against Cutrona and Russell’s (1990) social support typology to understand how social support is delivered at a peer-to-peer level. Full threads were then examined for evidence of value-creation such as participants thanking one another, expressing appreciation for the community at large, or expressing positive outcomes from suggestions made by others. Coding was then checked by another one of the authors and a senior academic external to the project. The approach to coding social support, using the individual post as the base unit of analysis, is consistent with prior studies that analyze social support in online health communities (Drentea and Moren-Cross 2005; Eichhorn 2008; Malik and Coulson 2008; Mo and Coulson 2008). The use of full threads to identify evidence of value-creation is consistent with recent work by Laing, Keeling and Newholm (2011). Once the coding was considered complete, and based on the two levels of coding, intersecting coded threads and posts were identified for further consideration and analysis regarding the interplay between social support and consumer value. Additional themes beyond the original coding schema were identified at this time leading to a proposed extension to Holbrook’s typology, described further within the results section.
Results
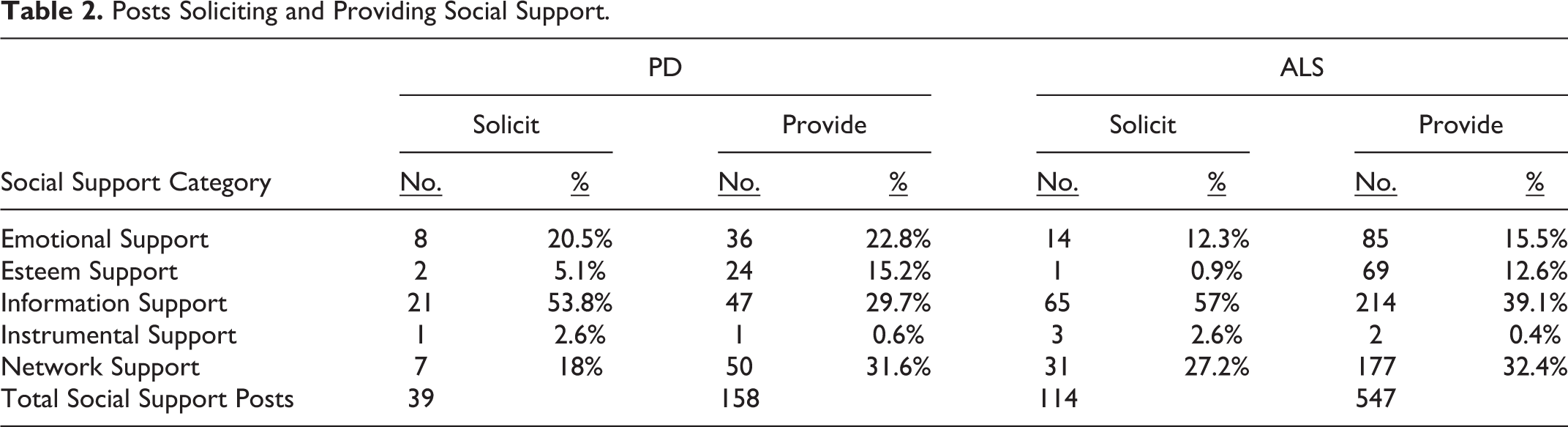
Table 2 shows the number of posts soliciting and providing social support within the two online communities. 1 Information support is provided most frequently within both communities, followed closely by emotional support. Low frequency of instrumental support (tangible assistance) is commensurate with the limited opportunities to provide instrumental support in an online environment.
Posts Soliciting and Providing Social Support.
Applying Holbrook’s (1999b) typology of consumer value to examine the entire conversation thread shows how different types of social support can deliver co-created value. A small number of example observations are provided as demonstrations of social support delivering co-created value.
Extrinsic and Self-orientated: Efficiency (Active) and Excellence (Reactive)
The most common reason for posting to an online community is to seek information, or to provide information in response to a request from another member. Information support leads to both efficiency and excellence. An example of efficiency is observed when PD013, who has not yet been diagnosed but is experiencing symptoms, asks the community what a “tremor” feels like in the early stages of PD. Responses in the form of information and network support arrive rapidly from participants in the UK, Ireland, Germany, U.S., and Canada. Within a day PD013 is able to thank people from around the world who have described their experiences of tremors (information support), assured her that she is not alone (network support) and offered empathy and compassion (emotional support). PD013 then asks more detailed follow-up questions about the tremor experiences. Her follow-up questions indicate co-created value, as she is able to gather additional support tailored to her specific information requirements. Gathering this level of first-hand information support and building a network of peer-advisors would have taken far longer, and more effort, if it were not for the inherent characteristic of an online community in which participants are geographically isolated but able to access one another at any time of day with minimal cost.
Excellence, or quality, (Holbrook 1999b) is experienced when the social support leads to a desired outcome. A number of posts request information, and the responses provided are of help to one or more recipients. The following illustrates this type of exchange. Participant PD008 posts a question about her body “freezing” and being unable to move: Does anyone ever experience freezing that lasts for hours on end? Please reply urgently. (PD008).
PD007 quickly responds, not with a personal anecdote, but with information support in the form of a large amount of data from a book or Internet resource on the subject of Parkinson’s disease with suggestions about how to “unfreeze.” PD008 posts again, indicating the excellence value received from this information: PD007, this is wonderful information. It is so valuable! I tried several of the methods you suggested and I have found one that works for me. I’m telling you it WORKS. I’m so excited!!!!!! I have been so worried about what would happen if I were alone and I froze, and now I have new freedom. Thank you PD007.
Consideration of PD007’s post in isolation does not demonstrate whether the information provided is of any value to PD008. PD008’s response is what demonstrates value co-created by PD008 trying the techniques provided by PD007 and solving her mobility problem. In this example we not only see excellence value in the information provided, but the conversion of that information into an improved quality of life for PD008 through applying the information provided by PD007. Even though excellence is a reactive form of value, PD008’s application of text-based information from an unknown community member with presumably no medical training converts a simple information request into much more. The exchange has given PD008 the ability and self-assurance to face difficult physical challenges.
Extrinsic and Other-oriented: Status (Active) and Esteem (Reactive)
Status, or impression management, is a form of value acquired through being admired or thought of in a positive light by others (Holbrook 1999b). Several times during the observation period PD007 posts large amounts of information sourced from the Internet and links to additional resources. PD007 is usually thanked by the recipient and this recognition contributes to PD007’s status as a provider of information support. Her involvement in co-creating status value for herself is evidenced by the following statement: I am good at locating information, so if you need assistance anytime please ask and I’ll try to help. (PD007)
A poignant example is demonstrated within the ALS community when ALS053 (wife and care giver) posts an update about her husband, ALS055, who is recovering from surgery for a tracheotomy. ALS053 and ALS055 are well-known community members and ALS053 berates herself online for persuading her husband to have this painful and difficult surgical procedure. The online community members respond with messages of emotional and esteem support to boost her confidence and reinforce her status as a loving and caring wife: You only followed the pulmonologists’ advice, so stop blaming yourself. (ALS054) Don’t be so hard on yourself. We all have to make hard decisions, and no one wants to be in our situation. (ALS017) You and ALS055 are super-loving, caring and amazing. You show the true meaning of marriage and I am in awe of both of you and your teamwork. (ALS057)
These posts provide an indication and verification of status: PD007 as a reliable provider of information and ALS053 as a compassionate and caring wife. These participants are engaged in co-creating status value by contributing posts that attract status-fulfillment responses.
Esteem value is similar to and often confused with status value (Holbrook 1999b). Whereas status value is experienced as admiration in the eyes of others, esteem value is a feeling of self-worth experienced by the individual. Table 2 shows esteem support is provided regularly, usually unsolicited, but few examples demonstrate participants actively co-creating esteem value. Those few examples indicate that participants co-create esteem value by offering something in the form of information support to the online community that in turn attracts praise and thanks. An example occurs when a participant posts a link to a site with information about ALS. This post attracts favorable responses from participants along with esteem building comments such as: Thanks for posting this. We tend to forget a lot about what we have learned and how far we have come. (ALS049) Good info. Helpful to us all. Many thanks (ALS022)
What remains unknown is whom, if anyone, gains esteem value from these esteem-building posts. This is an example of the difficulty of identifying co-created value within an online community. ALS049 and ALS022 have attempted to provide esteem support for other participants, but a reader or researcher cannot be certain how the esteem-building posts are experienced by the other participants. In one of the few examples, we see esteem support leading to co-creation of esteem value: Be positive and don’t let Parkinson’s Disease beat you. Continue to be positive for your lovely children. (PD005 as one of several posting to new member PD024). Now I know that I have virtual friends out there and I’m very grateful to you all. It’s really nice to hear words of encouragement. (PD024 posting back to PD005 and others).
Intrinsic and Other-oriented: Spirituality (Reactive) and Ethics (Active)
Holbrook (1999b, pp. 22–23) describes spirituality as “acceptance, adoption, appreciation, admiration or adoration of an “Other” where this “Other” may constitute some “Divine Power, some Cosmic Force, some Mystical Entity, or even some otherwise inaccessible Inner Being.” Within the period of observation a thread is posted indicating a level of spiritual value co-created between some of the community members. PD009 from Mexico posts information about her husband who is gravely ill with Parkinson’s-related complications. PD007 from Canada responds initially with emotional support indicating her deep regard for PD009: “You are an inspiring, devoted and very special woman.” This is then followed by a post of a spiritual nature from PD002 in the UK: I’m here for you, anytime. Sometimes when I am thinking about you I am sure you called my name and I turn to look for you. I am always with you in Spirit and I will never leave you alone.
Some participants refer to their experience with the online community as spiritual, and they express this to others through emotional support. For example: Hold on tight to us all dear Angel and when you feel more brave you can release your grip (PD002). You are all my invisible friends and I am so grateful to you all (PD024).
Ethics value is achieved through actions that are motivated by a desire to do the right thing by others (Holbrook 1999b). The following example, one of several observed within both communities, demonstrates ethics value in the context of a post that provides information, emotional and network support.
PD026 joins the PD community and posts a question asking the community to assess his self-reported symptoms and give him an indication of whether he has Parkinson’s Disease. The other community members offer helpful suggestions but refuse to discuss diagnosis. This post from PD002 is an example of how participants weave emotional support into a gentle refusal to diagnose: I hope you can keep smiling. It’s not a good idea for any of us on this forum to diagnose you because we are not doctors, we haven’t seen you and we don’t know enough about you. I know this must be frustrating, we can’t diagnose you with an incurable neurological disorder; can you understand? It would be best for you to see a “movement disorder neurologist.”
PD026 responds indicating that he has accepted the refusal and has received value from the emotional support provided. His gracious response contributes to the overall value co-created by participants in this and similar discussions that follow from requests for diagnosis: Thank you. I do understand, but I was hoping for some advice and insight, and I received both. I’m going to see a neurophysicist and I would like to see a movement disorder neurologist, but there are only a few of those in <name of country> and they have long waiting lists. Anyway, I thank you and I’ll stay in touch (PD026).
Intrinsic and Self-oriented: Aesthetics (Reactive) and Play (Active)
Holbrook (1999b, p. 19) refers to aesthetic value as “an appreciation of some consumption experience valued intrinsically as a self-oriented end in itself.” An example of aesthetic value is delivered through emotional support in the form of a poem about emotional strength posted by PD010. PD002 responds with her appreciation of the poem and of PD010’s gesture in posting it (esteem support): That poem is so beautiful, and so are you PD010. Thank you for posting this for all of us. It is truly appreciated and you are very thoughtful.
Play value (i.e., fun and enjoyment) is observed a number of times within both communities through the telling of jokes or amusing stories about symptoms and treatments. An example occurs when ALS024 posts a photograph of himself sitting in his new power-controlled wheelchair. Along with posts of admiration (esteem support) that provide status value, the following posts indicate play value experienced by the participants through supportive, shared banter that reinforces their involvement in a community of others, many of whom are also wheelchair-bound (network support). Nice wheels. Did the matching shades come with it? (ALS026) Great colour, and they say men have no taste! (ALS028) Nice wheels! Watch out for the cat’s tail! (ALS032) He’s right. I ran over my dog’s tail the first week I had my chariot. (ALS033)
Emerging Theme: Community Value
Other threads in the data show intrinsic, self-oriented active value is much more than just playful fun. Throughout the period of observation, participants’ posts indicate that they find the act of social support exchange within the online forum to be a valuable experience in itself, and by reading and responding to others’ posts they are involved in the co-creation of that value. An example occurs when PD024 introduces herself as a new member and tells the story of her symptoms, diagnosis and family situation, receiving information and emotional support in return. Then, through delivery of esteem support back to the community members, she expresses her appreciation of the online community experience: Thanks everyone for being there. I’m still learning how to use this site, but I feel a lot better knowing that I have friends out there who can relate. My husband can’t, but he’s trying.
Members of the ALS community regularly acknowledge the appeal of the online community experience. An example is posted by ALS046, again in the form of esteem support: I want everyone to know that we have a lovely community here. It’s the people who make this such a great place to hang out. Many of you make me smile, and I look forward to catching up with you.
These are not isolated examples. Participants time and time again use effusive language to describe their appreciation of the online community experience and the cohesion that exists between participants despite the absence of face-to-face contact. The concept of perceived cohesion, which encompasses “an individual’s sense of belonging to a particular group and his or her feelings of morale associated with membership in the group” (Bollen and Hoyle 2000, p. 482), is an excellent description of the value participants are experiencing as a consequence of their involvement in the online health communities. Appreciation and enjoyment of belonging to a group, combined with satisfaction, develops from the only form of social interaction available to many of these chronically sick or disabled participants. Many primarily seek information support, yet experience value through other forms of support, namely emotional, esteem and network support. These additional forms of support that emerge through the online community experience build the sense of communitas (Arnould and Price 1993; Turner 1969) that is possibly the most valuable outcome for those who are unable to participate fully in everyday public life.
Discussion
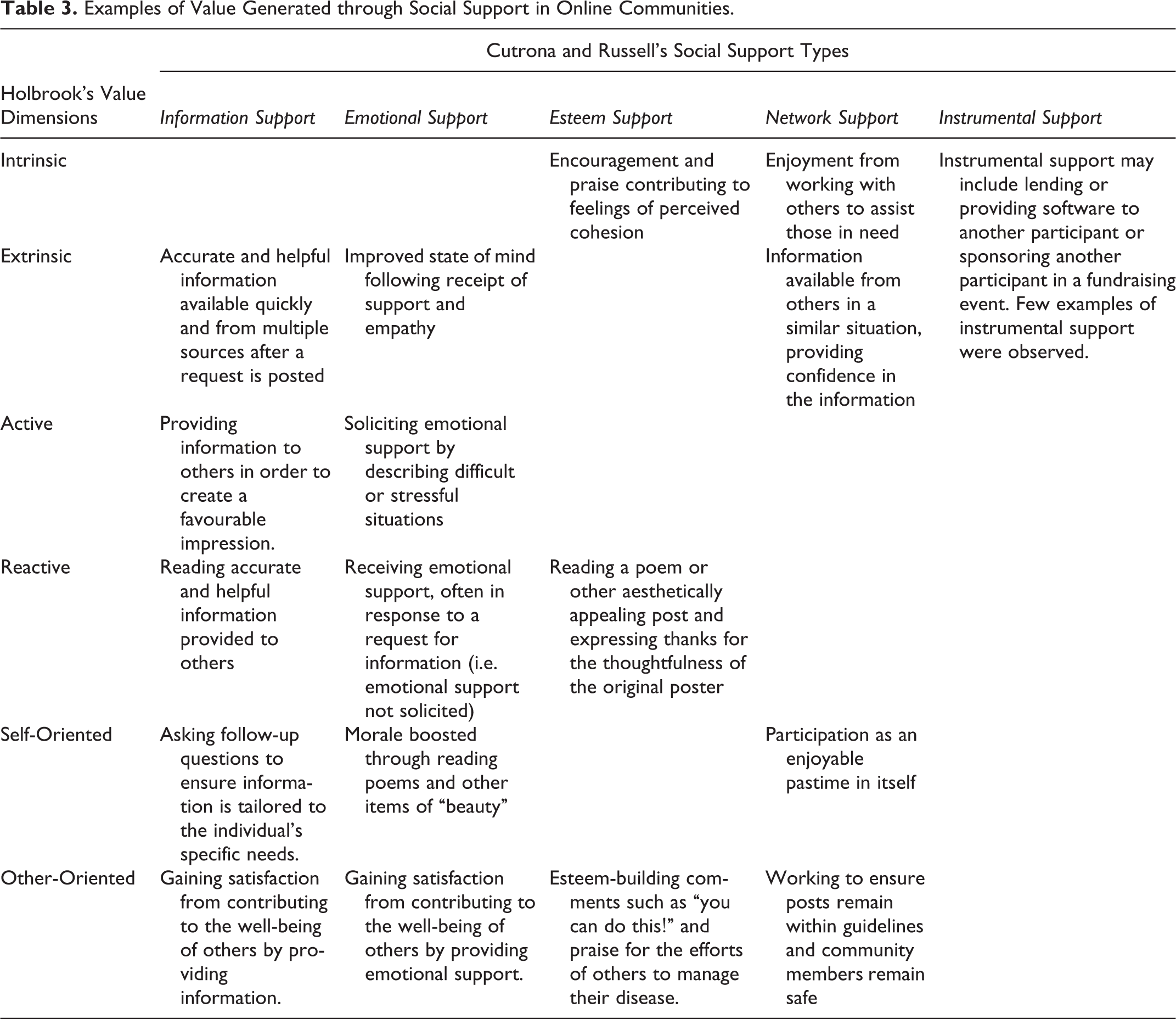
Prior studies investigating social support within online health communities focus on individual and collective behavior without links to the co-creation of consumer value (Ballantine and Stephenson 2011; Fischer, Bristor, and Gainer 1996). Whilst the confirmation of co-created value can be elusive, results demonstrate members of online health forums participate and experience the co-creation of different types of consumer value through the exchange of social support. Table 3 gives examples of the observed relationships between types of social support provided and co-created value experienced by participants during the period of observation. Some community members experience spiritual value through bonds built with others over time, others experience esteem value from esteem support provided. Play value is experienced through the enjoyment of being part of a community (network support) and aesthetic value through reading and responding to beautiful poems or videos (esteem and emotional support). Some gain ethics value from contributing to the well-being of others (network support).
Examples of Value Generated through Social Support in Online Communities.
Recalling that the participants in these particular online communities are often quite disabled and highly dependent with limited potential for conventional social contact, it is possible that some members of the community enter a liminal state in which the lack of physical capability is left behind on the “outside” and they enter a virtual world in which they are all competent, capable members of social network who can both create and experience value by providing support to others (Turner 1969, 1983). The public nature of the online communities means that the social support and derived value are available to all kinds of participants, patients, doctors, family members and even researchers. The obvious advantages within the PD and ALS communities are for those who are suffering the physical challenges associated with these diseases. Online communities give these individuals the opportunity to contribute on an equal basis with all other members and can share equally in the resources of the community, thus creating value with and for themselves and others. A sense of “communitas” develops within the online community as participants work together to create a shared, safe and supportive environment for those who are affected by these diseases (Arnould and Price 1993; Turner 1969).
Holbrook’s three value dimensions provide a useful structure to explore consumer value, but they do not adequately capture the value that highly disabled and dependent patients experience from operating in an online social community of both abled and disabled people equally contributing to the well-being of others. This form of intrinsic, active value that is both self and other-oriented is much more than either “ethics” or “play”, especially in a context where consumers are experiencing and enjoying what may be their primary means of social exchange. Other consumer value frameworks offer even less guidance as to the nature of the value experienced from this form of collective activity, providing only broad categories such as “emotional value” (de Ruyter et al. 1997; Sánchez-Fernández and Iniesta-Bonilla 2007; Sheth, Newman, and Gross 1991) or “satisfaction” (Zeithaml 1988). Prior work in online brand communities identifies the spiritual or quasi-religious communion that can occur between participants who are committed to a particular brand and spend time online evangelizing that brand (Kozinets 1999; Muniz and Schau 2005). Members of an online health community do not evangelize their disease nor are they committed to a “brand” but, like members of brand communities, they demonstrate value from their collective experience. Further work is needed to fully understand the nature of consumer value experienced as an outcome of collective experience in different contexts.
Two communities within a limited observation period only introduces the potential for this line of research, but the time is right for such research due to its intersection with a number of areas of scholarship receiving noticeable attention. First is the notion that consumers are involved in the co-creation of the value experienced through consumption activities (McColl-Kennedy et al. 2012; Nambisan and Nambisan 2009; Vargo and Lusch 2004). Second, research into online forums and other consumer activity on the Internet as a source of rich data is maturing in terms of methodology and ethical practices (Hine 2005; Joinson 2005; Kozinets 2010). Third, scholars are questioning the term “co-created value” and looking more deeply into what value means to the consumer (Füller et al. 2009; McColl-Kennedy et al. 2012). This research study sits at the intersection of those three areas, extending prior work in the study of co-created value in the context of online health communities.
Limitations and Directions for Future Research
Passive observation in the collection of posts is the data collection method most frequently used for studies of online health communities to avoid intrusion into the social networks of a vulnerable population (Braithwaite, Waldron, and Finn 1999; Coulson 2005; Coulson, Buchanan, and Aubeeluck 2007; Coulson and Kniff 2007; Malik and Coulson 2008, 2010; Mo and Coulson 2008). Analysis of online discourse between community members in “native” form, with no influence from research professionals and no narrowing of context via survey instruments, can be seen as a strength of this method and of this study. A limitation of this data collection method is that it can only ever reveal a point-in-time snapshot of the online community, and researchers may misinterpret observed online behavior. Online and face-to-face interviews have been shown to provide deeper insight into the online community experience in both health (Kivits 2005; Laing, Keeling, and Newholm 2011) and non-health (Hine 2000; Orgad 2005) contexts while providing an opportunity for the researcher to clarify observed behavior directly with respondents. Online surveys of community participants are used to explore consumer experience across a number of different online communities (Beaudoin and Tao 2007). Further study involving a combination of methods exploring one or more online health communities is likely to provide a richer level of analysis. Additionally the inclusion of direct contact between the researcher and participants would enable a more comprehensive exploration of the role of the online community in the wider support environment of participants.
A researcher may be tempted to assume that co-created value in the online communities selected for this study will generalize to other online health communities, however that is not necessarily the case. Value is perceived differently by individuals, and cultural differences between online communities may impact the extent to which social support is perceived by participants as a form of value (Seale 2005). Other constructs should also be explored for their potential to contribute to co-created value. For example, studies investigating consumer well-being (Sirgy, Lee, and Rahtz 2007) and quality of life (Achat et al. 1998; Malhotra 2006) within online health communities may provide further demonstrations of co-created value beyond those identified within this study using social support.
Additionally, the perceived cohesion (Bollen and Hoyle 2000) and communitas (Arnould and Price 1993; Turner 1969) experienced by participants in the two communities included in this study are unlikely to be characteristic of all online health communities. Further investigation is needed to identify what features of an online health community promote this sense of community through shared experience.
All of the cited studies of social support within online health communities use qualitative research methods, consistent with the dominance of qualitative methods in this research context (Hamm et al. 2013). To date, we have been unable to locate a study that explores the relationship between social support and consumer value within an online health context and the qualitative results demonstrated in this study need to be validated with further empirical work. As the internet-enabled population becomes older, and demands on medical services in Western countries increase, online health communities may become a form of service that is operated by (or recommended by) medical service providers and Health Departments to supplement face-to-face services for people with particular health problems. Understanding which health problems are most suited to online peer-generated support is a key issue for the future, as is the understanding of how the structure and operational mode of the online community contributes to the perceived value of the experience. A wider panel survey with respondents from a variety of different online communities might begin to identify whether particular online communities’ features or modes of operation provide greater value to participants. A wide-ranging survey could also explore whether particular categories of health issues are more suited to online community participation.
Finally, this research focuses solely on consumer value within consumer-led communities. Health care organizations that sponsor online health communities need to consider value captured by both the consumer and the sponsoring organization. Such online communities need to be able to demonstrate a return on investment for the firm (Cothrel 2000), which is not captured using Holbrook’s (1999b) consumer-focused typology.
Conclusion
With health central to quality of life and a just society, healthcare and associated health delivery mechanisms are a concern for macromarketing systems. This research highlights the importance of peer-to-peer health networks that remove barriers of information asymmetry and provide value and support to vulnerable people.
Previous work exploring consumer value within non-health online communities identify relationships between consumer value and the constructs of social capital (Mathwick, Wiertz, and de Ruyter 2008), personal fulfillment, and collective action (McLure Wasko and Faraj 2005). Clearly the consideration of consumer value, and in particular consumers co-creating value with peers, has merit in the study of health delivery. Research by McColl Kennedy et al. (2012) explores the means by which consumers co-create value within face-to-face health encounters. This study extends that work by considering consumer co-creation of value within online health communities using Cutrona and Russell’s (1990) social support typology and applying Holbrook’s (1999b) established consumer value framework to analyze the ways in which consumers experience value.
This demonstration has theoretical significance in a new application of existing marketing theory (Holbrook’s typology) to further our understanding of the concept of value co-creation. Our study identifies the need to extend Holbrook’s typology to include intrinsic, self-oriented, active value that is not only related to “play” but encompasses feelings of cohesion and connectedness with others. We also identify the need for researchers studying value within online communities to examine the entire thread of conversation rather than individual posts, as the thread represents a series of communications that build value whereas an individual post represents only what one person chooses to communicate, with no indication that value is captured by other participants.
This study also has practical significance, further developing our appreciation and understanding of the value of online community life for people with serious illnesses and limited capacity for meaningful engagement in conventional community life. Specifically, this study is of practical significance to health professionals and health service managers as it demonstrates that health consumers create value with or without the involvement of health practitioners (who are absent in both of the communities studied). In situations where patients may be physically dependent on health professionals and family members to locate support resources, carers of such patients should understand the value of online community life and potential support benefits of online community interaction.
This study points to the need for policy makers to understand that the health system, as perceived by consumers, must deliver more than medical solutions. Health consumers seek forms of consumer value that deliver quality of life across a spectrum of which medical treatment is only one part. Esteem, play, aesthetics, spirituality and ethics all form part of a consumer’s concept of value derived from encounters with health service systems. This study demonstrates that consumers can and will create those forms of value together if they have the means to do so.
Footnotes
Acknowledgement
The research team would like to thank Dominic Rowe, Professor of Neurology at the School of Advanced Medicine, Macquarie University Hospital, for his generous assistance with this project. The research team also acknowledges the generous and constructive comments of the anonymous reviewers, which have considerably strengthened the analysis and findings of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.