
Abstract
Background
Administration of contrast medium (CM) is an important image quality factor in computed tomography (CT) of the chest. There is no clear evidence or guidelines on CM strategies for chest CT, thus a consensus approach is needed.
Purpose
To survey the potential impact on differences in chest CT protocols, with emphasis on strategies for the administration of CM.
Material and Methods
A total of 170 respondents were included in this survey, which used two different approaches: (i) an online survey was sent to the members of the European Society of Thoracic Imaging (ESTI); and (ii) an email requesting a copy of their CT protocol was sent to all hospitals in Norway, and university hospitals in Sweden and Denmark. The survey focused on factors affecting CM protocols and enhancement in chest CT.
Results
The overall response rate was 24% (n = 170): 76% of the respondents used a CM concentration of ≥350 mgI/mL; 52% of the respondents used a fixed CM volume strategy. Fixed strategies for injection rate and delay were also the most common approach, practiced by 73% and 57% of the respondents, respectively. The fixed delay was in the range of 20–90 s. Of the respondents, 56% used flexible tube potential strategies (kV).
Conclusion
The chest CT protocols and CM administration strategies employed by the respondents vary widely, affecting the image quality. The results of this study underline the need for further research and consensus guidelines related to chest CT.
Keywords
Introduction
Computed tomography (CT) of the chest plays an important role in the diagnosis and treatment of many thoracic disorders (1,2). The use of contrast-enhanced CT is indicated for the assessment, delineation, and differentiation of a wide range of clinical conditions including vascular, pleural, and pathologic diseases (3,4). Administration of CM must be carefully planned and precisely performed to ensure that CT scans are diagnostically accurate and also to minimize potential risks from excessive radiation and/or CM load (5–7).
Contrast-enhanced CT is affected by numerous interacting factors (6). Within chest CT, it has been common practice to use a fixed volume of iodinated CM independent of body weight (1). However, research has shown a clear relationship between vessel and tissue enhancement, and patient weight (8–11). The use of a fixed CM administration strategy is problematic when patients vary in size; small patients may receive too much CM and large patients may receive an insufficient volume. This will result in an inconsistent image quality due to variations in CM enhancement (12–14).
In addition to CM volume, injection rate and CT scanning factors also affect the magnitude of vascular and parenchymal enhancement (6,15,16). Moreover, performing CT examinations at low tube voltages increases the contrast of structures imaged using CM with a high effective atomic number, such as iodine. This facilitates a reduction in iodine load, and thus, a reduced risk of post-acute kidney injury among patients with impaired renal function (17,18). The iodine load will be reduced by reducing the CM volume and/or concentration (19).
Large inter-practice variation and lack of consensus in chest CT protocols is still observed in clinical practice and scientific articles (20,21). Few published studies have investigated routine chest CT protocols and CM administration strategies in detail. Previous studies (20,21) have focused on variations in non-enhanced CT or CT protocols including both chest and upper abdomen. Therefore, the aim of the present study was to survey the chest CT protocols currently in use, focusing on variations in administration strategies of CM and parameters affecting enhancement of CM.
Material and Methods
Factors affecting CM protocols and CM enhancement for chest CT were investigated by surveying professionals working with CT and thoracic radiology within their respective institution/hospital.
Study design and population
The study population included members of the European Society of Thoracic Imaging (ESTI), plus all the hospitals (local and university hospitals) in Norway, and university hospitals in Sweden and Denmark. Data were collected using two different approaches:
ESTI members were contacted through the Society itself in September 2019. An email message was sent to ESTI members inviting them to complete the questionnaire and providing a link to the online survey. Four weeks were allocated for completion of the survey. After three weeks, a follow-up email was delivered to non-respondents to promote survey participation. An email explaining the purpose of the study and requesting a copy of the chest CT protocol currently in use, including CM administration strategy, was sent to all hospitals in Norway and all university hospitals in Sweden and Denmark in January 2019. The requested protocol was returned by email providing the same information as the online questionnaire completed by the ESTI members. Data collection was completed at the end of December 2019 when all the hospitals had responded to our email. Emails requesting additional information elaborating the CM protocol were sent when needed.
Questionnaire
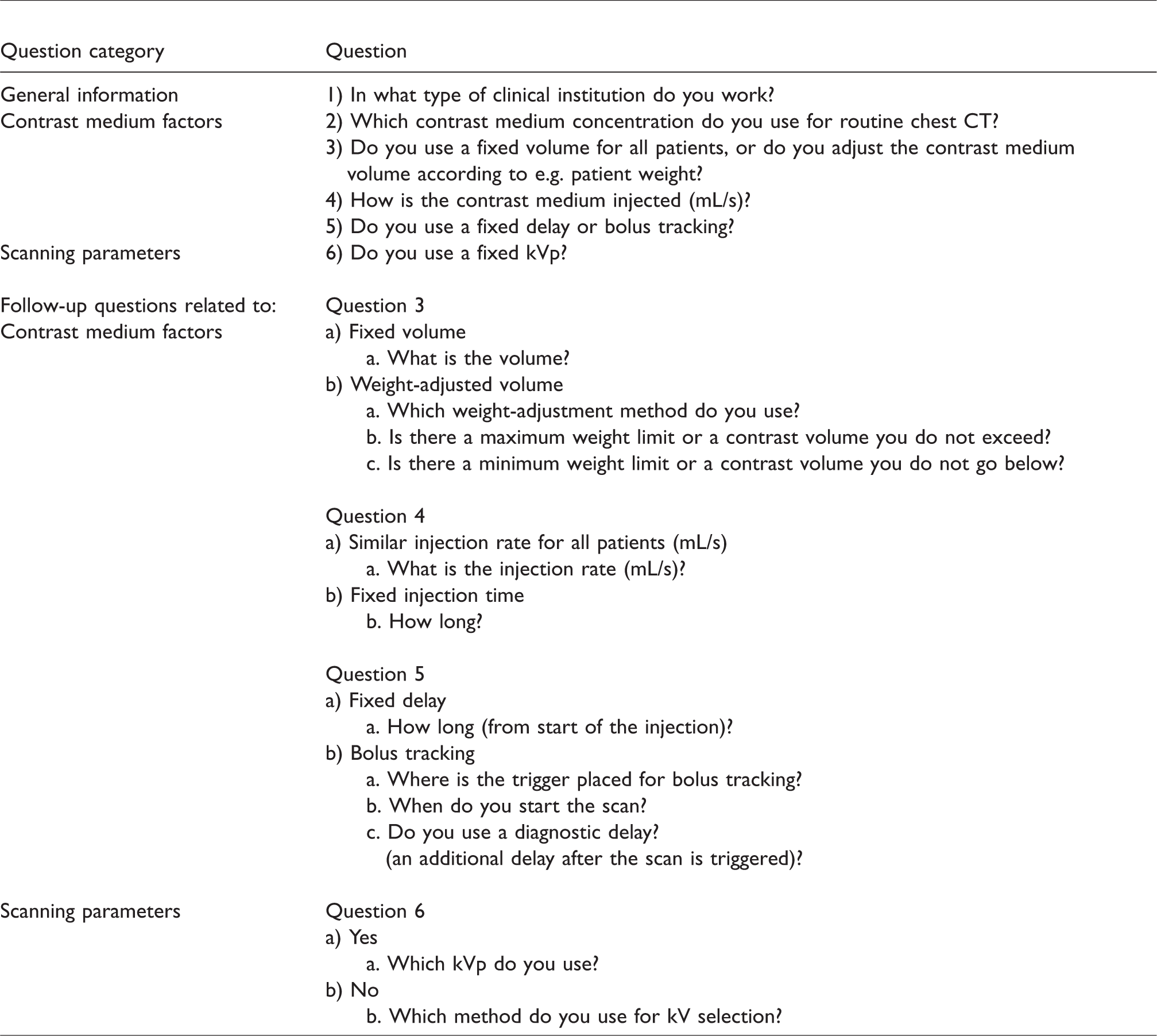
A concurrent mixed-methods design was adopted to prepare the questionnaire, which was adapted based on the study objectives to obtain information from all the participants involved in chest CT examination. The questions were verified by the research group involved in the present study. It was specified that the aim of the study was to investigate differences in administration regimes of CM in routine chest CT only, and not any combined liver/abdomen and chest CT protocols. The questionnaire comprised both quantitative, closed questions and qualitative, open-ended questions about factors affecting the CM administration in a chest CT. Closed questions allowed the respondent to choose from a list of predefined answers, whereas open-ended questions allowed respondents to input text, and were used to gather detailed and comprehensive information regarding each factor. The questionnaire was prepared and tested in the online environment after approval by the research group. Four different healthcare settings were included in the online questionnaire study: primary, secondary, and tertiary hospital levels, and private healthcare institutes. The questions were subdivided into three different topics (Table 1): (i) general information; (ii) CM-related factors affecting contrast enhancement; and (iii) scanning parameters affecting contrast enhancement. Some questionnaire items included follow-up questions to obtain more specific information. Type of CT scanner and other technical specifications were not included in the survey.
Questionnaire.
Ethics
The study was performed in accordance with General Data Protection Regulations and approved by the local Data Protection Services in Norway. Consent to participate was implied by voluntary return of the questionnaire.
Data analysis
The data were extracted from the web-based survey software Nettskjema (Nettskjema version 786, University of Oslo, Norway) or the email into an Excel 2016 spreadsheet. Data were transferred and analysis was performed with Excel and statistical software (Stata 16, 2016; Stata, College Station, TX, USA). A P value < 0.05 was considered significant. Various descriptive statistical analyses were performed. Data were described in absolute and relative frequencies. Chi-square statistics were used to compare categorical variables. Student’s t-test was performed to compare the mean contrast medium values between the different CM volume strategies.
Results
The response rate for the individual and the hospital approach was 15% (99/650) and 100% (71/71), respectively, giving an overall response rate of 24%. The response rate of the 170 individuals related to the type of healthcare institution where they work is shown in Fig. 1.

The contrast medium volumes used at the different hospital levels participating in this survey. The error bars indicate standard deviation. The pie chart shows the proportion of the responses originating from each of the four different hospital levels.
The characteristics of contrast medium factors for routine chest CT protocol are summarized in Tables 2 and 3.
CM factors used by 170 respondents.
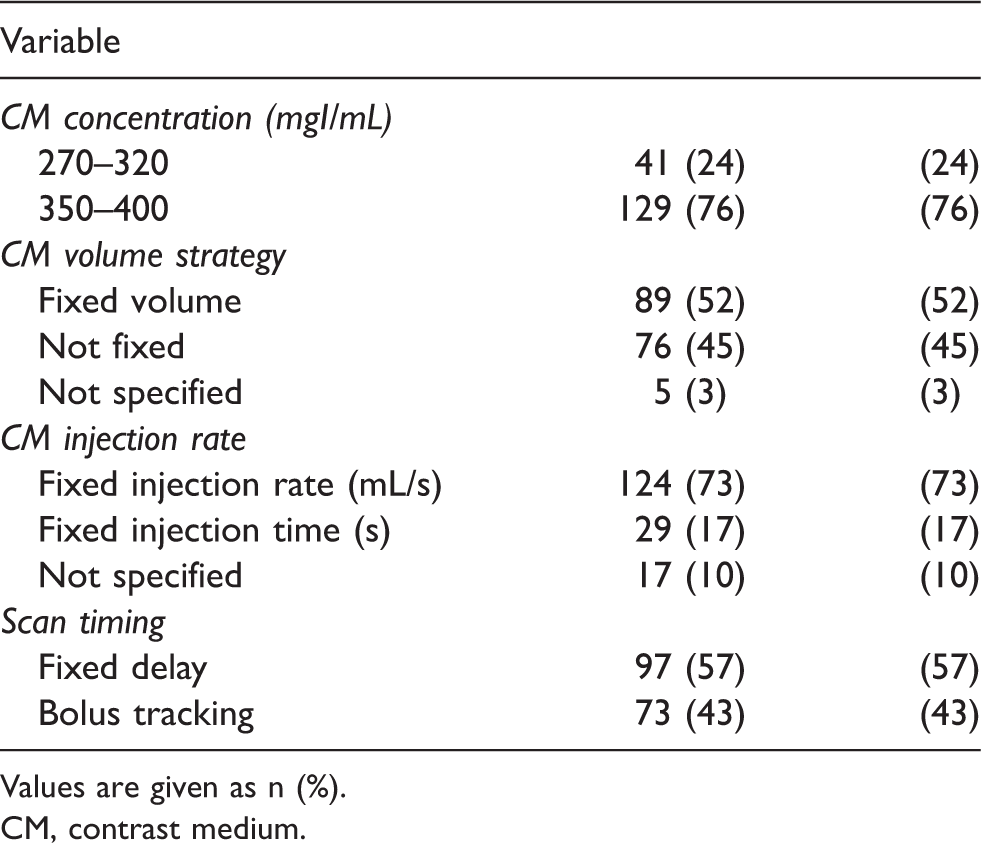
Values are given as n (%).
CM, contrast medium.
Characteristics of contrast medium factors for routine chest CT protocol.
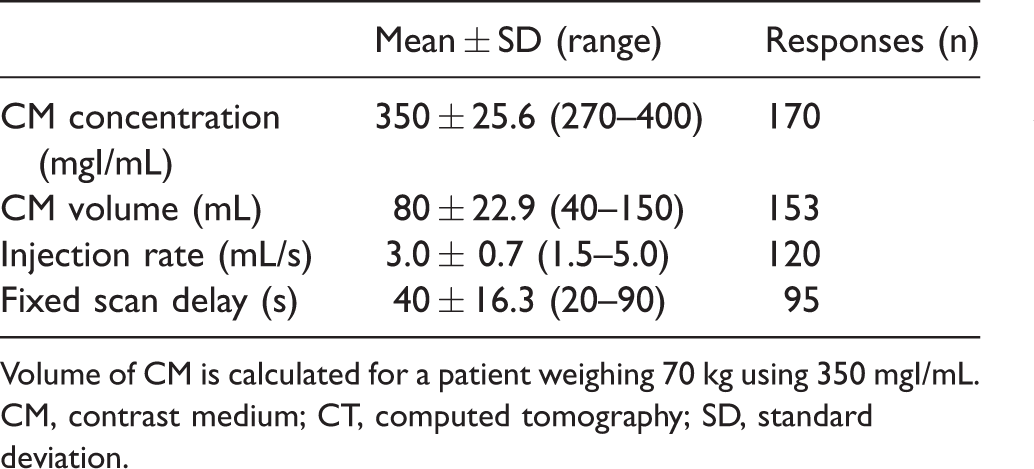
Volume of CM is calculated for a patient weighing 70 kg using 350 mgI/mL.
CM, contrast medium; CT, computed tomography; SD, standard deviation.
Concentration and volume of CM
The most commonly used concentrations of CM were 350 mgI/mL (67%) and 300 mgI/mL (19%). Of 170 respondents, 89 (52%) reported using a fixed CM volume independent of patient size, while 76 (45%) used various weight-tailored CM administration strategies (Fig. 2). Only 3% did not specify or adjusted the strategy to clinical indication.
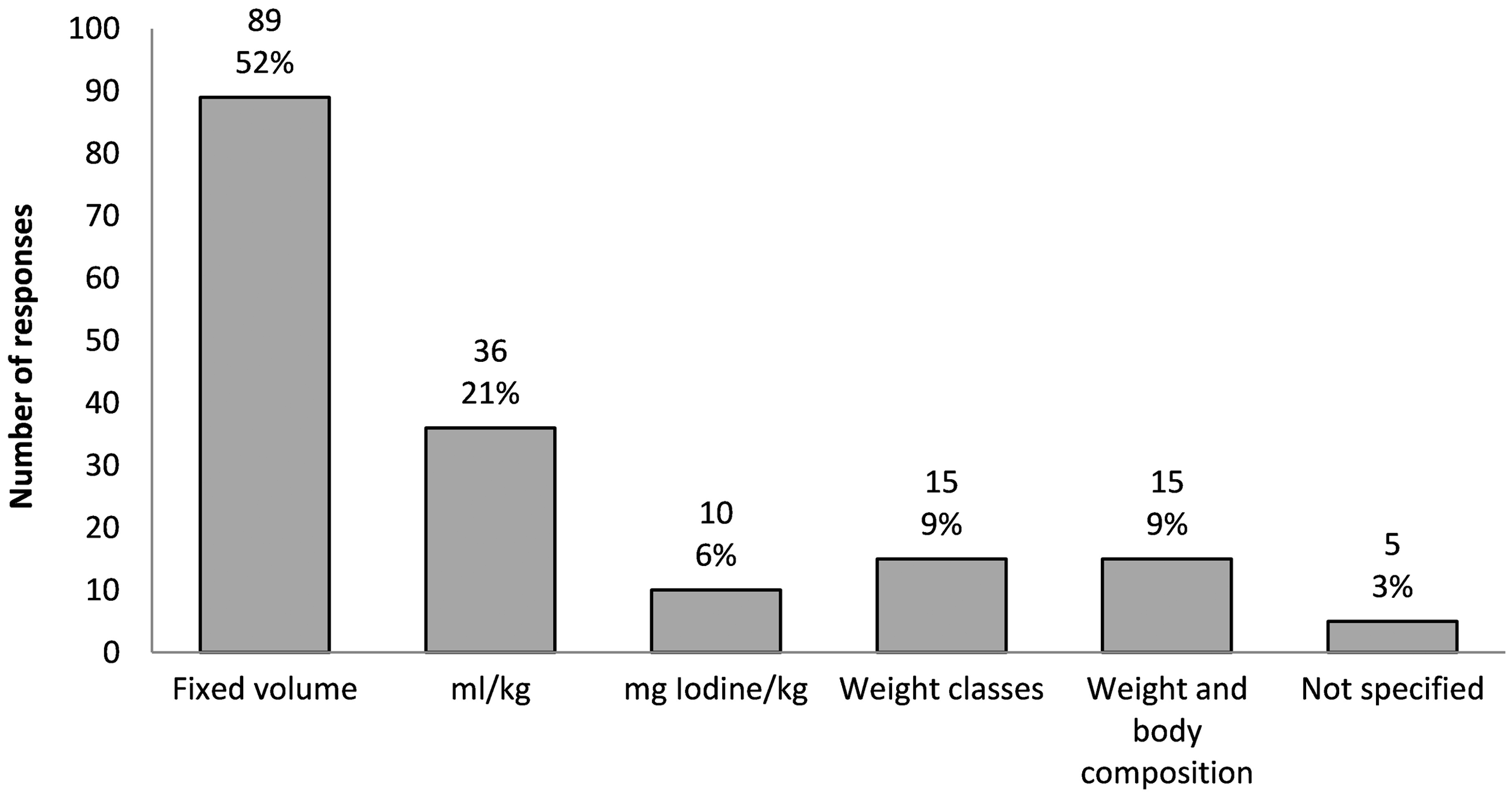
The reported contrast medium volume strategies reported by the 170 respondents.
For the respondents who reported practicing a weight-tailored strategy (mL/kg) to calculate the volume of CM, the median dosage of CM was 1.3 mL/kg, in the range of 0.6–2.0 mL/kg. Of these 36 respondents, 23 (64%) reported using 1.1–2.0 mL/kg, while 13 (36%) reported using less (0.6–1.0 mL/kg). Respondents whose weight-tailored strategy involved calculating iodine content used a median of 310 mg iodine/kg with a range of 300–500 mg iodine/kg. The patient’s body composition as strategy for CM volume assessment was reported by 9% (15/170). This strategy included volume of CM based on a combination of patient weight and subjective evaluation of body composition (i.e. fat and muscle mass in relation to total body weight [TBW]) together with a local CM dosage chart (12/15), calculations based on lean body weight formula according to patient’s sex (2/15), or use of body mass index (1/15) (data not shown). Respondents at tertiary-level hospitals more frequently used weight-based strategies (51%) than CM fixed volume (43%), while the opposite was true for respondents at the other hospital levels (Fig. 1). This difference was statistically significant (P = 0.007).
The CM volume for a patient weighing 70 kg whose dosage was calculated according to the fixed volume versus the weight-tailored strategy was in the range of 40–114 mL (median = 80 mL) versus 42–150 mL (median = 91 mL), respectively (P = 0.00014) (Fig. 3).
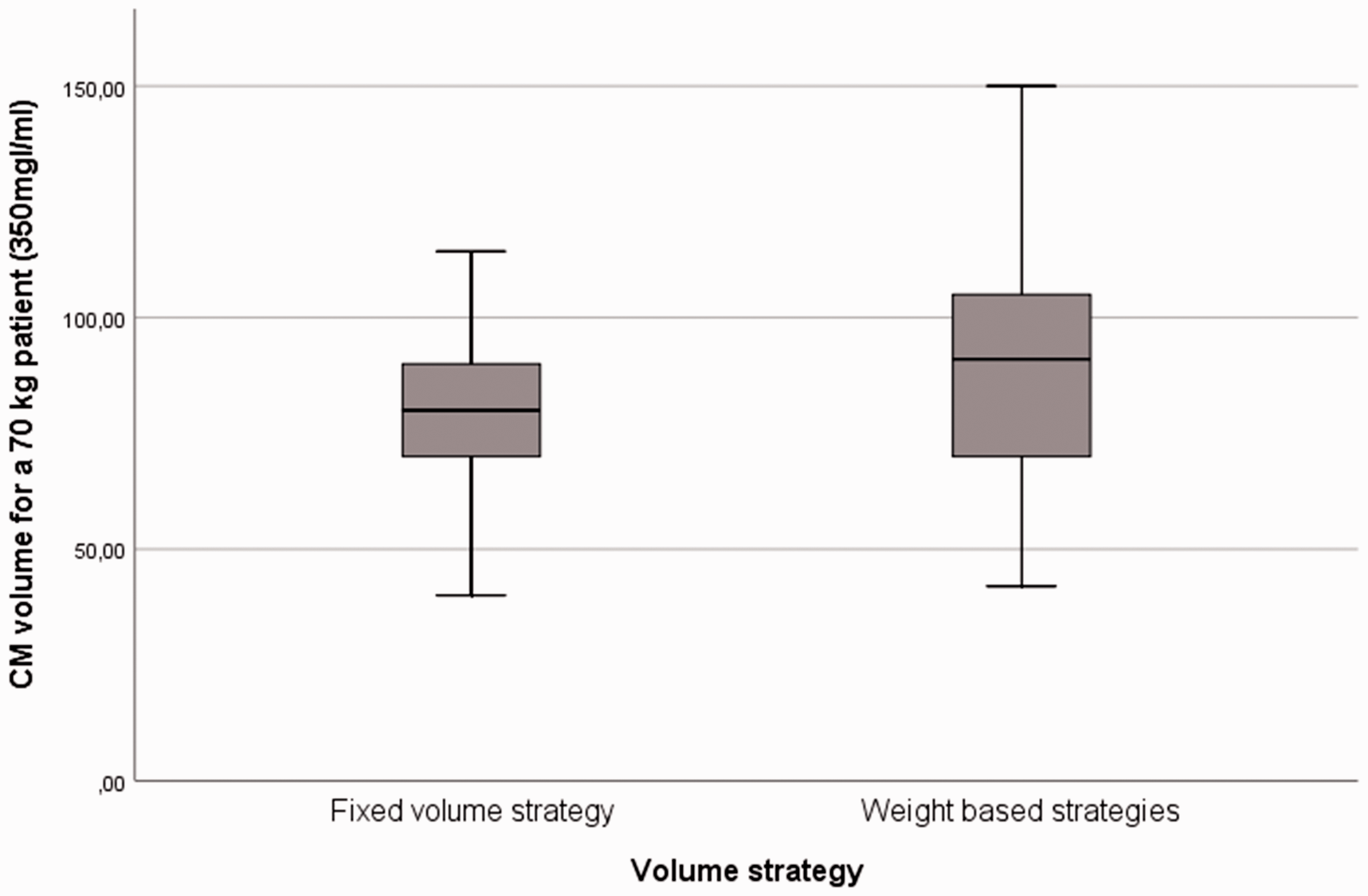
Box and whisker plots for CM volume strategies calculated for a patient weighing 70 kg using fixed and weight-based CM strategies. Weight-based strategies include weight-based and weight/body composition-tailored administration of CM. CM, contrast medium.
Injection rate and injection time of CM
Of the 170 respondents, 124 (73%) used the same injection rate in all patients, with 3.0 mL/s being the most common; however, rates were in the range of 1.5–5.0 mL/s. Of the 170 respondents, 29 (17%) used a fixed injection time, with a median of 29 s (range = 15–40 s). In addition, 17 (10%) reported varying the injection rate and/or injection time depending on different clinical or technical parameters.
Scan timing (time between CM injection start and scan start)
Of the 170 respondents, 97 (57%) reported a fixed delay, in the range of 20–90 s. Of these, 55 (57%) reported a constant delay in the range of 20–45 s, while 40 (41%) used 50–90 s. Two respondents did not specify.
Of the 170 respondents, 73 (43%) used bolus tracking to decide when to start the scan. The descending aorta was the most commonly selected anatomical reference level (32 of 73, 44%), while the ascending aorta and the pulmonary artery were selected by 25% (18/73) and 23% (17/73), respectively. Six respondents (8%) reported using other localizations or did not specify the selected level. The predefined threshold was in the range of 100–250 HU with a median value of 120 HU. Further, 49% (36/73) reported an additional diagnostic delay after achievement of predefined threshold, in the range of 4–60 s (median = 20 s).
Scanning parameters affecting contrast enhancement
Of the 170 respondents, 75 (44%) reported using a fixed kVp, while 95 (56%) used flexible kV strategies (Fig. 4). The most commonly used method for kV selection was kV modulation (81%) while only 4% reported use of dual-energy or spectral imaging as standard for chest CT.
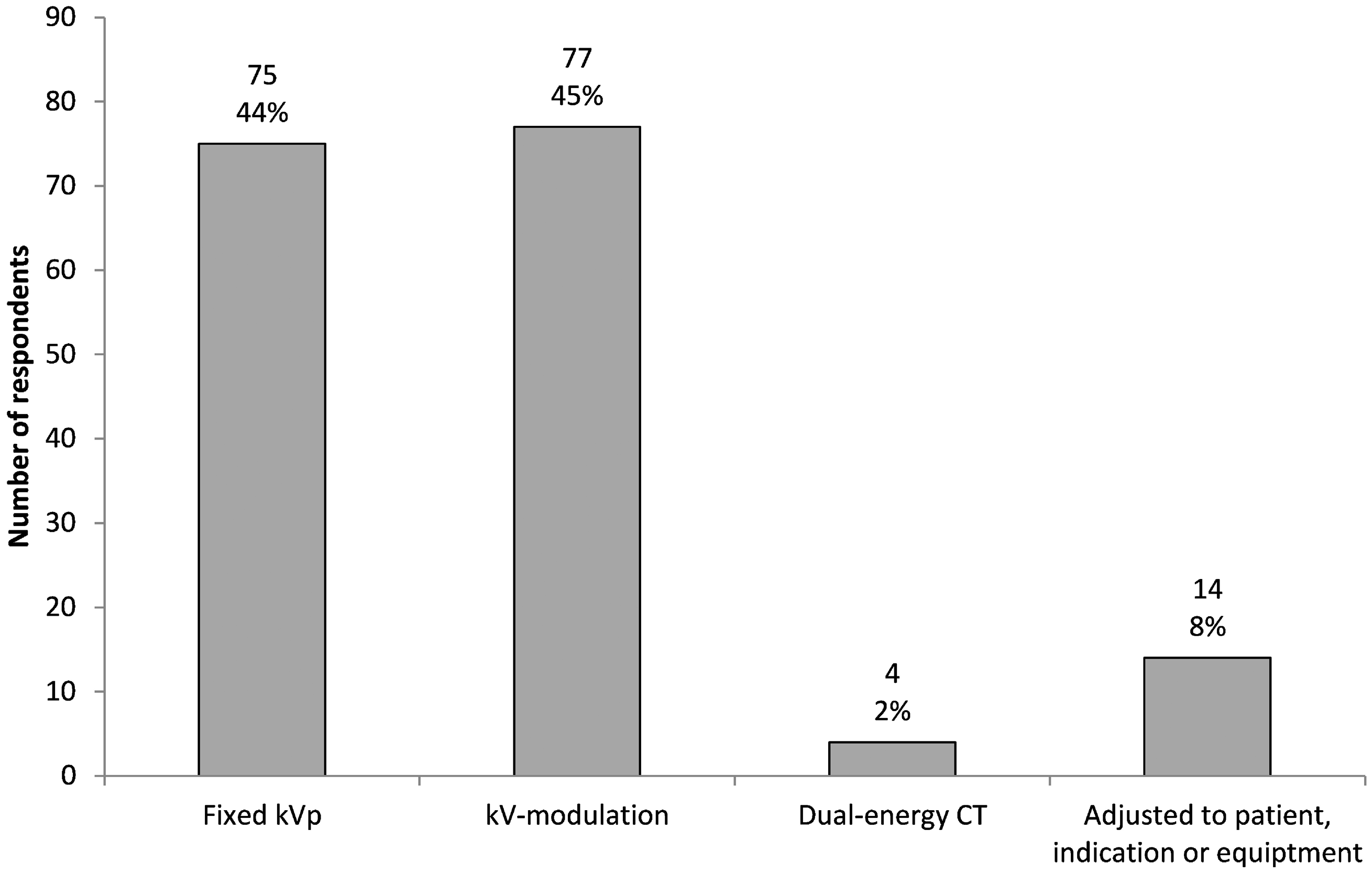
Applied tube voltage strategies in routine chest computed tomography by the 170 respondents.
Fixed kVp values were in the range of 80–140kVp; however, 120 kVp was the choice preferred by 69% of the study participants (Fig. 5).
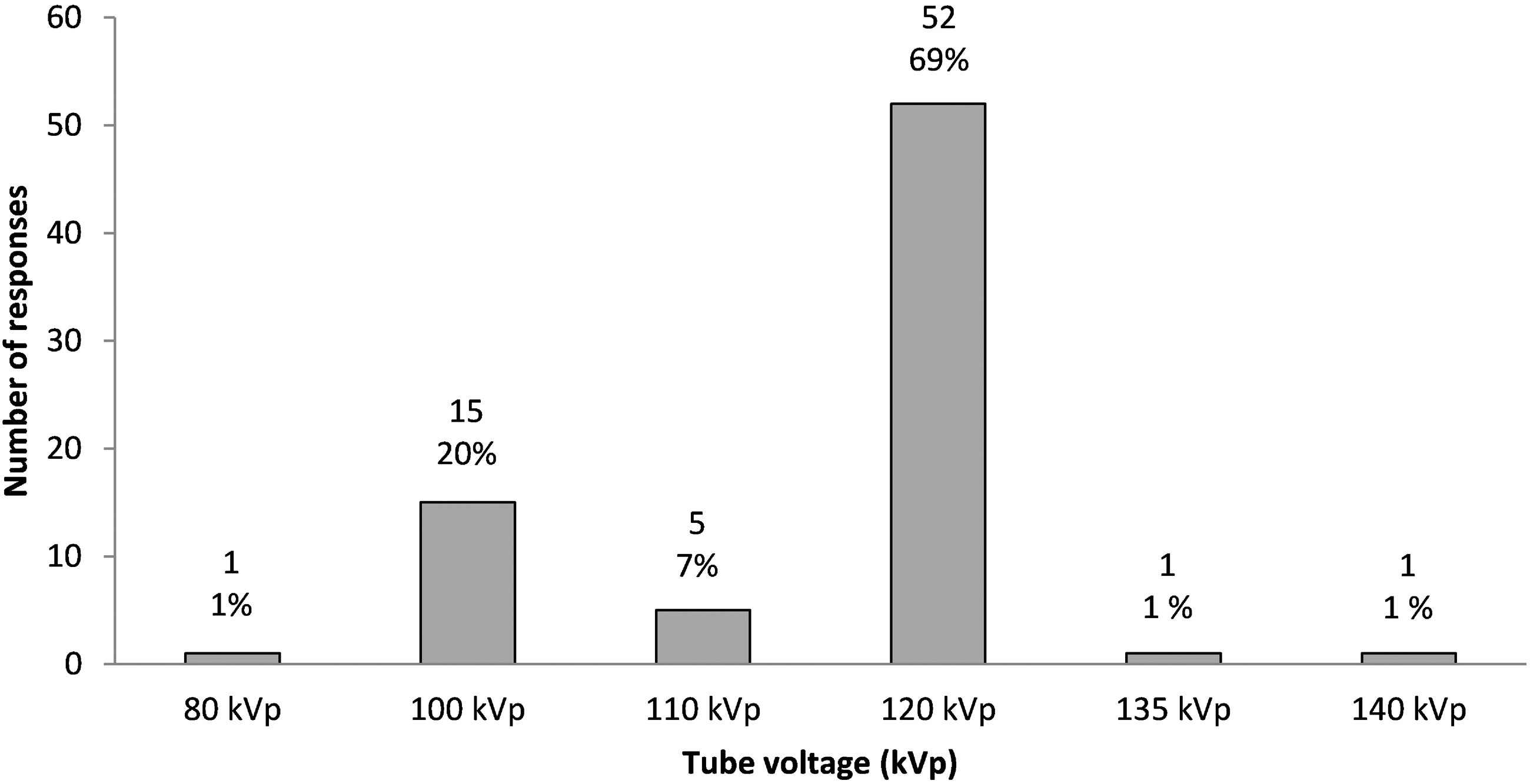
Fixed tube voltages (kVp) applied for chest computed tomography by 75/170 respondents. The rest of the participants used kV-modulation.
Discussion
This survey demonstrates the variation in CM protocols and provides data about the most common CM strategies used in routine chest CT imaging. Our results show large variations in all the principal factors affecting enhancement of CM. The greatest discrepancies appear in CM volume, injection rate, and scan timing. The respondents showed a preference for fixed CM strategies over individually adapted CM injection protocols.
The concentration of CM has substantial impact on vascular and parenchymal attenuation in CT examinations (22,23). Therefore, several studies have proposed using CM with high iodine concentrations (24–26). That this practice has been adopted was confirmed in our study, as 76% of the respondents used CM with high concentrations (350–400 mgI/mL), while only 24% used CM concentrations ≤320 mgI/mL.
The majority of the respondents (52%) reported using a fixed CM volume. This is a paradox because weight-based regimes have been shown to provide more predictable enhancement and more accurate dosing than fixed-volume protocols (8,22,27,28). However, it is important to note that a significantly higher number of tertiary-level hospitals applied weight-based strategies. These results indicate a higher degree of individually tailoring of CM volume at the tertiary-level hospitals, possibly owing to barriers to implementing evidence-based interventions into hospital systems at lower-level hospitals (29) or due to logistic difficulties. There are a number of arguments for using an individually tailored rather than a fixed CM strategy for CT examinations (13,30). Multiple weight-based regimens using several size indices have shown more robust enhancement and comparable image quality to fixed-volume strategies, despite less use of materials and lower cost (31–33). However, no single weight-based method has been conclusively shown to be superior to the others, and the assessment of body size and body composition has proven challenging (34). In the present study, TBW was reported to be the most commonly used weight-based strategy. This approach is in accordance with the publications of Eijsvoogel et al. (35) and Svensson et al. (36), where a consistent enhancement was achieved merely by adjusting to TBW, without using more complicated parameters.
The current study revealed a difference of over 100 mL for a patient with a weight of 70 kg, indicating non-consistent diagnostic quality in routine chest CT. This large variation may make it difficult to compare images and cause great interpatient variability in the results obtained from the same clinical assessment. Furthermore, the greatest variation in the volume of CM was reported by the respondents who used weight-based strategies. However, substantial divergence was found regardless of CM volume strategy. These results emphasize the need for greater consensus about how to approach chest CT. Standardized imaging protocols will provide a consistent image acquisition, and a better viewing and interpretation experience for referring providers, patients, technologists, and radiologists. Moreover, protocol standardization across regions ensures continuity of protocols regardless of location.
The effect of injection rate on contrast enhancement has been studied by a number of investigators (37–39). The median injection rate of 3.0 mL/s reported by the respondents included in the present study corresponds with the literature recommendations (Table 3) (1,40). However, this survey clearly demonstrates substantial variability in the flow rates used in routine chest CT imaging, in the range of 1.5–5.0 mL/s. Furthermore, the majority of respondents (73%) in the present study reported using a fixed injection rate rather than a fixed injection time (17%). Fixed injection time has been reported to be favorable in combination with weight-tailored CM volume as more consistent image quality can be achieved (41,42), most likely because the concentration of CM in the central blood compartment in patients of different sizes may be almost constant when this strategy is used.
The injection strategy and scan timing are critical aspects of the CT examination as they may facilitate the acquisition at a specific level of contrast enhancement (1). Based on our results, a fixed delay of ≤45 s is the most commonly used scan timing approach for routine chest CT (57%); however, reported timing varied by 70 s. The lack of consistency may be due to the fact that thoracic CT scans are routinely performed for a wide range of clinical indications, thus with a variety of protocols (21,43). While some publications recommend scanning at a 60-s delay to achieve a better evaluation of pleural findings and malignant lesions (44–46), other guidelines and authors specifically recommend scanning early, after a delay of 20–35 s (1,47). Some authors also recommend a dual-acquisition strategy including both early and delayed phases for the evaluation of pleural findings associated with malignancy (48,49). Our results illustrate that the optimal strategy for contrast enhancement in chest CT protocols still is being debated, which may explain the lack of congruent practice documented in this survey.
A kVp of 120 has been the traditional choice in chest CT scanning (24). In the present study, 44% of the respondents reported using fixed kVp, and 69% of that subgroup stated that 120 kVp still was the preferred tube voltage for routine chest CT examinations. However, the majority (56%) of the respondents used flexible kV strategies. The use of lower kVp has been reported to reduce both radiation dose and CM load in chest CT, while maintaining image quality (50,51). Especially for vascular CT examinations, lower kVp settings are advantageous as higher noise is counterbalanced by higher vascular attenuation (52). However, the present study did not investigate to what extent the CM volume strategies are adjusted to the automatically selected tube potential.
The present study has some limitations. The main limitation is its lack of representativity. The present study used two different approaches for data collection. However, the same data were collected regardless of approach. Another limitation is the low response rate: only 15% of active ESTI members responded to the online survey. This is in line with response rates in other survey studies (53,54), and the survey provides information about a subset of members. Moreover, the high response rate attained with the hospital approach improved the overall response rate.
Contrast-enhanced chest CT is performed for a wide range of clinical indications. Consequently, one must expect some lack of consistency in when and why patients are referred for chest CT, how the scans are done, and the quality of the resulting images. To minimize this problem, the invitation to participate clearly stated the aim of the study, and an open-ended question was included at the end of the survey.
A third limitation is the lack of demographic data in the 99 surveys returned electronically (individual approach), leading to the possibility of duplicate answers from Nordic respondents. However, according to the ESTI member list, only a minority of the members are in Nordic countries. This, combined with the high response rate achieved with the hospital approach, means that the participants were not evenly distributed among the countries. However, since the purpose of the study was to investigate variations in CM protocols in chest CT, duplicate answers would have little influence on the results. As such, we believe that our results are a fair reflection of current practice, particularly in the Nordic countries, and demonstrate significant variation in the CM protocols in chest CT.
In conclusion, the present study illustrates large variations in CM protocols and lack of consistency in routine chest CT imaging. The wide variability underlines the need for further research and consensus guidelines.
Footnotes
Acknowledgements
The authors are indebted to the board of the European Society of Thoracic Imaging for their support and to the respondents for contributing to this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.