
Abstract
In Colorado, “treatment victim advocates” (TVAs) serve alongside providers and probation/parole officers on “multidisciplinary treatment teams” (MTTs) to oversee domestic violence offender’s treatment. Although this model provides an opportunity for victim safety concerns to be heard, the utility of using victim advocates as advisors regarding interventions for domestic violence offenders has yet to be studied. Using survey data and narrative responses from TVAs (N = 37), the current study examines the challenges and opportunities TVAs face while serving on MTTs. Results suggest that, overall, TVAs are successful in communicating with other members of the MTT, are confident that their perspectives are valued in the offender decision-making process, and are able to provide a wide variety of services and referrals to the victims with whom they are engaged. Implications and recommendations for the Colorado model as well as correctional professionals managing domestic violence offenders internationally are presented and discussed.
Victim advocacy organizations have been at the forefront of the evolution of domestic violence (DV) from a “private family matter” to an “important social problem” worthy of organizational and institutional support. In this vein, the concept of victim advocacy has included two distinct avenues aimed at reducing DV and improving responses to victims. The first avenue focuses on providing direct services to victims. Examples of direct services include education, safety planning, and court advocacy, all of which serve to empower victims to make informed decisions for themselves and their families. The second avenue relates to affecting larger criminal justice system responses to DV such as working to change state or federal legislation, conducting trainings with criminal justice system personnel, and serving as liaisons between victims and criminal justice system actors.
In 2010, with the institution of the Revised Standards for Domestic Violence Offender Treatment (referred to hereafter as Standards), Colorado’s Domestic Violence Offender Management Board (DVOMB) drew on both avenues in developing a dual role for DV “treatment” victim advocates (referred to hereafter as TVAs) across the state. TVAs not only provide direct support services for victims but, as mandated by the Standards, also serve as equal representatives with treatment providers and probation/parole officers on multidisciplinary treatment teams (MTTs) that monitor DV offenders. As a result, TVAs in Colorado have the opportunity to encourage the consideration of victim safety concerns among the traditional targets of DV offender treatment such as cognitive/behavioral change and offender containment.
Among the guiding principles set forth by the DVOMB in 2010 is the idea that “the process by which domestic violence offenders are assessed, treated, and managed by the criminal justice system and social services systems should be coordinated and improved” (p. 3.1). Although the exact nature of Colorado’s coordination and improvement is novel, “coordinated community responses” to DV, consisting of interagency partnerships between criminal justice actors and community-based organizations more generally, have proliferated across the country (Bouffard & Muftić, 2007).
Given the often clandestine nature of DV, TVAs may provide insights that increase victim and community safety that could not be identified by other sources. At the same time, there may be inherent power differentials between treatment providers, probation officers, and TVAs, and issues of victim confidentiality may affect victim advocates’ ability to be an effective part of the MTT (Gover, Richards, & Tomsich, 2015). The present research examines TVAs’ experiences on MTTs as well as the challenges and opportunities they face in contributing to the team decision-making process for DV offenders as they complete their court-mandated DV treatment. The current study provides important information regarding how a novel multidisciplinary model—drawing perspectives from treatment, containment, and victim safety—“works” in practice and recommendations for improvement and/or proliferation of current practices are offered.
Victim Advocates and Domestic Violence
Victim advocates working at community agencies provide a range of direct services to victims of DV such as crisis hotlines, individual and group counseling, emergency shelter and transitional housing, and safety planning services (Burt, Zweig, Schlichter, & Andrews, 2000). According to Burt and colleagues (2000), estimates indicated that there were more than 775 programs serving victims of DV and more than 870 programs serving victims of both DV and sexual assault. A primary function of victim advocates includes assistance with “safety planning” or the development of a plan for the victim, and in many cases the victim’s children, to maximize safety during an abusive partner’s violence. Safety planning usually includes identifying weapon-free “safe zones” in the victim’s home and/or packing an emergency bag that includes important legal documents (e.g., social security cards, birth certificates), clothing, money, and contact information for resources such as the closest DV shelter. During safety planning, advocates may encourage the victim to create a plan of action regarding where to go, and how to get there, in the event a quick escape from her partner’s violence is necessary.
Victim advocates may also assist in filing protection orders or complete pro se preparation with the victim so that she may file the orders herself. In some cases, victim advocates liaise directly with attorneys who provide pro bono representation for victims in protection order and/or emergency custody hearings. Other direct assistance may include assisting victims in the development of victim impact statements, accessing state victim compensation programs, and making referrals to medical or social service providers.
In addition to delivering “tangible services,” victim advocates also provide social support to victims during important decision-making processes such as deciding whether to leave an abuser, file a protective order, or pursue criminal action against their abuser (Goodman & Epstein, 2008). Given the private nature of DV, victim advocates may serve as a victim’s primary or sole formal support provider. Indeed, Payne (2007) notes that, “just as a defense attorney works to protect the offender’s rights and interests, the victim advocate works to protect the victim’s rights and interests” (p. 84). Furthermore, Zweig and Burt (2007) found that victims who perceived that advocates supported their autonomy in making decisions (i.e., victims felt in control) were more likely to report that they would seek help from the agency again if they needed it compared with victims who perceived that victim advocates did not support their autonomy in making decisions.
Victim Advocates, Criminal Justice System Actors, and Domestic Violence
Victim advocate/criminal justice system collaborations have proliferated since the early 1990s, in part due to The STOP Violence Against Women Formula Grants Program that stemmed from the Violence Against Women Act (VAWA), Title IV of the Violent Crime Control and Law Enforcement Act of 1994 (P.L. 103-322; Roberts, 2002). One of STOP’s primary goals is to develop and/or strengthen victim services and to encourage coordinated interagency collaborations to promote positive victim experiences (Zweig & Burt, 2007). A key component of these responses includes embedding victim advocates into criminal justice system agencies. Currently, many jurisdictions have dedicated advocates that serve as liaisons between DV police units and/or courts and the victims they serve (Epstein, Bell, & Goodman, 2003).
System-based advocates, or advocates who are embedded in criminal justice system agencies, also provide assistance and support to DV victims. Their relationship with a victim begins during or after the victim engages with the criminal justice system. System-based advocates may help gather information from victims (i.e., evidence collection and fact finding), which may include accompanying victims to forensic interviews in cases of DV that includes sexual assault or results in physical injuries. Similar to community-based advocates, system-based advocates may also provide victims support through the court process and provide them with information or assistance regarding orders of protection, counseling, and shelters, and other social services (Camacho & Alarid, 2008). At the same time, system-based advocates must balance the needs of the victim with the needs of their agency, given that the victim serves as the primary and, in many cases of DV, only witness for the criminal justice system (Doerner & Lab, 2005). For example, Epstein et al. (2003) noted that system-based advocates may be required to reveal information considered “‘exculpatory’ such as the victim’s substance use, mental health status, or participation in therapy” to prosecutors as well as defense attorneys (p. 487).
Research demonstrates a host of benefits regarding partnerships between victim advocates and representatives of criminal justice system agencies. For example, cooperation between law enforcement and victim advocates is useful to both parties in the course of DV investigations. Victim advocates may serve as facilitators during these processes, using trauma-informed interviewing skills to obtain information that is relevant to the crime while minimizing victim stress and discomfort and protecting victims from secondary victimization (e.g., victim-blaming attitudes; Maier, 2008; Martin, 2005). Court-based advocates can serve as important conduits between the victim and the prosecutor in accompanying victims throughout the often complex and ever-changing court process.
Less research is available regarding collaborations between victim advocates and other criminal justice system actors—namely, probation officers—regarding DV. Such examples stem from larger “coordinated community responses” that engage multiple criminal justice system actors such as law enforcement, judges, and probation officers with practitioners such as victim advocates, mental health counselors, and substance abuse treatment services to improve interagency coordination in DV cases. Although coordinated approaches vary widely across sites, Bouffard and Muftić (2007) contend that community coordinated responses generally aim to meet multiple objectives including (a) improved system effectiveness, (b) delineation of services across agencies, (c) delivery of appropriate services to the victim with minimal distress, (d) protection of the victim, and (e) successful sanctioning of the offender. For example, Duluth, Minnesota’s coordinated community response includes an assessment of victim’s risk for further abuse by offenders completed by victim advocates (using the Danger Assessment; Campbell, 1995), which is not only used to determine the level of service offered to victims but also shared with probation officers tasked at performing pre-sentence investigations (Shepard, Falk, & Elliott, 2002). Probation officers use this information on victim risk, in addition to other information about the offender, to make recommendations about an offender’s containment needs (e.g., the amount of jail time to be served, the assignment of DV offender treatment, the length of probationary supervision; Shepard et al., 2002). Likewise, an evaluation of a coordinated community response in Cardiff, British Columbia identified that information sharing between criminal justice and non-criminal justice agencies (including victim advocates) was vital to responding to DV because it allows for the integration of offender information and the victim’s perspective in the decision-making process (Robinson, 2006).
Despite successful collaborations between victim advocates and actors within the criminal justice system, there are questions as to whether the philosophies and objectives of social service practitioners and criminal justice agencies are too often at odds to effectively partner in accomplishing feminist goals, especially with regard to DV (Beeman & Edelson, 2000; Burke, 1999). Further research has uncovered additional barriers to effective collaborations such as differential levels of authority among partner organizations, fear about confidentiality and data sharing, and differential access to resources (Allen, 2005; Clark, Burt, Schulte, & Maguire, 1996; Mills et al., 2000).
Colorado’s Unique Approach: MTTs
Consistent with the spirit of coordinated community responses to DV, TVAs are included in Colorado’s approach to domestic violence offender treatment in a unique and innovative way (Tunstall, Weible, Tomsich, & Gover, 2015). In Colorado, TVAs serve alongside providers and probation/parole officers on MTTs to oversee and manage DV offenders’ progress in treatment. In this role, TVAs represent general victim safety concerns, and in some cases, specific concerns from the victim (that the victim has given them permission to share). Comparatively, the provider focuses on recommendations regarding cognitive/behavioral change for the offender and the probation/parole officer prioritizes offender monitoring and containment. Together, MTTs have a three-pronged approach to offender treatment and management: treatment plan assessment and needs, victim safety, and offender containment. According to the Standards, concerns for these factors should be used to make decisions regarding offenders’ initial placement in treatment, placement reassessments throughout treatment, and discharge decisions.
In addition, TVAs are responsible for providing victims with support. One of the TVA’s roles is to reach out to the victim and inquire as to whether the victim is interested in various forms of information or services and whether she wishes to be contacted during the offender’s time in treatment. The TVA may also assist the victim in creating a safety plan that may include identifying danger warning signs, developing a list of phone numbers for emergency services, and a list of safe places and emergency shelters, among other resources. TVAs may also advise the victim on how to obtain a protection order and information regarding the Colorado Crime Victim Compensation Program. In Colorado, a victim’s level of involvement with a victim advocate is always “victim driven” per an empowerment model that views the victim as an autonomous decision maker (see, for example, Zweig & Burt, 2007).
The Current Study
The ways in which advocates provide direct services to victims of crime, and specifically DV victims, are generally well understood, and their influence within the larger criminal justice system such as interactions with law enforcement and DV courts has been previously examined. There is a gap in the literature, however, regarding how these experiences may translate into an advisory role in DV offender treatment. Furthermore, previous research about Colorado’s MTTs by Gover et al. (2015) identified specific gaps in knowledge regarding victim advocate roles on MTTs including (a) their ability to provide direct services to victims, (b) their role in MTT decision making regarding offender treatment, and (c) their frequency and quality of communication with other MTT members.
Given Colorado’s longstanding focus on DV as an important social issue, structured standards for DV treatment, and coordinated efforts by the DVOMB regarding DV perpetration and victimization, we expect that TVAs will report high levels of direct service provisions for victims they serve. We also expect TVAs to report a range of available referral sources and high rates of victim participation in victim advocate contracts and associated available services. Although the Standards envision TVAs serving in an equal role alongside their treatment provider and probation/parole officer counterparts, taking into consideration the power differentials between MTT members—TVAs are employed by treatment providers, and treatment providers receive referrals from probation officers—we expect that TVAs will report experiencing subordinate roles on MTTs as well as poor quality, and low rates of communication. In this vein, the current research will explore the specific roles TVAs play on MTTs in the treatment of DV offenders across the state of Colorado, their experiences on MTTs, as well as the challenges and opportunities they face in this role.
Method
Sample and Data
The initial sampling frame for the current analysis included the population list of TVAs (n = 110) currently working with DV offender treatment providers in Colorado on at least one MTT (n = 172) 1 that was provided to the research team by the DVOMB staff. Victim advocate information was cross-checked with treatment provider information to confirm that all victim advocates on the list were associated with at least one DV treatment provider and that all DV treatment providers were associated with at least one TVA. Seven victim advocates were omitted from the sample because their contact information (phone number and email addresses) were missing from the DVOMB records, which resulted in a final sampling frame that included 103 TVAs.
Thirty-seven victim advocates responded to the online survey for a response rate of 36%. Two respondents “opted out” of participating in the survey, resulting in a current sample of 35 victim advocates. Victim advocates reported serving clients in 28 of Colorado’s 64 counties, with the greatest representation (five or more advocates) from Adams, Arapahoe, Denver, Jefferson, and Boulder counties. 2 Slightly more than half of the TVAs (51%) reported holding more than a BA/BS degree, while 23% reported holding a BA/BS degree, 9% reported an AA/AS degree, 14% reported some college, and one advocate reported receiving a high school diploma. TVAs reported a wide range of prior experience working with DV victims and/or DV offenders. Advocates reported between less than 1 year’s experience and 31 years’ experience (M = 11 years). All victim advocates reported receiving specialized training on the topic of DV. TVAs reported receiving between 2 and 100 hours of training with 50% of advocates reporting 49 hours or more of training. In addition, 74% of TVAs reported serving on MTTs with providers whose clients include a special population of DV offenders, such as female offenders or offenders from same-sex couples. Among those advocates who reported working with these populations, 66% reported receiving specialized DV training to work as an advocate with these populations.
The majority of TVAs worked for one treatment provider (n = 23); 14 advocates reported that they worked with two or more treatment providers. 3 Victim advocates reported caseloads of between 3 and 30 cases (for the time period January to August, 2015) with an average of 23 cases. In addition, the majority of TVAs (83%) reported holding other employment in addition to their position as a victim advocate.
Instrument and Procedure
The survey instrument was developed based on the specific mandates for Colorado TVAs (outlined in the 2010 Revised Standards for Domestic Violence Offender Treatment) and the results of a prior process evaluation that examined Colorado’s response to DV (Gover et al., 2015). Specifically, the survey focused on the services provided to victims, MTT communication issues, and MTT decision-making processes. The Institutional Review Board at one of the investigator’s institutions approved the research procedures.
The instrument was pilot tested by research team members, other researchers, and several DVOMB staff. Modifications were made to the survey based on the pilot testing results and were incorporated prior to the survey’s launch. 4 The survey instrument was administered online to participants using Qualtrics survey software. Specifically, an email invitation was sent to each potential participant, which included a brief overview of the research, information on the risks and benefits of participation, and a unique link to the survey. Participants were asked to respond to the survey invitation by completing the survey or declining to participate within 14 days of receiving the invitation email. Survey reminders were sent via email on Days 3, 5, and 7, and a final reminder was delivered via phone on Day 10. Only respondents who had not yet completed the survey were included in the reminder at each time point. Respondents were compensated for their time with a US $10 Amazon e-gift card.
Results
The purpose of this exploratory study was to examine the experiences of TVAs in Colorado and to identify the challenges and opportunities they face serving on MTTs. Specifically, we were interested in victim advocates’ (a) ability to provide direct services to victims, (b) their role in MTT decision making regarding offender treatment, and (c) their frequency and quality of communication with other MTT members. Given our review of the prior literature and prior research regarding the response to DV in Colorado, we expected that TVAs would report that they were able to provide high levels of direct services to victims as well as a range of available referral sources, and high rates of victim participation in services. Furthermore, based on the prior process evaluation of Colorado DV treatment by Gover and colleagues (2015) and our knowledge of the power differentials between the MTT members, we hypothesized that victim advocates would indicate serving in secondary decision-making roles on MTTs and report infrequent and poor-quality communication with other MTT members. The results of TVA survey data are presented below.
Victim Support Provided by Victim Advocates
First, we examined whether or not DV victims were actually engaging with TVAs. Results revealed that TVA’s engagement with victims of DV varied widely across TVAs with respondents reporting as few as 1% to as many as 95% of victims choosing not to engage with victim advocates on MTTs. Half of the victim advocates sampled here reported that 30% or more of the DV victims to whom they are referred do not maintain involvement with them after an initial contact; almost 20% of TVAs reported that 80% or more of victims choose not to engage in an ongoing advocacy relationship.
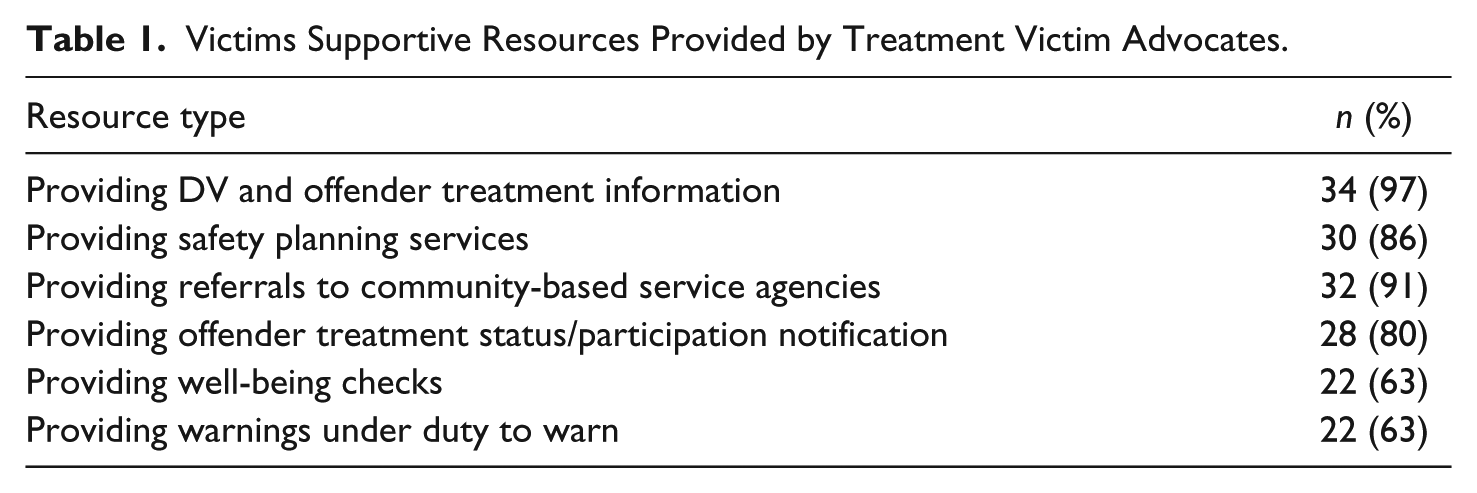
A primary goal for victim advocates on MTTs is to provide victims with support while the offender is engaged in the treatment process. Among advocates who reported delivering services and/or referrals to victims, a wide variety of options were utilized (see Table 1). For example, victim advocates provide DV and offender treatment information (97%), safety planning services (86%), referrals to community-based service agencies (91%), status/treatment participation notification (80%), victim well-being checks (63%), and warnings under duty to warn (63%). 5
Victims Supportive Resources Provided by Treatment Victim Advocates.
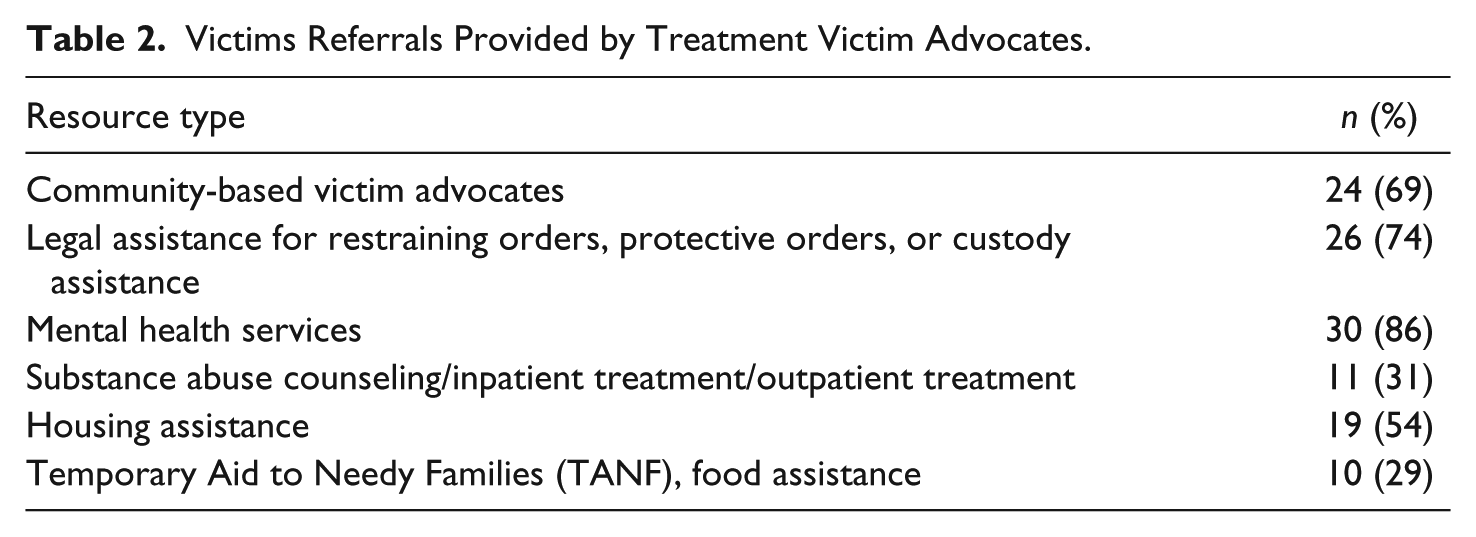
The Standards further indicate that TVAs can provide victims appropriate referrals to community programs. Victim advocates reported regularly providing a range of referrals for mental health services (86%), legal assistance (74%), community-based victim advocates (69%), housing assistance (54%), substance abuse counseling and/or treatment (31%), and TANF/food assistance (29%; see Table 2). Consistent with our hypothesis, the majority of victim advocates (80%) did not report barriers to providing referrals to victims of DV. When MTT victim advocates did identify barriers to providing referrals, barriers included unavailable contact information for victims and lack of transportation options for victims for service engagement.
Victims Referrals Provided by Treatment Victim Advocates.
Victim Advocates and MTT Decision Making
Contrary to our expectations, a majority (66%) of TVAs reported that MTT decision making for offenders’ initial placement in treatment was made as a team. Overall, victim advocates described reciprocal decision making whereby treatment providers shared the results of their standard assessment of offenders, other members reviewed the information and added comments, and consensus was reached after discussion. For example, one TVA noted, “Any member can suggest review and all members with knowledge of the case share their input. [It is a] very functional group process. Mutual respect is evident.” While another reported, “Each member provides their feedback and information they have collected regarding the offender, then as a group we discuss what would be the best level of treatment . . . of course also taking in account the guidelines requirements.”
Some TVAs reported a slightly different process for reaching consensus where the treatment provider and probation officer provided an “initial” recommendation for treatment intensity level and then the victim advocate was free to confirm this decision or recommend a change in the decision regarding treatment level. For example, one victim advocate indicated, The treatment provider sends an initial contact sheet with brief overview of arresting incident/other pertinent information and this often includes treatment level (or presumed treatment level), along with victim contact information. Later, the treatment provider sends their assessment and write up which includes their treatment level recommendation; this also gets sent to probation. As a treatment advocate, I can disagree and talk to the treatment provider about any concerns about treatment level or other treatment recommendations.
Another victim advocate shared a similar protocol, There is usually a meeting between the provider, and any other agencies involved (probation, parole, etc.) and they decide the level of treatment. I usually meet with the therapist individually to give my report on the victim in the case. I give ongoing updates and if concerns arise than a meeting is held about how to address those concerns.
Among TVAs reporting that one team member was the primary decision maker, 83% indicated that the treatment provider made the decisions regarding offender placement whereas 17% reported that the probation officer made such decisions. For example, TVAs reported, “the evaluation is done by the treatment provider and I am told what treatment level the offender is placed in,” “I don’t have any decision making authority over an offender’s treatment plan,” and “the treatment provider makes the determination based on intake information and court documents relative to the case.” Among victim advocates reporting that the probation officer has primary decision-making authority on the MTT, one TVA reported, It is essentially the probation officer making treatment related decisions—it is the treatment provider who needs the referral, [and providers] are less invested in holding the client accountable for the sake of obtaining additional referrals. Therefore, the victim advocate has little to no role other than occupying a chair.
At the same time, almost three quarters of TVAs (74%) reported feeling that other MTT members valued their opinions. And, likewise, approximately one quarter of victim advocates respectively reported that they had felt compelled to agree with the treatment provider or disregard their concerns in favor of the treatment provider’s perspective (23%) or the probation/parole officer’s perspective (26%).
Communication Among MTT Members
Inconsistent with our hypothesis, few TVAs (31%) reported that they experienced regular exclusion from communication by the other members of the MTT.
According to the Standards, MTT members can use a variety of methods to communicate information related to an offender’s treatment plan (i.e., treatment intensity level placement, treatment plan reviews, etc.). TVAs reported that email was the most frequently used mode of communication (83%), followed by phone conversations (77%), face-to-face communication (63%), and internal software such as ReliaTrax (26%). Other forms of communication used included fax, internal reports, and mail. Regarding communication, one victim advocate noted, “It’s important to reiterate that most treatment advocates have other jobs and cannot participate directly in meetings (in person or otherwise) during regular business hours.” Likewise many victim advocates suggested increasing the use of internal software for communication and organization of case information—a strategy that might circumvent scheduling issues while still allowing victim advocate input at all stages of the treatment process. For example, one victim advocate suggested “standardizing the use of Reliatrax and making sure that users of Reliatrax use the system’s Treatment Plan review feature so that victim advocates can approve/reject placement levels and add comments and concerns.”
Also contrary to our expectations, the majority of the TVAs reported high-quality communication on their MTTs. Specifically, most victim advocates (86%) reported that they were able to successfully advocate for victim safety concerns to the other members of the MTT regarding offenders’ initial placement in treatment and (80%) reported that they were able to successfully advocate for victim safety during offenders’ treatment plan reviews. At the same time, several recommendations for improving TVAs’ ability to support victim safety were reported. Recommendations focused on obtaining timely information from MTT counterparts regarding either the victim or the offender. For example, one victim advocate indicated, “It would be nice to receive the police report with every single victim. That should be mandatory for every victim advocate . . . I need to have the police report and in a timely manner.” TVAs also noted, “better access to victim info would be huge”; “It is very important that the treatment provider consults with victim advocate at time of treatment plan review to make sure progress and needs are addressed properly”; and “Timely victim referrals. I often receive victim contact sheets many weeks or even months after an offender has started treatment so I haven’t been able to work with the victim during the entire process as intended.”
Discussion
The purpose of this study was to explore the experiences of TVAs in Colorado who serve on MTTs with probation officers and DV offender treatment providers to oversee DV offender treatment. We were interested in victim advocates’ experiences particularly in regard to the opportunities presented to provide victims with direct services and the challenges they face in doing so. Furthermore, we were interested in victim advocates’ roles in MTT decision making regarding offender treatment and their frequency, quality, and mode of communication with other MTT members.This study captures the voices and experiences of TVAs who are part of a novel collaboration with other system actors to make decisions about offenders’ progress in treatment.
Findings indicate that there is wide variation in the provision of services by TVAs, primarily due to challenges regarding victim engagement. Victim reluctance to pursue criminal justice system resources is not a new phenomenon and, in many cases, this hesitation does not come without cause. A significant body of literature has documented that many victims of gender-based violence including DV (and sexual assault) are met with negative responses by criminal justice personnel, and in some cases experience a “second assault” including disbelief, victim blaming, and a general lack of sensitivity by first and second responders (Erez & Belknap, 1998; Smith, 2000). Victims also report experiencing negative treatment by prosecutors and law enforcement officers when they do not actively cooperate with the criminal justice system process, and in some jurisdictions, victims are forced to participate or face subpoenas or prosecution themselves (Dempsey, 2009; Esptein, 1999). Furthermore, research indicates that victims of DV who seek help from the criminal justice system, but do not perceive law enforcement officers to be helpful or interested in them or are not satisfied with how the law enforcement officers handle the incident, report a lower likelihood of seeking assistance again (Johnson, 2007). Taken together, TVAs may have to clear significant hurdles to increase engagement by victims, especially those victims who have been “let down” by the criminal justice system in the past.
Victim engagement is not a unique problem to Colorado—many survivors who are no longer in relationships with their abusive partners choose to completely disengage from the system and therefore do not receive referrals for assistance from advocates. Comparatively, victims who remain in relationships with their partners may choose to disengage from the system as a sign of renewed commitment to their partner or in an effort to put “the incident behind them.” At the same time, Gamache (2012) suggests that an appropriate assessment of partner danger requires the victim’s involvement and input so that the context of the situation can be framed completely. Thus, TVAs and the DVOMB more generally must prioritize increasing victim engagement.
Currently, the treatment provider is the conduit between the victim and the TVA. First, the offender must be assigned a treatment provider. Then, the treatment provider must obtain the victim’s contact information and then provide it to the TVA. Over the course of this process, several weeks or more might pass, and as previously mentioned, the victim may change addresses or simply “move on” from the incident. In addition, it is unclear from the current findings whether providers obtain victim contact information from the offenders themselves or from police reports. As such, a more streamlined system must be developed to engage victims in the process immediately after the violent incident.
One suggested mechanism to achieving “fast tracked” engagement is to develop a centralized clearinghouse. For example, a staff person or trained intern at the Colorado Division of Criminal Justice (or the DVOMB) could complete a follow-up call with all victims immediately after the incident comes to the attention of the criminal justice system. The purpose of this initial contact would be to explain the MTT process including the role of the TVA and services available to them. In addition, an inventory of the victim’s contact information could be completed in addition to a “collateral contact,” such as a friend or family member who could serve as a back-up form of contact for reaching the victim. Such an effort would require some innovation and coordination, but has the potential to increase victim engagement in the MTT process, and as a result, encourage more informed decision making regarding offender treatment on MTTs. Future academic–practitioner partnerships could support the development of a pilot program and then test the impact of the program against “control” jurisdictions without the strategy to increase victim engagement with the system.
Transportation was also identified as a barrier to service engagement for many victims. Policy makers should consider the allocation of funding from sources such as VAWA funds, state block grants for victim services, and/or victim compensation funds to provide bus tokens or taxi vouchers to increase victims’ access to services. With ever-shrinking budgets, creative solutions could be drawn from the nascent literature on telecounseling for victims of DV where service providers connect with clients remotely through technology (McCord et al., 2011) and/or mobile medicine where providers travel to community centers or into neighborhoods to serve clients en masse.
Regarding decision making, the majority of TVAs felt that their opinions were valued during the decision-making process and that the MTT treated them as an equal team member and made decisions about offenders together as a team. Most advocates described decision making as a thoughtful and respectful process where information is exchanged among all team members before consensus is reached. Prior research on coordinated community responses have identified that an “inclusive climate” is paramount to effective collaborations for responding to DV (Allen, 2005, p. 58). Although the majority of advocates’ experiences are aligned with the expectations of the Standards (i.e., reciprocal decision making involving discussion and consensus), other incongruent models were also uncovered. For example, some TVAs reported that their MTTs operated such that the treatment provider recommended the initial placement level to the advocate and probation officer and then provided them with an opportunity to express concerns and confirm placement. Other TVAs reported that decisions were made unilaterally by the treatment providers or probation officer, and that they did not have any influence over the decision-making process. As a result, neither general, nor specific victim safety concerns as understood by the TVAs were routinely considered by the MTT.
Overall, the results from this study suggest that power dynamics within the structure of MTTs may affect some team decision making. Such power imbalances have been identified in previous assessments of coordinated community responses to DV and associated with problems meeting the collaboration’s goals (Allen, 2005; Clark et al., 1996). Interestingly, among TVAs who felt compelled to agree with another team member rather than express their own opinion, more advocates felt compelled to align with probation officers rather than treatment providers, even though the treatment provider often employs the advocate. It may be that victim advocates perceive probation officers as inherent authority figures due to their association with the criminal justice system, or it may be that authoritative personalities “self-select” into work as probation officers.
The DVOMB might consider identifying MTTs that constitute “model” teams across different types of jurisdictions (e.g., urban/suburban, rural, frontier) and aim to proliferate these models across the state. In addition, cross-training TVAs, treatment providers, and probation officers may improve understandings of each MTT member’s role on the team. Furthermore, the creation of ombudsmen who can mediate problems between MTT members could prove beneficial given the power dynamics and multiple, and potentially conflicting, goals of MTTs (e.g., victim safety, offender containment, offender progress in treatment, matriculation of offenders from caseloads).
Findings also suggest that many TVAs work for several different treatment providers. Some victim advocates work in advocacy or counseling roles beyond their work on MTTs, and others have additional employment besides their advocacy work, leading to the conclusion that TVA positions rarely constitute full-time employment. Given that TVA positions many times constitute second, third, or even fourth jobs, advocates may be limited regarding their availability for MTT communication and collaboration. In consideration of these findings, the DVOMB may consider developing some concrete guidelines regarding structured availability of TVAs for communication purposes. Furthermore, in designing the sampling frame for the current research, we discovered that some the contact information for some TVAs (i.e., email and phone number) that was on file with the DVOMB was no longer correct. Although the DVOMB currently completes bi-annual reviews of treatment providers and TVAs, it might consider completing annual reviews.
Relatedly, although multiple reminders (phone and email) were completed with potential respondents to reduce non-response bias (McPeake, Bateson, & O’Neill, 2014), our study yielded a 36% response rate. Previous attempts by the DVOMB to survey advocates also resulted in minimal response whereas another effort created for outreach, information collecting, and information sharing—a Yahoo group only for TVAs—is rarely used. Furthermore, research on collaborations between practitioners and researchers suggests that practitioners are often skeptical of research, indicating that researchers do not accurately capture their voice when examining the criminal justice response to DV (Murray et al., 2015). As a result, it may be that when practitioners are given the opportunity to express their views and opinions, such as in the research here, advocates fail to participate due to uncertainty about how they will be portrayed. At the same time, response rates for online surveys are often lower than other forms of surveys (Lozar Manfreda, Bosnjak, Berzelak, Haas, & Vehovar, 2008; Sax, Gilmartin, & Bryant, 2003). It is possible that some key perspectives may have been omitted or overstated due to undetected sample selection bias. It is also possible that TVAs who did respond represent those with polarized responses—those who have had very positive experiences on MTTs and those who have had poor experiences on MTTs. Furthermore, given that TVAs are often employed by treatment providers, it is likely that some did not feel comfortable completely sharing their experiences in the current research.
Conclusion
Colorado has developed a novel response to DV rooted in the risk/needs/responsivity literature: the utilization of a multidisciplinary team including representation from DV treatment, offender containment, and victim safety to manage offender supervision. One of the most distinctive aspects of Colorado’s approach is the inclusion of a TVA in offender treatment decisions. However, even the most thorough evidenced-based intervention is only as good as its implementation (i.e., the “devil is in the details”).
Results from this study demonstrated several challenges to complete implementation of Colorado’s MTT model from the perspective of TVAs. Chief among these challenges are TVA’s ability to engage victims, power differentials among MTT members, and problems with MTT communication. Recommendations to improve victim engagement and increase TVA’s delivery of services are the timely transfer of victim contact information to the TVAs and assistance with transportation for victims. Another area in need of improvement for the DVOMB is maintaining updated TVA contact information. From the execution of this study, we discovered that some TVA contact information maintained by the DVOMB was outdated. An open flow of communication across MTTs and the DVOMB is key to successful implementation of the Standards.
Despite remaining implementation challenges, the current study presents encouraging findings regarding TVAs’ influence and impact on the MTT model. Among victims who are being reached, a wide variety of referrals and direct services are being provided. In addition, the majority of TVAs felt that decisions were made as a team and that their voices were being heard, which completely aligns with the intention of the Standards. Overall, with some small achievable modifications, the MTT model can be further improved for offenders seeking DV offender treatment in Colorado.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.