
Abstract
Arsonists are considered a type of violent offender by some and a distinct group of offenders by others. Assuming the latter could be beneficial to offer tailor-made psychotherapeutic treatment to these offenders. The present study investigated whether arsonists (n = 55) and violent offenders (n = 41) are differentiable regarding several demographic and personal characteristics, and criminal career. Results indicated that arsonists were significantly more often diagnosed with a Diagnostic and Statistical Manual of Mental Disorders (DSM) Axis II disorder, and more socially isolated and lacking coping skills. Violent offenders, on the other hand, demonstrated more drug abuse/dependence, a younger age at the first manifestation of antisocial behavior, a more extensive criminal history and higher percentage of recidivism. In light of these results, it is conceivable that arsonists could benefit from a slightly different treatment approach, for example, with more attention to relational and emotion regulation skills.
Introduction
According to the Federal Bureau of Investigation (2012), out of the estimated 1,375,000 fires reported in the United States in 2012 (NFPA Fire Analysis and Research, 2013) 45,926 (30%) were deliberately set. In the Netherlands, the percentage of reported fires due to firesetting is even higher. In 2012, 18.4% of the 14,400 fires in or at buildings, along with a compelling 67.4% of the 19,700 open air fires, were attributed to arson (CBS Statistics Netherlands, 2013). With an average cost of 12,796 dollar per arson, the resulting damages are considerable. Such significant financial—not to mention the concomitant immaterial—consequences call for further investigation of arsonists, with the aim of improving treatment options to prevent further damage. Even more so because arsonists are considered to be a high-risk group of offenders with recidivism rates running up to 60% (Brett, 2004).
Gannon and Pina (2010) reviewed the characteristics of firesetters and described the typical firesetter as a Caucasian, low-skilled, young male with a weak socioeconomic status and an early onset of criminal behavior. Also common were neglect, abuse, and dysfunctional attachment styles in the family situation, alongside of a limited social network, poor social skills, and low self-esteem. Furthermore, the average firesetter exhibits a high level of impulsivity, frequently combined with conduct disorder (CD)/antisocial personality disorder (PD), schizophrenia, substance abuse, and affective and/or anxiety disorders. Horley and Bowlby (2011) confirmed these characteristics in their review, but pointed out that they do not necessarily distinguish arsonists from other types of offenders. The same seems to be true for risk factors. Previous convictions, alcoholism, below average intelligence, and the presence of a mental disorder—in particular PDs—are not exclusive to arsonists (Burton, McNiel, & Binder, 2012; Dickens et al., 2009; Harris & Rice, 1996; Lindberg, Holi, Tani, & Virkkunen, 2005; Repo & Virkkunen, 1997). Where it may seem obvious that fascination with fire would differentiate firesetters from other offenders, actual pyromania (repeated arson for pleasure, gratification or relief) is rarely observed in firesetters (Gannon & Pina, 2010). Ritchie and Huff’s (1999) outcomes, for example, where only three of the 283 investigated arsonists were diagnosed with pyromania, support this.
Stickle and Blechman (2002) postulate that firesetting is an expression of grave antisocial behavior instead of a specific craving for fire. In their study, juvenile arsonists (n = 85) exhibited significantly more aggressive antisocial acts than non-firesetting offenders (n = 134). In both groups, however, the same general patterns of antisocial behavior, such as oppositional behavior (ODD) and CD, were found. According to the researchers, these findings suggest that the magnitude of aggression and antisocial behavior could distinguish firesetters from non-firesetters, at least regarding juveniles. Forehand, Wierson, Frame, and Kemptom (1991) came to a similar conclusion. They compared 36 incarcerated juvenile delinquents categorized in three groups: firesetters, non-firesetters high CD (comparable with the firesetters in terms of the number of CD symptoms), and non-firesetters low CD (displaying fewer CD symptoms than the other two groups). The juveniles’ caregivers were asked to complete the Child Behavior Checklist (CBCL; Achenbach & Edelbrock, 1983). Results showed that the firesetters and non-firesetters high CD scored similarly on the CBCL subscales Withdrawal (interpersonal ineffectiveness/skills deficit), Aggression and Delinquent (both measures of antisocial behavior), while the group with less CD symptoms differed. This led the researchers to hypothesize that committing arson is more likely to represent a more advanced stage of antisocial behavior instead of a unique syndrome.
Considering firesetting behavior as an expression of aggression and part of antisociality is not restricted to juveniles in the literature. In their review, Gannon and Pina (2010) also established a link between adult firesetters and violent offending. They noted that firesetters frequently reoffended with a violent offense and that aggression seemed to play a considerable role in the act of arson. This is not a recently developed view; in 1987, Jackson, Glass, and Hope proposed a model of recidivistic arson. This model integrated several factors associated with pathological arson, including displaced aggression aimed at attempting to change the environment.
Another indication of a connection between arson and aggression could be the reoffending of firesetters with other types of offenses than arson. For example, Rice and Harris (1996) examined recidivism in a sample of 208 adult males formerly admitted to the maximum security division of a large psychiatric institution after firesetting. Sixteen percent of the participants reoffended with arson, 57% with non-violent offenses, and 31% with a violent offense within a follow-up period of 20 years. Moreover, results showed that firesetters relapsed with violence (55 months) at a faster rate than with non-violence (83 months). This diversity of offense types within their criminal career implicates that arsonists tend to be rather generalists than specialists (Doley, Fineman, Fritzon, Dolan, & McEwan, 2011).
Accordingly, studies comparing arsonists with other types of offenders found resemblances between these groups. Jackson et al. (1987) compared 36 male patients from a maximum security hospital, half of them admitted for committing arson and the other half for interpersonal violence. Results did not differentiate the two groups in terms of several demographic variables (such as age) and other characteristics like IQ and mental health. More recently, Enayati, Grann, Lubbe, and Fazel (2008) showed that 214 arsonists did not significantly differ from 2,395 other types of offenders on most Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association [APA], 1994) diagnoses, except for learning disabilities and Asperger’s syndrome (which were more common in the arsonist sample). Labree, Nijman, van Marle, and Rossin (2010) also found few differences in terms of psychopathology between 25 arsonists and a control group of 50 sexual and homicide offenders.
Other studies, however, do report differences between arsonists and violent offenders. For instance, Räsänen, Hakko, and Väisänen (1995) compared arsonists with homicide offenders and found the former to be more often single, lower educated, showing a less stable employment record, and previous psychiatric admissions. In addition, arsonists displayed significantly more alcohol abuse problems, 84% as opposed to 62% in the homicide offender sample. Gannon et al. (2013) compared matched groups of 68 imprisoned adult firesetters and non-firesetters. Firesetters not only distinguished themselves with respect to fire-related characteristics (such as identification with fire) but also regarding emotional/self-regulation characteristics (e.g., lower levels of general self-esteem). Social competence, proneness to boredom, impression management, and offense-supportive attitude measures, however, did not discriminate between the two groups. Hagenauw, Karsten, Akkerman-Bouwsema, De Jager, and Lancel (2015), on the other hand, also found differences. The 14 arsonists in their sample of 73 patients committed in a forensic psychiatric hospital (FPH) demonstrated poorer social and relational skills. Moreover, results showed that the arsonists displayed more behavioral problems before the age of 12, longer treatment history, higher prevalence of psychosis, and higher rates of hostility, passive-aggressiveness, and irritability. Hagenauw et al. suggested that the lack of social and relational skills is particularly suited to address in psychotherapeutic treatment aimed at reducing recidivism risk. Following the Need principle of the Risk-Need-Responsivity model (Andrews & Bonta, 1998), it is expected that treating dynamic risk factors (also called criminogenic factors) will considerably decrease recidivism risk.
Ducat, McEwan, and Ogloff (2013) compared non-firesetters, exclusive firesetters (no other types of offenses except firesetting), and mixed firesetters (firesetting and more than three other types of offenses) and found that the firesetters were more regularly unemployed than the non-firesetters, had shown more behavioral problems in childhood and suicidal ideation, and had a history of psychiatric or psychological treatment and Axis I and II disorder diagnoses. Resuming, Ducat et al. assumed firesetting to be associated with greater levels of criminogenic need compared with the non-firesetting offenses, because of the versatility of offense type in the firesetters’ criminal history. This could indicate that firesetters do not present different criminogenic needs per se but, stringing along with Stickle and Blechman’s proposition, rather the magnitude of aggression, antisocial behavior and other psychopathology distinguishes them from other offenders. Translating this into possible implications for psychotherapeutic treatment, it could be beneficial to adjust treatment intensity (e.g., the frequency of sessions and treatment duration) rather than content.
To further examine the potential need for distinct treatment approaches, the present study compared a group of Dutch forensic outpatient arsonists with their violent peers. The investigated characteristics included risk factors found in previous studies (e.g., previous convictions, substance abuse, mental disorders, social network) and recidivism rates. It was expected that the two groups would emerge more similar than different concerning the studied variables, except for the arsonists possibly displaying a greater magnitude of psychopathology.
Method
Participants
The research group of this retrospective cross-sectional study was composed of De Waag clients. As forensic outpatient treatment center in the Netherlands, De Waag offers several outpatient therapies to juveniles (12-18 years) and adults with criminal tendencies. Cognitive-behavioral treatment is offered in a group or individually, as well as pharmaceutical, relation, and systemic therapy. Therapy is mainly focused on learning to identify and avoid risk situations, and building a prosocial way of life. Acute psychosis and severe addiction are general exclusion criteria, which need to be addressed prior to admittance to De Waag. For this study, participants accepted for treatment at De Waag between 1992 and 2003 were selected from the client registration system. Inclusion criterion was the reason for admittance for treatment, with the type of offense being convicted arson or (domestic) violence. Due to a limited number of available cases, almost all of the obtainable arsonists were included (provided that file information was sufficient), except for women and participants with a violent offense in their criminal history. Because of the larger scope of the violent offender group, the included participants were randomly selected using Statistical Product and Service Solutions (SPSS; 2009).
Arsonist Sample
The arsonist sample consisted of 55 males. The main part of the group (89.1%) was born in the Netherlands, and the remaining six were born in Surinam, Morocco, Canada, or Indonesia. The mean age of the arsonists at the time of their admission was 29.3 (SD = 9.89; range = 18-58 years). The highest level of completed education was elementary school for 34.5% of the participants, middle school for 27.3%, high school for 30.9%, and college/university for 3.6%. Almost half of the arsonists were unemployed (45.3%). The mean treatment duration had been 352 days (SD = 267.92; range = 45-1,264 days).
Violent Offender Sample
The sample of violent offenders contained 41 males. Preceding, two violent offenders were excluded from the sample, because of arson antecedents in their criminal history. Similar to the arsonists, most violent offenders were born in the Netherlands (82.5%), and the remaining seven originated from Morocco, Turkey, Great Britain, and Spain. The mean age of the violent offenders was 29.3 years (SD = 8.85; range = 18-53 years). The highest level of education was elementary school for 45%, middle school for 40%, high school for 5%, and college/university for 7.5 %. For 2.5 % of the participants, the level of education was unknown. About a quarter of the sample was unemployed (25.6%). The mean treatment duration had been 423 days (SD = 403.47; range = 37-2,171 days).
Independent t tests revealed no significant differences between the two research samples regarding age at treatment admittance and treatment duration, t(94) = 0.009, p = .993 and t(94) = −1.028, p = .307, respectively. Differences between birth country, educational level, and employment were tested with chi-square analyses. Only educational levels showed significant differences between arsonists and violent offenders, χ2(1, n = 95) = 10.324, p = .035.
Measures
Following review studies such as Gannon and Pina’s (2010), a number of variables were selected considered relevant to the study of arsonists. These were collected by means of risk assessment. Operationalizations were adopted from items of several risk assessment instruments, such as the Historical Clinical Risk management-20 (HCR-20; Webster, Douglas, Eaves, & Hart, 1997), the Structured Assessment of Violence Risk in Youth (SAVRY; Borum, Bartel, & Forth, 2002), and the Level of Service Inventory–Revised (LSI-R; Andrews & Bonta, 2000). For the present study, these variables were uniformly coded 0 to 2, representing no, moderate, or high presence. Unemployment was marked “yes” if the participant was not employed for 6 months or longer. Alcohol and drug abuse/dependence and DSM Axis I disorder and DSM Axis II disorder were dichotomously (yes/no) scored according to Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; APA, 2000) criteria. In addition, the types of disorders were recorded. Cognitive impairment was marked “yes” in case of mental retardation; learning disabilities were not regarded as cognitive impairment. Participants were labeled socially isolated if they indicated an absence of social network (excluding family members or partners). Suicidal thoughts were considered present if the client had expressed any of such thoughts in present or past.
Recidivism was defined by the first new conviction for any offense (general recidivism). Following the Dutch Criminal Code, the specific offense types were categorized into arson, physical violence, domestic violence, verbal aggression, vandalism, property crime, and sexual offense. Previous convictions, that is, offenses committed prior to admittance to treatment, were categorized correspondingly. Participants were labeled a specialist if their prior and current offenses were of exclusively one type (arson or violence) and a generalist in case there were convictions concerning two or more offense type categories.
Procedure
Client files were studied to obtain information about the research variables. These files generally consist of an extensive intake, data from judicial and police reports, and reports of other (forensic) mental health care centers. During a 60-min intake session, a psychologist or psychiatrist conducts a structured interview about relevant issues to outpatient forensic care, such as family (situation), education, and work. Moreover, a clinically assessed diagnosis according to the standards of the DSM-IV-TR (APA, 2000) is derived in consultation with a multidisciplinary team (psychiatrist, psychotherapists, and psychologists).
Two psychologists with several years of experience in risk assessing carried out the risk assessments by means of the Risk Assessment Instrument for Forensic outpatients Mental Health (RAF MH; Horn, Wilpert, Eisenberg, Scholing, & Mulder, 2012). This instrument is composed of, inter alia, items of the above-mentioned risk assessment instruments. In earlier research (Horn, Wilpert, Bos, Eisenberg, & Mulder, 2009), the interrater reliability of the items of the RAF MH proved excellent (Intraclass Correlation Coefficient = .88).
To survey the criminal history and recidivism of the sample, information was requested from the judicial authorities (Judicial Documentation System [JDS]). The JDS is managed by the Central Judicial Documentation Service (CJD) and offers an overview of all (legal) persons registered for violations of the law (leading to settled as well as non-settled criminal cases). In this study, only convictions were included as offense. The follow-up time (end of treatment until reference date) varied between 34 and 221 months (M = 111.19 months; SD = 39 months).
Chi-square and Mann–Whitney tests were performed to compare the two study samples regarding the categorical and ordinal variables described under Measures, except for recidivism. Recidivism rates were calculated using Kaplan−Meier survival analysis, which takes individual differences in follow-up periods into account (Bijleveld, Mooijaart, Brouwers, & Loewenthal, 1998; Wartna, 2000). The survival analyses were performed with the dates of the first recidivism offense, and all subsequent reoffenses were excluded. Finally, the log-rank test was utilized to determine differences between the survival curves.
Results
Characteristics of Arsonists and Violent Offenders
The first aim of this study was to investigate the similarity of arsonists and violent offenders regarding several personal characteristics. In Table 1, the numbers of the participants meeting the criteria for the presence of these variables are presented.
Characteristics of Arsonists (n = 55) and Violent Offenders (n = 41) in Numbers (n) and Valid Percentages (%).
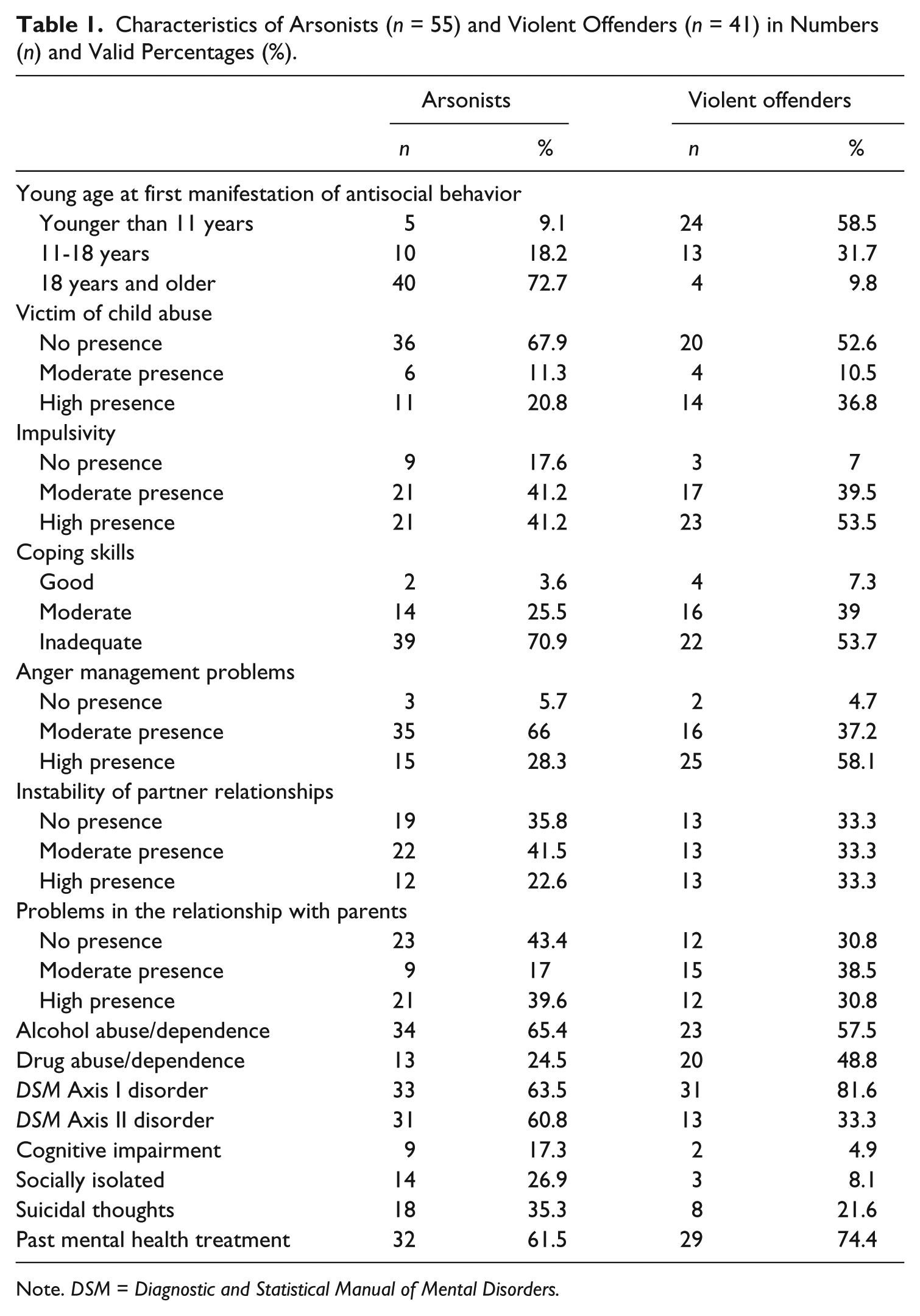
Note. DSM = Diagnostic and Statistical Manual of Mental Disorders.
Compared with the violent offenders, a significantly greater proportion of the arsonists displayed PDs, χ2(1, n = 90) = 6.665, p = .010), higher levels of social isolation (Fisher’s exact test, p = .030), and inadequate coping skills (U = 938.00, p = .040, r = −.21). The violent offenders, on the other hand, showed a higher incidence of drug abuse/dependence, χ2(1, n = 94) = 5.968, p = .015, as well as a younger age at their first manifestation of antisocial behavior (U = 332.50, p = .000, r = −.65).
Exploring the DSM Axis I and Axis II disorders further, results showed that the arsonists were mostly diagnosed with impulse control disorder (n = 18, 54.5%) and PD not otherwise specified (PD-NOS; n = 15, 68.2%), with traits of narcissism appearing most frequent (31.8%). Four participants (7.3%) were diagnosed with pyromania. The arsonists demonstrated a higher disposition to a combination of Axis I and II disorders compared with the violent offenders (26.9% vs. 19.4%, respectively), although this difference was non-significant, χ2(1, n = 88) = .655, p = .418. In the violent offender sample, the most frequently diagnosed disorders were also impulse control disorder (n = 19, 44.2%) and PD-NOS (n = 13, 76.5%), however, with antisocial traits being most prevalent (43.3%).
Criminal history and recidivism
To further compare arsonists and violent offenders, their criminal careers were studied. Table 2 shows an overview of the criminal history and recidivism by offense type for each study sample.
Criminal History and Recidivism Arsonists (n = 55) and Violent Offenders (n = 41) Based on Convictions for Several Offense Types in Numbers (n) and Percentages (S%).
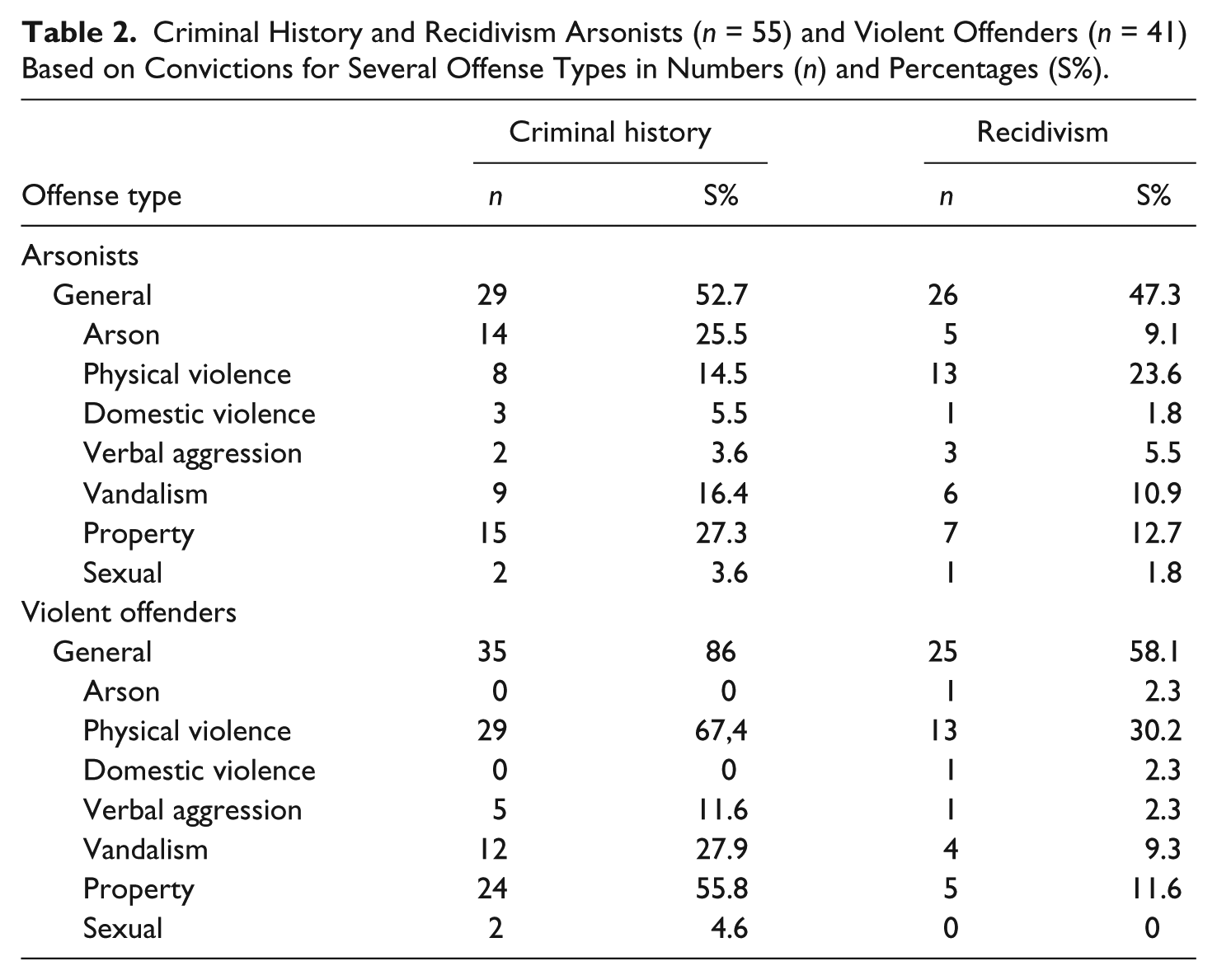
More than half of the arsonists (52.7%) had been previously convicted for one or more different types of offenses. The violent offenders surpassed this with 85.4%, resulting in a significant difference, χ2(1, n = 96) = 11.260, p = .001. The discrepancy in the number of generalists within the samples, 65.5% in the arsonists and 36.6% in the violent offenders, was also significant, χ2(1, n = 96) = 7.861, p = .005.
Figure 1 depicts the recidivism rates for general offenses during the first hundred months after treatment. Almost half of the arsonist sample (47.3%) was convicted for a new offense. Out of the five participants reoffending with arson, one was diagnosed with pyromania. The general recidivism rate for the violent offenders was 58.1%, which differed significantly from the arsonists’ reoffending: log rank, χ2(1, n = 96) = 3.864, p = .049.
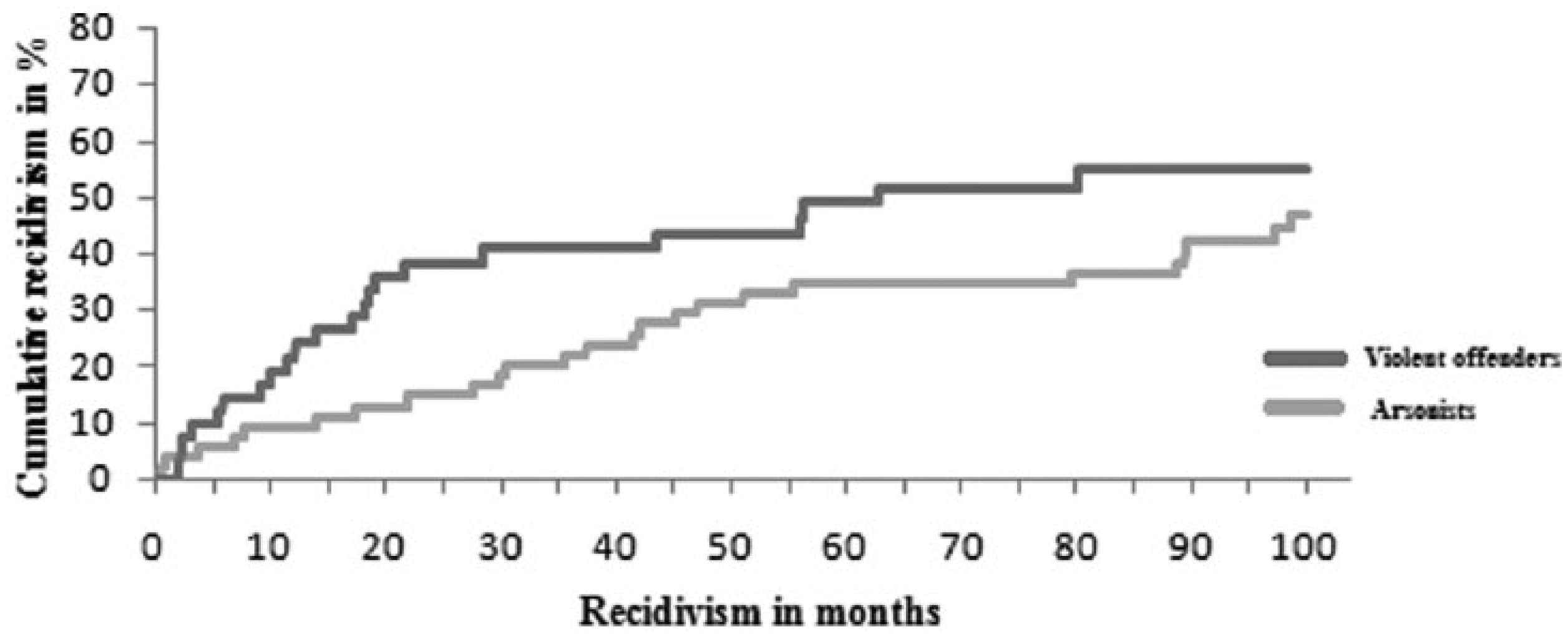
General recidivism percentages convictions arsonists (n = 55) and violent offenders (n = 41) following 100 months after treatment.
Discussion
To examine the resemblance between arsonists and violent offenders, various characteristics from client files and criminal records were compared. Based on previous literature, it was expected that the two groups of offenders would demonstrate more similarities than differences. This proved to be the case for the main part of the studied variables, however, five variables differed significantly. Arsonists displayed Axis II disorder diagnoses, social isolation, and lack of coping skills more often; whereas, violent offenders showed more drug abuse/dependency and were younger at their first manifestation of antisocial behavior. Regarding differences in criminal career, violent offenders were significantly more likely to have committed prior offenses and demonstrated a higher recidivism rate. Concerning the types of offenses, however, the expectation that the group of arsonists would contain more generalists than specialists, compared with the violent offenders, was confirmed.
In DeLisi’s (2006) study, offenders (regardless of type of offense) arrested at age 14 demonstrated a more chronic and versatile criminal career than offenders exhibiting later onset. This could explain the violent offenders surpassing the arsonists in criminal history and general recidivism in the present study. On the other hand, it seems to contradict the higher amount of specialists in the violent offender sample, especially because in Ducat et al.’s (2013) study, the generalists showed a more extensive criminal history. This considerable amount of prior offenses combined with a high prevalence of PDs led the researchers to suggest that the generalists could be more antisocial and therefore might benefit from more intensive treatment. This does not apply to the arsonists in the present study, however, where the violent offenders displayed antisocial behavior more often. Perhaps these antisocial tendencies could account for the extensive criminal careers of the violent offender sample. In this regard, the expectation that arsonists would show a greater magnitude of psychopathology was partially confirmed, by reason of the significantly higher prevalence of DSM Axis II diagnoses in their group. The DSM Axis II differences between the two samples did not become evident in the diagnosed disorders, however, but in the traits. Assuming firesetting results from antisocial tendencies, it could be expected that arsonists would be more frequently diagnosed with antisocial traits, but this was not confirmed. The arsonist sample being more socially isolated and lacking in coping skills, however, was in line with expectations and corresponded with Hagenauw et al.’s (2015) finding of poorer relational and social skills in arsonists.
Limitations and Suggestions for Future Research
The generalizability of the research sample can be considered binary. As studies investigating residential populations predominate the literature, results are harder to compare with previous outcomes. However, the outpatient character of De Waag clients draws the study participants closer to the “normal” population, compared with patients in residential facilities. Outpatients are a group of great importance, because they live in society and have more opportunities to reoffend and claim victims. It seems useful to conduct more research with outpatients to gain more insight into this relatively underexposed group.
Another issue worth addressing is the perhaps seemingly arbitrary assigning of participants to the research samples in this study. The categorizing of offender types itself is a rather precarious operation. In the present study, the choice as to make reason for admittance decisive was born out of necessity. Upon registration, there is little to no information about the criminal history of the participants, almost automatically establishing an offender type based on the referral target, that is, the type of offense. For study purposes, classified information was formally requested from the CJD. Subsequently, looking at the criminal histories of the participants diffuses categorizing offenders (except of course when they are first offender). A possible solution to this could be investigating first offenders exclusively, which could also prevent the possible bias resulting from the inclusion of generalists. The disadvantage, however, would be the inability to survey the development of criminal behavior.
The retrospective nature of the research brings indisputable limitations, because the acquisition of information is restricted to the completeness and quality of client files. Future research could benefit from a prospective approach, in which client interviews and/or self-report questionnaires could be utilized to reduce missing values in relevant information and increase the reliability of research results. Consequently, creating the opportunity to gather a specific set of variables potentially being more relevant to the topic. For example, it could be valuable to include instruments such as The Five Factor Fire Scale (Ó Ciardha et al., 2015) to see whether arsonists distinguish themselves from other offenders regarding fire-related variables such as serious fire interest, identification with fire, and perceived fire awareness, as Gannon et al. (2013) did. A further advantage of a prospective set up could be the possibility to assemble larger research groups, inter alia to be able to investigate specific recidivism (instead of only general) and explore predictors of recidivism to get a clearer picture of criminogenic needs. Moreover, it could be interesting to compare pyromaniacs with arsonists and other types of offenders to search for potential treatment needs. A larger research sample could also create the opportunity to match participants on possibly confounding characteristics, as Gannon et al. accomplished with variables such as number of total offenses, previous engagement with mental health services, and severity of index offense. Furthermore, it could be informative to compare juvenile and adult firesetters to explore whether age is connected to patterns of characteristics leading to firesetting.
Practical Implications
Contrary to expectations, the results of this study do provide some evidence for a slightly different approach for psychotherapeutic treatment of arsonists. Given their presumed enhanced social isolation and lack of coping skills, arsonists might benefit from more attention to relational and emotion regulation skills. Moreover, the outcome of predominating narcissistic PD traits could promote a therapy style taking into account the client’s vulnerabilities and need for acknowledgment (Links & Prakash, 2014).
The question whether arsonists would benefit from more intensive treatment, with, for example, more frequent sessions and longer treatment duration, needs more exploration. It could be assumed that the nature of generalists calls for a more multifaceted approach (targeting multiple areas such as social network and other environmental factors as well as personality), as suggested for generalist adolescent sexual offenders (Pullman & Seto, 2012). However, the outcome of arsonists proving to be more generalists is not very remarkable, as the literature shows generality to be typical and specialization rather exceptional (Brame, Mulvey, Piquero, & Schubert, 2014). Gannon et al. (2013), on the other hand, found enough significant differences to label arsonists specialists, which would advocate specific treatment as opposed to a more general approach.
Either way, the outcome of this study does not support assuming arsonists require less formal supervision and treatment-oriented programming than non-arson offenders, like Caudill, Diamond, Trulson, DeLisi, and Marquart (2012) found to be the case when comparing 5,223 juvenile felony offenders. Rather, it is justifiable to offer treatment specifically tailored for firesetters, for example, the structured intervention program described by Swaffer, Haggett, and Oxley (2001), incorporating sessions about the dangers of fire, development of skills, insight and self-awareness, and relapse prevention.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.