
Abstract
The aim is to determine the appropriate cutoff values of waist circumference (WC) for an increased risk of the metabolic syndrome in the Korean elderly population. We analyzed the WC cutoff values of four groups divided according to sex and age with a total of 2,224 elderly participants aged 65 years old and above from the Fourth Korean National Health and Nutrition Examination Survey using the receiver operating characteristic curve and multiple logistic regression. The WC cutoff values associated with an increased risk of metabolic syndrome were 89.6 cm for men and 90.5 cm for women for those who were 65 to 74 years old, and 89.9 cm for men and 87.9 cm for women for those who were 75 years old or older. WC cutoff points for estimating metabolic risk are similar in elderly men and women. Age-specific optimal WC cutoff points should be considered especially for elderly women in screening for metabolic syndrome.
Introduction
Since the metabolic syndrome was defined as a cluster of cardiovascular risk factors such as obesity, insulin resistance, dyslipidemia, and hypertension (World Health Organization [WHO], 1999), a number of expert groups have attempted to develop diagnostic standards for the metabolic syndrome. In 2004, the International Diabetes Federation (IDF; Alberti, Zimmet, & Shaw, 2006) consensus proposed a new definition for the metabolic syndrome that would provide a single internationally applicable diagnostic tool. This definition emphasized the importance of central obesity, measured by waist circumference (WC), with ethnic- and gender-specific cutoff points because it is more strongly correlated with the other metabolic features than any other parameter and is highly correlated with insulin resistance. Therefore, a study by the Korean Society for the Study of Obesity (KSSO; Lee et al., 2007) and other studies (Choi et al., 2004; Kim, Choi, & Yum, 2006) have proposed the WC cutoff values for central obesity in Korean adults as 90 cm for men and 85 cm for women. However, these cutoff value recommendations were based on studies that included predominantly young and middle-aged populations.
The aging process is characterized by a decrease in body weight and height, an increase in fat mass, and the redistribution of trunk and visceral adipose tissue (Moon, & Kim, 2005; Perissinotto, Pisent, Sergi, Grigoletto, & Enzi, 2002), influencing the profile of risk factors for developing the metabolic syndrome (Kim et al., 2009; Moon, & Kim, 2005; Seo et al., 2009). These changes occur differently according to sex; females are predominantly susceptible to increases in fat redistribution (Moon, & Kim, 2005; Perissinotto et al., 2002). However, in both sexes, there is a turning point during the aging process in which not only is the body mass index (BMI), the ratio of the weight to the squared height, reduced but the WC also decreases after they increase (Moon, & Kim, 2005; Perissinotto et al., 2002; Stevens, Katz, & Huxley, 2010), leading to health outcomes (e.g., morbidity and mortality) related to cardiovascular disease (Heiat, Vaccarino, & Krumholz, 2001; McTigue, Hess, & Ziouras, 2006). In both sexes, 75 years of age has been reported their turning points in previous studies (Moon, & Kim, 2005; Perissinotto et al., 2002; Stevens et al., 2010).
Therefore, the WC criteria of younger adults for metabolic syndrome cannot be applied to the elderly. However, no age-specific WC cutoff values for central obesity have been developed for the Korean elderly population. Thus the aim of this study is to determine the appropriate WC cutoff values for an increased risk of metabolic syndrome in the Korean elderly population.
Method
Study Population
This study used the health interview and health examination data from the Fourth Korean National Health and Nutrition Examination Survey (KNHANES, 2009) conducted by the Korean Centers for Disease Control and Prevention (KCDC) from 2007 to 2008. This survey used a stratified, multistage probability sampling design by administrative district, place of residence (urban/rural), and residential pattern (apartment/nonapartment) to select a representative sample of civilian, noninstitutionalized Koreans,. The respondents’ data were assigned weights to assure the equal probability of being sampled and to cover missing data.
Of a total of 14,338 participants from these sampling frames, 9,769 individuals (68.13%) agreed to participate in the survey. This particular study measured metabolic risk factors and was limited to elderly respondents aged 65 and older, with 2,224 individuals in total. The participants were separated into four groups, 645 males and 890 females between the ages of 65 and 74 years, and 234 males and 455 females aged 75 years or above, following the turning point of WC patterns based on age (Moon, & Kim, 2005; Perissinotto et al., 2002; Stevens et al., 2010) and the association of the responses with health outcomes (Heiat et al., 2001; McTigue et al., 2006) were analyzed in this study.
Measures
The values of WC and other parameters of the metabolic syndrome were identified from the results of a health examination survey conducted by well-trained examiners. WC was measured with a nonelastic tape at the end of normal expiration at the midpoint between the lower border of the rib cage and the iliac crest. Blood pressure (BP) was measured with a mercury sphygmomanometer (Baumanometer; WA Baum, Copiague, NY, USA) after a 10 min rest in the sitting position, while participants refrained from smoking and ingesting caffeine during the 30 min preceding the measurement. The systolic and diastolic blood pressure were measured, and the average of the measurements was used in the final analysis. If the first two measurements differed by more than 5 mmHg, additional readings were taken.
Blood samples for triglyceride (TG), high density lipoprotein cholesterol (HDL-C), and fasting glucose (FG) were obtained from an antecubital vein and stored in vacutainer tubes containing EDTA in the morning following an overnight fast and analyzed at a certified laboratory.
The criteria for metabolic syndrome followed the guidelines suggested by IDF (Alberti et al., 2006): central obesity defined according to ethnicity-specific WC plus a combination of two or more of the following risk factors: elevated TG, ≥150 mg/dL, use of medication for it; reduced HDL cholesterol, <40 mg/dL for men and <50 mg/dL for women, use of medication for it; elevated BP, systolic ≥130 mmHg, diastolic ≥85 mmHg, use of hypertensive medication; and elevated FG, ≥100 mg/dL or previously diagnosed type 2 diabetes, use of antidiabetic medication.
Other potential confounding data included education, employment status, economic status, and health-related behaviors such as smoking, alcohol consumption, and exercise collected from the questionnaire. Education level was categorized into four groups: elementary, middle, high, and university. Employment status was indicated by their present employment status (Yes/No). Economic status was determined from the household’s economic status, and was classified into one of four groups below each quartile: lower than 25%, 25% to 50%, 51% to 75%, and 76% to 100%. Smoking was assessed by current smoking (Yes/No), alcohol drinking was assessed by the typical daily intake of alcoholic beverages (Yes/No), and exercise was assessed by exercising three times per week regularly (Yes/No).
Data Analysis
Age- and gender-specific data were analyzed with descriptive statistics to determine the general and clinical characteristics of the study participants. The chi-square test and the independent sample t test were used to examine significant differences according to sex. The WC values associated with an increase in the prevalence of the metabolic syndrome were calculated using the receiver operating characteristics (ROC) curve by presenting the optimal thresholds for each parameter with the best combination of sensitivity and specificity. To identify the appropriate diagnostic criteria of the WC values with increasing the risk of prevalence of metabolic syndrome, multiple logistic regression analyses without or with adjustments for general characteristics of the study participants were performed by presenting odds ratios (ORs) and their 95% confidence intervals (CI). In these analyses, the WC values were categorized by their quintiles, with the first quintile used as the referent. All statistical analyses were conducted using SPSS 16.0.
Results
General Characteristics of the Study Participants
Table 1 represents the general characteristics of the participants by sex and age groups. Of a total of 1,535 individuals aged 65 to 74 years, men (n = 645) accounted for 42.0% of the participants and women (n = 890) accounted for 58.0%. There were significant differences between the sexes in regard to education, employment status, economic status, smoking, and alcohol drinking: women were found to be less educated, less employed, and in a lower economic status; on the other hand, men smoked more and drank less. There was no significant difference between sexes in relation to exercise.
General Characteristics of the Study Participants (N = 2,224), n (%).
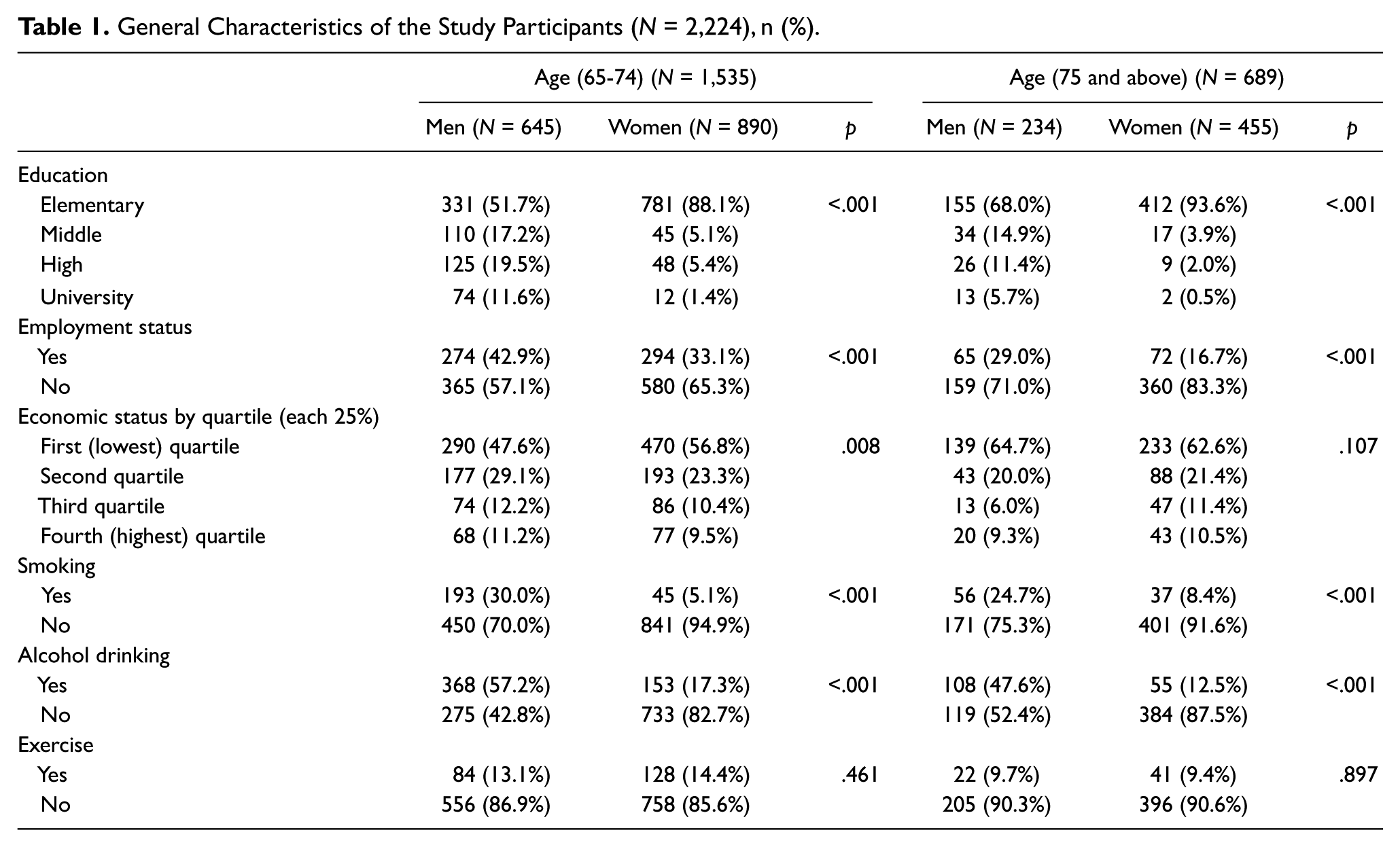
Of a total of 689 individuals aged 75 years and above, men (n = 234) accounted for 34.0% of the participants and women (n = 455) accounted for 66.0%. There were significant differences between the sexes with regard to education, employment status, smoking, and alcohol drinking: women were found to be less educated and less employed; on the other hand, men smoked more and drank less. There were no significant differences between the sexes for economic status and exercise.
Clinical Characteristics of the Study Participants
Table 2 presents the clinical characteristics related to metabolic syndrome of the participants by sex and age groups. For those 65 to 74 years old, there were significant differences with regard to triglyceride levels: the mean triglyceride level was higher in women (149.1 ± 86.1) than in men (134.8 ± 79.4). However, there were no significant differences found with regard to the other metabolic syndrome parameters, HDL-C, systolic BP, diastolic BP, fasting glucose, WC, and metabolic syndrome (N ≥ 2). Although there was no difference between the sexes with regard to WC, the mean WC was higher in women (85.3 ± 9.7) than men (84.9 ± 8.6). The percentage of participants who had metabolic syndrome was 41.4% in men and 45.8% in women.
Clinical Characteristics of the Study Participants n (%).
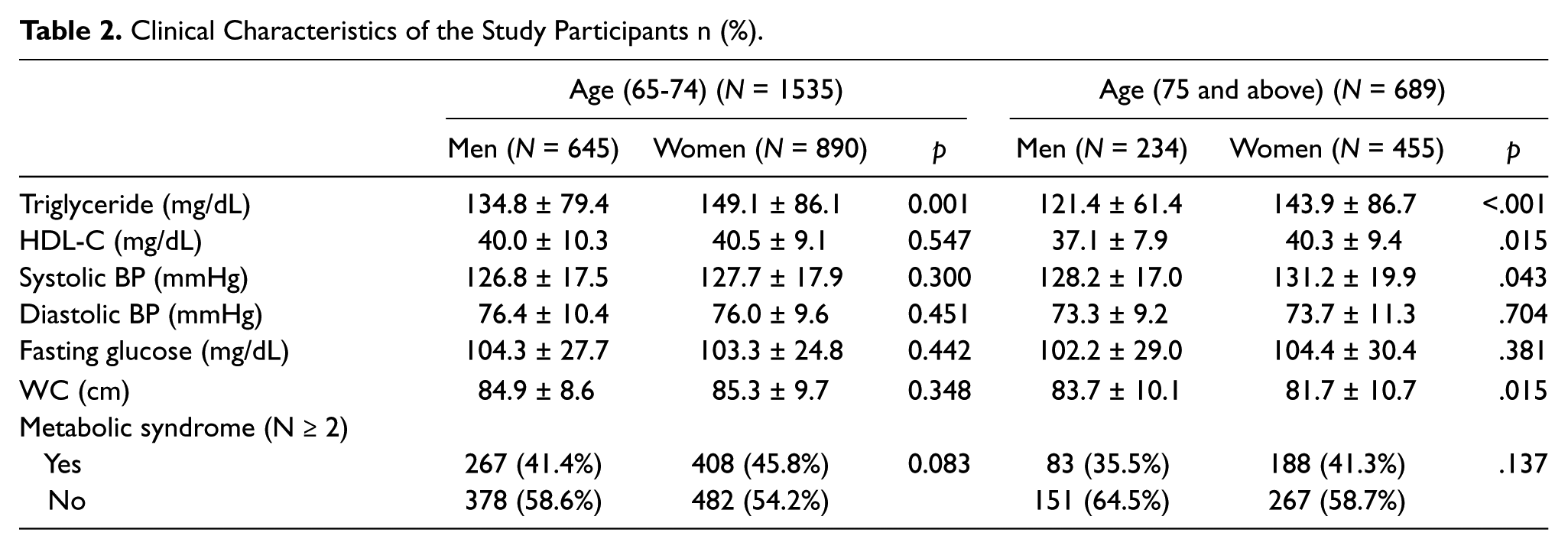
For those who were 75 years old and above, there were significant differences in regard to triglyceride levels, HDL-C, systolic BP, and WC: the mean triglyceride level, HDL-C, and systolic BP were higher in women (143.9 ± 86.7, 40.3 ± 9.4, and 131.2 ± 19.9, respectively) than in men (121.4 ± 61.4, 37.1 ± 7.9, and 128.2 ± 17.0); the mean WC was higher in men (83.7 ± 10.1) than women (81.7 ± 10.7). However, there were no significant differences found with regard to the other metabolic syndrome parameters, diastolic BP, fasting glucose, and metabolic syndrome (N ≥ 2). The percentage of participants who had metabolic syndrome was 35.5% in men and 41.3% in women.
WC Values Associated With an Increase in the Prevalence of the Metabolic Syndrome
Figure 1 and 2 present the WC optimal values maximizing sensitivity and specificity by using the ROC curve. In those who were 65 to 74 years old, the WC values were 83.5cm for men (sensitivity 66.9%, specificity 52.0%, p < .001) and 83.5cm for women (sensitivity 69.5%, specificity 51.1%, p < .001). In those who were 75 years old and above, the cutoff values for WC using the ROC curve were 84.5cm for men (sensitivity 61.4%, specificity 60.3%, p < .001) and 80.5cm for women (sensitivity 67.6%, specificity 60.3%, p < .001).
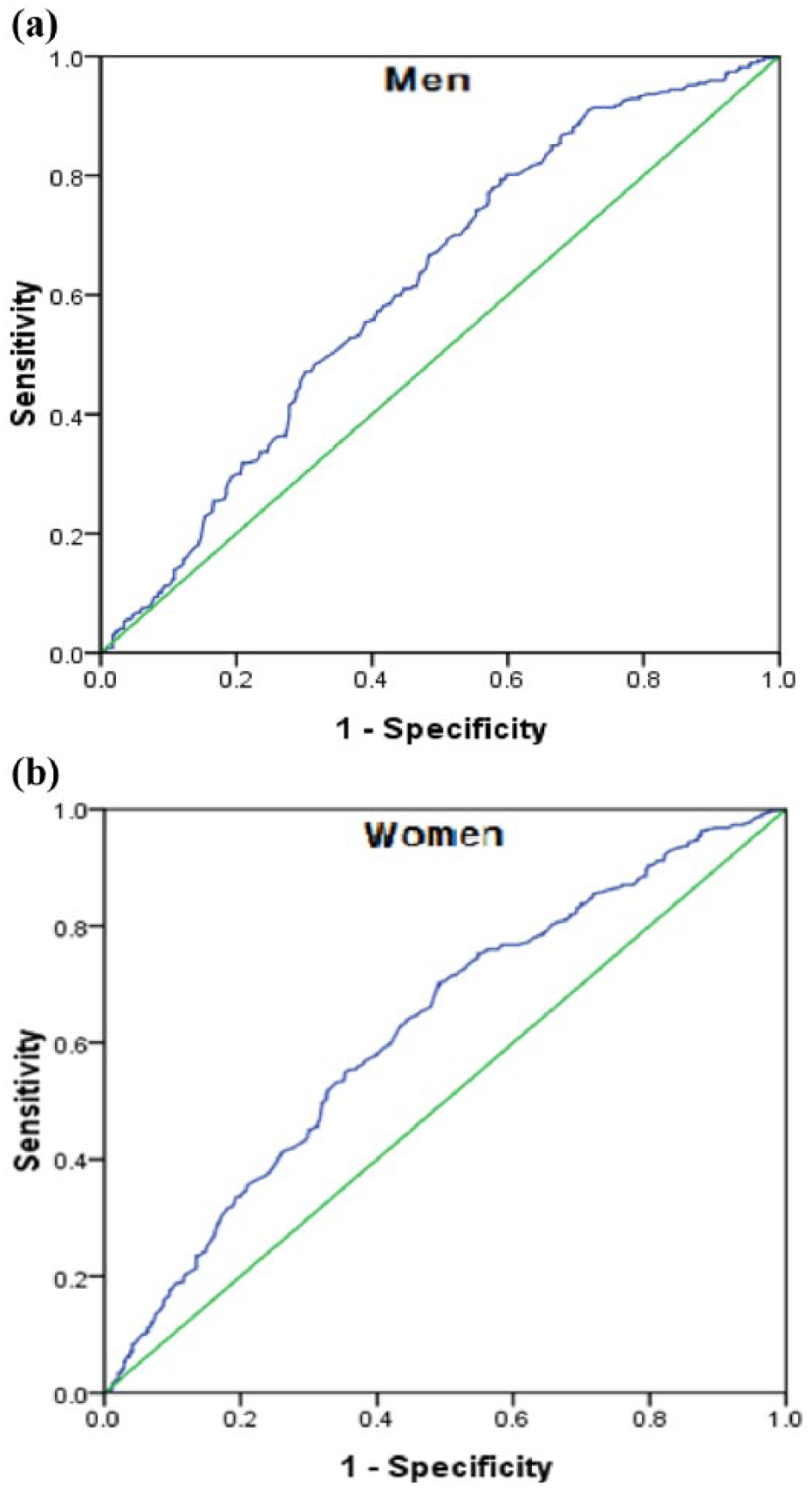
Receiver-operating characteristic (ROC) curves for the WC values associated with an increase in metabolic syndrome for the age group of 65 to 74 years.
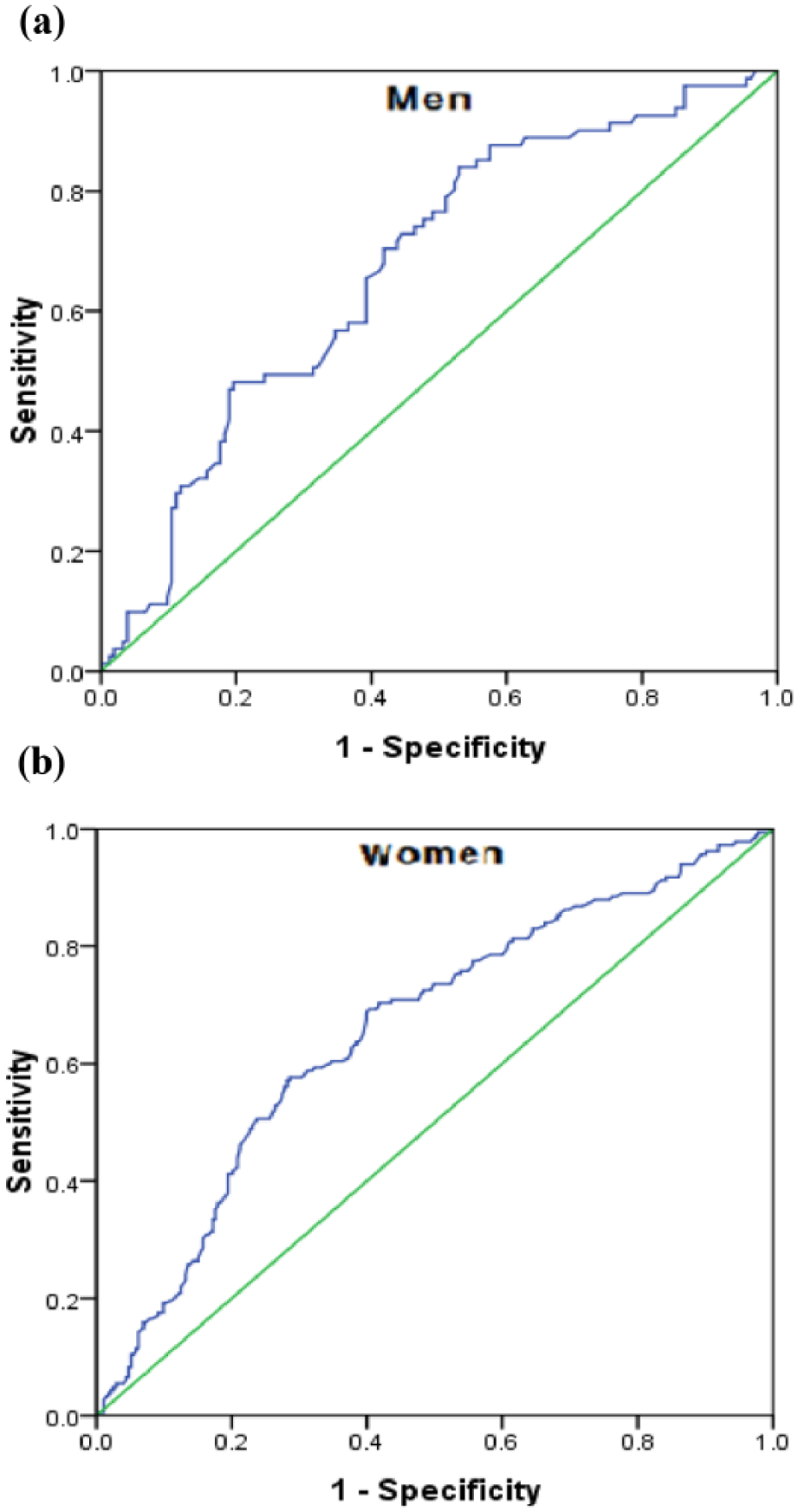
Receiver-operating characteristic (ROC) curves for the WC values associated with an increase in metabolic syndrome for the age group of 75 years and above.
WC Cutoff Values for Predicting Metabolic Syndrome
Table 3 represents the ORs for predicting the presence of metabolic syndrome according to the WC quintiles based on the first quintile with adjustments for general characteristics made. In men 65 to74 years old, the ORs for predicting metabolic syndrome were statistically significant from the second quintile of 80.5 cm (WC) (OR: 3.8, p < .001), the third quintile of 85.3 cm (WC) (OR: 3.6, p < .001), the fourth quintile of 89.6 cm (WC) (OR: 5.7, p < .001), and to the fifth quintile of 96.8 cm (WC) (OR: 4.7, p < .001). In women 65 to 74 years old, the ORs for predicting metabolic syndrome were significant from the third quintile of 85.6 cm (WC) (OR: 2.4, p < .001), the fourth quintile of 90.5 cm (WC) (OR: 3.0, p < .001), and to the fifth quintile of 98.5 cm (WC) (OR: 3.2, p < .001). In men 75 years old and above, the ORs for predicting metabolic syndrome were significant from the third quintile of 84.6 cm (WC) (OR: 5.0, p = .004), the fourth quintile of 89.9 cm (WC) (OR: 3.8, p = .017), and to the fifth quintile of 97.2 cm (WC) (OR: 8.2, p < .001). In women 75 years old and older, the ORs for predicting metabolic syndrome increased significantly from the fourth quintile of 87.9 cm (WC) (OR: 5.3, p < .001) to the fifth quintile of 97.1 cm (WC) (OR: 3.7, p < .001). The ORs for the presence of metabolic syndrome increased abruptly in the fourth quintile, of which the mean WC was 89.6 cm for men and 90.5 cm for women aged 65 to 74 years, and 89.9 cm for men and 87.9 cm for women aged 75 years or older.
Prevalence of the Metabolic Syndrome (MS) According to waist circumference (WC) Category.
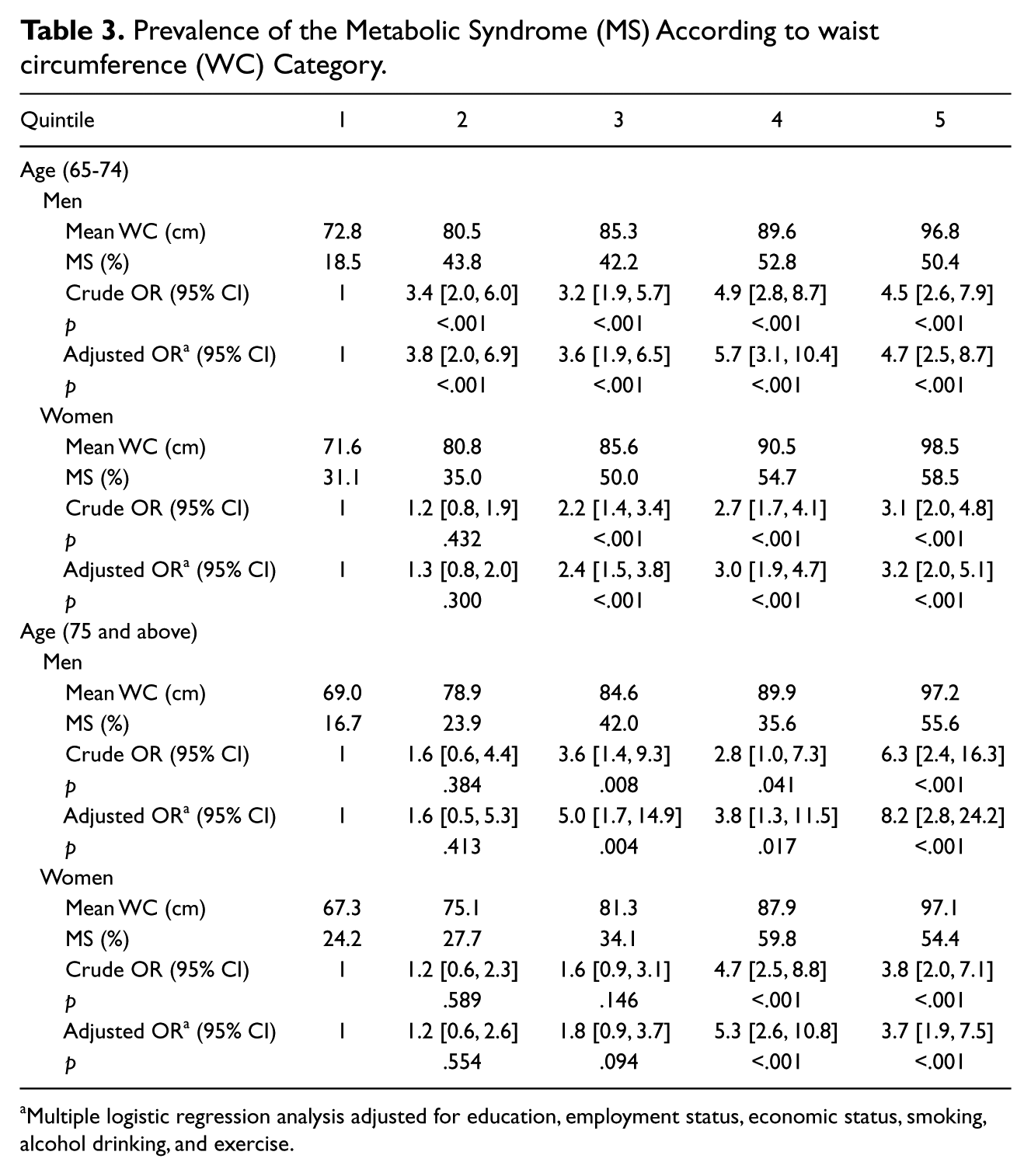
Multiple logistic regression analysis adjusted for education, employment status, economic status, smoking, alcohol drinking, and exercise.
Discussion
Central obesity has been recognized to be an important diagnostic marker for the metabolic syndrome, which is related to cardiovascular disease (Alberti et al., 2006; Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults, 2001; Kim et al., 2009). Among the ways of measuring central obesity, WC, an anthropometric measurement of visceral fat, has been widely used for screening the general population because it is easy, practical, has demonstrated good predictability for visceral fat (Kim et al., 2006; Moon, & Kim, 2005; Pouliot et al., 1994), and has also been demonstrated to be a more predictive measure for disability and mortality in the elderly than any other anthropometric measurement (Guallar-Castillón et al., 2007; Testa et al., 2010; Visscher et al., 2001).
In Korea, 90cm for men and 85cm for women have been widely used for WC cutoff values of central obesity regardless of age, as proposed by the KSSO based on the results of a study conducted on predominantly middle-aged adults (Lee et al., 2007). Compared to the WCs of younger adults, those of older adults show different trends with age according to sex. Younger men generally have a higher WC compared to younger women (Choi et al., 2004; Kim et al., 2006; Moon, & Kim, 2005), but there was virtually no difference for those aged 65 to 74 and only a small difference for those aged 75 and above in this study (Table 2). The results of the latter coincide with previous studies (Kim et al., 2009; Moon, & Kim, 2005; Seo et al., 2009). Increases in intra-abdominal fat accumulation occur first in men, in middle age, then in women, in the postmenopausal period (Kotani et al., 1994; Perissinotto et al., 2002). The increase in WC caused by decreased estrogen levels in postmenopause is profound for Korean women aged 65 to 74. Although the trend of the reduction in WC during aging is similar in both sexes, the decrease in WC is greater for older women aged 75 and above. This result is inconsistent with that of a longitudinal study conducted on another ethnicity; the reduction in fat mass is greater in aging men (Hughes, Frontera, Roubenoff, Evans, & Singh, 2002). A further longitudinal study is necessary to clarify whether this is a Korean ethnic-specific phenomenon.
As for the results of the absolute WC risk of metabolic syndrome in this study, older men were at statistically significant metabolic risk in a lower WC quintile and at greater metabolic risk in the same quintile than older women. Also, the metabolic risks of WC after adjusting health behaviors were higher in older men compared to older women, meaning that the health-related behaviors (especially smoking and alcohol drinking, which were shown to be different at baseline between the sexes [Table 1]) measured in this study affected older men more than women although this effect was not significant statistically. Therefore, older men, even those with a low WC, require further attention regarding the prevalence risk of metabolic syndrome.
On the other hand, older women showed worse baseline clinical data related to metabolic syndrome in this study; older women have high triglyceride levels, HDL-C, and systolic BP, accounting for three of the four predisposing factors for metabolic syndrome. Since the metabolic syndrome is defined as a combination of two or more of the above risk factors but its prevalence of did not differ between the sexes, the metabolic syndrome risk factors seem to cluster more in older women (Gomes, Santos, Christofaro, Santos, & Júnior, 2011; Seo et al., 2009).
These results coincided with previous studies on diverse ethnicities, in that a higher central obesity is prevalent predominantly in women at an older age, affecting the prevalence of metabolic syndrome in older women more so than older men (Regitz-Zagrosek, Lehmkuhl, & Weickert, 2006; Stevens et al., 2010). However, the impact of health behaviors on the prevalence of the metabolic syndrome between the sexes is different depending on ethnicity; health behaviors were shown to not be associated with the prevalence of metabolic syndrome in both elderly Korean men and women in a cross-sectional study (Moon, & Kim, 2005), while another study produced different results (Zhu, St-Onge, Heshka, & Heymsfield, 2004). To utilize health behaviors for the prevention or management of metabolic syndrome in the Korean elderly population, further longitudinal studies on the relationships between health behaviors and the prevalence of the metabolic syndrome according to sexes are necessary.
To determine WC cutoff points for the elderly, this study conducted multiple logistic regression analyses to calculate the absolute risk for metabolic syndrome as well as ROC analyses to maximize sensitivity and specificity. Whereas ROC analyses are the most frequently used methods of calculating optimal cutoff values, they are highly correlated with population means independent of the health outcomes of interest (i.e., metabolic syndrome) and any other contributing factors (i.e., demographic or health behavioral factors; Wang, Ma, & Si, 2010), causing difficulties for predicting health outcomes. Thus, calculating an absolute risk for the health outcome of interest can be an alternative for determining the cutoff values. Most previous studies have proposed their appropriate cutoff values by determining the existence of prominent increases in the absolute risks (Choi et al., 2004; Lee et al., 2007; Wang et al., 2010). On top of abrupt increases in the absolute risks shown, we considered the prevalence of metabolic syndrome defined as a combination of two or more of risk factors, which did not differ between the sexes (Table 2); the 4th quintiles were used uniformly to set WC cutoff points in this study. Thus the WC cutoff points were 89.6 cm for men and 90.5 cm for women who were 65 to 74 years old, and 89.9 cm for men and 87.9 cm for women who were 75 years old or older.
Since 90 cm for men and 85 cm for women, the WC cutoff points for predominantly middle-aged adults suggested by KSSO, were based on the same upper 80th percentile for WC values using KNHANES of 1998 (Lee et al., 2007), different WC criteria should be set for older women. On the other hand, the cutoff values of this study were higher than a previous cohort study of Korean elderly individuals (aged ≥ 63 years), which were 86.5 cm for men and 86.5 cm for women, determined by using the National Cholesterol Education Program (NCEP) Expert Panels on the Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (ATP III) criteria and analyzed by using only the ROC curve (Seo et al., 2009). However, it still showed similar findings as the present studies, in that older men and older women had similar WC cutoff points for estimating metabolic syndrome risk. Although the latter study used a cohort design, it was limited in that they recruited a relatively small number of participants (N = 308 for men and N = 381 for women) from only a region in Korea.
Since we used a cross-sectional sample, this study was limited to estimating different WC criteria in young and elderly participants. To clarify more reliable WC criteria in different age groups, further studies using a longitudinal design in a representative sample of the adult population is needed. On the other hand, a strength of this study is its use of a representative sample of the general Korean elderly population. Thus, it is possible to generalize to the age-specific Korean elderly population.
Therefore, we suggest that WC values of 89.6cm for men and 90.5cm for women aged 65 to 74 years old, and of 89.9cm for men and 87.9cm for women aged 75 years old or older are appropriate cutoff points for central obesity in Korean elderly. This indicates that WC cutoff points for estimating metabolic risk become similar in older men and older women. Age-specific optimal WC cutoff points should be considered in screening for metabolic syndrome.
Footnotes
Authors’ Note
The Korean Centers for Disease Control and Prevention (KCDC) provided the data for this work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This paper was supported by research funds of Chonbuk National University in 2012.