
Abstract
Background
The additive value of dual-energy spectral computerized tomography (DESCT) in breast cancer imaging is still unknown.
Purpose
To investigate the role of DESCT in improving the conspicuity of primary breast cancer.
Material and Methods
Twenty-nine patients who were histopathologically diagnosed with breast cancer and underwent DESCT for staging of lung metastasis were evaluated retrospectively. The visual conspicuity of breast cancer was scored by two readers separately in reconstructed virtual monochromatic images obtained at 40, 60, 80, and 100 keV. A circular region of interest slightly smaller than the maximum contrasted portion of the primary breast cancer was manually placed. Iodine enhancement (HU) and iodine content (mg/mL) values of tumor, normal breast tissue and pectoral muscle, and contrast-to-noise values of images at four different energy levels were calculated.
Results
The lesion conspicuity score peaked at 40-keV series for both readers and was significantly higher than those at other energy levels (all P < 0.001). Lesion iodine enhancement was highest at 40-keV virtual monochromatic image reconstructions (P < 0.001). The iodine content was significantly higher in tumor than normal breast tissue, and pectoral muscle (P < 0.001). The highest contrast-to-noise value was obtained at 60 keV (4.0 ± 2.5), followed by 40 keV (3.9 ± 2.2), without a significant difference (P = 0.33).
Conclusion
The conspicuity of primary breast cancer was significantly higher in low keV virtual monochromatic images obtained by DESCT. This gives us hope that DESCT may play an effective role in detecting incidental breast lesions. It also raises the question of whether quantitative values obtained by DESCT can be used for characterization of primary breast lesion.
Keywords
Introduction
Breast cancer is the second leading cause of cancer related deaths in women, after lung cancer (1–3). The lungs are the most common site of breast cancer metastasis, similar to many types of cancer. Screening of patients for such lung metastases in diseases with a high potential of metastasis, namely colon cancer, breast cancer, malignant melanoma, and renal tumor, is performed with contrast-enhanced thorax computed tomography (CT) scans (4). Currently, thorax CT investigations are preferred as the primary imaging modality for the screening of breast cancer metastases; however, CT is unable to characterize the primary tumor of the breast in detail (5,6).
On the contrary, several studies suggested that routine contrast-enhanced thorax CT scans performed for indications other than breast diseases may have high diagnostic efficacy in detecting breast masses. Assessment of morphological and contrasting features of the mass, in particular, was found to be useful for discrimination between malignant and benign breast lesions (7–9).
By means of technical development, dual-energy spectral CT (DESCT) has started being used frequently in recent years for the diagnosis and follow-up of oncologic diseases. The causes of its preference are mainly lower contrast agent usage and radiation exposure than routine contrast-enhanced single energy thorax CT obtained with multidetector CT (10,11). Various studies revealed that the conspicuity of vascular pathologies and soft tissue tumors is increased in DESCT (12,13). In addition, some quantitative analyses (iodine enhancement [IE] and iodine content [IC]) and material decomposition images can be derived thanks to this method (14,15). Thereby DESCT aids discrimination considerably between benign and malignant lesions and staging of cancer in oncology patients (16,17).
In the literature, there is no study that evaluated the conspicuity of breast lesions in thorax DESCT. Our main objectives in this study are: (i) to discover whether the optimal virtual monochromatic image series provides better visualization of primary breast cancer in patients who underwent the thorax DESCT scan for staging purposes; and (ii) to discover whether the quantitative values obtained by DESCT can be used in the characterization of the primary lesion.
Material and Methods
Patients
The ethics committee of our hospital approved this retrospective study and written informed consent was obtained in all patients before imaging. A total of 29 consecutive patients with 39 histopathologically proven primary breast tumors, who underwent contrast-enhanced thorax CT scans with DESCT mode from April 2015 to Februrary 2016, were included in our study. Contraindications for imaging were known reactions to iodinated contrast material (a previous history of anaphylactic reaction), impaired renal function (glomerular filtration rate <45 mL/min), and pregnancy.
CT examinations and radiation dose
All CT examinations were performed with a high definition CT scanner (Discovery CT750HD, GE Healthcare, Milwaukee, WI, USA). Patients were injected with 80–100 mL (1.35 mL/kg of body weight) non-ionic iodinated contrast material (Iopromide, Ultravist, 300 mg I/mL, Bayer Schering Pharma, Berlin, Germany) via antecubital vein at a rate of 3–4 mL/s; enhanced scans were obtained with DESCT mode about 50 s after the injection of contrast agent. The scanning parameters for Gemstone Spectral Imaging (GSI) mode were as follows: tube voltage = dynamic switching 80–140 kVp within 0.5 ms; tube current = 275–640 mA (based on a pre-specified BMI protocol); detector collimation = 0.625 × 64 mm; rotation speed = 0.6–0.8 s; helical pitch = 1.375:1; field of view = 500; collimation = 40 mm; section thickness = 5 mm; and gap = 5 mm.
DESCT post-processing
The Gemstone Spectral Imaging Viewer software on an independent advanced workstation (Advantage Workstation 2.0; GE Healthcare) enables the automatic reconstructions of 101 sets of monochromatic images at photon energies in the range of 40–140 keV and the iodine-based material decomposition images for every patient. In this study, four image series with different energy levels of 40, 60, 80, and 100 keV were reconstructed. The spectral information of dual-energy data was used to generate iodine maps and virtual monochromatic images in axial slices with a thickness of 2.5 mm for objective and subjective image analysis.
Objective image analysis
All series were transformed to the clinical workstation, which can calculate the CT attenuation values of monochromatic images in the range of 40–140-keV energy levels. CT attenuation (IE) and ICs were measured in mean Hounsfield units (HU) and mg/mL, respectively, by placing a circular region of interest (ROI) in the primary breast tumor, ipsilateral pectoral muscle, and normal fibroglandular breast tissue. To ensure data consistency, all measurements were performed three times and average values were calculated avoiding obvious necrosis and image artifacts. The lesion contrast-to-noise ratio (CNR) was calculated using the following formula: CNR = (ROIbreast lesion – ROInormal fibroglandular breast tissue)/SD; where SD represents the standard deviation of CT numbers in the adjacent normal fibroglandular breast tissue.
Subjective image analysis
For subjective assessment, two radiologists (YM and NOM, with eight and five years of experience in thorax CT, respectively) interpreted the images independently. Readers were informed about the diagnosis and the location of biopsy-proven breast cancer in all patients but were blinded to the image reconstruction method. Window settings were automatically set in soft-tissue window (width = 400; level = 40 HU) to show the enhancement details of lesions, but readers were allowed to adjust these values freely to improve tumor visualization. Each reader graded the conspicuity of lesions individually on a 5-point confidence scale (5 = well seen, 4 = readily seen, 3 = seen, 2 = probably seen, and 1 = not seen) based on the contrast enhancement of lesions on the four different (40, 60, 80, and 100 keV) VMI sets. We also analyzed intercorrelation values.
Statistical analysis
Statistical analyses were performed using commercially available statistical software (IBM SPSS Statistics, version 22.0, IBM SPSS, Armonk, NY, USA). Continuous variables were described as mean ± standard deviation (range). P < 0.05 was considered statistically significant. The normality of data distribution was defined using the Kolmogorov–Smirnov test. The differences of all CNR and lesion IE (HU) measurements between the four monochromatic image series were assessed with the repeated-measures analysis of variance (ANOVA) test. The subjective lesion conspicuity was assessed by averaging the definite 5-point scores of both readers. The non-parametric Friedman test with Wilcoxon signed-rank test was used for comparison and assessment of statistical significance of subjective ratings between the various image series.
Results
Patient characteristics
The mean age of the 29 patients was 53 ± 12 years (age range = 30–83 years). Histopathologically, 30 lesions with invasive ductal carcinoma, two with lobular invasive carcinoma, two with ductal carcinoma in situ, two with mucinous carcinoma, two with invasive carcinoma, and one lesion with medullar carcinoma were diagnosed.
The mean CT dose index (CTDI) was 8.16 ± 1.42 mGy and the mean dose length product (DLP) was 442.26 ± 15.6 mGycm.
Quantitative image analysis
Primary breast cancer’s IE increased gradually as the photon energy decreased from 100 keV to 40 keV and the maximum mean value (171 ± 44 HU) was achieved at the 40-keV VMI sets, which was significantly higher than all other energy levels (P < 0.001) (Fig. 1).
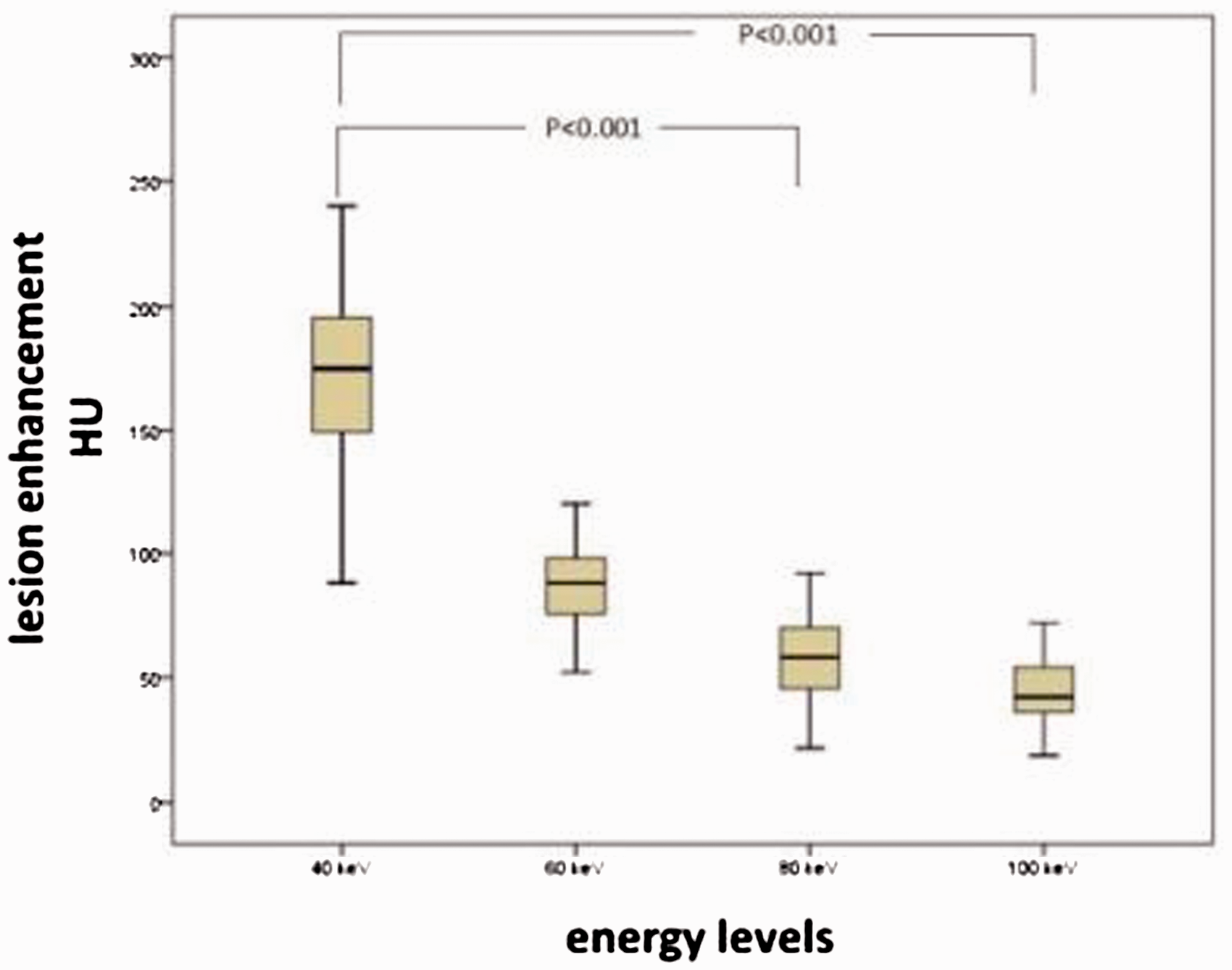
Box-and-whiskers plot of primary breast tumor enhancement in VMI reconstructions at 40, 60, 80, and 100 keV. Boxes represent the middle 50% of the cases, horizontal lines mark the median values; the whiskers represent minimal and maximal values. Tumor enhancement peaked in the 40-keV VMI series (all P < 0.001). Tumor enhancement in the 60-keV series was superior to the 80-keV and 100-keV series (all P < 0.001).
IEs of normal breast and muscle tissue in spectral HU curve analysis were not significant at different keV VMI datasets, which improved the visibility of primary breast tumors at decreasing energy level VMI images (Fig. 2).
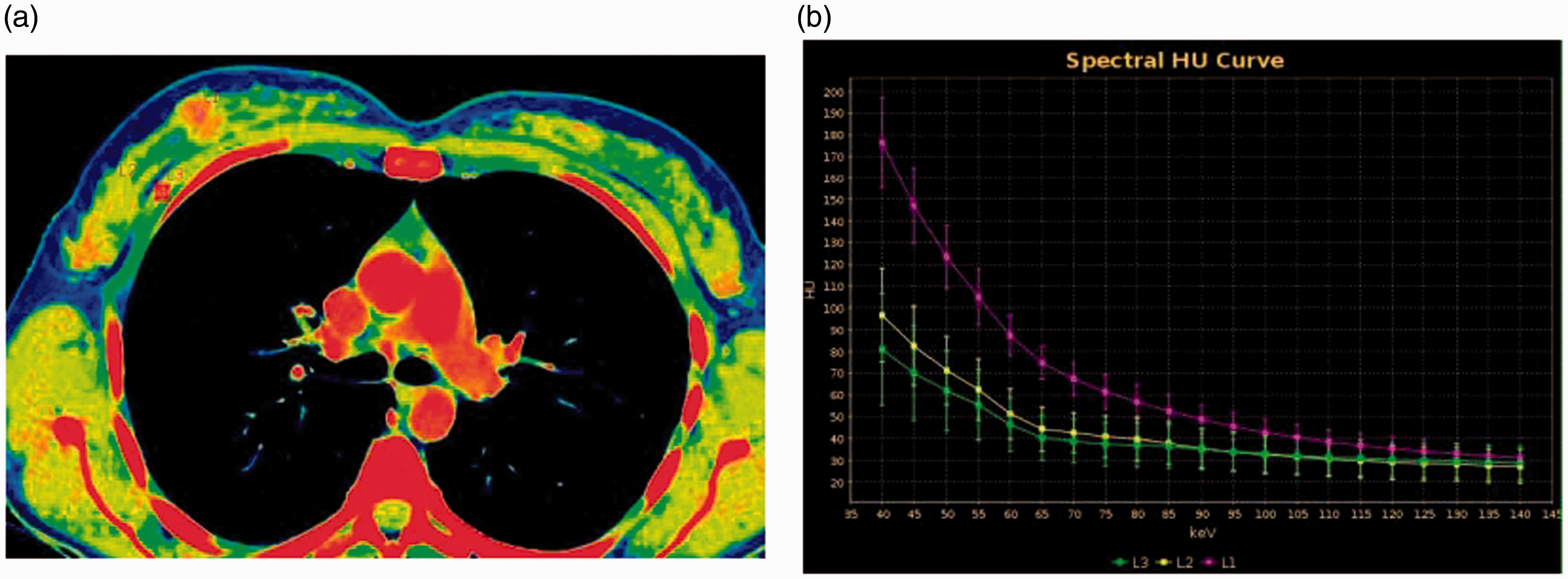
Spectral HU curve analysis demonstrating IE of primary tumor (L1), normal breast tissue (L2), and muscle tissue (L3) at different keV VMIs.
IC of primary breast cancer (17.85 ± 4.5 mg/mL) was significantly higher than the IC of muscle (5.1 ± 1.5 mg/mL) and normal fibroglandular breast tissue (2.9 ± 2 mg/mL) (P < 0.001) (Fig. 3).
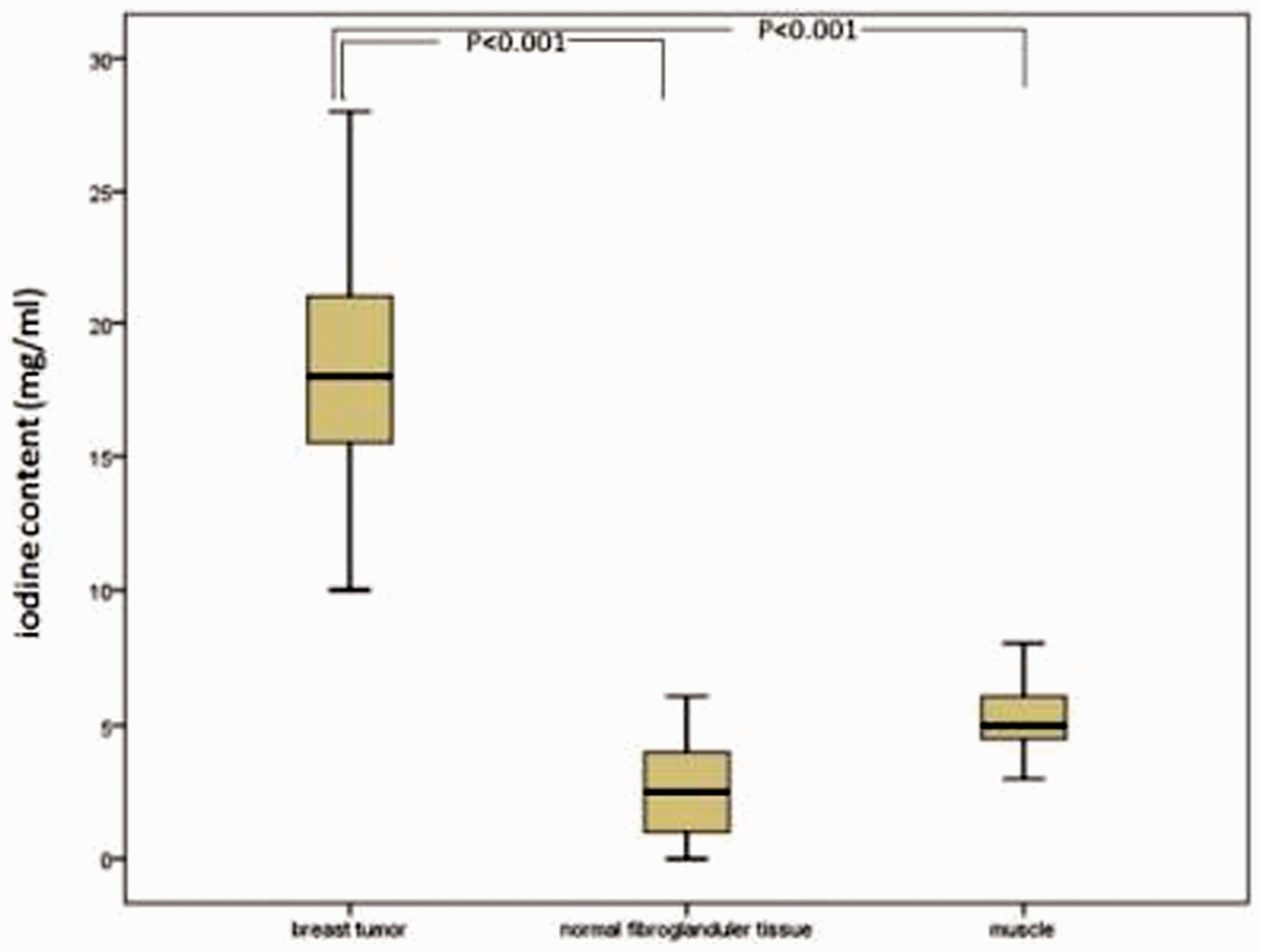
Box-and-whiskers plot of primary breast tumor IC (mg/mL) in the material decomposition images. Boxes represent the middle 50% of the cases, horizontal lines mark the median values; the whiskers represent minimal and maximal values. The tumor’s IC is significantly higher than normal fibroglandular breast tissue and muscle tissue.
The highest calculated lesion CNR values were obtained at 60 keV (4 ± 2.5) and at 40 keV (3.9 ± 2.2). There was no statistically significant difference between these values (P = 0.33). Lesion CNR in 80-keV VMI (2.9 ± 2) and 100-keV VMI (2.4 ± 1.9) were significantly lower than the lesion CNR values at 40-keV and 60-keV VMIs (P < 0.001) (Fig. 4).
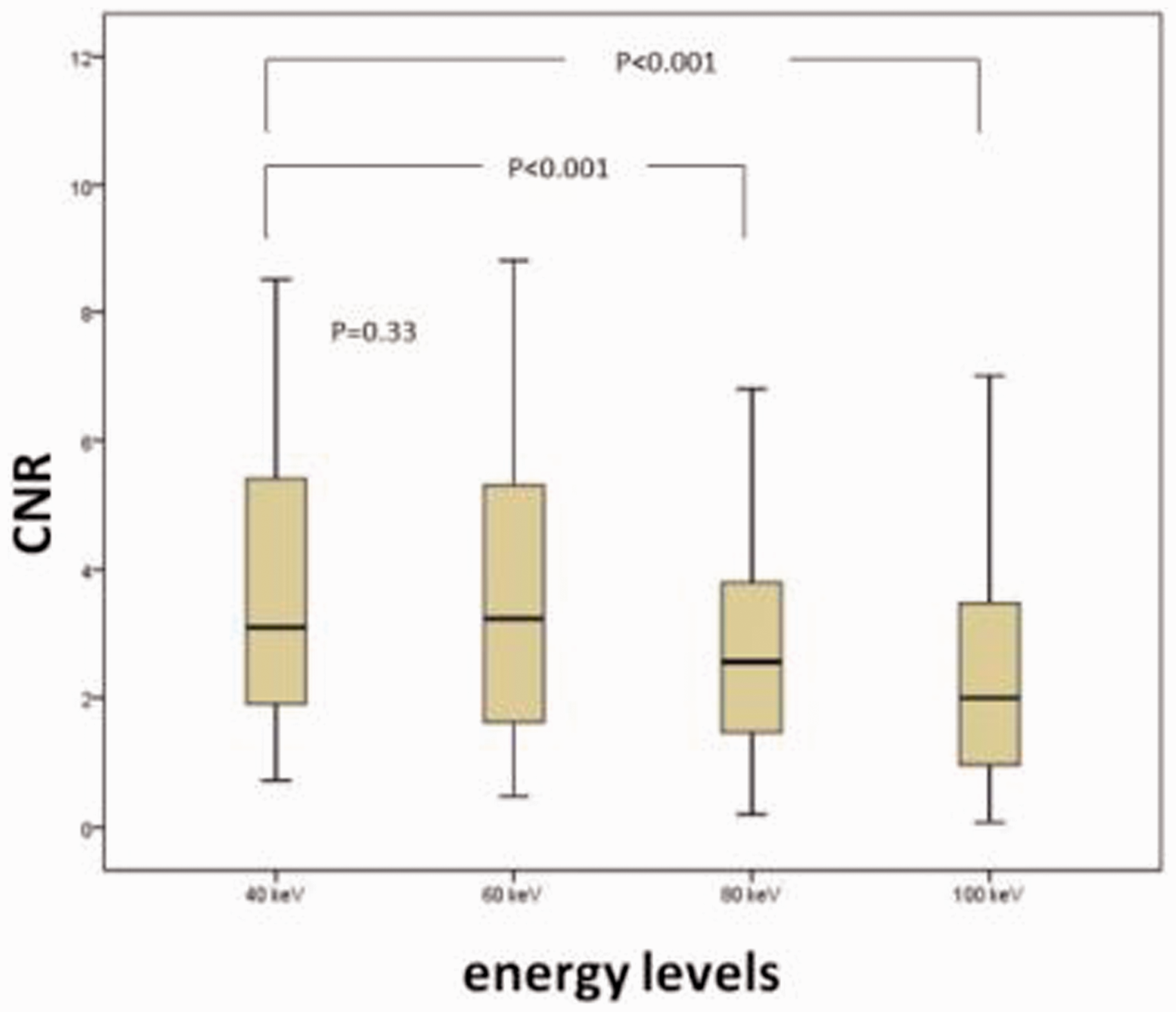
Box-and-whisker plots of CNR in the monochromatic images at 40, 60, 80, and 100 keV. Boxes represent the middle 50% of the cases, horizontal lines within mark the median values, and the whiskers represent minimal and maximal values. The CNR value peaked in the 40-keV and 60-keV series and was significantly higher than the 80-keV and 100-keV reconstructions series. There was no significant difference between the 40-keV and 60-keV series.
Lesion conspicuity score analysis (subjective image analysis)
The summary of lesion conspicuity scores of two readers is presented in Table 1. The subjective score of the tumor conspicuity was highest at the 40-keV VMIs and lowest at the 100-keV VMIs of both readers (4.85 ± 0.37 and 4.74 ± 0.44, 2.3 ± 0.7 and 2.1 ± 0.7, respectively), which was significantly higher than all other energy levels (P < 0.001) (Fig. 5). Both readers had good inter-observer correlation at 40 keV and 60 keV (kappa values 0.69, and 0.79, respectively). However, inter-observer correlation was moderate at 80-keV and 100-keV VMIs (kappa values 0.49 and 0.60, respectively).
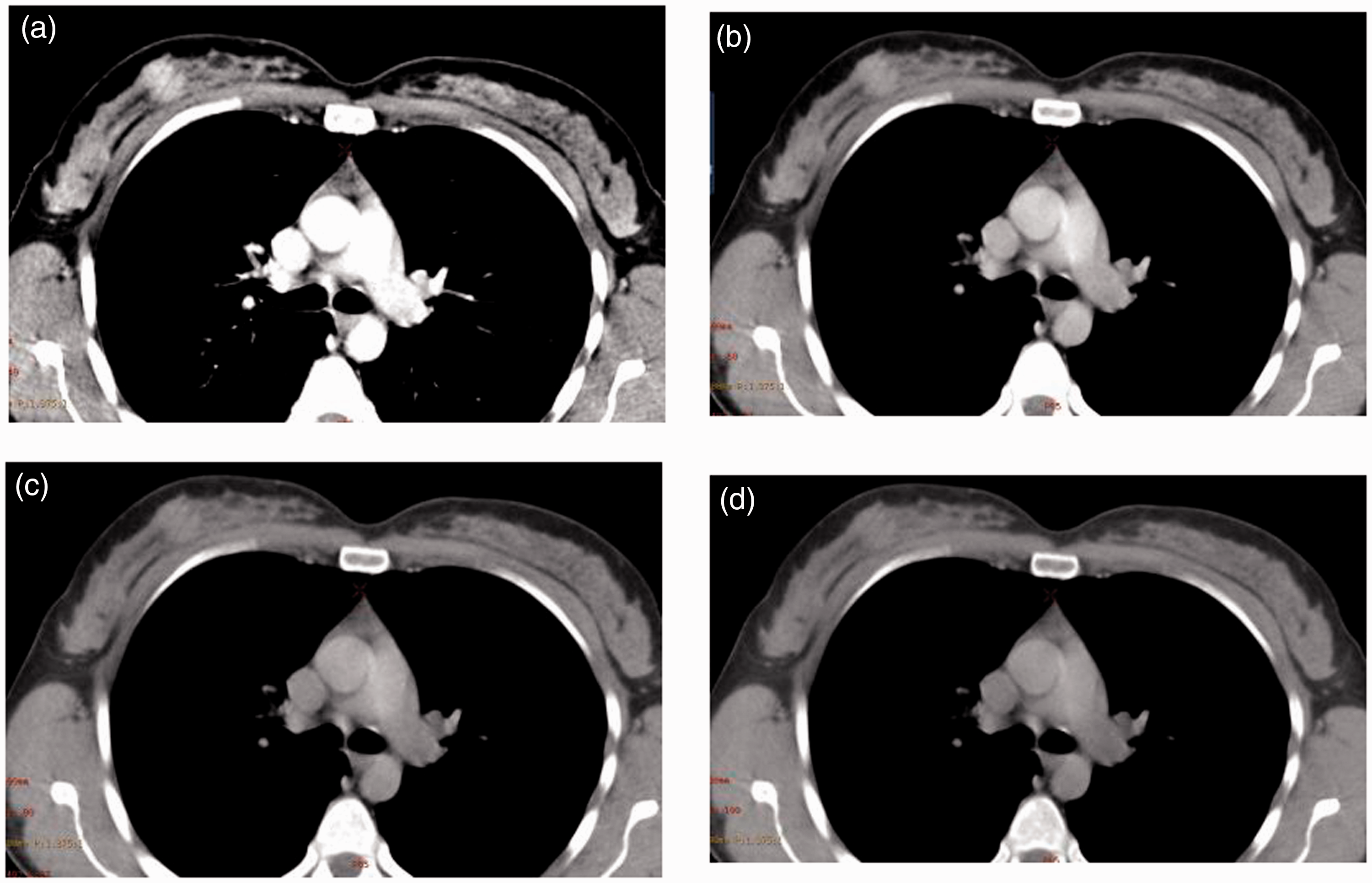
Axial CT images of a 45-year-old female patient with pathologically proved right invasive ductal carcinoma. VMI reconstructions at 40 keV (a) show the highest lesion attenuation. VMI reconstructions at 60 keV (b) demonstrate second highest lesion attenuation. The 80-keV (c) and 100-keV (d) VMI reconstructions demonstrate decreased lesion attenuation. The highest lesion conspicuity scores were obtained at 40 keV (all P < 0.001) (same patient as Fig. 2).
Subjective image analysis of breast tumor conspicuity at different energy levels and inter-observer correlation analysis .

Discussion
In this study, we evaluated the virtual monochromatic images of different energy levels using DESCT both objectively and subjectively to discover the optimal energy levels for increased image quality and the conspicuity of pathologically proven breast cancer. We discovered higher IE and CNR values at 40-keV VMIs compared to other different energy levels. Thus, we revealed the highest lesion conspicuity score at 40 keV with good inter-observer correlation. Moreover, we observed increased IC in breast carcinomas compared with normal fibroglandular breast tissue and muscle tissue using iodine-mapping images. Our study is the first to demonstrate the superior ability of DESCT at low keV VMIs in discrimination of breast carcinomas.
DESCT is an imaging mode based on the rapid switching between 80-kVp and 140-kVp datasets from view to view during a single rotation to produce both the monochromatic spectral images at 101 energy levels in the range of 40–140 keV and the material decomposition images, which provides opportunity for selecting the optimal energy levels to improve image quality for lesion detection and also for analyzing some quantitative parameters such as IE and IC (18). The other application of DESCT in clinical practice is the capability of material differentiation named as material-decomposition images, which aids obtaining material-specific images with separation, for example of iodine, calcium, barium, and uric acid on an image obtained in a single examination. Elements included in lesions become detectable by means of that method; for instance, the structure of renal calculi or iodine content of a malignant lesion. The capability of obtaining different material-specific datasets (iodine map) in the same acquisition can improve lesion detection and characterization (19,20). We demonstrated that primary breast carcinomas had the highest IE at 40-keV VMI sets compared to other energy levels. Moreover, we discovered significantly increased iodine attenuation compared to normal breast and muscle tissue with decreasing energy levels at spectral HU curve analysis.
Iodine-mapping images can only be achieved using DESCT due to imaging at low keV VMIs. Additionally, DESCT promotes the dramatic improvement in visibility of high-contrasting lesions. The ability of DESCT to gain different keV images also helps in different obtaining images with varying CNR. Images with high CNR would markedly enhance lesions. It seems that CNR increases in parallel with decreasing keV images to some extent. However, in image sets < 60 keV, the noise increased more prominently than contrast, which decreased CNR. We documented that the highest CNR value was obtained at 60 keV, followed by 40 keV without significant difference. Therefore, both higher contrast and CNR of the images aid in conspicuity of the lesion in low keV images.
Kaup and Hou demonstrated significantly superior primary lesion iodine enhancement, CNR value, and subjective image quality score at low keV levels compared to higher keV using DESCT for primary lung carcinomas (21,22). Meng et al. found lower IC in normal gastric mucosa with respect to gastric carcinomas at iodine-mapping images by DESCT, which facilitated discrimination of pathologic lesions from normal tissue (23). Similarly, Uhriq et al. reported considerably higher recognition of metastases in patients with malign melanoma using iodine-mapping imaging; their explanation was due to higher IC in pathologic tissue. All of these studies exploited iodine-based material decomposition images to discriminate between pathologic lesions and normal anatomic structures. We revealed that primary breast tumors had higher IC compared with normal breast and muscle tissue, in parallel to the aforementioned studies. Therefore, it seems prudent to say that DESCT may help lesion discrimination in different locations due to the increased IC of pathologic lesions.
The primary radiologic imaging methods for evaluation of breast pathologies are mammography and ultrasonography. Breast magnetic resonance imaging (MRI) is increasingly utilized due to recent advances (24). Thorax CT examination has no primary role in evaluation of breast pathologies. However, the examination of breast lesions is quite possible with CT since breast tissue is included in thorax CT images. There are no data in the current medical literature regarding the use of DESCT in identification of breast carcinoma. However, Lin et al. mentioned that adding quantitative CT enhancement value to the qualitative assessment of incidental breast lesion morphology might increase the diagnostic accuracy for differentiating benign from malignant breast lesions. They showed that malignant breast lesions had higher attenuation on contrast-enhanced CT (7). In the present study, we found that breast cancers had higher IE (HU) and IC (mg/ml) compared to normal breast parenchyma.
In the literature, there is no study in which primary breast lesions were examined by qualitative and quantitative parameters obtained by thorax DESCT. Our results showed that use of contrast-enhanced DESCT may enhance identification of breast pathologies by low-energy VMIs and iodine-mapping imaging. If we speculate, this may lead to the hypothesis that DESCT images gained in order to evaluate lung pathologies may help to detect and characterize incidental breast lesions by VMIs and iodine mapping. In addition, quantitative parameters obtained by this method may allow the characterization of breast lesions correctly, thus reducing the need for additional examinations or unnecessary biopsy. Moreover, in patients who cannot undergo MRI due to various reasons, DESCT images may improve local staging of breast carcinomas by higher lesion conspicuity.
This study is the first to investigate the conspicuity, IE, and IC of primary breast cancer by DESCT. Nevertheless, our study has some limitations. First, we included the thorax DESCT scans obtained for staging of primary breast cancer patients diagnosed histopathologically. We did not evaluate benign breast lesions in our study. Therefore, our results might not be similar for discrimination of benign and malignant lesions using IC and IE.
Second, since this study is primarily based on chest CT scans, the appropriate scanning time after contrast media injection and the amount of contrast media to identify breast cancer could not be detected. Most of the studies about dynamic contrast-enhanced MRI suggested taking the first post-contrast images 2 min after the injection of contrast media (25,26). In addition, the scans were taken 2 min after the contrast media injection to increase the conspicuity of malignant lesions in contrast-enhanced spectral mammography studies (27). As is routine in thoracic CT examinations, 50 s after contrast agent injection, the scan started in our study. Therefore, the best enhancement of the images in the second minute could not be obtained . Studies on the conspicuity of primary breast lesion in dynamic studies in which late-term images were taken may be performed in the following years.
Lastly, radiation exposure may be another important limiting factor. CDTI volume in DESCT was not higher than a standard chest scan obtained with a 128-row detector CT. Regarding the radiation dose, our mean radiation dose in terms of DLP was 442.26 ± 15.6 mGycm. This value was similar to mean DLP in 128-row detector CT in our institution (DLP = 449.91 ± 23.4 mGycm).
In conclusion, although CT has no primary role in the detection of breast lesions, the examination of low keV VMIs in the thoracic CT scans obtained by DESCT may increase the evidence of breast carcinomas. This may lead to an increased detection rate of incidental breast lesions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.