
Abstract
Intimate partner violence, including threats, stalking, emotional, physical, and sexual assault by a spouse or partner, has significant influences on the well-being of women of all racial and social backgrounds. This study of a nationally representative sample of women from varying racial and ethnic groups examined specific types of violent acts on health and well-being. An association between intimate partner violence and poor physical and mental health was found. Types of partner violence also had different associations with the well-being of women of different racial and ethnic backgrounds. Social and demographic factors played an important role in moderating women’s outcomes. Suggestions for future studies are discussed.
Introduction
Intimate partner violence (IPV), defined as single or recurrent acts of threat of violence, and mental, physical, and sexual abuse by a previous or current partner, is a significant and pervasive threat to women’s health (Bell & Naugle, 2008; Campbell, 2002; Coker, Weston, Creson, Justice, & Blakeney, 2005; Tjaden & Thoennes, 2000). Recent estimates suggest that 3 out of 10 women in the United States experience rape, physical violence, and or stalking; and individuals experiencing violence by an intimate partner are vulnerable to a range of negative outcomes (NIPSVS, 2010). As a source of morbidity, intimate partner violence can result in poor quality of life and physical and mental health problems (Azzizz-Baumgarter, McKeown, Melvin, & Dang, 2011; Campbell, 2002). Studies using representative samples are, however, needed to provide more accurate assessments of the health effects of intimate partner violence. Research examining health outcomes of abused women is often gleaned from clinical or community based samples (Basile, Arias, Desai, & Thompson, 2004; Bonomi et al., 2006; Carbone-Lopez, Kruttschnitt, & McMillan, 2006; Lown & Vega, 2001).
Although the risk for poor health outcomes increases among abused women, it is still unclear whether certain acts of violence are more harmful and have lasting effects on some women more than others. In many instances, attention is given to more severe types of violence with minimal attention to minor forms of abuse (Bonomi et al., 2006; Miller, 2006; Pico-Alfonso et al., 2006). Until more recently, the influence of threat of violence and stalking on the well-being of women has rarely been included in analyses. It is necessary to evaluate the specific types of abuse on the well-being of women as different violent acts may affect women in various and differing ways.
An understanding of the effects of intimate partner violence on the well-being of ethnic women is especially warranted. Along with generally higher rates of intimate partner violence, women of color have different social experiences and challenges that may predispose them to poor outcomes at a higher level than women who are not faced with these challenges (Campbell, 2002; Hien & Ruglass, 2009; Kelly, 2010; Lown & Vega, 2001; Tjaden & Thoennes, 2000; Williams, Oliver & Pope, 2008). In particular, women of color are often confronted with poor structural and living conditions, and discriminatory practices that are not only pathways for abuse but sources of stressors that are associated with poor physical and mental well-being (Hummer, 1999; Karlsen & Nazroo, 2002; Murali & Oyebode, 2004; Patel, Bhaju, Thompson, & Kaslow, 2012; Williams, Neighbors & Jackson, 2003). However, the health statuses of abused women of varying ethnic backgrounds remain an understudied area of research (Campbell, 2002; Chen, Rovi, Vega, Jacobs, & Johnson, 2006; Ramos, Carlson, & McNutt, 2004a). This study therefore addresses the influence of specific types of partner violence on the health and well-being of abused women from different racial and ethnic backgrounds.
Background
The relationship between partner violence and women’s health has been well established in the extant literature. Studies have found that abused women are at risk for a myriad of negative physical and mental consequences (Campbell, 2002; Carbone-Lopez et al., 2006; Dutton et al., 2006). According to some studies, physical encounters by an intimate partner can result in bruising, cuts, broken bones, and internal injuries (Crowell & Burgess, 1996; Tjaden & Thoennes, 2000). Women victims of physical partner violence are also susceptible to sexually transmitted diseases (STD), back and limb problems, memory loss and dizziness, and gastrointestinal and stomach conditions (Campbell, 2002; Coker et al., 2005; Dutton et al., 2006; Ellsberg, Jansen, Heise, Watts, & Garcia-Moreno, 2008; Schollenberger et al., 2003). In addition to these known general physical health ailments, intimate victimization can affect reproductive health, leading to miscarriages, gynecologic disorders, unwanted pregnancy, premature labor, and delivery (Carbone-Lopez et al., 2006; Tufts, Clements, & Wessell, 2010).
While physical health outcomes are often most visible, what is not necessarily seen are the mental and psychological effects of abuse on women both long and short-term. A number of studies have indicated that the mental health correlates of partner violence include depression, posttraumatic stress disorder (PTSD), anxiety, controlled substance and alcohol use (Afifi et al., 2008; Bonomi et al., 2006; Caetano & Cunradi, 2003; Campbell, 2002; Coker, et al., 2002; Gleason, 1993; Golding, 1999; Howard, Trevillion, & Agnew-Davies, 2010; McPherson, Delva, & Cranford, 2007; Plichta, 2004). The mental health status of abused victims is further compromised by heightened risk for suicidality and use and abuse of tranquilizers, antidepressant and/or other forms of legal and illegal drugs (Carbone-Lopez at al., 2006; Hedtke et al., 2008; Vive-Cases, Ruiz-Cantero, Escriba-Aguir, & Miralles, 2011). Depression and PTSD however, remain the most common forms of mental health problems associated with intimate partner victimization (Golding, 1999). Among depressed women, approximately 60% were found to have histories of abuse (Dienemann et al., 2000).
Research geared toward understanding how specific types of abuse affect women’s physical and mental health remains limited; in particular, the affects of stalking and threats of violence remain understudied. In some studies certain types of abuse were more closely associated with particular outcomes. For example, increases in rates of depression, anxiety, nightmares, PTSD, and poor self-reported health were found for victims of physical and sexual abuse (Bennice, Resick & Astin, 2003; Bonomi et al 2006; Caetano & Cunradi, 2003; Campbell, 2002; Carbone-Lopez et al., 2006; Coker et al., 2002; Cortina & Kubiak, 2006; Liebschutz et al., 2002; Temple, Weston, Rodriquez, & Marshall, 2007). Notably, higher depression scores were found among abused women victims of sexual abuse than nonvictims (Pico-Alfonso et al., 2006). Among psychologically abused victims of intimate partner violence, depression and anxiety symptomatology were also possible outcomes for certain women (Pico-Alfonso et al., 2006; Temple et al., 2007). Although the health consequences of stalking have only recently been investigated, data suggest an association with depression (Cavanaugh, 2011; Mechanic, Weaver, & Resick, 2008).
Specifically how intimate partner violence affects the well-being of racial and ethnic minority women remains unclear due to a lack of research focus and limited systematic studies (Ramos, Carlson, & McNutt, 2004b; Taft, Bryant-Davis, Woodward, Tillman, & Torres, 2009). While studies in general have provided evidence that intimate partner violence poses a health risk to women of all racial, ethnic, and social backgrounds, the risks may be far greater for some women due to higher incidences of violence compounded with greater exposure to poor life conditions and circumstances and limited access to resources and support networks during times of crisis (Sharps & Campbell, 2006). Women of color in particular have consistently reported higher rates of violence in comparison to white women (Caetano, Schafer, & Cunradi, 2001; Cho, 2011; Field, Caetano, & Nelson, 2004; Hien & Ruglass, 2009; Lipsky & Caetano, 2007; Lipsky, Caetano, Field, & Barargan, 2005; Taft et al., 2009; Tjaden & Thoennes, 2000). Added to increased exposure to violence, racial and structural inequities as well as discriminatory practices experienced by women within these populations have shown to negatively affect their physical and mental states (Fryers, Melzer, & Jenkins, 2003; Hien & Ruglass, 2009; Hummer, 1999; Hunter & Schmidt, 2010; Jackson et al., 1996; Karlsen & Nazroo, 2002; Kessler et al., 1994; Lee, Sanders, Thompson, & Mechanic, 2002; Mays, Cochran, & Barnes, 2007; Murali & Oyebode, 2004; Williams et al., 2003; Yoshihama, Hammock, & Horrocks, 2006). The combination of these factors therefore may increase abused women of color’s risk for poorer physical and mental health outcomes.
In intimate partner violence studies, high rates of depression were found for female Hispanic victims of abuse (Caetano & Cunradi, 2003). Chen and colleagues (2009) reported that among Hispanic women in primary care, approximately two thirds had symptoms of depression, and poor health was associated with all forms of abuse. Poorer self-assessed health status, heart attacks or heart problems, chronic health problems and increased somatic symptoms were also associated with sexually abused Mexican American women (Lown & Vega, 2001). In addition, sexual assault by a current partner was also predictive of PTSD among women within this population (Temple et al., 2007). Kelly (2010) found pain and sleeping difficulty as correlates of various forms of intimate partner violence and sexual abuse among abused immigrant Latinas.
Among Black physically and sexually abused women, depression was a consistent health risk found in studies (Caetano & Cunradi, 2003; Ramon et al, 2004b). Increased substance abuse rates were also evident for physically and sexually abused women (El-Bassel et al., 2003). Moreover, sexual assault by a current partner and nonpartner was predictive of PTSD symptoms for African American women (Temple et al., 2007). Additionally, African American abused women were found to have more health problems on average in each medical and emergency room visit when compared with women who have never been abused (Schollenberger et al., 2003). One study found that African American women reported less symptoms of PTSD in comparison to European American, though depression was a strong predictor for both groups (Lilly & Graham-Berman, 2009).
Although very limited studies have been conducted on abused Asian women (Cho, 2011), there is evidence that suggests women within this population report similar effects of intimate partner violence as other women. For example, U.S. South Asian abused women were significantly more likely than women with no history of intimate partner violence to report poor mental health, anxiety, depression, and suicidal ideation (Himelfarb Hurwitz, Gupta, Liu, Silverman, & Raj, 2006). Battered Chinese descent women victims were also vulnerable to poor mental health outcomes. Positive associations were found between depression and physical and verbal aggression. Associations were also found between somatization and these types of aggression (Yick, Shibusawa, & Agbayani-Siewert, 2003).
Study Aims
The current study builds on previous work by exploring in a nationally representative sample the role of specific types of abuse (i.e., psychological, physical, rape, stalking, and threat of violence) on the health (i.e., perceived general health) and well-being (i.e., alcohol use, substance use, and depression) of women who have been victimized by a current spouse or partner (whether same or opposite sex). This study further evaluates the relationship between intimate partner violence and physical and mental health of women across different racial and ethnic groups.
Method
We analyzed cross sectional data from the National Violence Against Women Survey (NVAWS). The NVAWS was jointly sponsored by the National Institute of Justice (NIJ) and the National Center for Injury Protection and Control (NCIPC), Centers for Disease Control and Prevention (CDC). The study sampled 8,000 women aged 18 years and older across 50 states and the District of Columbia between 1995 and 1996 about their general fears and experiences with violence as an adult and a child. The study used a modified version of the conflict tactic scale (CTS) to estimate violence (Straus, 1979). Random digit dialing procedure was used to generate the sample. Within regional strata, a simple random sample of residential phone numbers was drawn. Telephone interviewing was the primary method of obtaining information on selected participants. Questions were administered both in English and Spanish. To determine representativeness of the sample, demographic characteristics were compared to the general population as measured by the U.S. Census Bureau’s 1995 Current Population Survey and were found to be similar. Due to instances of under and over representation of subgroups, sample weights were considered to correct for possible biases but were not introduced due to the negligible differences in weighted and unweighted prevalence rates of violence (Tjaden & Thoennes, 2000). Overall, the survey yielded a response rate of 72.1%.
Predictor Measures
Controls
The control variables included age, marital status, household income, education, employment status, and race and ethnicity. Age was grouped in five categories (i.e., 18-24, 25-34, 35-44, 45-54, 55 and above). Marital status was coded into three categories: married or common law; divorced, separated or widowed; and single or never married. The educational level of sampled participants was separated into three categories: less than high school, high school, and college (i.e., some college, 4 year college degree and postgraduate). Household income was coded into three categories to reflect low, middle and upper income respondents. The income categories included: less than US$25,000; US$25,000 to US$50,000; and US$50,000 and above. We recognize that these categories overlap; however, this could not be avoided due to the original manner in which the data were collected. Employment status was categorized into two categories: employed (i.e., full-time, part-time, in the military) and not employed (i.e., unemployed/looking for work, retired/not looking for work, homemaker, and student). The racial and ethnic backgrounds of participants were obtained by the question, “Which of the following categories describes your racial background?” Responses included White, Black/African American, Asian/Pacific Islander, American Indian/Alaskan Native and mixed race. To determine the heritage of Latino respondents, participants were asked, “Are you of Hispanic origin?” The response categories included “yes” and “no.” Therefore, participants that self-identified as non-Hispanic White were categorized as White. Non-Hispanic Blacks were categorized as Black. In this study, participants were categorized as Hispanic if they were of Latino origin, irrespective of their race. The “other” category included those participants that self-identified as Asian/Pacific Islander or American Indian/Alaskan Native or mixed race without Latino heritage. Participants not belonging to either of these racial or ethnic categories were excluded from analysis.
Psychological abuse
Psychological abuse was an index of three measures in the survey: Whether a current spouse or partner made them feel inadequate, called them names or put them down in front of others, or shouted or swore at them.
Physical abuse
Physical abuse consisted of a combination of acts that included throw something that could hurt; push, grab, or shove; pull your hair; slap or hit; kick or bite; choke or attempt to drown; hit you with some object; beat up; threaten with a gun; threaten with a knife or other weapon besides a gun; use of gun; or use of knife or other weapons besides a gun.
Rape
An index of five measures was used as markers of rape. Participants were queried about whether a current spouse or partner had ever made them have sex by using force or threat to harm them or someone close; made them have anal sex by using force or threat of harm; made them have oral sex using force or threat of harm; put fingers or objects in their vagina or anus against their will by using force or threats; and attempted to make them have vaginal, oral and anal sex against their will, but intercourse or penetration did not take place.
Stalking
Stalking victims were those who acknowledged that their current spouse or partner (a) followed or spied on them; (b) sent them unsolicited letters or written correspondence; (c) made unsolicited phone calls to them; (d) stood outside their home, school or workplace;(e) showed up at places where they were even though he or she had no business being there; (f) left unwanted items for them to find; (g) tried to communicate with them in other ways against their will; and (h) vandalized their property or destroyed something they loved.
Threat
A single question was provided to respondents about threats by a current spouse or partner. Participants were asked, “Aside from any incidents already mentioned, has anyone else, male or female, ever threatened to harm or kill you?”
Any abuse
Any abuse was a binary composite measure of all the preceding types of abuse discussed (i.e., psychological abuse, physical abuse, rape, stalking, and threat). Participants who experienced any abuse were those who experienced at least one element of the abuse listed.
Outcome Measures
Depressive symptoms
The measures of depressive symptoms in the survey were adopted from the SF-36 Health Survey version 1.0. The SF-36 Health Survey is a multipurpose short health survey that assesses the functional health and well-being of individuals. Questions on the survey included “How often in the past week did you feel full of pep?” “How often in the past week have you been nervous?” “How often in the past week have you felt so down in the dumps that nothing could cheer you up?” “How often in the past week did you have a lot of energy?” “How often in the past week did you feel downhearted and blue?” “How often in the past week did you feel worn out?” “How often in the past week have you been a happy person?” Positive items were reverse coded into negative scales. The items were measured on an ordinal scale (e.g., never, rarely, some of the time, and most of the time). The sum of the individual items yielded an internal consistency of .759 (coefficient alpha) and was averaged for analysis.
Alcohol use
To address the use of alcohol among abused women, respondents were asked the question, “How often did you usually drink any alcohol beverages, including beer, wine coolers, or liquor during the last 12 months.” Possible responses were: everyday, nearly everyday, three or four days a week, one or two days a week, two or three days a month, once a month or less, and never. This measure was coded to reflect those who had ever engaged in such activities as opposed to those who had not (e.g., 0 = never use, 1 = ever use).
Substance use
The substance use indicator included all drugs excluding tobacco and alcohol. An index of “used tranquilizers, sleeping pills or sedatives,” “used uppers, speed or amphetamines,” “used anti-depressants,” “used prescription pain killers,” “used marijuana,” and “used any other recreational drugs, such as crack, heroin, or angel dust” was created for past month substance use. For our analyses, respondents were separated into those that used drugs versus those who did not engage in such activities (e.g., 0 = did not use, 1= used).
General health
The perceived general health of respondents was derived from the following question: “In general, would you say your health is. . . .” Possible answers were as follows: excellent, very good, good, fair, or poor. In line with previous studies (Carbone-Lopez et al., 2006), we dichotomized the health variable to focus on participants with poor health in comparison to those who claim other health statuses (e.g., 1= poor; 0 = good).
Analyses
We used logistic and ordinary least square (OLS) regression analytic procedures to address the bivariate associations. In this study we primarily focused on U.S. women in general, non-Hispanic White, Black, and Hispanic participants. Other subgroups were not examined due to limited cases. The same statistical tests were used for multivariate analyses. In the four multivariate regression models, sociodemographic factors (i.e., age, race, education, income, employment, and marital status) were included as controls. We also conducted analyses on racial and ethnic subgroups. However, all subgroup analyses were not possible because of small sample sizes. In the multivariate analysis we focused on U.S. women in general. Odds ratio, betas, and confidence intervals were reported. Statistical Package for the Social Sciences (SPSS) was used to generate the results. An alpha of .05 was set for significance.
Diagnostics Test
The relationship between abuse indicators (i.e., rape, physical, and psychological abuse) was examined prior to multivariate tests. In the diagnostic test, a low to moderate relationship (e.g., r = 0.0 - 0.5) between indicators were observed, limiting colinearity concerns when these indicators were simultaneously entered in the multivariate models.
Results
Of the participants included in the study 78.3% were White, 9.4% Black, 7.9% Hispanic and 4.3% representing “other” racial and ethnic groups (see Table 1). While participants spread across various age categories, most participants fell within the 55 years and older (26.3%) age group. The vast majority of participants in the sample was either married or in common law relationships (62.9%). The education level of participants was diverse; however, the majority (54.7%) had obtained a college education (i.e., some college, four year degree, postgraduate education), and most (60.7%) participants were employed (i.e., whether part-time, full-time, or in the military). Also, the household income of respondents was commonly between the ranges of US$25,000 to US$50,000 per year (37.2%).
Characteristics of Sample (N = 8000)

Note: Percentages are based on valid cases.
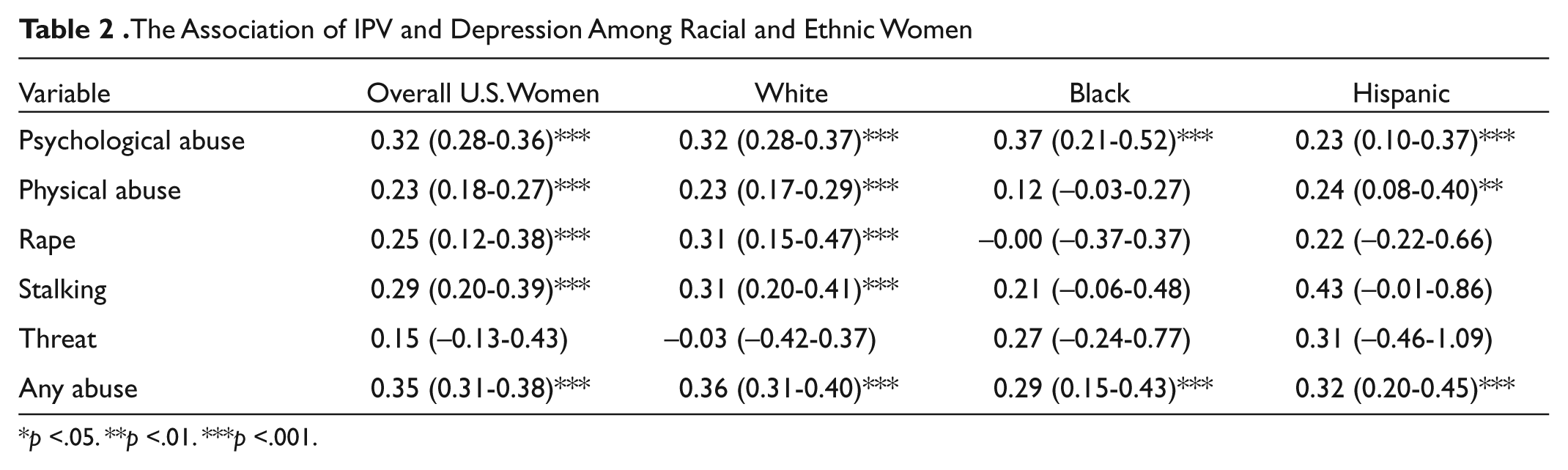
The Association of IPV and Depression Among Racial and Ethnic Women
p <.05. **p <.01. ***p <.001.
Bivariate Analyses
General Health
Table 5 presents the associations between abuse and participants’ perceived general health. Associations were found between specific types of violence and poor health indicator for U.S. women in general. For example, there was more likelihood for poor perceived health when women experienced psychological (OR = 1.76, p < .01) and any abuse (OR = 1.85, p < .01).
Subgroup analyses showed an association between poor perceived health and psychologically abused Hispanic women (OR = 3.09, p < .05), as well as Hispanic women who experienced any abuse (OR = 2.71, p < .05). Among other ethnic women, only physically abused Black victims were more likely to have poor perceived health (OR = 2.89, p < .05).
Alcohol Use
Table 3 shows the association between past 12 months alcohol use for psychologically abused (OR = 1.24, p < .01), physically abused (OR = 1.58, p < .001), stalking victims (OR = 2.05, p < .001) and for women who experienced any abuse (OR = 1.47, p < .001) among sampled U.S. women. In all cases U.S. women who experienced these particular acts of violence increasingly used alcohol. Significant relationships were not found for rape and those women who experienced threats of violence.
The Association of IPV and Alcohol Use Among Racial and Ethnic Women

Note: na means there was insufficient information to fit the model
p <.05. **p <.01. ***p <.001.
Similar results were observed for specific ethnic groups. For example, White, Black, and Hispanic women respectively, used alcohol when they were psychologically abused (OR =1.22, p < .05 vs. OR = 1.91, p < .05 vs. OR = 1.88, p < .05), physically abused (OR= 1.58, p < .001 vs. OR = 2.31, p < .01 vs. OR = 2.44, p < .01) and when they experienced any abuse (OR = 1.41, p < .001 vs. OR = 2.06, p < .01 vs. OR = 2.68, p < .001) with rates increasing across these three types. There were, however, varied ethnic responses in the case of stalking. While associations were found between stalking and alcohol use among White (OR = 1.83, p < .01) and Black women (OR = 4.36, p < .01), this was not the case for Hispanic stalking victims.
Substance Use
As shown by Table 4, there was an association between increased substance use by women victims of psychological abuse (OR = 2.14, p < .001), physical abuse (OR = 1.73, p < .001), stalking victims (OR = 2.16, p < .001) and those that experienced any abuse (OR = 2.86, p < .001).
The Association of IPV and Substance Use Among Racial and Ethnic Women

Note: na means there was insufficient information to fit the model.
p <.05. **p <.01. ***p <.001.
The Association of IPV and Poor Perceived Physical Health Among Racial and Ethnic Women
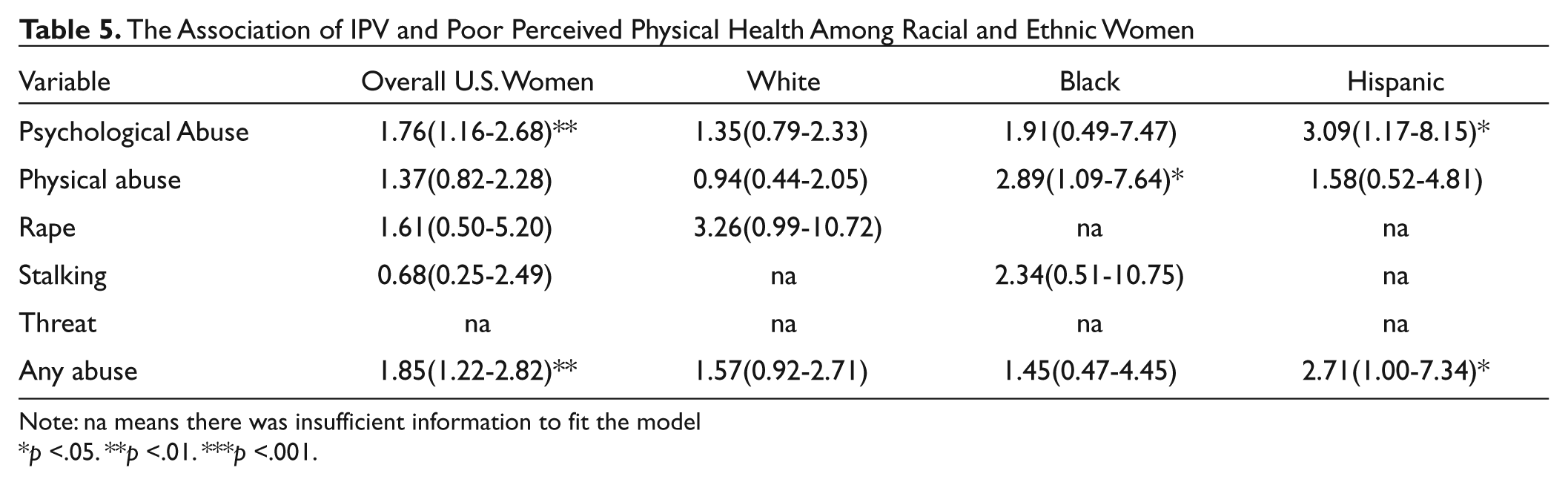
Note: na means there was insufficient information to fit the model
p <.05. **p <.01. ***p <.001.
There were also observed associations in substance use between specific types of abuse among different racial and ethnic group women. This association specifically extended to psychological abuse (OR = 2.02, p < .001), physical abuse (OR = 1.48, p < .01), rape (OR = 2.56, p < .01), stalking (OR=2.11, p < .01) and any abuse (OR=2.59, p < .001) for White women.
Similar to White women, there was greater likelihood for substance use among psychologically abused Black (OR = 2.89, p < .001) and Hispanic (OR = 2.94, p < .001) women. Black (OR = 3.44, p < .001) and Hispanic (OR = 3.61, p < .001) women were also more likely to use substances when they experienced any abuse. Increased risk for substances use were also found for physically abused Hispanic victims (OR= 2.77, p < .001), unlike their Black counterparts.
Depressive Symptoms
As illustrated by Table 2, higher levels of depressive symptoms were observed among U.S. women who experienced psychological abuse (B = 0.32), physical abuse (B = 0.23, p < .001), rape (B = 0.25, p < .001), stalking (B = 0.29, p < .001), and any forms of abuse (B = 0.35; p < .001).
Among racial and ethnic women, increases in depressive symptoms were found for Whites across abuse categories including psychological abuse (B = 0.32, p < .001), physical abuse (B = 0.23, p < .001), stalking (B = 0.31, p < .001), and any forms of abuse (B = 0.36, p < .001). This differed for women of color where increases in depressive symptoms were only found for psychologically abused Black (B = 0.37, p < .001) and Hispanic (B = 0.23, p < .001) women. Black (B = 0.29, p < .001) and Hispanic (B = 0.32, p < .001) women who experienced any abuse were also prone to elevated depressive symptoms. In addition, higher levels of depressive symptoms were found for physically abused Hispanic (B = 0.24, p < .01) victims of abuse.
Multivariate Analysis
The effects of specific incidents of abuse on the well-being of women controlling for possible confounding factors are summarized in Table 6. Two abuse indicators (i.e., threat and stalking) were not included in the first set of regression models due to low endorsement. We were also unable to evaluate the effects of specific abuse on poor perceived health for similar reasons. Nonetheless, the study findings indicate that physically abused women were at increased odds (OR = 1.68, 95% CI [1.11, 2.53]; p < .05) of using alcohol. Similarly, the odds of using alcohol significantly increased when participants were divorced, separated or widowed (OR = 2.89, 95% CI [1.39, 5.98]; p < .05) and among single women (OR = 2.23, 95% CI [1.31, 3.78]; p < .05) compared with married and common law women. Furthermore, there were increased odds of alcohol use for women between the ages of 25 to 34 (OR = 1.64, 95% CI [1.23, 2.19]; p < .001) and 35 to 44 (OR = 1.45, 95% CI [1.09, 1.92]; p < .05) in comparison with older women. There, however, were reduced odds for alcohol use among low (OR = 0.45, 95% CI [0.35, 0.60]; p < .001) to mid income women (OR = 0.65, 95% CI [0.52, 0.81]; p < .001) compared with higher income women. Unemployed women were also at reduced odds (OR = 0.76, 95% CI [0.61, 0.94]; p < .01) of using alcohol compared with employed women. The odds of using alcohol were also reduced for Black (OR = 0.36, 95% CI [0.25, 0.54]; p < .001) and women of other ethnicities (OR = 0.45, 95% CI [0.27, 0.76]; p < .01) when compared with White women.
Multivariate Analysis of Socio-Demographic Characteristics and Specific Types of Intimate Partner Violence Predicting Well-Being
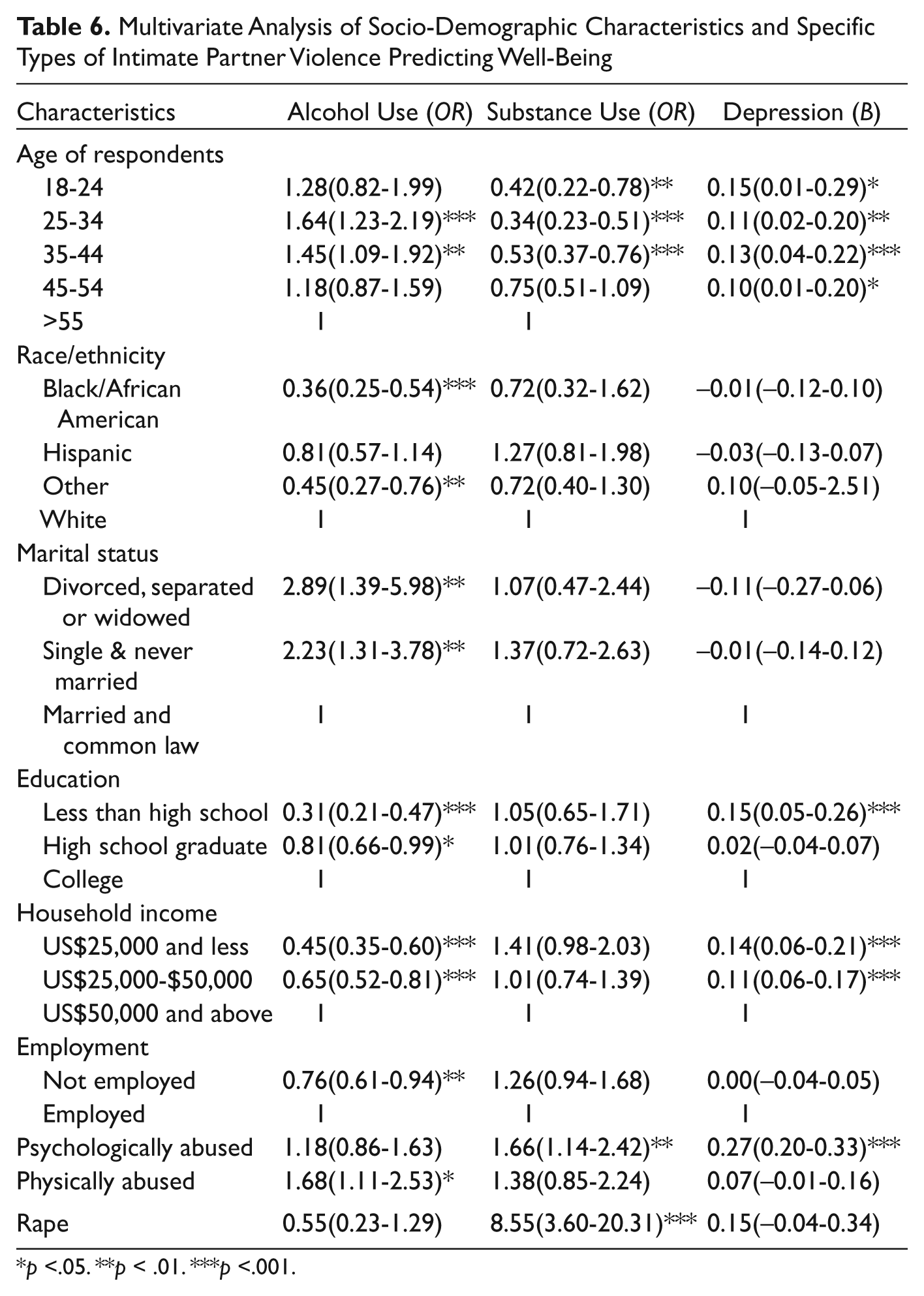
p <.05. **p < .01. ***p <.001.
Psychologically abused women (OR = 1.66, 95% CI [1.14, 2.42]; p < .01) and rape victims (OR = 8.55, 95% CI [3.60, 20.31]; p < .001) were also at greater odds for substance use. The odds of using substances were reduced in certain age groups. Specifically, there were lower odds for substance use for women between the ages of 18 to 24 (OR = 0.42, 95% CI [0.22, 0.78]; p < .01), 25 to 34 (OR = 0.34, 95% CI [0.23, 0.51]; p < .001), and 35 to 44 (OR = 0.53, 95% CI [0.37, 0.76]; p < .001) in comparison with older women.
The study findings also showed higher levels of depressive symptoms for psychologically abused women (B = 0.27, 95% CI: [0.20, 0.33]; p < .001) when other factors were controlled. These increases in level of depression were also observed for low (B = 0.14, 95% CI: [0.06, 0.21], p < .001) and mid (B = 0.11, 95% CI: [0.06, 0.17]) income level women, as well as women with less than a high school education (B = 0.15, 95% CI: [0.05, 0.26]; p < .001). These relationships were also found for women of certain age groups: 18 to 24 (B = 0.15, 95% CI [0.01, 0.29]; p < .05), 25 to 34 (B = 0.11, 95% CI [0.02, 0.20]; p < .01), 35 to 44 (B = 0.13 95% CI [0.04, 0.22]; p < .001) and 45 to 54 years old (B = 0.10, 95% CI [0.01, 0.20]; p < .05).
In the final set of multivariate models, we examined the index of any abuse (i.e., psychological, physical, rape, threat, and stalking) on the well-being of women (see Table 7). The analyses show a similar pattern to results of the models that examined specific types of violence. According to the findings, there were increased odds for alcohol use (OR = 1.51, 95% CI [1.23, 1.85]; p < .001) when women experienced any form of abuse. Subsequent findings indicate greater odds for alcohol use for women in different age categories including 18 to 24 (OR = 1.81, 95% CI [1.18, 2.76]; p < .05), 25 to 34 (OR = 1.74, 95% CI [1.30, 2.34]; p < .001) and 35 to 44 (OR = 1.42, 95% CI [1.07, 1.89]; p < .05) when compared with older women. Divorced, separated or widowed respondents (OR = 1.83, 95% CI [1.11, 3.04]; p < .05) were also at increased odds for alcohol use in comparison to married women. Conversely, the odds of using alcohol were significantly reduced for women with less than a high school education (OR = 0.48, 95% CI [0.33, 0.69]; p < .001) in comparison with college-educated women. Lower odds of alcohol use were also found among Black (OR = 0.41, 95% CI [0.29, 0.58]; p < .001) and “other” women (OR = 0.42, 95% CI [0.26, 0.69]; p < .001) when compared with Whites. The same was true for low (OR = 0.42, 95% CI [0.32, 0.55]; p < .001) and mid (OR = 0.61, 95% CI [0.49, 0.76]; p < .001) income women as well as not employed (OR = 0.78, 95% CI [0.64-0.97]; p <. 05) women who were at reduced odds for alcohol use.
Multivariate Analysis of Socio-Demographic Characteristics and Any Abuse Predicting Well-Being
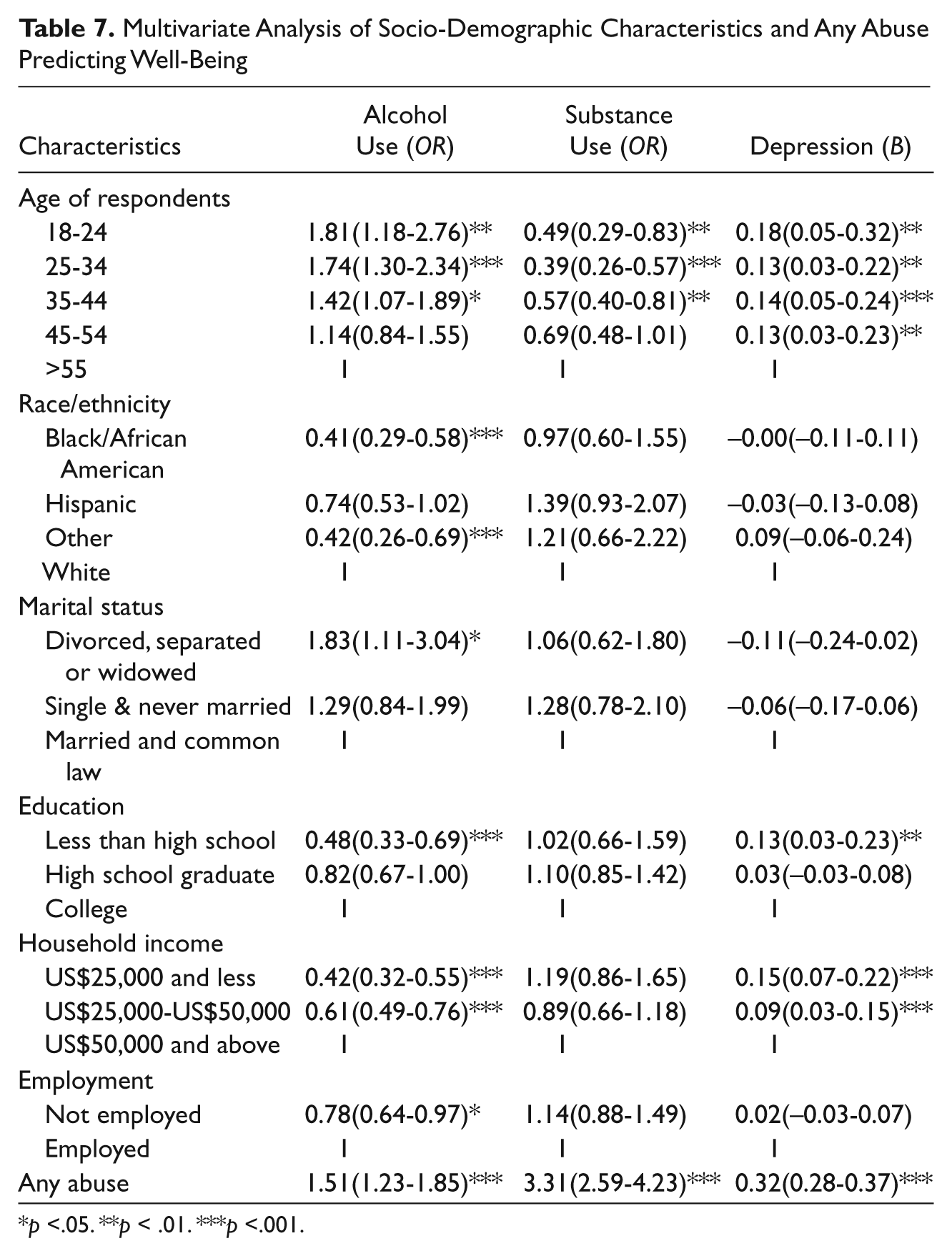
p <.05. **p < .01. ***p <.001.
Women experiencing any form of abuse were also at greater odds (OR = 3.31, 95% CI [2.59, 4.23]; p < .001) for substance use. Among women in the sample, the odds for substance use was reduced for women between the ages of 18 to 24 (OR = 0.49, 95% CI [0.29, 0.83]; p < .01) 25 to 34 (OR = 0.39, 95% CI [0.26, 0.57]; p < .001), 35 to 44 and (OR = 0.57, 95% CI [0.40, 0.81]; p < .01).
The multivariate findings provided additional evidence of relationships between any form of abuse and depressive symptoms (B = 0.32, 95% CI [0.28, 0.37]; p < .001) when other factors were controlled. The relationship further extends to the age, education, and income of the woman. In particular, there were increases in depressive symptoms for women between the ages of 18 to 24 (B = 0.18, 95% CI [0.05, 0.32]; p < .01), 25 to 34 (B = 0.13, 95% CI [0.03, 0.22]; p < .01), 35 to 44 (B = 0.14, 95% CI [0.05, 0.24]; p < .001) and 45 to 54 (B = 0.13, 95% CI [0.03, 0.23]; p < .01). Increases in depressive symptoms were further found for low (B = 0.15, 95% CI [0.07, 0.22]; p < .001) and mid (B = 0.09, 95% CI [0.03, 0.15]; p < .001) household level income women. Women with high school and less education (B = 0.13, 95% CI [0.03, 0.23]; p < .01) also had an increase in depressive symptoms when compared to their counterparts.
Discussion
The primary goal of this study was to explore the effects of specific incidences of abuse by a current spouse or partner on the health and well-being of women. We also examined ethnic variation across various subgroups in the health outcomes of abused women. Our bivariate findings indicate that women in general were adversely affected by intimate partner violence. In general, U.S. women that experienced various forms of abuse were more likely to report alcohol use, substance use, depressive symptoms, and poor physical health. In all cases, however, we did not find such association between threat of violence and women’s well-being. This possibly could be the result of low frequency of agreement for this abuse indicator. There were also differences in association in health outcomes on the basis of race and ethnicity for victims of intimate partner violence. Poor perceived general health was associated with psychological and any abuse for Hispanic women but not for Black and White women; physical abuse was further associated with this outcome for Black women but not other women. In addition, there was a relationship between various types of abuse and substance use for White women. This was different for women of color where physical abuse and stalking was not associated with substance use for Black women. Among Hispanic women, rape and stalking were also not related to substance use. Furthermore, specific types of violence such as rape and stalking were associated with depression for White women, but not for Hispanic and Black women. However, alcohol use was related to various kinds of abuse with the exception of rape and threat of violence for all women examined.
Adjusting for sociodemographic factors, there was further evidence pointing to the adverse effects of specific types of violence on the well-being of women. Particularly, women who experienced physical abuse were more vulnerable to alcohol use; psychologically abused women were at greater risk of substance use and depressive symptoms; and rape victims had increased substance use. In addition, women who experienced a combination of these types of abuse were also vulnerable to these outcomes. The immediate effect of violent acts quite possibly could cause some women to develop depressive symptoms. Along with this resulting effect, alcohol and substance use may be methods of coping with the abuse (Kilpatrick, Acierno, Resnick, Benjamin & Best, 1997). The study findings further suggest that social and demographic factors (e.g., age, race, marital status, education, income) contribute to women’s health outcomes. These results support previous findings while expanding knowledge about the relationship between specific types of intimate partner violence (Bonomi et al., 2006; Gleason, 1993; Golding, 1999).
In spite of these findings, there were several limitations to the study. First, the study was based on cross-sectional data, limiting any causal inferences. Thus, it could not be determined whether women’s outcomes were directly attributed to violence in the relationship or to other factors. Quite possibly, the abused victims may have already had poor health prior to her relationship with her current spouse or intimate partner. Comparative and longitudinal studies are needed to provide a better understanding. Second, we were limited by sample size, which limited analyses that would assist in fully addressing the research aims. Sample size also made it less possible to understand the relationships of types of violence and well-being among specific subpopulations within the sample. Finally, the sample was limited to few possible subjective health measures that victims of intimate partner violence are vulnerable to. Additional health measures using structured clinical tools are needed in future studies to provide more accurate assessments of the resulting effects of intimate partner violence.
Even with these limitations, the study enhances knowledge about possible outcomes of victims of intimate partner violence through use of nationally representative data. The study also addressed some of the gaps in the research on women of color and provides clarification on how different social and demographic groupings of women are affected by specific types of violence. However, limited sample sizes across racial and ethnic groups prevented us from fully examining the association between various types of violence and women’s health outcomes. This was more true for groups that are understudied in domestic violence research (i.e., Blacks, Hispanic, Asian/Pacific Islander, American Indian/Alaskan Native).
In sum, the results of this study suggest that different physical and mental health outcomes may be linked differentially across various types of abuse in different subgroups of women. Practically, this has implications not only for increased understanding of the etiology of abusive relationships, but may have significant implications for designing effective interventions and programs to prevent and treat the consequences of domestic abuse. Future studies should further aim to understand the influence of social and contextual factors in intimate partner violence, and the role these factors play in women’s health and overall well-being. Finally, this study also reveals the need for larger national samples of diverse racial and ethnic groups to fully understand the substantive meanings and intervention implications of these observed relationships.
Footnotes
Acknowledgements
The authors would like to thank Ms. Nidhi Talwar, Dr. James S. Jackson, and Dr. Daniel G. Saunders for their helpful insight on the direction of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Bios