
Abstract
Background
The efficacy of susceptibility-weighted imaging (SWI) for detecting intracranial bleeds (ICBs) in patients with mild traumatic brain injury (MTBI) has not been directly compared to that of T2*-weighted gradient-recalled-echo imaging (T2*WI). Further, its prognostic value for MTBI patients remains unproven.
Purpose
To compare the sensitivity of ICB identification between SWI and T2*WI and examine the prognostic value of SWI for MTBI patients.
Material and Methods
T2*WI, SWI, and clinical information of 63 MTBI patients were collected. Sensitivity was compared between T2*WI and SWI for ICB identification, and statistical analysis was conducted to understand the correlations between SWI and clinical characteristics.
Results
ICBs were detected in more patients (47 vs. 35, P < 0.001) and more ICBs were detected (276 vs. 147, P < 0.001) on SWI than T2*WI. On SWI, patients with conscious disturbance showed higher ICBs prevalence (84.6% vs. 58.3%, P = 0.020), and more patients from the post-concussive syndrome (PCS)(+) group than the PCS(−)group were ICBs positive (86.1% vs. 59.3%, P = 0.015). The numbers of ICBs were significantly higher in the PCS(+) group than the PCS(−) group (P < 0.001). Significant correlation was found between PCS and ICBs number (r = 0.510, P < 0.001). Multiple logistic regression analysis showed that ICB number was an independent variable predicting occurrence of PCS.
Conclusion
SWI is more sensitive than T2*WI in detecting hemorrhagic foci in MTBI patients and may offer valuable prognostic information regarding these patients, for example, information on PCS. Further, cerebral parenchymal hemorrhage may affect long-term outcomes in MTBI patients.
Keywords
Introduction
Traumatic brain injury (TBI) is common clinically, with an estimated incidence of 538.2 per 100,000 individuals in USA and 235 per 100,000 individuals in Europe (1,2). In most cases, TBI can be classified as mild TBI (MTBI), accounting for about 70–90% of all patients universally and 62% patients in eastern China (3,4). However, these rates may be underestimated because most individuals who sustain MTBI either consult their primary care physician days after the injury or seek no care at all. MTBI patients may recover fully or at least have a favorable prognosis if diagnosed and treated on time. However, MTBI is often challenging to diagnose and can be easily neglected, because of rapid resolution of acute signs and symptoms, and the typical absence of objective evidence of injury on conventional neuroimaging.
Computed tomography (CT) and conventional spin-echo (or turbo spin-echo) sequence have limited sensitivity in detecting intracranial bleeds (ICBs) and therefore find restricted use in assessing the severity of MTBI (5,6). Two-dimensional (2D) T2*-weighted GRE sequences (T2*WI) have been used for imaging cerebral microbleeds and show high sensitivity (7). However, Haacke et al. (8) presented a new three-dimensional (3D), fully velocity-compensated, gradient-echo sequence, which they referred to as susceptibility-weighted imaging (SWI). Combined with its higher spatial resolution, SWI at 1.5 T was reported to be more sensitive than T2*WI in identifying hemorrhage in patients with diffuse axonal injury and those with acute cerebral infarct (9). This may also hold true in the case of MTBI. While it has been proved to detect significantly more lesions than traditional sequences in patients with TBI (10), it has not yet been directly compared with T2*WI in MTBI patients. Additionally, its ability to translate its sensitivity into useful prognostic information remains unproven. Thus, this study aimed to compare SWI and T2*WI in terms of identifying ICBs in MTBI patients and determine whether SWI at 3.0 T offers useful prognostic information regarding MTBI patients.
Material and Methods
Patient selection and data collection
This study was approved by institutional review board of our hospital. Sixty-three patients admitted to the neurosurgery department of our hospital from November 2009 to July 2012, who met the inclusion criterion for MTBI, were enrolled. Informed consent was obtained from all patients at least 3 days after injury ensuring that they were adequately conscious. According to American Congress of Rehabilitation Medicine and World Health Organization Collaborative Center Task Force on Mild Traumatic Brain Injury (11–13), the inclusion criterion for MTBI is acute brain injury resulting from mechanical injury to the head from external physical forces, as manifested by at least one of the following: (i) any consciousness disturbance lasting approximately or less than 30 min; (ii) confusion, disorientation, or post-traumatic amnesia (PTA) for less than 24 h; (iii) focal neurological deficit(s) that may or may not be transient, such as headache dizziness, seizure, vomiting, and intracranial lesion not requiring surgery; (iv) Glasgow coma scale (GCS) ≥13 when examined 30 min after injury. MTBI must not be due to drugs, alcohol, medications, other injuries, or treatment for other injuries (e.g. systemic injuries, facial injuries, or intubations), other problems (e.g. psychological trauma, language barrier, or co-existing medical conditions), or penetrating craniocerebral injury (13). Patients with a history of cerebral infarction, hemorrhage, neoplasm, vascular malformation, or myelinopathy were excluded. All patients underwent T2*WI and SWI brain scans within 1 week of injury.
Information on patients' demographic data, clinical presentations at admission, mechanisms of trauma, imaging manifestations, treatments, and follow-up outcomes was recorded. All patients were followed up for 7–15 months (median, 11 months) to evaluate the presence of post-concussive syndrome (PCS). PCS was defined as a set of physical, behavioral, or emotional symptoms, with at least two of three cognitive items, namely: (i) a period of unconsciousness lasting more than 5 min; (ii) a period of post-traumatic amnesia that lasts more than 12 h after closed head injury; and (iii) a new onset of seizures (or marked worsening of a pre-existing seizure disorder) within the first 6 months after the closed head injury. Further, three or more of the following symptoms must persist for at least 3 months following closed head injury: easy fatigability; disordered sleep; headache; vertigo or dizziness; irritability or aggression on little or no provocation; depression, anxiety, or affective instability; lack of spontaneity or apathy; or a personality change (such as social or sexual inappropriateness) (14,15).
Imaging technique
All cerebral T2*WI and SWI scans were performed on Magnetom, Trio 3.0T, MRI scanner (Siemens, Erlangen, Germany), with an 8-channel phased-array head coil. Routine scanning for transverse sections was performed with T1W turbo spin-echo sequence (TR/TE, 550/15 ms), T2W turbo spin-echo sequence (TR/TE, 4500/100 ms), and fluid-attenuated inversion recovery sequence (TR/TE/TI, 8500/120/2500 ms). T2*WI was obtained using 2D phase spoiled GRE sequence with the following parameters: TR, 620 ms; TE, 20 ms; flip angle, 20°; matrix, 256 × 204; field of view (FOV), 220 × 220 mm; 19 slices; slice thickness, 5 mm; interslice gap, 1.5 mm; voxel size, 1.1 × 0.9 × 4.0; band width, 200 Hz/pixel; averages, 1; acquisition time, 2 min 9 s. SWI were obtained with high-resolution 3D phase spoiled and fully velocity compensated gradient-echo sequences. To accelerate acquisition, the generalized auto-calibrating partially parallel acquisition algorithm was applied with a reduction factor of 2. The imaging parameters were as follows: TR, 60 ms; TE, 31 ms; flip angle, 15°; slice thickness, 1.2 mm; inter-slice distance, 0.2 mm; in-plane resolution, 0.5 × 1.0 mm; FOV, 230 × 173 mm; matrix, 320 × 294; band width, 120 Hz/pixel; averages, 1; acquisition time 5 min 5 s. The phase images were high-pass (HP) filtered to remove background field effects and contrast-enhanced SWI magnitude images were created from the HP filtered phase images (8). Minimum intensity projections (mIPs) were performed over five slices centered on the slice of interest (8). Focusing on the central slices, all magnitude images, HP-filtered phase images and SWI mIPs were reviewed.
Image review
Blinded to the clinical data, two experienced radiologists (both with more than 10 years of experience in reading neurological MR images) evaluated the T2*WI and SWI images. The images were randomly allocated to one of these two reviewers. T2*WI images were first read in random order, and 1 week later, the SWI images were read, again in random order. Consensus was achieved after discussion. The reviewers assessed the scans for number, shape, size, and distribution of intracranial bleeds. The following seven brain regions were observed: the cortex, subcortical white matter, external capsule (EC)/internal capsule (IC), thalamus, basal ganglia gray matter, brainstem, and cerebellum. Lesions were localized to: (i) superficial, including cortex and subcortical areas; (ii) deep, including areas of EC/IC, thalamus, basal ganglia gray matter; or (iii) posterior-fossa, including brainstem and cerebellum. If lesions spanned multiple regions, they were assigned to the region with the majority of lesions. For both T2*WI and SWI, hemorrhagic lesions were defined as hypointense black dots-like regions, when cerebral micro-blood vessels, calcifications, intracranial air, extraneous materials, and skull base artifacts were excluded based on CT and SWI HP-filtered phase images. When an ICB was suspected on magnitude, HP-filtered phase or SWI mIPs, all three types of images were reviewed.
Statistical analysis
For each sequence, the inter-observer reliability for ICB evaluation was examined using Cohen k test. k values ≤0.4 indicated poor agreement, 0.41–0.6 indicated moderate agreement, 0.61–0.8 indicated good agreement, and ≥0.81 indicated excellent agreement. The Wilcoxon sign-rank test was used to analyze the difference in detected lesion number between T2*WI and SWI. The Pearson chi-squared test and Fisher's exact probability test were respectively used to identify differences in ICBs prevalence and distribution between T2*WI and SWI. Patients were divided into consciousness disturbance positive (CD(+)) and negative groups (CD(−)), PCS positive (PCS(+)) and negative groups (PCS(−)), and ICBs positive (ICBs(+)) and negative groups (ICBs(−)), respectively. Differences in prevalence or mean value between these group pairs were tested using the Pearson chi-squared test or Student t-test. The Wilcoxon rank-sum test (Mann-Whitney) was performed to identify differences of ICBs numbers between the PCS(+) and PCS(−) groups. Receiver operating characteristic curve (ROC) analysis was performed to compare sensitivity of SWI and T2*WI in predicting PCS. The relationship between ICB number and PCS status was analyzed using the Spearman correlation and multiple logistic regression analysis. All statistical analyses were conducted using SPSS 20 (IBM SPSS, Chicago, IL, USA). Significance was defined as two-tailed P < 0.05.
Results
Patients' clinical characteristics
Patients' clinical information.
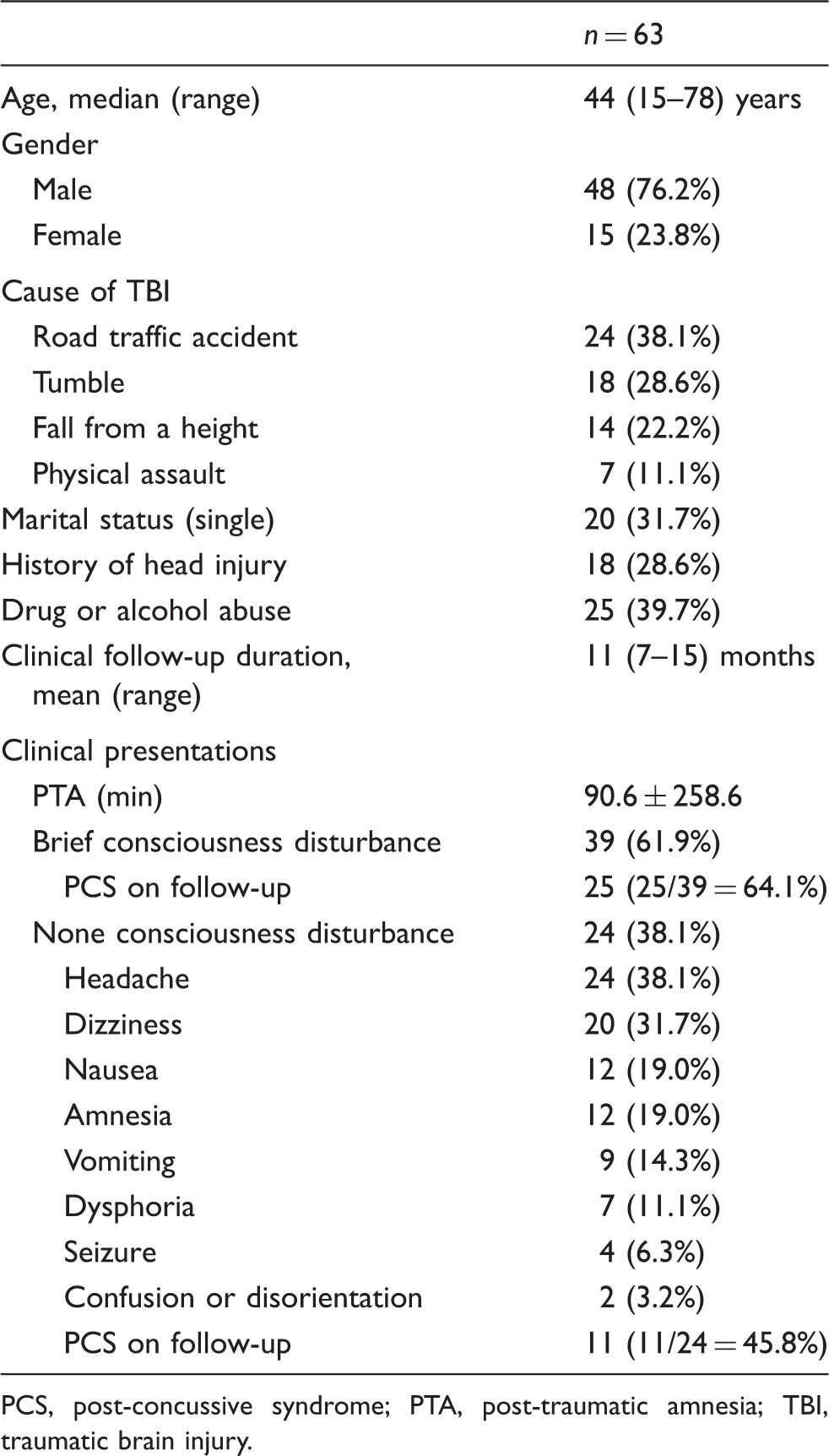
PCS, post-concussive syndrome; PTA, post-traumatic amnesia; TBI, traumatic brain injury.
Statistical comparisons of PCS incidence and ICB prevalence between patients from the CD(+) and CD(−) group.
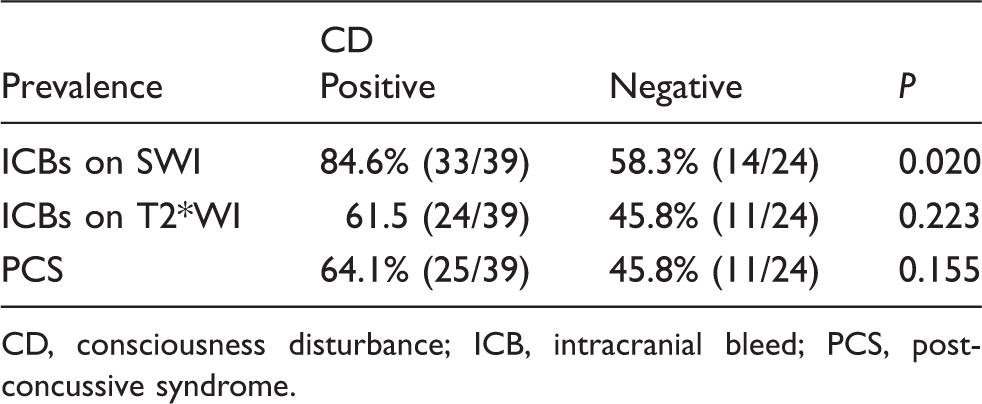
CD, consciousness disturbance; ICB, intracranial bleed; PCS, post-concussive syndrome.
Imaging features
The inter-observer reliabilities were good when analyzed both at individual level (T2*WI, k = 0.72; SWI, k = 0.83) and at the ICB level (T2*WI, k = 0.81; SWI, k = 0.87).
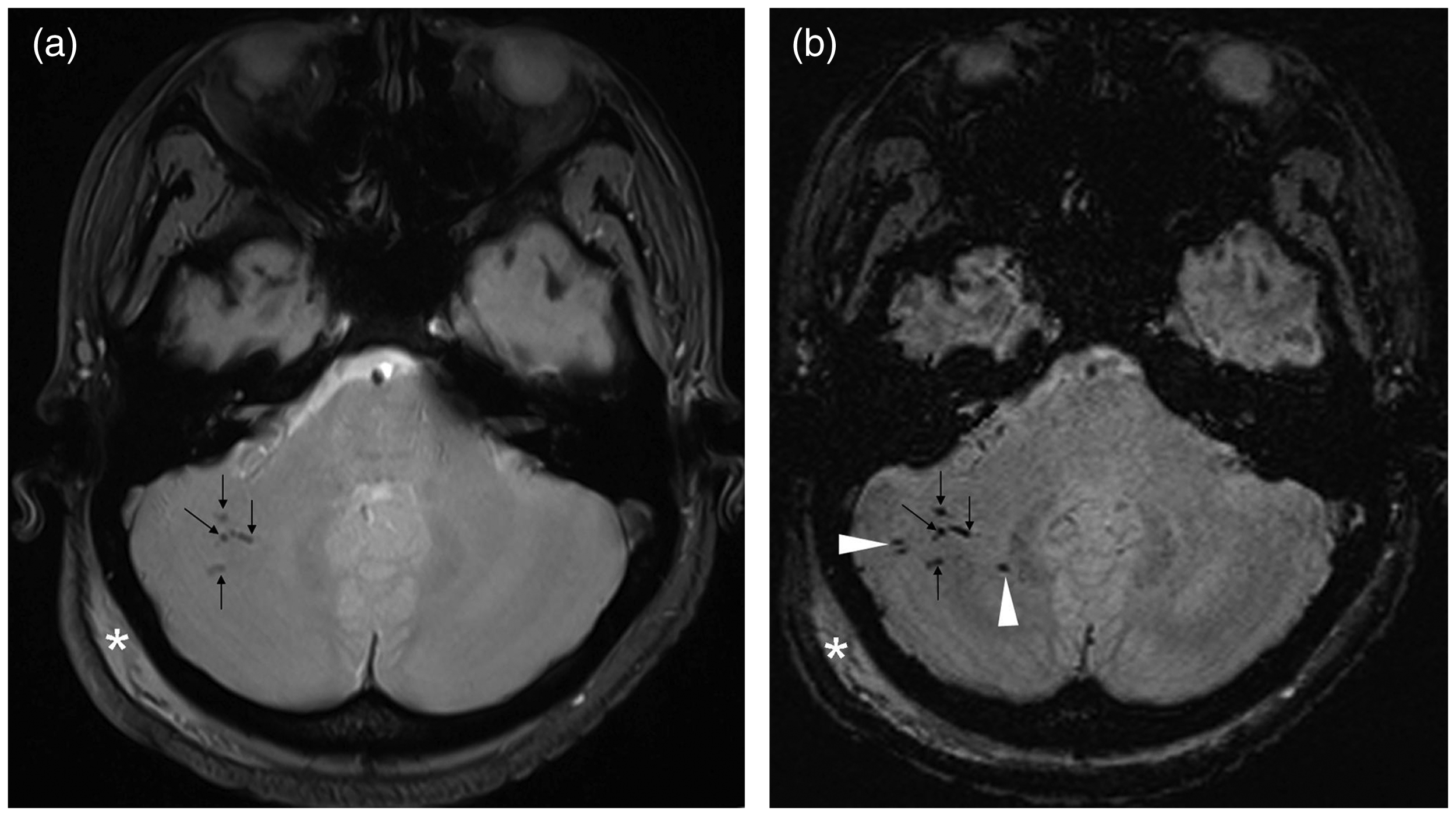
On SWI and T2*WI, ICBs presented as stippled, round to oval, or annulus-like hypointense signals (Figs. 1, 2), which were predominantly located in superficial areas (Fig. 1), but less commonly in posterior fossa (Fig. 2, Table 3). When multiple lesions were present, they tended to be multi-clustered or bead-like (Figs. 1, 2). The number of lesions were in the range of 1–19 on SWI and 1–13 on T2*WI, with total (median) number being 276 (5) and 147 (3), respectively (Table 3).
A 41-year-old man was admitted with headache and dizziness caused by violent assault. (a) 2D T2*WI scan on admission showed several blurry bead-like ICBs clustered in the left parietal cortex and subcortical area (arrows). (b) SWI scans taken around the same time showed more ICBs (arrowheads), which were better demarcated (arrows and arrowheads) than those on T2*WI. Diffused axonal injury was diagnosed. Injury to the left parietal scalp was found on both images (asterisks), which was consistent with the cerebral parenchymal abnormalities. The patient was diagnosed with PCS 3 months later. A 37-year-old woman was admitted with short-term consciousness disturbance, headache and dizziness, because of a fall from a height. (a) T2*WI scans showed couples of blurry ICBs clustered in the right cerebellar lobe (arrows). Additional clearer lesions (arrowheads) were seen on SWI scans (b) obtained on the same day. Images from both sequences showed edema in the right occipital scalp, which was consistent with the brain injury in the right cerebellar lobe (asterisks). Comparison between T2*WI and SWI. Percentage values are shown in parenthesis. Pearson chi-squared test. Fourteen patients showed no ICBs on either sequences. Wilcoxon sign-rank test. Fisher's exact probability test.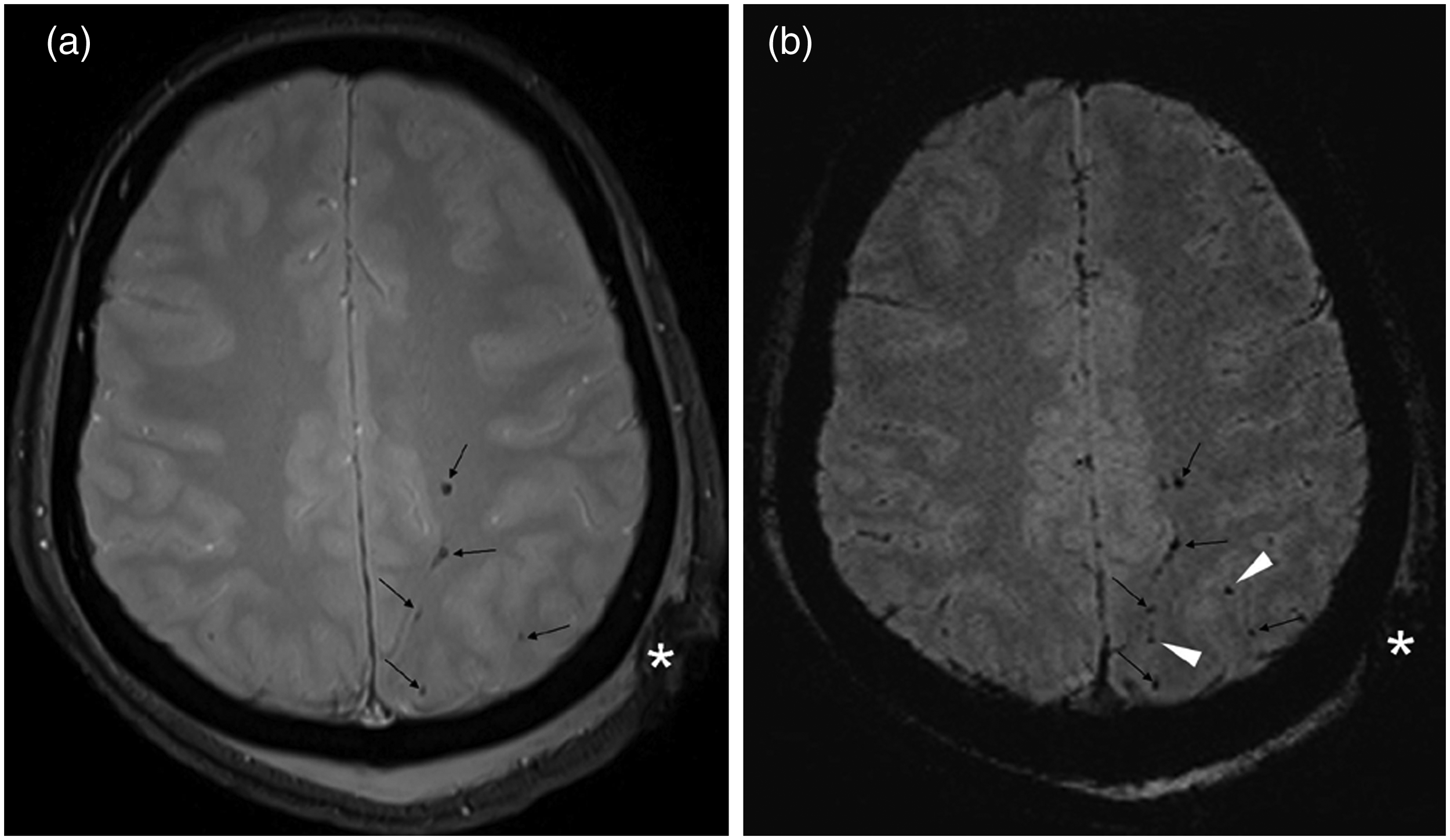
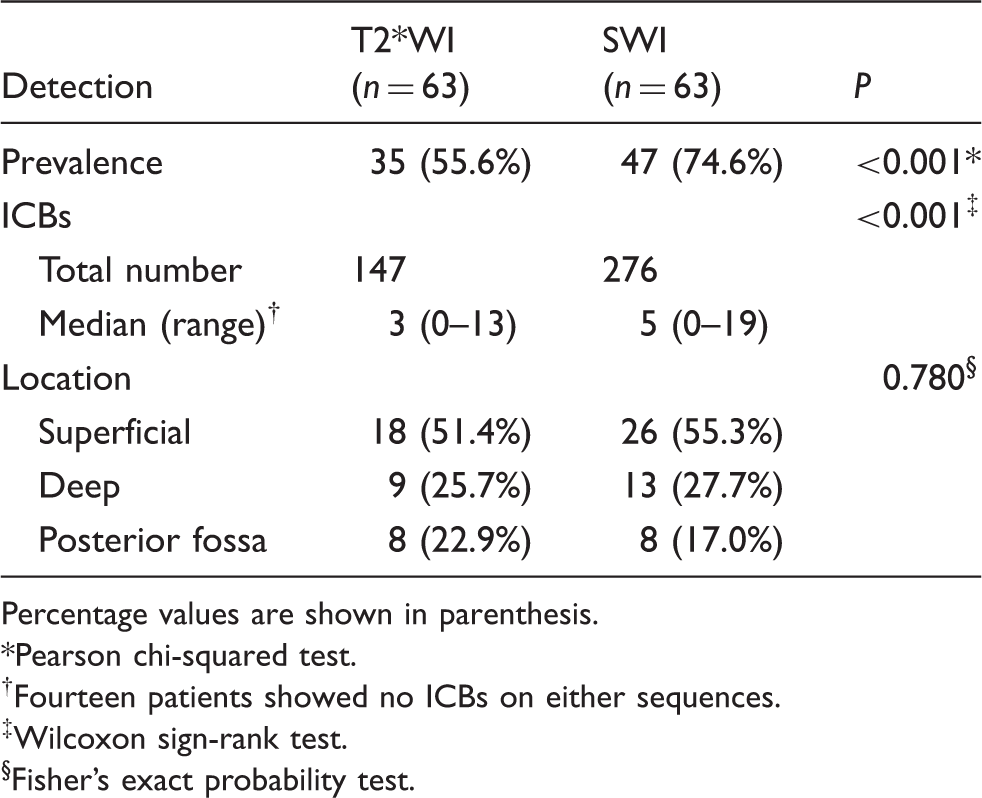
More patients were found to have ICBs on SWI than T2*WI (74.6% vs. 55.6%, Table 3). No ICB visualized on T2*WI was not visualized on SWI images. Among patients for whom ICBs were visible on both sequences (n = 35), significantly more ICBs were visualized on SWI images than on T2*WI images (median, 5 vs. 3; P < 0.001). However, no significant differences in lesions' disposition were found between these two sequences.
Correlations between ICBs and clinical characteristics
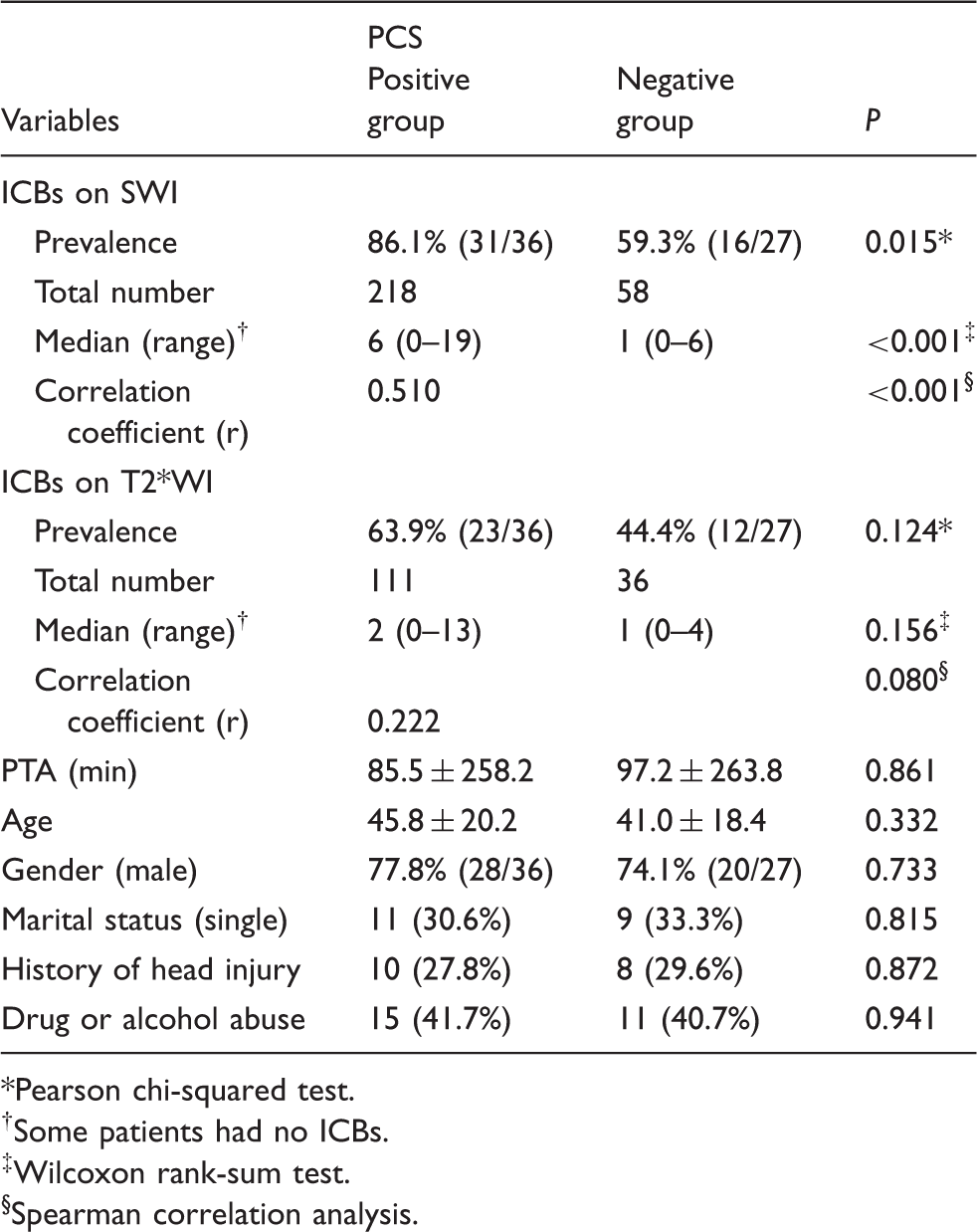
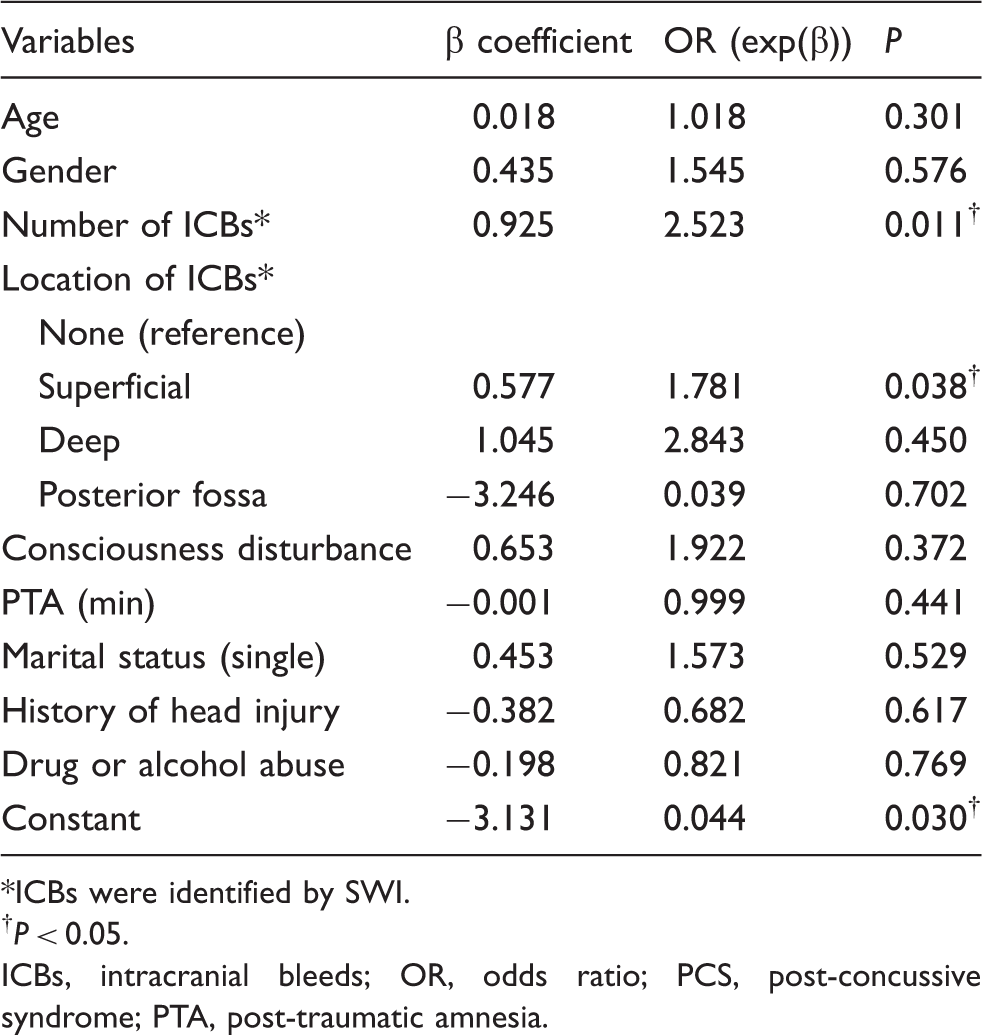
On SWI, the CD(+) group had a significantly higher rate of ICBs than the CD(−) group (84.6% vs. 58.3%, P = 0.020), but not on T2*WI (Table 2). Further, the prevalence and number of ICBs in the PCS(+) group were significantly higher than those in the PCS(−) group on SWI, but no significant differences were found on T2*WI (Table 4). With PCS as the state variable, ROC analysis showed that SWI was superior to T2*WI in PCS prediction (Fig. 3), with a cut-off point for ICB number of 2 on SWI having the largest Youden index. The corresponding sensitivity and specificity were 53% and 93%, respectively. Significant correlation was found between PCS and the ICB number on SWI (r = 0.510, P < 0.001), although no correlation was found between time of PTA, age, gender, marital status, history of head injury, and drug or alcohol abuse with PCS (Table 4). Multiple logistic regression showed that the number and superficial location of ICBs on SWI were independent variables predicting the occurrence of PCS (Table 5). An increase in the ICB number by 1 predicted an approximately 1.5-fold increase in PCS incidence, while compared to ICB-negative patients, those with ICB in a superficial location had an approximately 1.8-fold higher risk of PCS.
ROC curve showing the superiority of SWI to T2*WI in predicting PCS. The area under curve for SWI (0.773, P < 0.001) significantly exceeded 0.5, indicating that it is a reliable method for predicting PCS, while T2*WI is not (0.630, P = 0.080). Relationship between PCS and other variables. Pearson chi-squared test. Some patients had no ICBs. Wilcoxon rank-sum test. Spearman correlation analysis. Results obtained with the application of logistic regression analysis (dependent variable: PCS). ICBs were identified by SWI. †P < 0.05. ICBs, intracranial bleeds; OR, odds ratio; PCS, post-concussive syndrome; PTA, post-traumatic amnesia.
Discussion
Although MTBI is the most common type of TBI, its definition is still unclear. The definition related to GCS is widely used clinically: MTBI is defined as brain trauma with GCS ≥13, irrespective of the presence of neurological symptoms (16). According to GCS, patient with MTBI should show no sequelae in the future, because of the mild nature of injury. However, many clinical neurosurgeons have found certain pathophysiological abnormalities in the brains of traumatic patients with GCS ≥13, which might progress to severe secondary brain injuries, if not treated timely and appropriately (17,18). Therefore, MTBI cannot be simply regarded as patient whose GCS ≥13.
Some authors thus have advocated that information from medical imaging should be considered when assessing MTBI and its severity (6,19,20). The cerebral injuries in MTBI patients commonly include concussion, diffuse axonal injury, and cerebral contusion or laceration (21). Signs of parenchymal hemorrhage are the main evidence for diagnosing these abnormalities. The applicability and high sensitivity of 2D T2*WI for identifying cerebral microbleeds have been shown in previous studies (22,23). However, in current study, more ICBs were detected in more persons on SWI than on 2D T2*WI. This higher sensitivity of SWI could be related to superiority over T2*WI in predicting outcomes (such as PCS) in MTBI patients. Our findings are consistent with those of previous comparative studies between SWI and T2*WI for hemorrhagic lesions (9,24). The reason for the better ICB visualization on SWI could be its improved sensitivity for smaller hemorrhagic lesions over T2*WI, related to SWI features such as the thinner slice thickness and 3D imaging mode, whereby resolution is improved. Additionally, the relatively shorter TR of SWI (28 ms) than that of T2*WI (620 ms) brings about more T1W effect in SWI, making white matter appears brighter, and consequently making dark ICBs more conspicuous (25). Further, a lower bandwidth to increase the signal-to-noise ratio, phase-weighted imaging processing to remove the influence of field heterogeneousness, and mIPs to improve contrast between hemorrhagic foci and the surrounding brain parenchyma also contribute to improved visualization with SWI than with T2*WI (9,24).
The condition of MTBI patients may deteriorate, either leaving them with some neurological dysfunctions or leading to psychological disorders, but clinical examination usually does not reveal any positive neurological signs. It is reported that about 38–80% patients with MTBI may develop into PCS (15). These patients show a set of varied physical, cognitive, and behavioral or emotional symptoms, like headache, sleep disturbances, vertigo, nausea, fatigue, sensitivity to light or noise, concentration problems, depression, and emotional lability, but show no neurological signs (14,15). In this study, 36 (57.1%) patients showed PCS at the 7-month follow-up or later, a finding similar to that of a previous study (15).
Persistence or exacerbation of symptoms and occurrence of PCS are correlated with the extent of cerebral parenchymal injuries in MTBI patients. It is reported that the sizes and numbers of ICBs are related to the occurrence of cognition problems or senile dementia in the future (26). Ashwal et al. also found that the long-term prognosis of patients with TBI is closely related to the sizes and positions of ICBs (27). Using single photon emission computed tomography, Bonne et al. found that MTBI patients who had PCS showed areas of lowered metabolism and regional blood supply, indicating possible occurrence of cerebral damage in these area (28). This finding indicates that PCS incidence may be related to the number and size of ICBs in patients with MTBI. We found that ICB was an independent predictor of PCS. Damage in the superficial zone is most closely correlated to outcome, possibly because this zone comprises the four major brain lobes, has most of the brain volume, and is directly correlated with higher cognitive function. We believe that by enabling ICB identification, SWI can allow objective evaluation of MTBI patients and thereby predict the occurrence of PCS in the future.
The CD(+) group showed a higher incidence of PCS than the CD(−) group (64.1% vs. 45.8%), but this difference was not significant. This may because the CD(+) group also had a higher prevalence of ICBs than the CD(−) group.
It is unlikely that our results are incidental, since other factors like age, gender, PTA time, marital status, history of head injury, and drug or alcohol abuse, which may affect the outcome of MTBI patients (29), were homogeneously distributed between the PCS(−) and PCS(+) groups. Thus, confounding effects of these factors are weak. From our experience, we believe that SWI should be recommended for all patients with head injury, as it can identify ICBs that are easily missed by CT, conventional MRI, and even T2*WI. Nonetheless, CT is still useful because it helps in diagnosing and differentiating ICBs close to the skull base. In the future, DTI may help to detect white matter injury that better correlates with axonal injury, functional MRI (e.g. BOLD) may help to identify gray matter injury, and both may help to determine whether these areas impact prognostic evaluation.
This study has some limitations. First, we did not identify the pathological correlations of ICBs. We presumed that all “hypo-intense black dots” were ICBs, and that all of them were caused by brain trauma. Certain lesions may have been due to other reasons like hypertension. Thus, we may have overestimated the severity of injury. Second, the reviewers could not be blinded to the sequence type, as differences between them were obvious. However, we attempted to minimize recall bias by ensuring a 1-week gap between when the two sets of images were read, and the reviewers were blinded to patient details. Third, we may have missed some ICBs near the skull base because of susceptibility artifacts caused by air and bone interfaces.
In conclusion, MTBI often does not present objective findings, and its diagnosis is based entirely on clinical symptoms. Cerebral parenchymal hemorrhage may impact long-term outcome of MTBI patients. SWI is superior to conventional 2D T2*WI in detecting hemorrhagic foci in MTBI patients and can offer valuable objective information, for example, for predicting occurrence of PCS.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.