
Abstract
Music is commonly found in substance using contexts yet little is known about whether music acts as an auditory cue for emotions and cravings that might lead to substance use. The current study addressed two questions: first, whether individuals in treatment for substance use disorders (SUD) show different emotional responses to music compared to matched controls, and second, whether music listening can increase and reduce cravings to use substances in individuals with SUD. Participants were 19 adults in residential treatment for SUD and 19 healthy adults matched for age and gender (both samples had a mean age of 31 years and 53% males). There were significant between-group differences in emotional response to relaxing, happy, and sad music – in particular, participants with SUD showed a dampened response to happy music. Furthermore, after listening to a participant-selected song related to their substance use, individuals with SUD experienced an increase in cravings, while after listening to a nominated abstinent song, there was a decrease in cravings. These results show that music may act as a mild auditory cue for emotions and cravings in adults with SUD. Potential uses of music in SUD treatment are discussed, such as musical stimuli for cue exposure.
The role of music as an important therapeutic tool is well established in the treatment of many psychological disorders including psychosis (Gold, Solli, Krüger, & Lie, 2009), depression (Maratos, Gold, Wang, & Crawford, 2008), and other internalising disorders such as anxiety and social withdrawal (Miranda, Gaudreau, Debrosse, Morizot & Kirmayer, 2012). In the arena of substance use disorders (SUD) however, practice and research regarding music is still in its infancy (Aldridge & Fachner, 2010; Dingle, Gleadhill, & Baker, 2008; Silverman, 2003). As a result, many fundamental questions about how individuals with substance use problems respond to music have not been answered. One of these basic questions is: how do substance users respond emotionally to music? If individuals in treatment for substance use disorders show a different emotional response to music compared to healthy controls, does this have implications for treatment of substance misuse?
Emotional responses to music
Strong emotions are one of the most widely cited maintaining factors for substance misuse in that the substance numbs or alleviates negative internal states – a process of negative reinforcement (Kassel, 2010; McCarthy, Curtin, Piper, & Baker, 2010). Furthermore, a large body of research demonstrates that music listening can both induce and help alleviate strong emotions (Juslin & Sloboda, 2010). Therefore, understanding how substance users emotionally respond to music has potentially important implications for substance use treatment. Of the published studies investigating the emotional responses of substance users to music, the majority have investigated substance users’ emotional responses to music therapy techniques (Baker, Gleadhill, & Dingle, 2007; de l’Etoile, 2002; Jones, 2005; Silverman, 2003, 2011; Soshensky, 2001). Only one study to the authors’ knowledge has explored the effects of everyday music listening on the emotional responses of substance users (Dingle, Kelly, Flynn, & Baker, under review). In this study, participants were asked to reflect on their substance using period prior to admission into treatment, and to describe how music affected their substance use experience and vice versa. While more than half of the participants chose not to answer these two questions, among those who responded, emotional effects were most noticeable. For example, music played during substance use was reported to enhance the euphoria from the substance use (41.2%) and also to enhance feelings of sadness and loss (23.5%). Music listening during substance use also influenced the vividness of dreams and memories (17.6%). Conversely, substance use while listening to music was reported to intensify both positive and negative emotional responses (21.4%). A minority (14%) indicated that the combination of music and substances made them feel worse. Although these preliminary findings do suggest that substance users have strong emotional responses when listening to music, it is unknown whether these effects occur once individuals have entered treatment and are abstinent from substance use.
The most well-established experimental protocol for examining listeners’ emotional responses to music has been to record individuals’ responses to specific musical stimuli, often in the form of short pieces of classical music which have been previously shown to induce specific emotions (see, e.g., Baumgartner, Esslen, & Jäncke, 2006; Etzel, Johnsen, Dickerson, Tranel, & Adolphs, 2006). The current study used this protocol to examine emotional responses to happy, sad, and relaxing music among individuals with SUD, and in particular, to determine if their emotional responses to music differ from that of matched control participants.
Craving responses to music
The second aim of the study was to examine the relationship between music listening and craving for substances in the SUD treatment sample. Craving has been described in the DSM-5 (American Psychiatric Association, 2013) as “a strong desire or urge to use the substance” and desire may be defined as “an affectively charged cognitive event in which an object or activity that is associated with pleasure or relief of discomfort is in focal attention” (Kavanagh, Andrade, & May, 2005, p. 447). Cue reactivity research demonstrates that visual and olfactory cues for substances can induce cravings (Loflin & Earleywine, 2014; Pulido, Brown, Cummins, Paulus, & Tapert, 2010). This occurs through a classical conditioning process of repeated exposure to environmental cues (such as the sight of alcohol or the smell of cannabis) paired with thoughts regarding the substance’s effect. Consequently in the presence of the same cue, the conditioned thoughts then drive urges to use the substance (Stacy, Widaman, & Marlatt, 1990). The links between cues, cravings and substance use behaviour are well established and therefore strategies to manage craving are commonly included in treatment programs for substance addiction (Addolorato, Abenavoli, Leggio, & Gasbarrini, 2005; Weiss et al., 2003).
In cue exposure treatments, the participant is repeatedly exposed to stimuli relevant to the substance of abuse while the behaviour itself (use of the substance) is prevented. Over time, this process is expected to stop (extinguish) the substance use response to the cue. However, a meta-analysis of clinical studies using cue exposure treatment for a range of substances found it was ineffective (Conklin & Tiffany, 2002). The authors referred to evidence from animal studies to argue that cue exposure has not been effective because it is typically conducted in a setting that is isolated from the usual substance using context. Take, for example, a person who is alcohol dependent and undergoing cue exposure treatment in a rehabilitation centre where there is no alcohol. Conklin and Tiffany (2002) argue that the link between alcohol cues and drinking behaviour for this person will be stronger (and likely to be reinstated) in their home context where it was learned rather than in the rehabilitation context. This evidence indicates that cue exposure treatment could be improved by incorporating a broader range of contextual cues that approximate the participants’ typical substance using environment.
Despite the fact that music is commonly found in the environmental context of substance use, little is known about the potential for music to act as an auditory cue for substance cravings and use. For example, an individual who has repeatedly smoked cannabis while listening to reggae music may experience cravings for cannabis when s/he hears reggae music during a period of treatment. But is there any direct evidence that music can cue cravings for substances? Despite anecdotal evidence suggesting it can (Horesh, 2010), the question has received very little research attention. Dingle, Kelly, and colleagues (under review) explored this question by surveying 106 clients from six different residential rehabilitation services, and 43% of clients reported that listening to particular songs increased their urge to use substances. Although these results suggest that music can increase cravings (at least in some individuals) only one study has tested this link using experimental methods. In this study, Jansma, Breteler, Schippers, De Jong, and Van der Staak (2000) played participants a “depressing” music clip in order to test the influence of depressed mood on cravings. This study found no effect of the depressing music on cravings; however, the music was paired with the cues of pouring and sniffing a glass of alcohol so the specific effects of the music could not be determined.
If music can indeed increase cravings in substance users, the next logical question is can music also reduce these cravings? In a study exploring this question, Silverman (2011) assigned 141 patients in a detoxification unit to either a “rockumentary” music intervention (lyric analysis of the song “Under the Bridge” by the Red Hot Chili Peppers along with discussion of the band’s history and substance use and questions about how the lyrics relate to the clients’ own substance use and recovery), a recreation music therapy condition (“music bingo” plus discussion), or a (non-music related) verbal therapy condition and measured differences between groups in cravings. Results revealed no statistically significant differences between groups at post-test (post-test only design), though participants in both music therapy conditions had lower mean craving scores than participants in the verbal therapy condition. Overall, these results do suggest that music had a favourable impact on cravings; however, the study did not gather pre-test data and therefore it is unclear whether music did indeed decrease cravings from pre- to post-test. Furthermore, it is not possible to determine the influence of music listening in particular upon cravings from these results because several music therapy methods were used in combination in this study.
The current study uses an experimental design in which adults undergoing residential treatment for SUD (and a matched control sample) will be played experimenter-selected music that has been found in previous research to elicit emotions of relaxation, happiness, and sadness in listeners. Previous research suggests that adults in treatment for substance use disorders are emotionally sensitive to music, therefore hypothesis 1 is that there will be no difference between the treatment group and the control group in emotional responses to happy, sad, and relaxing music. In addition, we will investigate participants’ urge to use a substance before and after hearing a piece of music s/he nominates as being associated with previous substance use, and after hearing a second piece of music selected for helping him/her stay abstinent. In accordance with the principles of cue conditioning and earlier research suggesting that adults in treatment for substance use disorders experience an increase in urge to use substances when listening to personally relevant music, hypothesis 2 is that there will be an increase in urge to use substances after listening to a participant-selected “urge” song, and a decrease in urge to use substances after listening to a participant selected “clean” song.
Method
Participants
SUD sample
Nineteen participants were receiving treatment at a residential Therapeutic Community in Queensland, Australia. The sample had a mean age of 31.05 (SD = 5.94), nine were female, and 10 male. The treatment program was of six months duration and at the time of testing participants had been living at the Therapeutic Community an average of 64 days (SD = 48). The program requirements included complete abstinence from alcohol and drugs (besides prescription medications) and daily participation in therapeutic activities (e.g., relapse prevention groups). Residents were accepted into the program after a clinical interview had determined that they met DSM-IV criteria for substance dependence. 1 Participants’ most problematic substance was alcohol (42%), amphetamines (32%), marijuana (11%), prescription drugs (11%), and heroin (5%). All but one participant reported being a polysubstance user (more than one substance in a day), with the mean number of years of polysubstance use of 12.47 years (range: 1–24 years). Regarding musical involvement, 26% of the sample was currently singing in a choir/group or playing a musical instrument, 63% had done so at some point in their lives, with a mean number of years doing these activities of 7.11 years. Regarding levels of enjoyment for classical music, the SUD sample had a mean rating of 2.58 out of a possible 7 (1 = not at all to 7 = a great deal).
Control sample
Nineteen age and gender matched controls were recruited through word of mouth via their acquaintance with the first author. The absence of a substance use disorder in each control participant was determined by means of a short interview with a qualified clinical psychologist. Regarding musical involvement, 26% of the sample was currently singing in a choir/group or playing a musical instrument, 84% had done so at some point in their lives, with a mean number of years doing these activities of 7.47 years. The mean rating of enjoyment for classical music was 4.16 out of a possible 7. There was no significant difference between the two samples in the percentage of the sample currently singing in a choir/group or playing a musical instrument: χ2 (1, N = 38) = 1.00, p = .32, percentage who had done so at some point in their lives: χ2 (1, N = 38) = 0.27, p = .60, or in the mean number of years doing these activities: F (1, 37) = 0.02, p = .89. There was a significant difference between groups in enjoyment for classical music: F (1, 37) = 7.67, p < .01, so this was entered as a covariate in the relevant analyses. A power analysis using the software package G*Power 3.1.9.2 (Faul, Erdfelder, Lang, & Buchner, 2007) calculated that for a repeated measures ANOVA with mixed within–between interactions, N = 38 with two groups and three measurements, a medium effect size (0.25) and alpha set at 0.05, the power is 0.92.
Measures
Genre preferences
Participants’ preferences for musical genres were assessed via 14 items each representing a different genre (blues, jazz, classical, folk, rock, alternative, heavy metal, country, soundtracks, pop, rap/hip-hop, RnB/soul/funk, electronic/dance, and religious) based on the most preferred music genres in previous research (Schäfer & Sedlmeier, 2009). Participants were asked to rate their “level of enjoyment for each musical style” on a 7-point Likert scale (1 = not at all to 7 = a great deal).
Emotional response
Emotional valence after each piece of music was assessed with the item “How pleasant/unpleasant do you currently feel?”, which listeners rated on a 7-point Likert scale from 1 = very unpleasant/negative to 7 = very pleasant/positive. Emotional arousal was assessed with the item “How calm or aroused do you currently feel?”, also rated on a 7-point scale from 1 = very calm to 7 = very aroused. The second measure of emotional response, the Geneva Emotions in Music Scale (GEMS-9; Zentner, Grandjean, & Scherer, 2008) is a 9-item self-report scale that measures the type and intensity of an individual’s emotional response to a musical stimulus. Specifically devised to measure musically evoked emotions directly following music listening, each of the 9 items represents an emotion label (e.g., “Peacefulness”), and within each emotion label are emotion adjectives which help to define each label (e.g., “Peacefulness: serene, calm, soothed”). Respondents rate the intensity with which they feel each emotion label on a 5-point Likert scale (1 = not at all to 5 = very much). For the purpose of the current study, only the three GEMS-9 items representative of the emotions induced by the three music pieces were analysed. These were “Peacefulness: serene, calm, soothed” (for the Relaxing music condition), “Joyful activation: joyful, amused, bouncy” (for the Happy music condition), and “Sadness: sad, sorrowful” (for the Sad music condition).
Craving measures
Craving to use substances was assessed after each music stimulus by a single item formulated for this experiment: “I have an urge to use/drink” on a 7-point Likert scale (1 = no urge to 7 = very strong urge). In addition, an adapted version of the Alcohol Urge Questionnaire (AUQ; Bohn, Krahn, & Staehler, 1995) was used. The AUQ is an 8-item measure of drinking urges and asks participants to endorse the extent to which they agree or disagree with statements relating to their desire to drink, expectation of a desired outcome from drinking, and inability to avoid drinking if alcohol was available. The scale has high internal consistency (α = 0.91), high test-retest reliability (1-day acute craving complete interval, 0.82), and good construct validity evidenced by strong correlations with measures of alcohol dependence severity and the Obsessive Compulsive Drinking Scale (Love, James, & Willner, 1998). Item wording was adjusted so that all items were applicable to both drug use as well as alcohol use.
Music stimuli
Three separate pieces of classical music were chosen which previous research had shown to elicit feelings of relaxation, happiness, and sadness in listeners (Sandstrom & Russo, 2013; Witvliet & Vrana, 1996). The relaxing music was Georges Bizet’s Carmen Suite no. 1: Intermezzo; the happy music was Mozart’s Horn Concerto No. 4 in E flat major, K495: Rondo, Allegro vivace; and the sad music was John Stanley’s Grand Voluntary in D major, Adagio. Witvliet and Vrana (1996) demonstrated that these three songs reliably induced the three different emotional states in two separate samples of undergraduate students (N = 85 and N = 67). Each piece was played for 60 seconds. The title and artist of the urge songs and clean songs nominated by participants in the treatment sample are listed in Table 1.
Urge songs and clean songs nominated by the adults in residential alcohol and drug treatment.

Procedure
SUD sample
For each participant, testing was carried out in three phases. In the first phase, participants completed a 5–10 minute questionnaire which included items regarding participant demographics, substance use history, music involvement, and the music genre preference items. Couched within this questionnaire were two items which asked each participant to nominate an “urge song” (“Please write below a song that makes you want to use/drink?”), and a “clean song” (“Please write below a song that helps you stay clean/sober?”). The second and third phases were carried out one week later so as to reduce any effect of priming in the experimental procedure. In the second phase, participants completed baseline measures of their emotional state (valence, arousal, GEMS-9) and cravings (single-item, adapted AUQ). They were then asked to listen to the three pieces of classical music (relaxed, happy, and sad), and directly following each piece, participants rated their emotional response and cravings. Participants were given written instructions to rate how the music made them feel and not to describe the music or what emotion it might express. The order of presentation of the three musical stimuli was counterbalanced. In the third phase, participants listened to their selected “urge song” followed by their selected “clean song”. After each song, participants again rated their emotional response and cravings. All stimuli were presented and responses gathered on a computer interface using Qualtrics survey software. Music stimuli were downloaded from iTunes and embedded in the experimental procedure for each unique participant.
Control sample
The age and gender matched controls completed phase one and two of the experimental procedure described above (without the cravings measures). Participants in both groups were all required to listen to the music excerpts using headphones (Sennheiser HD215). All participants were also assured of voluntary participation and confidentiality, and each was debriefed as to the purpose of the study following completion. The methods were approved by the University of Queensland Ethics Committee, #201100953.
Results
Emotional responses to music
Valence
Mean valence ratings for each group across the three music emotions are presented in Figure 1. A 2 (Samples) × 3 (music emotions) mixed analysis of variance conducted on valence showed no main effect of group: F (1, 36) = 0.49, p = .491. There was a significant main effect of music emotion: F (1.65, 59.39) = 14.03, p < .001,

Mean emotional valence ratings for relaxing, happy, and sad music given by 19 adults with substance use disorders (diamonds) and 19 matched controls (squares).
Arousal
Mean arousal ratings for each sample across the three music emotions are presented in Figure 2. There is a clear divergence of arousal response between the two samples when listening to the happy music. A 2 × 3 mixed ANOVA showed no significant main effect of sample: F (1, 36) = 0.34, p = .564 or music stimulus: F (2, 72) = .51, p = .602. However, the group × music interaction was significant: F (2, 72) = 7.95, p < .001,
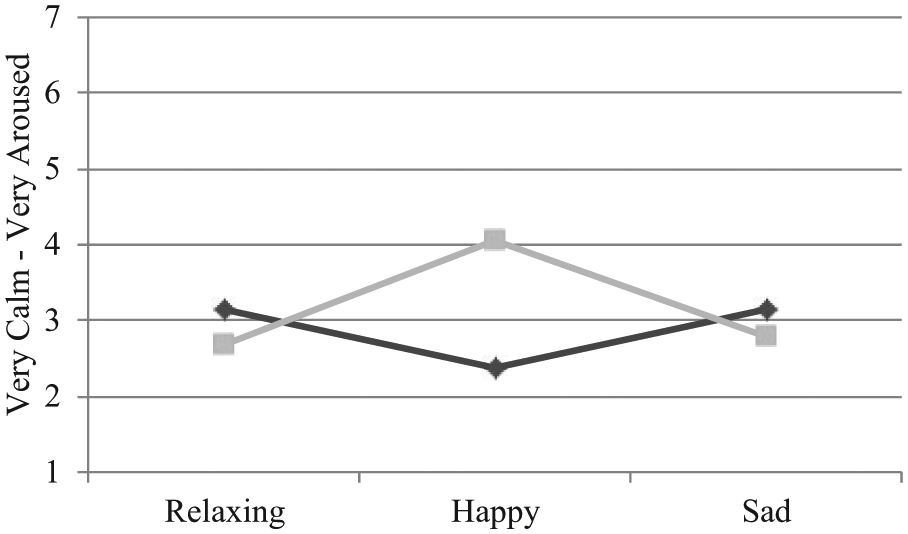
Mean emotional arousal ratings for relaxing, happy, and sad music given by 19 adults with substance use disorders (diamonds) and 19 matched controls (squares).
GEMS items
Group means on the GEMS items for each music piece are presented in Figure 3. Results of three separate one-way ANOVAs revealed that there was a significant difference between groups for the happy music: F (1, 36) = 14.00, p < .01,
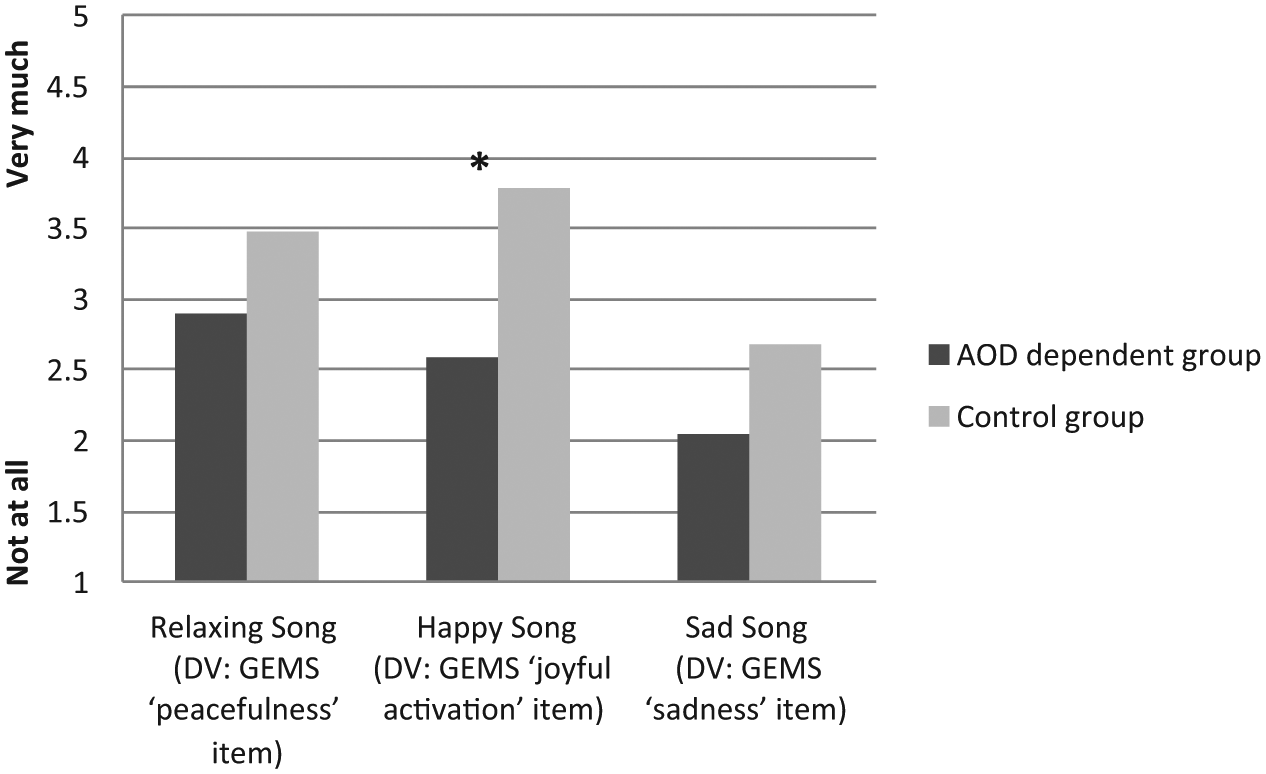
Group means on the Geneva Emotion in Music Scale items for each music stimulus.
Music and cravings
Single craving item
A one-way repeated measures ANOVA revealed a significant effect of Time on craving: F (153, 27.46) = 19.01, p < .001,
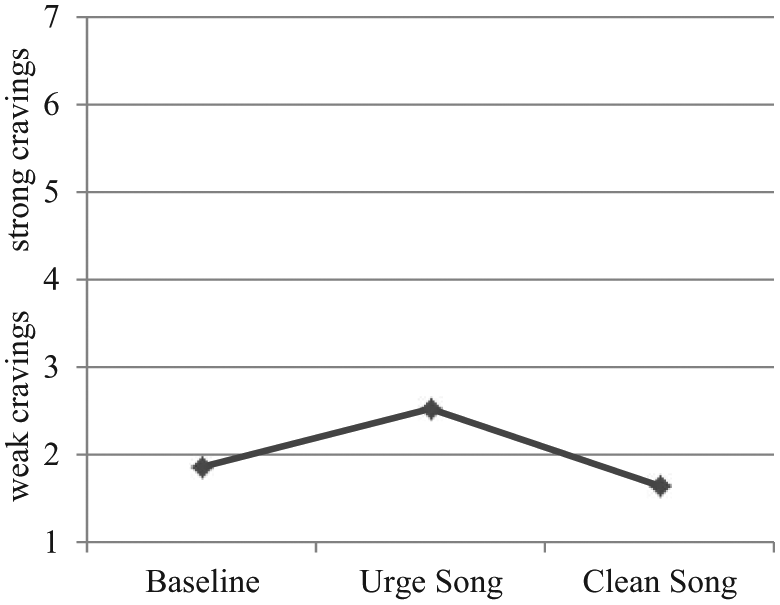
Mean ratings on the adapted Alcohol Urge Questionnaire at baseline and after listening to music in 19 adults with substance use disorders.
Adapted AUQ
A similar pattern of results was found on the adapted AUQ (see Figure 4). A one-way repeated measures ANOVA revealed a significant effect of Time on craving: F (2, 36) = 15.44, p < .001,
Discussion
The current study aimed to answer some fundamental questions regarding how individuals in treatment for substance use disorders respond to music. We first explored whether people with SUD have different emotional responses when listening to experimenter-selected relaxing, happy, and sad music compared to healthy controls. Overall, results revealed that compared to controls, the participants in the therapeutic community showed significantly less variation in emotional response across relaxing, happy, and sad music. The group difference was most pronounced for happy music whereby the SUD individuals’ ratings of pleasure (valence), intensity of joyful activation and emotional arousal were significantly lower than controls’. The results cannot be attributed to differences between groups in musical involvement and training, as the groups had comparable musical backgrounds. In terms of different preferences for classical music, Table 1 shows that the participants in the SUD sample listened to music from genres such as hip-hop, rock, pop, and RnB but did not list any classical music pieces as either their “urge” song or their “clean” song. Furthermore, their mean preference rating for classical music was significantly lower than that for the Control sample. Experimenter-selected classical music excerpts were used in the study because they have been found in previous research to evoke the desired emotional states and we wanted experimental control over the music stimuli. However, it is quite possible that the pattern of emotional responses was influenced by the experimenter-selected music and further research is required to understand how SUD participants respond emotionally to personally meaningful happy, sad, and relaxing music.
Another possible explanation for the between-group effects – in response to both happy and sad music – was the likely presence of depression in the SUD group. Separate research conducted at the same therapeutic community revealed high rates of depression amongst residents, particularly in first few months after entering the program: 44% had experienced serious depression in the month before entering the community, and 22% had suicidal thoughts (Dingle, Stark, Cruwys, & Best, 2014); however, depression symptoms were not measured in participants of the current study. The SUD sample rated the sad music as more pleasant and less sad than the Control sample; and they rated the happy music as less pleasant and less joyful than the Control group. Assuming that participants experienced some depressed mood, this pattern of responses to happy and sad music may reflect a preference for music that is mood-congruent, as has been found in previous research (Papinczak, Dingle, Stoyanov, Hides & Zelenko, 2015; van den Tol & Edwards, 2013). Furthermore, previous research has revealed that people with depression show more blunted emotional responses to musical excerpts representative of a range of emotions (Al’tman, Alyanchikova, Guzikov, & Zakharova, 2000; Osuch et al., 2009; Punkanen, Eerola, & Erkkilä, 2011).
Although the effect of music on emotions in this study was modest, it is consistent with a larger body of research on the uses of music to influence mood and/or behaviour, both in the addiction treatment context (Baker et al., 2007), and other settings such as music mood induction during laboratory studies (Etzel et al., 2006), music for anxiety and pain management in dental and medical settings (Bernatzky, Presch, Anderson, & Panksepp, 2011; Thoma et al., 2014) and music to influence emotions and performance in sporting contexts (Lane, Davis, & Devonport, 2011).
The second research question explored whether music listening could influence cravings for substances in people with SUD undergoing rehabilitation. To the authors’ knowledge, this was the first study to empirically test whether music listening alone can influence self-reported cravings to use substances using an experimental pre–post music listening design. Figure 4 shows that at baseline, participants’ cravings and urges to use substances were rated as low. Listening to their nominated urge song significantly increased ratings of cravings and urges to use substances, and these ratings returned to baseline following listening to their nominated clean song. Although these changes in cravings were not dramatic, they were observed for the majority of participants. It may be that music stimuli evoke a milder craving response than other stimuli directly associated with the substance (such as the sight or smell of drug taking equipment), although a direct comparison of various types of stimuli is needed in order to verify this. The modest changes in cravings may be explained by the fact that participants were already settled in rehabilitation, were stabilised in terms of physiological withdrawal, and had already learned several strategies and techniques in the treatment program to control and contain their cravings. A limitation of the study was that we played the urge song before the clean song in all cases to ensure that participants would not complete the study with an increased urge to use substances. Unfortunately this means the effect of listening to the “clean” song on its own remains uncertain. Nevertheless, this finding suggests that clients could listen to their clean song/s while experiencing a craving to experience a modest decrease in craving.
The clinical implications of the findings are that individuals in SUD treatment should be strategic in their choice of music to evoke the effects they want. For instance, it may be useful to evoke strong emotions during therapy so that clients can explore and learn to tolerate these emotions in a substance-free environment (Baker et al., 2007). Given their blunted emotional response, clinicians may need to work with clients to select pieces of music that induce high levels of emotional valence and arousal, and additional techniques may be required to strengthen the intensity of their emotional experience (e.g., imagery – see Holmes & Matthews, 2010) in order for emotions to reach a threshold with which they can be effectively explored.
There are several important clinical implications of the findings regarding cravings. First, clinicians could educate clients in SUD treatment about the potential effect of their everyday music listening on cravings. An analysis of the nominated urge songs and clean songs is beyond the scope of the present study; however, it can be seen from the song list in Table 1 that many of the urge songs contained themes about substance use and some lyrics normalise or even glorify substance use (for example, Blister in the Sun by the Violent Femmes contains the lyrics “… yeah I’m so strung out, I’m high as a kite I just might stop to check you out”; while the song Drugged and Driving by Dayglow Abortions includes the lyrics “I just ate 25 speeders and I could feel the adrenaline … I stepped on the gas and went with the power”). The messages in such songs are working against the messages that participants receive in treatment and this is an issue that clinicians could bring to their clients’ attention during a discussion of their music listening choices. Clients could be encouraged to review the music in their personal music players to identify songs that trigger and reduce urges to use, and when to listen to them. Simply identifying these songs and raising clients’ awareness of their effects may constitute a useful intervention.
The current findings also highlight the potential for music to be included as part of cue exposure treatment for substance use disorders. Cue exposure therapy is gaining acceptance as a useful treatment for substance use disorders, although there is mixed scientific evidence regarding its efficacy (Carter & Tiffany, 1999; Conklin & Tiffany, 2002). The cues traditionally employed in cue exposure therapy treatment have been alcoholic beverages, drug using equipment, and external environments previously associated with drinking and using. Clients in early abstinence may find such cues extremely confronting and as a result cue exposure therapy has been associated with high drop-out rates (Marissen, Franken, Blanken, van den Brink, & Hendriks, 2007). Music listening may constitute a more tolerable and context relevant stimulus for use in cue exposure procedures and could even be used as a first step in a cue exposure hierarchy.
Future research could investigate whether the blunted emotional response to music of SUD individuals is also found on physiological measures. Although there would be some practical and logistical considerations to overcome, it would also be interesting to conduct brain imaging of people in SUD treatment while they are listening to their urge song and their clean song, to further examine which brain regions may be implicated in these responses to musical stimuli. Additional contextual influences could be explored to ascertain if the effects found in the current study change when participants listen to music in groups (vs. alone), and when living in the community (vs. in residential treatment), as previous research suggests that emotional responses vary depending on the listening context (Gabrielsson, 2001; Scherer & Zentner, 2001). As mentioned above, it would also be worthwhile investigating whether the results found in the current study generalise to relaxing, happy, and sad music selected by participants, and of different musical genres.
In conclusion, this study found preliminary evidence that music listening can act as an auditory cue for emotions and cravings among adults in treatment for substance use disorders. Music listening holds potential as stimuli for personalised cue exposure therapy for these individuals.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.