
Abstract
An overview of the literature and theories concerning revenge is presented in this study. The aim is to clarify the boundaries between a healthy and pathological way of dealing with revenge to improve diagnostics, with regard to both theory and clinical practice. Revenge is an intrapersonal phenomenon and the extent to which people need revenge has a certain degree of stability. A healthy way of dealing with revenge may restore the psychological balance that has previously been disturbed. However, the desire for revenge can be long-lasting and dysfunctional due to, among other things, early problems in development and specific personality traits. Consequently, a pathological way of dealing with revenge can be part of a disorder and can lead to destructive acts such as homicide and even mass murder. Some clinical examples are presented and points of attention regarding diagnostics and treatment are discussed.
In Germany in 1981, Marianne Bachmeier killed the murderer of her 8-year-old daughter in the courtroom; this resulted in 3 years imprisonment. This example shows the irrationality of behavior concerning revenge in relation to reality and intrapersonal experiences. Marianne did not get her child back, but her psychological balance might have been partially restored, that is, the death of the murderer of her child was compensation for her loss.
This article presents a psychological analysis of the phenomenon of revenge and differentiates between reality (the unchangeable past) and the intrapersonal experience (the restored psychological balance) with regard to the reason why people take revenge. This is a different approach than the one undertaken by Jon Elster (1990), who addressed the individual rationality of revenge behavior (the suffering cannot be undone, worrying takes time and energy, and there is a risk of counter-revenge).
In Western societies, revenge is considered taboo; taking revenge is thought to be childish and unethical and the responsibility of the constitutional state only. Nevertheless, we seem to feel ambivalent about revenge. Those who do not avenge (and perhaps also forgive) are seen as weak or cowardly. Some border of acceptability is probably given by the severity of the act of revenge.
Reports of homicide, sometimes followed by suicide, and mass murder or terrorism regularly appear in newspapers and on television. Although revenge seems to be part of human nature, it can have a dangerous side. Nevertheless, few studies have examined its psychological underpinnings and there is no generally accepted definition of revenge. What is revenge, psychological speaking? Could revenge be part of healthy functioning? If so, is it possible to distinguish between “healthy” and “pathological” revenge? Is there a connection between revenge and psychological or psychiatric disorders?
The aim of this study is to present an overview of the psychological understanding of revenge and provide more insights into how to cope with it. A contribution is made regarding the definition of revenge/revengefulness to further an empirical approach toward these phenomena and, hopefully, to contribute to the theory and diagnostics of revenge for clinical practice.
This review does not include the neurobiological literature, for example, the role of striatum activation (seen in positron emission tomography (PET) imaging) when human volunteers play a game designed to elicit revengeful acts (de Quervain et al., 2004; Knutson, 2004). Also, social and cultural influences (such as honor killing) are not taken into consideration. This article examines revenge from an individual psychological perspective.
Method
A literature search was conducted using the electronic databases PsycINFO, ERIC, PubMed, Web of Science, Google Scholar, and Scopus, without any limitation regarding date of publication. The keywords “revenge,” “vindictiveness’” and “vengeance” were used together with “motivation,” “psychopathology,” “emotions,” or “personality,” either individually or in combination.
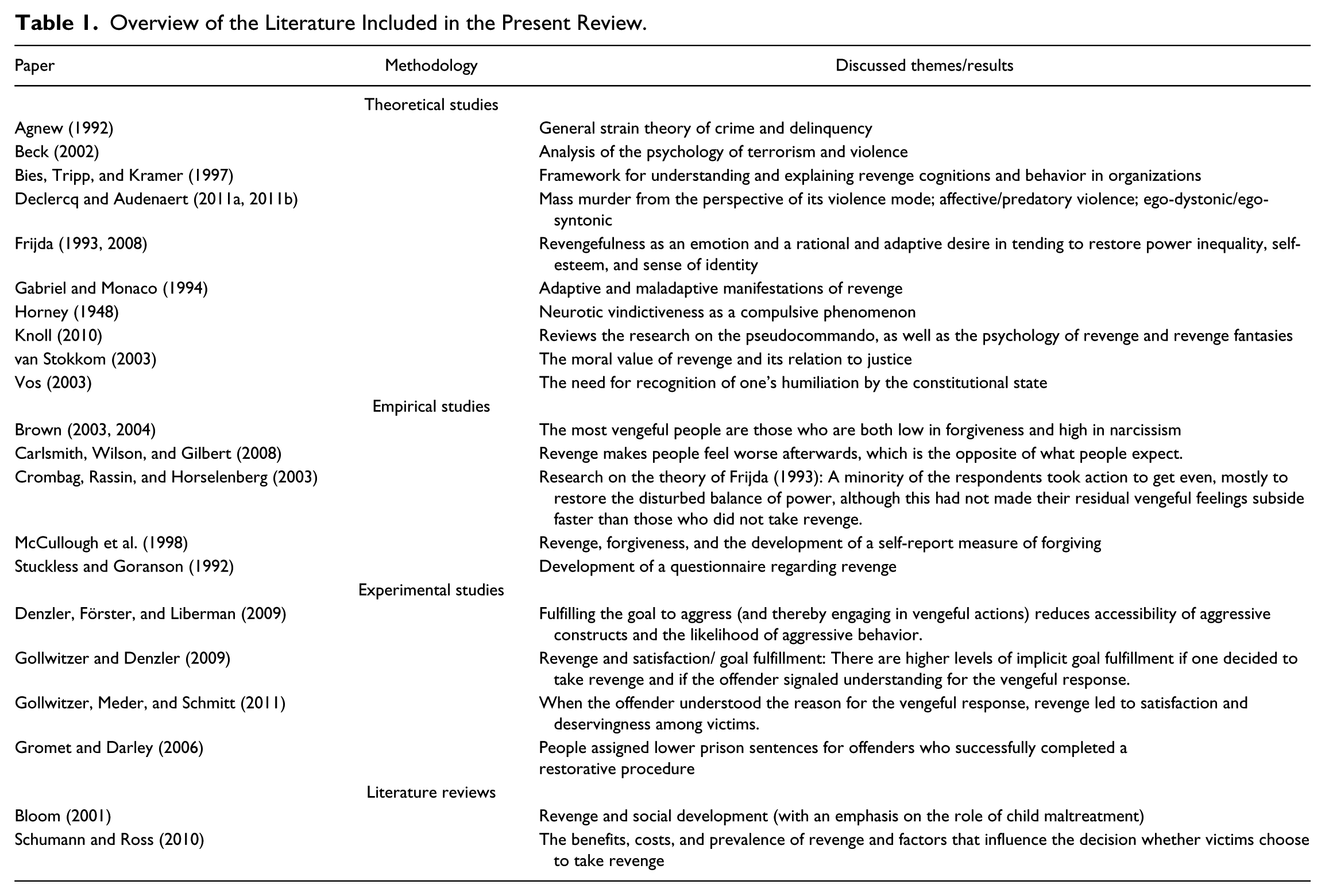
The inclusion criteria were published in the English or Dutch language: a theoretical study, literature review, empirical study, experimental study, or case study on the topic revenge. Revenge had to be the central theme of the article. After a search applying these criteria, 165 articles were selected; these articles were then judged on their relevance for the current research questions. The selected studies are summarized in Table 1.
Overview of the Literature Included in the Present Review.
Theories About Revenge
Definitions of Revenge
Theoretically, revenge can be conceptualized as behavior that follows revengefulness. A differentiation between revenge and retaliation is seldom made (Table 2 presents a brief description of terms used). Vos (2003) described retaliation as regulated revenge. The form of the response is of interest, as in “no more than one eye for an eye, no more than one tooth for a tooth,” as opposed to revenge, which is about the content and the subjective satisfaction. Retaliation has the purpose to discourage the adversary and involves a fast and rational response (Stuckless & Goranson, 1992). In case of revenge, the avenger wants to eliminate an uncomfortable, painful emotion. Revenge is intense and long-term in nature, because it often takes place after the person has ruminated about his or her suffering and his or her offender. The term “punishment” is also used in scientific articles about revenge (see, for example, Carlsmith, Wilson, & Gilbert, 2008). Despite their differences, the distinction between the terms punishment, revenge, retaliation, and retribution is often ignored, except by philosophers (e.g., Zaibert, 2006).
Brief Description of the Terms Used in Various Publications.

Furthermore, revenge is commonly associated with emotions such as aggression, anger, and hate. However, getting outraged will not restore the disturbed psychological balance after an injury.
According to van Stokkom (2003), revenge concerning anger has to be distinguished from revenge concerning hatred. Regarding anger, revenge is outward-facing and the person who is experiencing the revengefulness is sensitive to proportionality. This is unlike revenge connected to hatred, which is more obsessive and inward-facing. People who hate do not show empathy, and because of their obsessive character, they do not have to feel or experience their vulnerability.
Psychoanalysis refers to a relation with loss of gratification and to the function to disguise repressed feelings of helplessness and emptiness. Horney (1948) published an article titled “The Value of Vindictiveness” in which she distinguished between vindictiveness arising from rational anger (proportional to the provocation) and vindictiveness arising from neuroticism, which is compulsive and can become a character trait. Horney stated that revenge can amount to “a way of life” with a drive to humiliate, frustrate, or exploit the other without any room for reason or logic. Due to this, isolation and egocentrism prosper. Patients will not be motivated to receive treatment, which makes revenge difficult to treat. Superficially, revenge offers too much: defense, self-respect, and a sense of identity.
Vos (2003) divided the desire for revenge into four elements: humiliation (damage to self-esteem), the belief that the damage to self-esteem is incorrect, the drive for restoration of equality of power, and the desire to cause harm, including the risk of excessiveness and the desire to elevate oneself morally above the other.
Frijda (2008) suggested that society should not deny or condemn the desire for revenge and mentions several benefits of revenge: deterrence from future harm doing (so that interests of the avenger will be protected), the desire to settle an account, the repair of loss or lack of power, the restoration of pride, and the escape from shame or pain. Frijda (2008) stated that the desire for revenge has all the usual characteristics of a very powerful emotion. He describes it as a condition of impulse, which is generated by an appraisal and accompanied by physical excitement, preoccupation, and fixation on the pursuit of one goal. However, perhaps the idea of revengefulness as a pursuit, rather than an emotion or feeling, is a more useful approach. Whether the purpose is actually going to be achieved is irrelevant, revengefulness is intrapersonal and independent of reality. This pursuit to restore the psychological balance accompanies feelings (which are under the influence of cognitions) as well as basic emotions, such as aggression.
Origin of Revenge
Robert Agnew’s General Strain Theory (1992) stated that strains (disliked events and conditions, for example, the sense of perceived injustice) lead to negative emotions such as anger, frustration, and resentment, thereby providing pressure for corrective action, for example, criminal acting out. Crime can be used to reduce or escape from the strain, temper negative emotions (e.g., through the use of illegal drugs), or seek revenge against the source of the strain. Bies, Tripp, and Kramer (1997) developed a similar theory; after a provoking stimulus (e.g., abuse), people tend to ruminate about the event and determine the responsibility of the offender. Whether people get angry and have revengeful fantasies or behavior depends on this appraisal. According to the attribution theory (Heider, 1958), blame for negative circumstances can either be internally or externally attributed. Thus, aggressive impulses are either directed outward or inward, which can even result in homicide or suicide or self-destructive behavior such as self-mutilation and risky behavior (Bloom, 2001; Horowitz, 2007).
In a letter to Einstein, who asked him a question about the reason behind war, Freud replied that human beings are endowed by nature with hostile and violent feelings that start to build up over time, leading to a grand catharsis (i.e., war; Beck, 2002). After this catharsis, equilibrium is restored. The second assertion is that the enemy we see is a reflected image of our inner nature; our denied aggressive impulses are projected onto the enemy.
In contrast to this psychoanalytic model, Beck (2002) proposed a cognitive model about the roots of all forms of violence:
When we perceive ourselves or our group as threatened . . . our internal representation of ourselves is usually of goodness and that of other people with whom we are in conflict of badness . . . We are disposed at the times to see ourselves as the victims victimized by others . . . Over time our view of the other person or group progresses from opponent to antagonist to Enemy. We see the Enemy as dangerous, needing to be isolated, punished, or eliminated. We may seek revenge for the damage that we believe we have sustained or we may make a pre-emptive strike to forestall damage. The target of the violence is generally portrayed as the aggressor, as the victimizer. (p. 212)
Cognitive distortions, he added, like overgeneralization, dichotomous thinking, and tunnel vision, contribute to the threatening image of the other.
The desire for revenge and justice may be directed at the original perpetrator of the offense act or may be displaced onto others, often those entirely innocent of the initial injury. So when the original perpetrator is not the target of the revenge, the satisfaction that revenge can give is a sense of dominance over the original perpetrator through the mechanism of displacement (Bloom, 2001).
According to Declercq and Audenaert (2011b), revenge is one of the most recurrent motives for mass murder (murder is considered as mass murder in case of three or more victims; Meloy & Felthous, 2004). Mass murderers see themselves as victims of an unjust world, in the terminology of Knoll (2010), they are called “collectors of injustice.” They retreat into a fantasy life of violence and revenge. These fantasies serve the functions to provide sadistic gratification, to obliterate an intolerable reality and aversive self-awareness, to restore the grandiose self, and to maintain the image of others and the world as evil and dangerous. Ultimately, these fantasies enable them to commit mass murder-suicide. Declercq and Audenaert (2011a, 2011b) called such revenge fantasies, which center on authority and omnipotence and in which people identity themselves with violent characters, ego-syntonic. These fantasies are assumed to emotionally supply the subject’s pathological narcissism, in contrast with ruminations that are ego-dystonic and compulsive. These ruminations impose themselves on the offender’s mind like intrusions and recurrent recollections (e.g., after traumatization) rather than being evoked by them. In this case, the goal of the violence is relief after an unendurable tension because of the repeated intrusions of revenge.
As a part of everyday life, revenge will restore the psychological balance that has been disturbed earlier; it is a normal phenomenon with a protective function by maintaining self-esteem or being beneficial in the grieving process. Gabriel and Monaco (1994) called this “adaptive revenge.” In this case, revenge is not destructive, enables acceptance and redefinition, encourages progression and ego stability, and disappears over time. Destruction, such as homicide, is at the other end of the continuum and is described by Gabriel and Monaco as “maladaptive revenge.” According to Draijer (2000), those pathological forms of revenge, which lead to, for example, homicide, are part of a psychological disorder, often a borderline or narcissistic personality disorder. Early problems in development (e.g., traumas, hostility, or “being ignored”) carry a great deal of weight in such cases.
Summary
To summarize, revenge should be distinguished from concepts such as retaliation and punishment, just as revengefulness should be distinguished from emotions such as hate or anger. Instead, we consider revengefulness as a pursuit. It develops after a certain strain, is intrapersonal because of its cognitive, introverted nature, can be directed inward (toward oneself) or outward (toward the other), and can substantially increase over time. Cognitive distortions contribute to the threatening image of the other, who needs to be avenged or eliminated. This can even lead to the point of homicide and mass murder. This depends on the personality of the avenger and the function the revenge fantasies and ruminations have. As noted, revenge is a normal phenomenon with a protective function. When the fantasies function to disguise repressed feeling of emptiness and loss, or to restore the grandiose self, these revenge feelings are ego-syntonic. When revenge has the function to offer relief, the fantasies are ego-dystonic. Both ego-syntonic and ego-dystonic feelings can lead to acts of violence, albeit with different purposes.
Thus, due to the variety of emotions, feelings and personality traits involved, there are individual differences in intensity and functionality when people are striving for revenge. With the aim to learn more about which factors are most important in differentiating between a healthy and pathological way of dealing with revenge, and under which circumstances the processes operate and can lead to acts of violence, we now examine the experimental and empirical research on revenge.
Experimental and Empirical Studies
Some decades ago, the idea of “revenge as a disease” found support among psychotherapists as they began to show interest in research on forgiveness (McCullough, Kurzban, & Tabak, 2011). However, failing to forgive does not necessarily mean seeking revenge, just as the absence of seeking revenge does not equal the presence of forgiveness (Brown, 2003, 2004).
Subsequently, Brown (2004) searched for a defining factor and included “narcissism” as a personality variable in his investigation, given the grandiose belief in oneself and the feeling that the world is in service of their needs. Questionnaires were filled out by 248 students. The degree of narcissism was measured by the Narcissistic Personality Inventory (NPI; Raskin & Hall, 1979; Raskin & Terry, 1988) and the degree of vengeance-seeking tendencies with the Vengeance Scale (Stuckless & Goranson, 1992). The tendency to forgive and the global feelings of healthy, non-narcissistic self-worth were also measured by questionnaires. The scores from these questionnaires were compared with each other. The results showed that the degree of narcissism could make a successful distinction between vengeful and non-vengeful people among individuals who were low in dispositional forgiveness. Narcissism was unrelated to vengeance among individuals with a high degree of forgiveness. The most vengeful people were those who had a low degree of forgiveness and were high in narcissism, independent of gender and healthy self-esteem.
In experimental social research, attention is mainly focused on the positive or negative consequences for the avenger but does not include his or her possible psychopathology. According to Carlsmith et al. (2008), people expect to feel better when they take revenge. In reality, they feel worse and ruminate more about the offender because people underestimate the affective consequences of the responsibility for harming another person. An important factor is, however, whether the other person shows understanding of the vengeful response, because this offers the victim more satisfaction (Gollwitzer & Denzler, 2009; Gollwitzer, Meder, & Schmitt, 2011). Besides this understanding, the recognition for one’s pain the victim receives might also be an explanation for the improvement of feelings among victims. In one study, when offenders successfully completed a restorative justice program (usually a face-to-face meeting with the victim) as compared with a traditional court procedure, the participants of that study assigned lower sentences to the offenders (Gromet & Darley, 2006). It should be mentioned, however, that the participants read the court cases with the assignment to think about how to treat the offender, so the participants were not the victims themselves.
Obviously, the conceptualism of revenge influences the design of experimental social research. Furthermore, ethical concerns impose restrictions. In this type of research (Carlsmith et al., 2008; Denzler, Förster, & Liberman, 2009; Gollwitzer & Denzler, 2009; Gollwitzer et al., 2011), the injury is about something we do not get instead of something that is being taken away. Subsequently, there is also a difference in abstraction. Taking away someone’s dignity by rape or humiliation is less concrete than taking away a small amount of offered money, which falls under retaliation instead of revenge.
To avoid the artificiality of the generative feelings of revenge, one can ask questions about a revenge taken in the past, as in retrospective research. Empirical research by Crombag, Rassin, and Horselenberg (2003) showed that most people do not actually take revenge but merely have thoughts, feelings, and fantasies about it (see also Crombag, 2003). Most people become reconciled with the offender and many people decide to let bygones be bygones. Some of the people who did take revenge could not explain their reason for doing so. Crombag et al. offered an explanation for this by stating that revenge is impulsive, and whether rationalization afterwards (when they retrospectively consider an acceptable explanation for their behavior when forced to think about it) leads to an acceptable explanation or not. A different explanation might be that people may process their injury and integrate the feelings of pain and hurt that were initially more external in expression. Revenge can be influenced by, for example, fear of counter-revenge or getting fired. Thus, rather than an automatic response to injustice, many victims analyze the relative cost and benefits of taking revenge and compare this with other methods of coping with their injury (Schumann & Ross, 2010). It should be noted that, in the study of Crombag et al., the group of people who took revenge even after a period of time still struggled with more vengeful feelings than the people who did not take revenge. Although 58% experienced satisfaction and 16% experienced triumph, only 19% reported their vengeful feelings to be completely gone, compared with 40% of the people who did not take revenge (Crombag et al., 2003).
In summary, experimental and empirical research shows that most people decide not to take revenge. However, even after a period of time, those who did take revenge continued to struggle with vengeful feelings. The degree of narcissism could offer an explanation for the stability over time, because this distinguishes vengeful from non-vengeful people who are low in dispositional forgiveness. In that case, the level of satisfaction, related to the understanding of the original perpetrator for the vengeful response, could also be translated to the acquisition of respect and gratification of feelings of grandiosity.
Clinical Measurement
Few scales are available that measure feelings, fantasies, or thoughts about revenge. The “Vengeance Scale” measures attitudes toward revenge (Stuckless & Goranson, 1992). High scores on items such as “Revenge is sweet” and “I live by the motto ‘Let bygones be bygones’” (reverse coded) indicate a positive attitude toward revenge, but the questionnaire does not assess revengeful behavior or fantasies. The Transgression-Related Motivations Inventory (TRIM; McCullough et al., 1998) measures the underlying motivation to forgive and includes revenge as a subscale. The subscale Revenge (R; the motivation to take revenge) and Avoidance (A; the motivation to avoid the harmdoer) both consist of several items to investigate the current thoughts and feelings after a recent and specific offense, albeit at a basic level: for example, “I’ll make him/her pay” (R) or “I withdraw from him/her” (A).
As shown in the above-mentioned studies, revenge and its associated emotions are not easy to translate to a laboratory setting in a practical and ethically acceptable way, which affects the ecological validity. To provide a more practical elaboration, to identify certain factors described above, and to clarify what to look out for in contacts with patients and in treatment, two examples of actual mass murders are discussed below.
Clinical Illustrations
Anders Breivik
Breivik is the perpetrator of attacks in Norway in 2011 during which he bombed government buildings in Olso and then carried out a mass shooting at a camp of the Workers’ Youth League of the Labor Party on the island Utøya. Seventy-seven people were killed and 319 others injured, most of them teenagers. On the day of the attack, Breivik distributed electronically a 1518-page manifesto in which he elaborates his worldview. In sum, it regards Islam and Marxism as the enemies of Europe and provides a reformation plan comprising several violent attacks.
Breivik claimed that the purpose of the attacks in Oslo and on the island was to save Norway and Western Europe from a Muslim takeover, adding that he had acted in self-defense and bore no guilt. The first team of psychiatrists to examine him diagnosed Breivik with paranoid schizophrenia and stated that he was psychotic during the attacks. The second psychiatric evaluation concluded that Breivik was sane, but with a narcissistic personality disorder. Ultimately, the Oslo District Court found Breivik sane and convicted him of mass murder and terrorism.
Breivik’s strain contained, in his eyes, the belief in an Islamic takeover of Western Europe, which led to intense and long-term anger, hate, and aggression. Pressure for action built up, revengefulness substantially increased over time, and with a great deal of rumination, as elaborated in his manifesto. He blamed political parties that support multiculturalism and attacked the Labour party for letting Norway down. He himself, Norway, and all of Western Europe are the victims, victimized by the Muslims, who are the Enemy, are dangerous, and need to be eliminated. There were no more differentiations, no more proportionality. The plan gave him a sense of identity, he considered himself to be the rescuer of Norway, the Norwegian people, and the rest of Western Europe. Therefore, he did not plead guilty. His fantasies were ego-syntonic and fit his narcissistic personality: He saved Europe from a dangerous enemy takeover, thereby aiming to achieve narcissistic gratification.
The Columbine Shooters
Eric Harris and Dylan Klebold were American high school seniors who murdered their classmates and teacher at the Columbine High School. In total, they killed 13 people and injured 23 others, after which they committed suicide. Later, it became clear that Columbine was intended to be a massive bombing after which Harris and Klebold planned to shoot the fleeing survivors but the bombs did not go off (Cullen, 2004). According to Fuselier and Ochberg, Harris and Klebold were different individuals with different motives and opposite mental conditions (Cullen, 2004). Where Klebold was hotheaded, depressed, suicidal, and self-blaming, Harris was cold, calculated, and homicidal. He wanted to rape girls, mutilate people, and had feelings of grandiosity, writing, for example, in the yearbook of his friends: “Ich bin Gott” (German for “I am God”). This is most likely the aspiration to be recognized as superior rather than a delusion of grandeur because he also wrote, “I feel like God and I wish I was, having everyone being OFFICIALLY lower than me” (Langman, 2009). Instead of merely hate, Fuselier and Ochberg recognize contempt in the journals Harris and Klebold kept and in the videos they made (Cullen, 2004). Hare describes a messianic-grade superiority complex in which a person is out to punish the entire human race for its appalling inferiority. Instead of just hate, it is more about demeaning people, Hare explains (Cullen, 2004). Because of the combination of narcissism, sadism, lack of remorse or empathy, deceitfulness, and rejection of morality and law, it was concluded that Harris was a psychopath (Cullen, 2004; Langman, 2009). Klebold appeared to have had a schizotypal personality disorder; he had social difficulties, odd behavior and appearance, and general “goofiness.” He misused language, created neologisms, and distorted actual words into words that do not exist. He was alienated (e.g., he wrote, “Being made a human without the possibility of BEING human”), viewed himself as a God-like being, and exhibited paranoia (Langman, 2009).
The strains of Harris and Klebold include rejection by peers, and their contempt and disgust with the people around them. As with Breivik, their emotions were long-term and intense, feelings of revenge prospered over time with a great deal of rumination without any fine-tuning. Harris, who wanted to hurt people, directed his aggressive impulses outward. His narcissistic grandiose view of himself, together with the lack of respect he experienced: A quote of Harris, after picking up a shotgun and making a shooting noise, is, “Isn’t it fun to get the respect that we’re going to deserve?” (Gibbs & Roche, 1999) provided pressure for violent acts. He identified himself with violence and liked to call himself “Reb,” short for rebel (Gibbs & Roche, 1999). Because they thought that the world would be interested to understand their act, they put their story on tape. Similar to Breivik, their act of revenge gave them a sense of identity: They wanted to create something so devastating that the world would never forget them. Survivors would have flashbacks for the rest of their lives, and they believed that directors would want to film their story (Gibbs & Roche, 1999). The fantasies seem to be ego-syntonic in the case of Harris; they centered on omnipotence, weaponry, and violence, and the act of mass murder provided him narcissistic gratification. In the case of Klebold, this is less clear. He had fantasies that were also centered on grandiosity, but possibly, within the context of grandiose delusions. In contrast with Harris, Klebold was hurting inside and wrote about his social difficulties in his diary (“Nobody accepting me even though I want to be accepted; me doing badly and being intimidated in any and all sports; me looking weird and acting shy—BIG problem”) and told his parents as a goodbye, “I didn’t like life very much. Just know I’m going to a better place than here” (Gibbs & Roche, 1999). It seems that the fantasies about the mass murder had the function to obliterate aversive self-awareness and provided a sense of identity. Ultimately, he dealt with his internal stressors (although recruited by Harris) by acting out, expressing in physical pain what he could not stand to feel emotionally.
Discussion
Revenge goes beyond anger or retaliation and involves more than a continuum of reciprocity. Keeping order or avoiding an offender to avert further harm is not revenge. The damage to self-esteem makes revenge more abstract and emotional than retaliation. Examination of the literature reveals multiple descriptions of revenge: as an emotion (Frijda, 1993, 2008), as a possible way to get back at the source of the strain (Agnew, 1992), as adaptive or maladaptive (Gabriel & Monaco, 1994), as a matter of personality, which can make it normal or pathological (Draijer, 2000), and, due to developmental problems (Bloom, 2001; Draijer, 2000). Acting on it can be satisfying or not (depending on, among other things, the offender’s understanding of the vengeful response; Gollwitzer & Denzler, 2009; Gollwitzer et al., 2011).
There is a time span between the victimization and the act of revenge against the offender, with the opportunity to ruminate and fantasize (Frijda, 2008; Stuckless & Goranson, 1992), which can be ego-syntonic or ego-dystonic (Declercq & Audenaert, 2011a, 2011b), and can even result in suicide, homicide, or mass murder (Bloom, 2001; Declercq & Audenaert, 2011a, 2011b; Horowitz, 2007; Knoll, 2010). However, the desire for revenge or the actual acting on this desire is correlated with, for example, the perception and understanding of the situation, the fear of counter-revenge, or fear of getting fired. Many victims analyze the relative cost and benefits of taking revenge and compare this with other methods of coping with their injury (Schumann & Ross, 2010), remindful of Agnew’s (1992) assertion that not all people respond with crime in the case of strain, because people have different cognitive (e.g., denial), emotional (e.g., drug use or expressing one’s emotions through art), and behavioral (e.g., seeking revenge) coping strategies, and several factors can facilitate coping, such as social support.
This article began with questions about the psychological meaning of revenge. Could revenge be part of healthy functioning? And, if so, is it possible to distinguish between “healthy” and “pathological” revenge? Is there a connection to psychological or psychiatric disorders? Our conclusion is that revenge is not pathological in itself but depends on the coping style and personality of the person. Dealing with strain, such as an injury, and with revenge feelings and cognitions has several manifestations that could be healthy or pathological, with a dimensional approach rather than a categorical one. We consider that revengefulness as a pursuit, which develops after a certain strain, is intrapersonal, because of its cognitive, introverted nature, and that it can be directed inward (toward oneself) or outward (toward the other) and can substantially increase over time. Cognitive distortions contribute to the threatening image of “the other,” who needs to be avenged or eliminated. This can even lead to homicide and mass murder. This is dependent on the personality of the avenger and the function the revenge fantasies and ruminations have.
Early problems in development can help to explain the rising emotions, feelings, and their relation with the sense of self. In case of a normally developed sense of self, setbacks may lead to gloominess, sadness, and withdrawal from social contact. In the presence of fantasies about grandiosity, setbacks lead to a narcissistic injury, resulting in aggression. Development of the ego-ideal, at an adequate distance from the self, fails in the case of a disturbed relationship with the parent. The child withdraws from the parent and from a desirable ideal. Hence, the child cannot invest in the construction of the ego-ideal. The energy flows back to the self, which leads to a fusion between the self and the ego-ideal (the distinction maintains). To protect the self against injury, fantasies about grandiosity emerge; the self with grandiose fantasies is called, in Kohut’s (1971) term, “the grandiose self.” The person with a grandiose self believes, among other things, that he or she is entitled to special treatment. This could fit the Diagnostic and Statistical Manual of Mental Disorders (DSM) classification of “narcissistic personality disorder” (Derksen, 2007). The aggression that arises following an injury is converted to activity with the aim of realizing the fantasies about grandiosity, which can lead to destructive acts such as homicide or mass murder. The extent to which people need revenge has a certain degree of stability. Thus, revenge is an important state of mind that has the potential to be destructive to those who ruminate over it and have a certain personality type, but it cannot by itself be classified as a healthy or pathological phenomenon.
Perspectives on Treatment
The above-mentioned theories and processes have to be taken into consideration in contacts with patients and in treatment. After severe traumatization (e.g., rape), revenge feelings and cognitions are easily sympathized with. The therapist must be on guard not to gloss over them but rather to validate them. He or she must keep in mind that when revenge maintains self-esteem and restores the psychological balance, it is a healthy way of coping with injury. When the need for revenge is long-lasting and becomes dysfunctional, for example, as a part of a disorder (narcissistic personality disorder, borderline personality disorder), it could be considered a pathological way of dealing with pain and revenge. The main problem of revengeful patients is their inability to feel and bear their emotions and feelings. Draijer (2000) recommended psychodynamic treatment in which the psychotherapist presents himself as a new “actual” object, supportive and acknowledging with regard to the original experienced injury. A precondition for successful treatment is that the injuries caused by trauma, insecurity, and/or neglect have not affected the development in such a way that the projections onto other people have the nature of a delusion. This treatment will be long-term and, as Lane (1995) stated it, “The therapist must be able to endure long periods ‘without joy,’ and be able to accept the patient’s complaints of constant suffering and pain” (p. 57). Negative therapeutic reactions are not uncommon. Hull, Lane, and Okie (1989) stated that patients will act provocatively to elicit behavior from the therapist to justify their own revengeful behavior. The therapist himself can become the object of cruelty (Brenman, 1985) and will be challenged to do something for the patient to show him his support or to satisfy the patient’s need of grandiosity in the therapist. Meanwhile, there is acute sensitivity of the patient to the therapist’s shortcomings (Lane, 1995). The special challenge for the therapist is to bear the provocation, the distrust, and negative transference and to offer an accepting environment, although with clear boundaries, and teach the patient to face his own shortcomings, as well as those of the therapist and of the offender, to start the actual grieving process (Draijer, 2000).
Conclusion
Little attention is paid to revenge within clinical psychology and treatment, which depends mostly on the clinical judgment of the clinician. At present, there is no consensus among therapists as to whether feelings of revenge should be considered as a positive or negative phenomenon. Some consider that the individual should work explicitly toward forgiveness, whereas others prefer the person to express resentment and indignation (Goudswaard, 2000).
The present analysis aimed to help clarify the boundaries between a healthy and pathological way of dealing with revenge and, hopefully, has made some contribution to diagnostics, both in theory and clinical practice. Better understanding generally leads to improved assistance to those who have feelings and thoughts of revenge; this might, in turn, prevent escalations of acting out a behavior that may even reach the point of homicide, thus helping both the patient and society.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.