
Abstract
Background
Muscle hardness indicates muscle condition, and its measurement before and after resistance exercise is essential for preventing resistance training-induced muscle injury.
Purpose
To investigate muscle hardness of the triceps brachii (TB) before and immediately after a resistance exercise session involving the elbow extensors.
Material and Methods
In 18 young men, muscle hardness of the long head of TB was measured at 50%, 60%, and 70% point along the length of the upper arm from the acromial process of the scapula to the lateral epicondyle of the humerus by using shear wave ultrasound elastography. At the same sites, muscle thickness of the long head of TB was also measured by ultrasonography. Resistance exercise was performed using a dumbbell with a mass adjusted to 80% of the one-repetition maximum.
Results
Although the exercise-induced increase in muscle hardness was significant at all the regions, muscle hardness was significantly higher at 70% of the upper arm length than at the other regions before and after resistance exercise. The exercise-induced increase in muscle thickness was also significant, but the relative changes in muscle hardness before and after resistance exercise were not correlated with the corresponding relative changes in muscle thickness at each region. These results indicate the small effect of exercise-induced muscle swelling on exercise-induced changes in muscle hardness.
Conclusion
We suggest that muscle damage and/or injury, particularly at the distal region of TB, should be carefully considered to safely perform resistance exercise.
Introduction
Long-term resistance training induces an increase in muscle strength and size, and consequently contributes to improving physical performance. In contrast, resistance exercise based on the principle of progressive overload (1) induces a great load on the muscle, and can cause muscle damage and/or injury (2). Muscle hardness can be used to objectively indicate the muscle condition (3,4), as muscle hardness increases under various conditions, including those involving muscle damage, cramps, and spasms (4–6). In addition, it is important to decrease muscle hardness in order to improve and/or maintain muscle condition (7,8). Therefore, the measurement of muscle hardness before and after resistance exercise is essential for preventing resistance training-induced muscle injury.
Damage to muscle fibers causes spontaneous shortening of these fibers (9), thus increasing muscle hardness (6). Furthermore, the exercise-induced increase in intramuscular pressure caused by fluid accumulation can also contribute to muscle hardness (4,6). For preventing muscle injury induced by resistance training, an increase in muscle hardness resulting from damage to muscle fibers is considered more important. Muscle hardness has recently been quantified using shear wave ultrasound elastography (7,8,10–12). Muscle thickness, which is closely related to the cross-sectional area (13–15) and volume (16) of limb muscles and thus is an index of muscle size, is also usually determined using ultrasonography. Considering that exercise-induced fluid shifts contribute to increased muscle size (17), exercise-induced changes in muscle hardness and thickness should be measured simultaneously using an ultrasound apparatus in order to more precisely understand the manner in which muscle injury due to resistance training can be prevented. The muscle shape is not uniform in the direction of the muscle’s long axis. Moreover, the extent of training-induced increase in muscle size (i.e. muscle hypertrophy) varies according to the region of the muscle (18–21). Thus, we hypothesized that muscle hardness increases with resistance exercise, regardless of the region where it is measured, and that the hardness differs at different regions along the muscle’s long axis before and after resistance exercise. Therefore, in this study, we determined the muscle hardness and thickness before and after resistance exercise at three specific regions along the long axis of the triceps brachii muscle (TB) using an ultrasonic apparatus and aimed to test these hypotheses.
Material and Methods
Resistance exercise
In this study, we selected the TB for examination because of its high responsiveness to resistance training in terms of increase in muscle size (19,22). The “lying triceps extension” exercise with a dumbbell was used as the resistance exercise in this experiment (Fig. 1) (21). Subjects lay supine with the shoulder flexed at 90°, and the examiner stabilized the upper arm by supporting the elbow. Each subject was then instructed to extend the elbow concentrically (for 2 s), and then eccentrically (for 2 s). One session of the resistance exercise consisted of five sets of eight repetitions, with a 90-s interval between sets. The mass of the dumbbell was adjusted to 80% of one-repetition maximum of concentric resistance exercise (1RM). These program variables (duration of contraction, load, and number of sets and repetitions) were in accordance with those reported in previous studies (19,21).
Schematic illustrations of the “lying triceps extension” exercise. Subjects extend the elbow concentrically for 2 s, and then eccentrically for 2 s.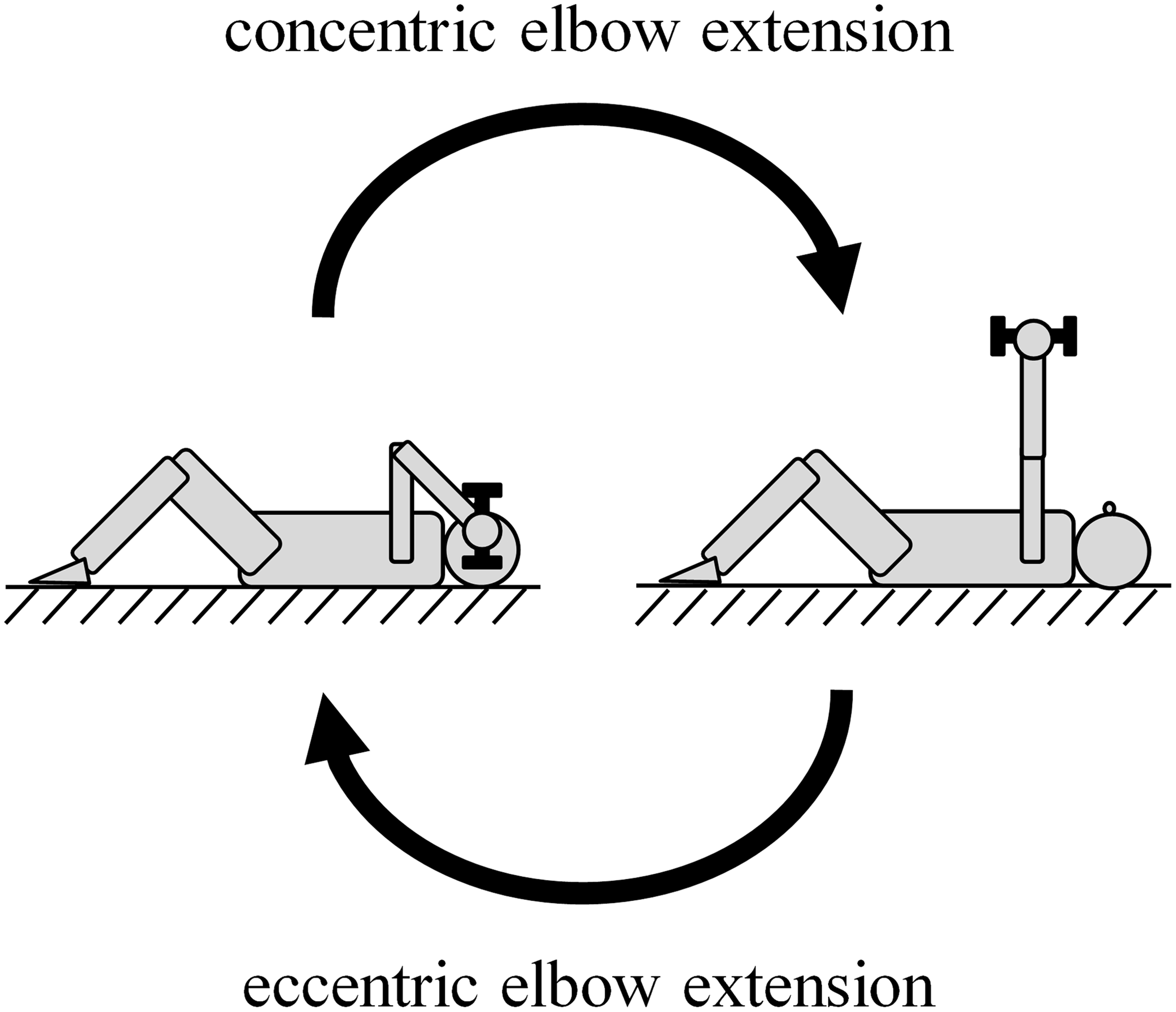
Subjects
Eighteen men (age, 22.4 ± 2.6 years; body height, 170.2 ± 5.4 cm; body weight, 59.6 ± 10.6 kg) participated in this study. The subjects were sedentary or physically active, but were not engaged in systematic resistance training of the upper extremity for at least 6 months before the experiment. The non-dominant arm in each subject was used to perform the resistance exercise. No subjects had abnormalities in the arms. The study protocol was approved by the Ethics Committee of the Japan Institute of Sports Sciences (permit number 2013-002). Each subject was informed in advance of the purpose and procedures of the study and possible risks posed by the measurements. Written informed consent was obtained from all subjects.
Experimental protocol
On the first day, body height and weight were determined, and the 1RM was measured to the nearest 0.5 kg value. Each subject was instructed to perform a specific warm-up of 3–5 repetitions at 3.5 kg and 1–2 repetitions at 5.0 kg. After performing the warm-up exercises, 1RM measurements were initiated. An attempt was considered successful when the movement was completed through a full range of motion, without deviating from proper technique and form. The initial load was selected by each subject, and the load was increased until the subjects could not lift the weight through the full range of motion. In order to avoid the effect of fatigue on the final result, the rest period between each attempt was longer than 90 s and 1RM measurements had to be completed within 3–5 attempts after the warm-up.
Upper arm length from the acromial process of the scapula to the lateral epicondyle of the humerus and muscle hardness and thickness of the long head of TB were determined 3–6 days after the above measurements. Prior to the measurements, we confirmed that none of the subjects experienced any pain or fatigue in their TB. First, upper arm length was measured to the nearest 0.5 cm with a steel tape, and muscle thickness was determined by ultrasonography at proximal 50%, 60%, and 70% point along the upper arm length (MT50, MT60, and MT70). During the measurements, subjects stood with their arms relaxed at their sides. Thereafter, subjects lay prone on a desk with their arms at their sides and the wrist pronated, and muscle hardness was determined using shear wave ultrasound elastography at the same regions (MH50, MH60, and MH70). After performing the resistance exercise, the muscle thickness and hardness were measured again and the measurements were recorded within 15 min. The temperature of the experimental room was kept constant at approximately 25℃ throughout the measurements.
Muscle thickness
The muscle thickness was measured using a B-mode ultrasonic apparatus (Aixplorer, SuperSonic Imagine, Bouches-du-Rhône, France). At each region, an electronic linear array probe (SuperLinear 15-4, SuperSonic Imagine) was transversely placed on the muscle as the largest muscle thickness in the mediolateral direction was observed near the transverse center of the image. Each position where the probe was located was marked with a pen to measure muscle thickness at the same sites before and after the resistance exercise. During this process, the examiner avoided compressing the muscle. Water-soluble transmission gel was applied to the contact surface. After obtaining the transverse ultrasound images, the muscle thickness – defined as the distance from the adipose tissue-muscle interface to the long head-lateral head of TB interface – was measured to the nearest 0.01 cm using an ultrasonic apparatus. The measurement was performed twice at each region and mean values of the two measurements were used for further analyses. The coefficients of variation (CVs) and intraclass correlation coefficients type 1,2 (ICCs(1,2)) were 2.6% ± 2.1% and 0.964 for MT50, 3.0% ± 2.9% and 0.974 for MT60, and 3.3% ± 2.4% and 0.987 for MT70, respectively.
Muscle hardness
The muscle hardness was measured using shear wave ultrasound elastography images obtained by using the ultrasonic apparatus (Aixplorer, SuperSonic Imagine). The electronic linear array probe (SuperLinear 15-4, SuperSonic Imagine) was transversely placed on the same position where the muscle thickness was determined, and water-soluble transmission gel was applied. The examiner avoided compressing the muscle, while placing the probe at the aforementioned marks.
Shear wave ultrasound elastography generated color-coded images with a scale from blue (soft) to red (hard), depending on the magnitude of shear wave speed (Fig. 2). Of the images stored in the ultrasonic apparatus at 11 Hz, we selected a single image on which a stable color distribution was observed during a certain time to determine the muscle hardness. In the image, a 10-mm-square region of interest (ROI) was set near the center part where the muscle thickness was measured. In addition, a 5-mm-diameter circle was set near the center of the ROI. Thus, the shear wave speed within the circle was automatically calculated to the nearest 0.1 m/s. The shear wave speed was measured five times at each site (SWS50, SWS60, and SWS70), in random order. Of the five measured values, we used group of three measurements that showed the lowest CV among 10 possible groups, and their mean value was used for further analyses. The CVs for the three adopted values were 2.9% ± 2.0% for SWS50, 2.6% ± 2.0% for SWS60, and 2.3% ± 1.8% for SWS70 with ICCs(1,3) of 0.974 for SWS50, 0.980 for SWS60, and 0.986 for SWS70.
Typical images of shear wave ultrasound elastography for the long head of the triceps brachii: (a) before resistance exercise, (b) after resistance exercise.
In this study, shear modulus was calculated as the product of muscle density and shear wave speed squared, and was considered to represent the muscle hardness (11). The muscle density was assumed to be 1084 kg/m3, which was the mean of the two values reported in a previous study (23).
Day-to-day reproducibility of the measurements
To ensure day-to-day reproducibility of the measurements, the same procedures before the resistance exercise were performed on a different day for two subjects. The CVs of the two measured values were 2.6% and 4.7% for MT50, 2.9% and 1.1% for MT60, 0.9% and 8.9% for MT70, 3.0% and 1.0% for SWS50, 4.2% and 9.2% for SWS60, and 2.8% and 5.5% for SWS70, respectively.
Statistical analysis
To examine the effects of resistance exercise on the muscle hardness and thickness, two-way analysis of variance (ANOVA) (test time [before and after resistance exercise] × region [proximal 50%, 60%, and 70% point along the upper arm length]) with repeated measures followed by the Bonferroni multiple comparison test was used. When a significant interaction between test time and region was found, a simple main effect test using the Bonferroni multiple comparison method was performed. Relative changes in muscle thickness and hardness before and after the resistance exercise were calculated, and Pearson’s product-moment correlation coefficients were calculated at each region.
Descriptive data are presented as mean (SD). Statistical significance was set at P < 0.05. When the results of the two-way ANOVA are presented,
Results
The 1RM value and upper arm length were 8.5 ± 1.2 kg and 30.9 ± 1.4 cm, respectively.
For muscle hardness, there were significant main effects of test time (P < 0.001, Muscle hardness of the long head of the triceps brachii before (○) and after resistance exercise (▴) (n = 18). MH50, MH60, and MH70 are muscle hardness values at proximal 50%, 60%, and 70% point along the upper arm length, respectively. There were significant main effects of test time (†††: P < 0.001) and region without a significant interaction between them. *(P < 0.05). ***(P < 0.001): a significant difference compared to MH70, detected by the Bonferroni multiple comparison test.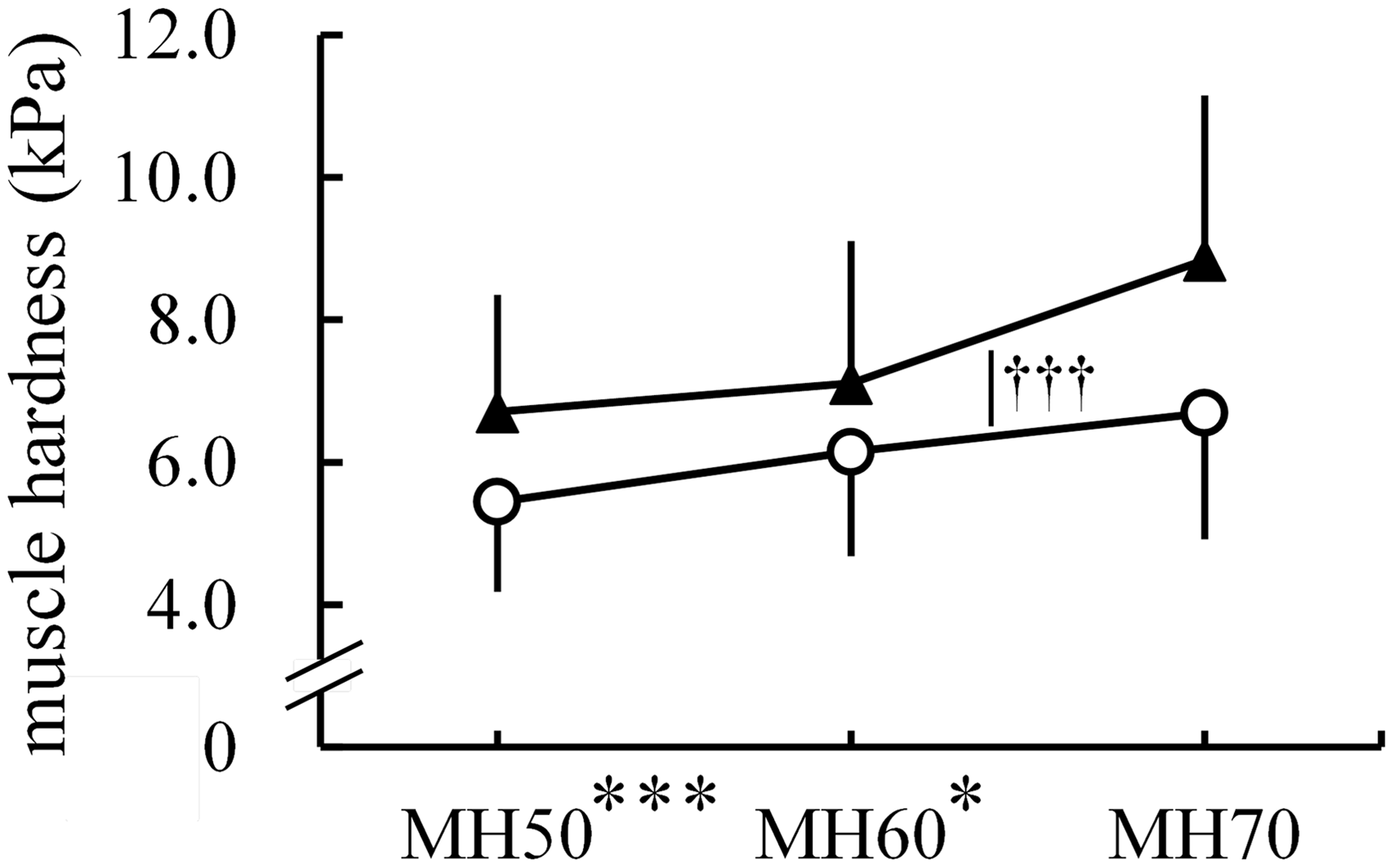
Fig. 4 illustrates the muscle thickness data. There was a significant interaction between test time and region (P = 0.039, Muscle thickness of the long head of the triceps brachii before (○) and after resistance exercise (▴) (n = 18). MT50, MT60, and MT70 are muscle thickness values at proximal 50%, 60%, and 70% point along the upper arm length, respectively. There was a significant interaction between test time and region. †††(P < 0.001): a significant difference between before and after resistance exercise, detected by the Bonferroni multiple comparison test. **(P < 0.01). ***(P < 0.001): a significant difference between muscle thickness at each region, detected by the Bonferroni multiple comparison test.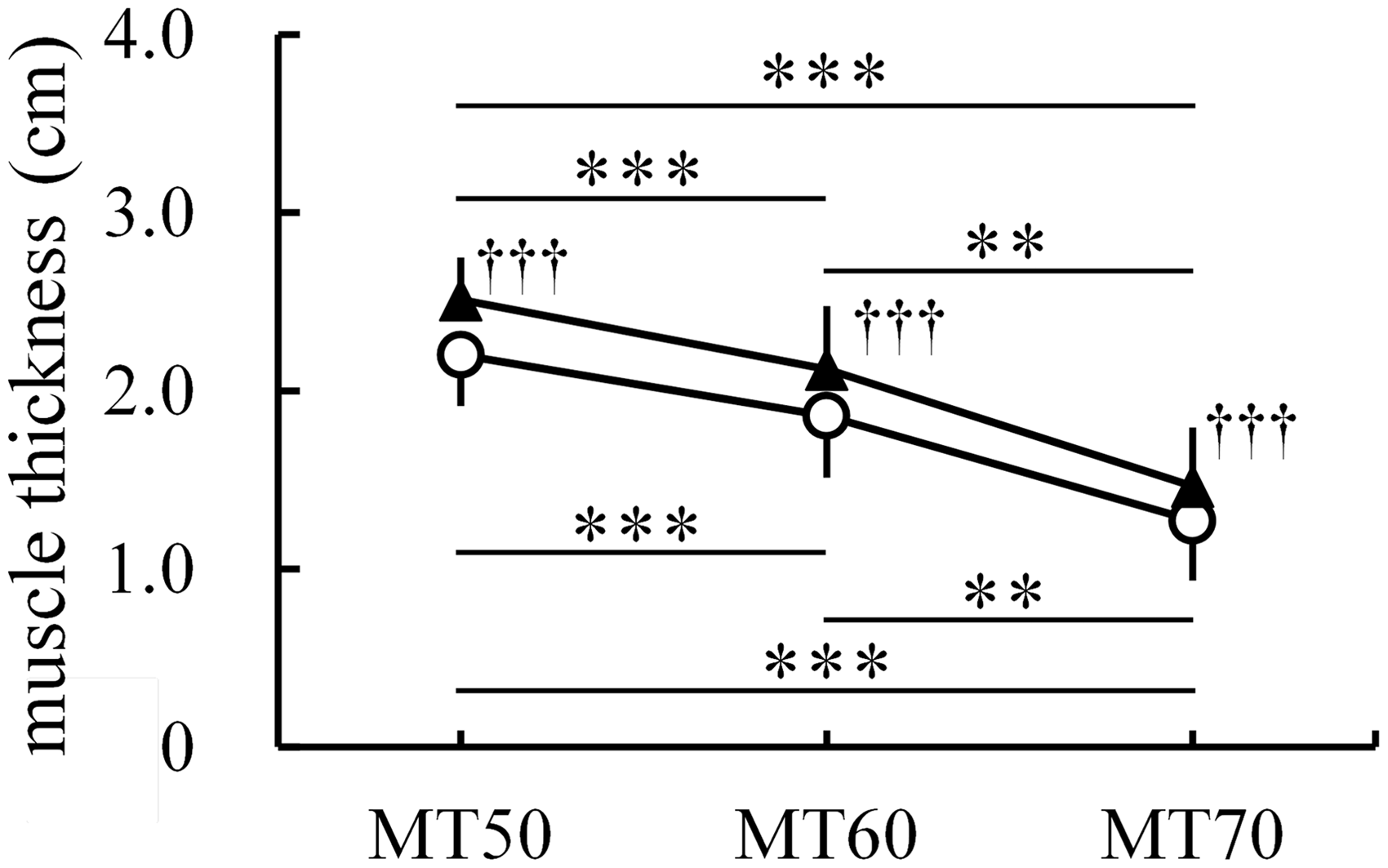
At each region, the relative change in muscle hardness was not significantly correlated with that in muscle thickness (50%: r = 0.329, P = 0.183; 60%: r = –0.423, P = 0.080; 70%: r = –0.081, P = 0.749).
Discussion
In this study, muscle hardness significantly increased with resistance exercise (Fig. 3). These results are in accordance with the findings of previous studies (4,6). Furthermore, MH70 was significantly higher than MH50 and MH60 both before and after resistance exercise (Fig. 3), which indicates the presence of a regional difference in muscle hardness along the muscle’s long axis. Thus, the current results support our hypotheses that muscle hardness increases with resistance exercise, regardless of the region where it is measured, and that the hardness differs at different regions along the muscle’s long axis before and after resistance exercise.
According to a previous study (6), it is likely that muscle hardness increases with resistance exercise not only due to the spontaneous shortening of muscle fibers resulting from damage but also due to the increased intramuscular pressure caused by fluid accumulation. In the present study, the original difference in muscle thickness among the regions was still noted after the resistance exercise (Fig. 4). Wakahara et al. (21) reported that the ratio of activated cross-sectional area to all cross-sectional areas in the long head of TB did not vary among the corresponding regions. Given that increased muscle size after resistance exercise primarily reflects the fluid movement from the vascular space into active but not inactive muscle (17), it is not surprising that the regional difference in muscle thickness before and after the resistance exercise did not change. Similar to muscle thickness (Fig. 4), muscle hardness also significantly increased with resistance exercise (Fig. 3); however, no significant correlations were observed between the relative changes in the muscle thickness and hardness at each region. These results suggest that the exercise-induced muscle swelling resulting from fluid shifts has a small effect on the increases in muscle hardness due to the resistance exercise. Thus, the corresponding increases in muscle hardness appear to be influenced to a great extent by the exercise-induced spontaneous shortening of muscle fibers caused by damage. Hence, attention to muscle damage and/or injury is needed to perform resistance exercise in a safe manner, particularly at the distal region of TB. It has been reported that exercise-induced muscle damage continues for some days (6,24) and a repeated bout of the same eccentric exercise within several weeks results in significantly less damage (25–27). Therefore, changes in muscle hardness for some days following one session of the resistance exercise and/or for several weeks during the resistance training program should be investigated in the future to collect more information regarding prevention of resistance training-induced muscle injury.
This study has certain limitations. First, we did not assess the medial and lateral heads of TB. There is no guarantee that the findings observed in the long head of TB correspond to those in the other heads. In a previous study (21), researchers found that during a session of resistance exercise, similar to that applied in this study, the ratio of activated cross-sectional area to all cross-sectional areas in the long head of TB corresponds to that in the medial head and is much greater than that in the lateral head of TB. Therefore, we had considered that the assessment of the long head of TB alone was sufficient to test our hypotheses. Second, the muscle hardness was measured transversely, but not longitudinally. In this study, muscle hardness and thickness were continuously determined. Given that muscle thickness is often measured using a transverse ultrasound image, both muscle hardness and thickness were determined transversely. However, previous studies (28–30) reported that the muscle hardness values measured transversely differed from those measured longitudinally. Furthermore, the contraction-induced increase in muscle hardness determined longitudinally was found to be greater than that determined transversely (29); these differences were believed to result from the anisotropy of the muscle. These observations imply that the assessment of the effect of resistance exercise on muscle hardness can change based on whether the muscle hardness is measured transversely or longitudinally. However, these researchers (29,30) could not conclude whether transverse or longitudinal measurement was more appropriate to evaluate muscle hardness. We consider that if the muscle hardness was measured in a similar manner both before and after resistance exercise, the exercise-induced change in muscle hardness can be appropriately evaluated regardless of the longitudinal and transverse directions of the ultrasound probe. Hence, despite the presence of muscle anisotropy and its individual differences, we believe that the current results are only minimally affected by the direction of muscle hardness measurement.
In conclusion, one session of the “lying triceps extension” exercise significantly increased hardness and thickness of the long head of TB at proximal 50%, 60%, and 70% point along the upper arm length. However, the exercise-induced increases in muscle hardness did not correspond to those in muscle thickness. Therefore, muscle swelling due to resistance exercise appears to have a small effect on the exercise-induced increases in muscle hardness.
Footnotes
Conflict of interest
None declared.
Funding
This study was partly supported by MEXT/JSPS KAKENHI Grant Number 24700689 (Grant-in-Aid for Young Scientists (B)) and the Nakatomi Foundation.