
Abstract
Persons with disabilities make up some 15% of the world’s population and are at higher risk of violence. Yet there is currently no systematic review of the effectiveness of interventions to prevent violence against them. Thus the aim of this review was to systematically search for, appraise the quality of, and synthesize the evidence for the effectiveness of interventions to prevent and mitigate the consequences of all the main forms of interpersonal violence against people with all types of disabilities. The method used consisted of searches of eleven electronic databases, hand searches of three journals, scanning of reference lists of review articles, contact with experts, appraisal of risk of bias using the Quality Assessment Tool for Quantitative Studies, and narrative synthesis of results. This resulted in 736 titles being identified, 10 of which met the inclusion criteria and 6 and 2 addressed people with intellectual disabilities and developmental disabilities, respectively. Only one was from a low- and middle-income country. All studies received a weak rating on the quality assessment tool and none could be considered effective after taking risk of bias into account. In sum, the current evidence base offers little guidance to policy makers, program commissioners, and persons with disabilities for selecting interventions. More and higher quality research is required, particularly from low- and middle-income countries and on other forms of disability such as physical impairments, sensory impairments, and mental health conditions.
Introduction
There is growing awareness that persons with disabilities constitute a significant minority—around 15% of the world’s population (World Health Organization [WHO], 2011)—who experience disadvantages in many domains of life. According to recent systematic reviews published in The Lancet (Hughes et al., 2012; Jones et al., 2012), persons with disabilities are at higher risk of experiencing violence. The increased risk of persons with disabilities of having experienced violence in the last year for adults is approximately 50%, with adults with mental health conditions being at nearly four times higher risk. Children with disabilities are more than three times more likely to have experienced violence in their lives than non-disabled children. The majority of studies included in these systematic reviews derive from high-income countries, and there is a lack of high-quality research from low- and middle-income countries. However, the available information suggests that the problem is also widespread in such countries (CREA, 2012; Human Rights Watch, 2005; Mohapatra & Mohanty, 2004; Ortoleva & Lewis, 2012).
Article 16 of the United Nations Convention on the Rights of Persons With Disabilities (2008) mandates States Parties to “take all appropriate legislative, administrative, social, educational and other measures to protect persons with disabilities, both within and outside the home, from all forms of exploitation, violence and abuse, including their gender-based aspects.” While awareness of the extent of the problem of violence against persons with disabilities is growing, research on the effectiveness of prevention strategies is still limited. Several publications highlight the importance of better prevention of violence against people with disabilities. Most, however, focus on broad policy and legal recommendations or provide good practice suggestions, the effectiveness of which is more difficult to rigorously evaluate than more circumscribed interventions (e.g., Gravell, 2012; Northway, Davies, Mansell, & Jenkins, 2007; Perry, 2004; Quarmby, 2011; Robinson & Chenoweth, 2011).
Several practice guides recommend ways of preventing abuse against children with disabilities. Protecting Children With Disabilities From Sexual Assault: A Parent’s Guide presents various strategies for parents to prevent sexual abuse of children but provides no evidence that these strategies are effective (Davis & Modell, 2010). AIAS Bologna Onlus (2004) released a booklet, Childhood, Disability & Violence, aiming to raise awareness regarding the importance of violence against children with disabilities. Alongside more specific recommendations, there are also general calls for greater funding to make services more accessible (Chang et al., 2003; Phipps, 2012).
Several previous reviews of interventions to prevent violence against people with disability have been conducted. Most do not focus primarily on the effectiveness of the interventions; few are systematic reviews; and none addresses all types of interventions to prevent all forms of violence against people with all forms of disabilities. For example, Lund (2011) focuses on community-based services and interventions for adults with disabilities who have experienced interpersonal violence and aims to identify and describe existing services and examine their nature and accessibility, in addition to reviewing those which have been evaluated. Barger, Wacker, Macy, and Parish (2009), in a “comprehensive” review, focus on sexual abuse prevention strategies for women with intellectual disabilities with the aim of determining the scope and nature of available programs, as well as reviewing their effectiveness. Mahoney and Poling (2011) examine the prevalence of sexual abuse against people with severe developmental disabilities as well as prevention strategies for this population; however, their review is neither systematic nor does it focus on the effectiveness of the strategies. Moore (2001) provides a “selective review” of literature concerning abuse of adults with learning disability by those employed to care for them, which only mentions the effectiveness of interventions. Doughty and Kane (2010) review studies on teaching abuse-protection skills to people with intellectual disabilities: Again, this review is not systematic, and focuses more on the nature of the interventions than on their effectiveness. A recurrent theme throughout all these reviews is the paucity of evaluations of interventions to prevent violence against people with disabilities. Thus, to date no previous review has systematically searched for, appraised the quality of, and synthesized the evidence for the effectiveness of all different types of interventions to prevent and mitigate the consequences of all forms of violence against people with all forms of disability. The current review aims to address this gap.
By doing so, this review also seeks to strengthen the public health approach to preventing violence against people with disability. Such a public health approach begins with understanding the magnitude, distribution, and the consequences of the problem: Some progress has been made on this question, most notably in the two recent meta-analyses on the prevalence of violence against children and adults with disabilities (Hughes et al., 2012; Jones et al., 2012). The second step involves the identification of risk and protective factors for, and underlying causes of, violence against persons with disabilities, in particular those that are modifiable—an area which remains under-researched in relation to violence against people with disabilities. The third step of the public health approach, and the focus of the current review, concerns the development and rigorous evaluation of strategies to prevent, and mitigate the consequences of, violence against persons with disabilities. The final step is to scale up those strategies that have been proven effective and evaluate their cost-effectiveness (Krug, Dahlberg, Mercy, Zwi, & Lozano, 2002).
Method
Eligibility criteria for this review were that studies evaluated the effectiveness of all types of universal, selected, and indicated interventions to prevent all the main form of interpersonal violence (i.e., child maltreatment, youth violence, intimate partner violence, sexual violence, and elder maltreatment—see Table 1 for definitions) against people with all the main forms of disabilities (physical impairments, sensory impairments, mental health conditions, and intellectual impairments) compared with either no intervention or services as usual, using outcomes that are both distal (measures of risk factors for violence) and proximal (measures of actual violence) based on all types of study designs, except for surveys of participants’ satisfaction. Studies had to be published between January 2000 and August 2011 in any language either in peer-reviewed journals or as reports in the gray literature.
Definitions of the Main Types of Interpersonal Violence (World Health Organization, 2013).

Information sources used to identify studies consisted of electronic databases (Cochrane, Medline, EBSCO, PsychINFO, Social Care Online, Google Scholar, NCJRS, Sociological Abstracts, Popline, Web of Knowledge, and the WHO Regional Databases); hand searches of journals since January 2000 (Disability and Society, Journal of Interpersonal Violence, and Child Abuse and Neglect); reference lists of review articles; and 12 international experts (from Canada, South Africa, Thailand, the United Kingdom, and the United States) who were e-mailed the list of studies identified and asked to suggest any others they may be aware of. These were selected from the network of experts in disability and violence prevention maintained by the WHO’s Department of Violence and Injury Prevention and Disability who had specific expertise in the area of prevention of violence against persons with disability in different regions of the world.
Search terms used included “violence,” “crime,” “abuse,” “assault,” “neglect,” “prevention,” “intervention,” “training,” disabled persons,” “people with disabilities,” “blind,” “deaf,” and other cognates and synonyms of these terms. The search terms used to identify relevant studies were adapted for use in the different databases and duplicates were removed. No language restrictions were applied. The full search strategy is available on request.
Study selection was carried out by one reviewer, with a second reviewer assessing a sub-sample. Doubts and disagreements were resolved by consensus among the three reviewers.
A data extraction form was developed and pilot tested on the full sample of 10 studies and subsequently refined. Data were extracted independently by two of the review authors and disagreements were resolved by discussion among the three review authors. No authors were contacted for further information. Data were extracted from each included study on number and characteristics of participants in the intervention and control groups (including country, sex, age, type of disability), type of intervention (including the types of violence it aimed to prevent; method of delivery; content; and whether universal, selected, or indicated), study design (using the typology of the Quality Assessment Tool for Quantitative Studies−Effective Public Health Practice Project [QATQS-EPHPP, 2013]), outcomes measures (including type, reliability and validity data, whether distal or proximal), results by outcome, as well as all other data required to apply the QATQS. All outcomes in the studies relevant to preventing violence—both proximal and distal—or mitigating its consequences for which results were reported were included.
To assess risk of bias in individual studies, the QATQS (EPHPP, 2009; see also Armijo-Olivo, Stiles, Hagen, Biondo, & Cummings, 2012) was applied by two review authors and the only minor disagreement that arose was resolved by discussion among them. This tool assesses outcome evaluations using all types of study design on selection bias, study design, confounders, blinding, data collection methods, and withdrawals and drop outs. Studies are considered “strong” if they receive no weak ratings on any of these components; “moderate” if they receive one weak rating; and “weak” if they receive two or more weak ratings. In addition, risk of bias was also assessed by examining if outcome measures were distal (e.g., risk factor for violence) or proximal (a measure of actual violence), as it is known that score changes on risk factors for violence do not always correspond to the likelihood of future abuse (e.g., Albarracin et al., 2003; Chaffin & Valle, 2003; Webb & Sheeran, 2006).
No single quantitative summary measure of treatment effect was used for all studies nor was a meta-analysis conducted. Significant differences in the characteristics of the populations (e.g., types of disability), interventions (including the type of violence they aimed to prevent), and outcomes used in the studies meant that comparison of summary measures of effect size and calculation of an overall average effect size across studies would have made little sense. Instead, narrative synthesis has been used.
The summary assessment of effectiveness of each intervention was performed in two stages—first without taking the assessment of risk of bias into account and, second, taking it into account. In the first stage, we judged the findings of a study to be “effective,” if there were statistically significant differences on the outcomes relevant to violence measured; “unclear,” if there was a balance of statistically significant differences and absence of differences on violence-related outcomes or if the there was insufficient information to make a determination; and “ineffective,” if there was no statistically significant differences on most of the violence-related outcomes. In the second stage, if the QATQS rating was “weak,” the summary assessment was downgraded from “effective” to “unclear” or from “unclear” to “ineffective.”
Results
Of the 736 initial publications identified, 10 publications were eligible for inclusion (see Figure 1) which reported the results of 10 separate studies evaluating the effectiveness of prevention or victim support programs.
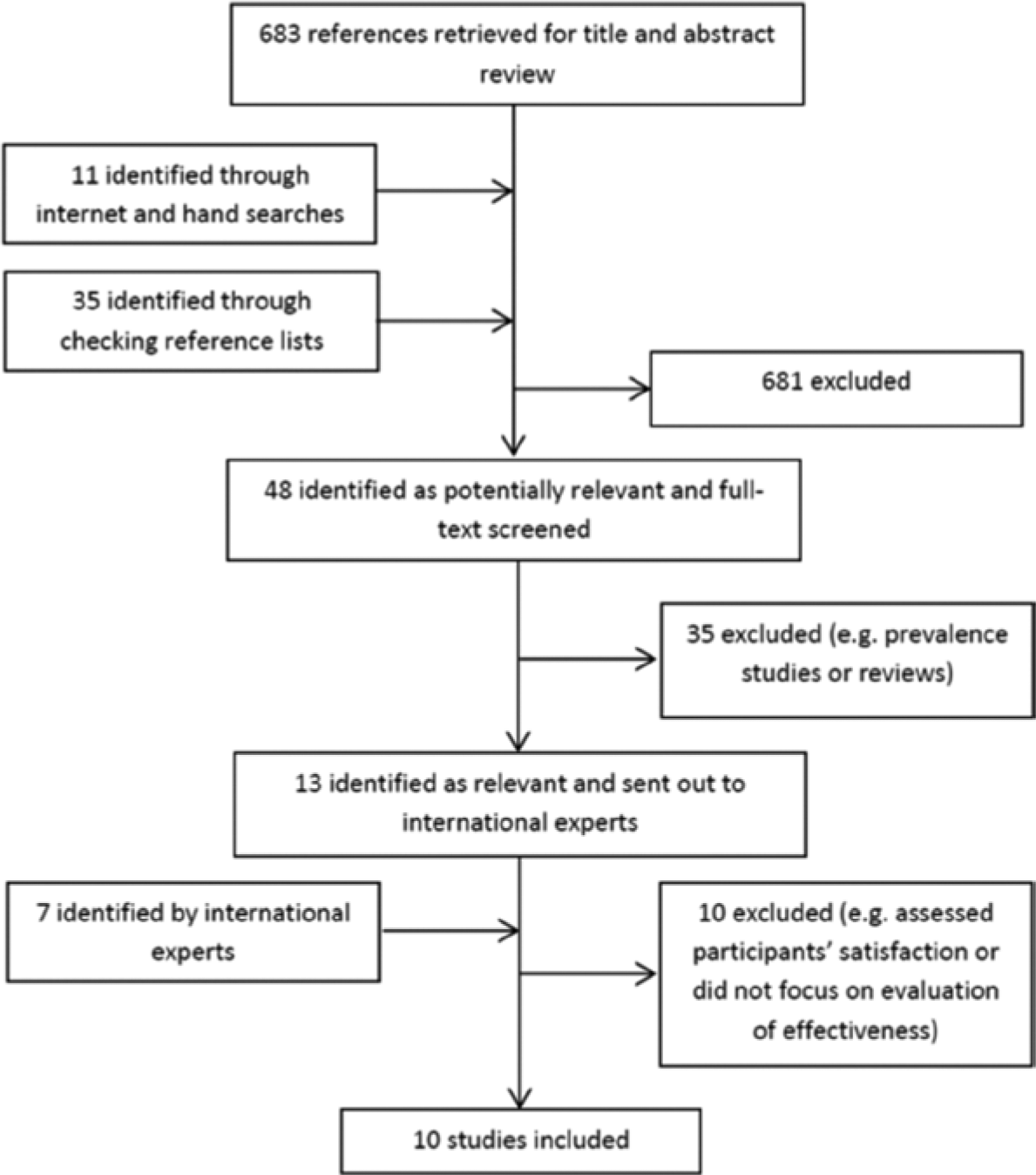
Flowchart of selection of studies.
Study Characteristics
Study participants
Sample sizes varied from 7 to 329 (Table 2), with a mean sample size of 95.4. Two of the studies (Mazzucchelli, 2001, and Peckham, Howlett, & Corbett, 2007) pointed out that their sample sizes were too small and that they probably lacked sufficient statistical power to detect effects had they been present. None of these studies, however, reports having performed power and sample-size calculations. Six of the studies included people with intellectual disabilities (including mental retardation); two, with developmental disabilities; two, with different types of disability; and one study did not specify the disability type (Table 2).
Characteristics of Studies.
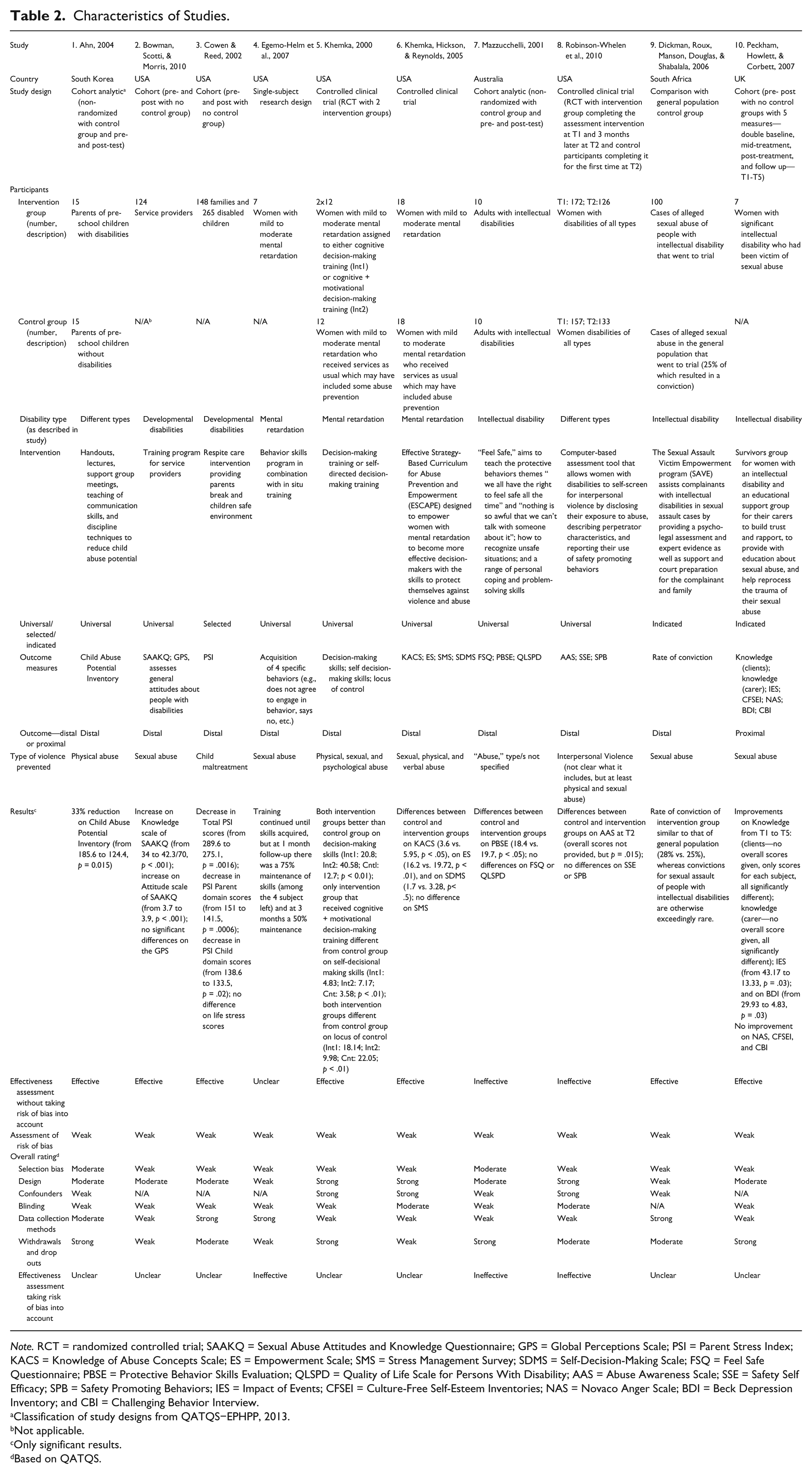
Note. RCT = randomized controlled trial; SAAKQ = Sexual Abuse Attitudes and Knowledge Questionnaire; GPS = Global Perceptions Scale; PSI = Parent Stress Index; KACS = Knowledge of Abuse Concepts Scale; ES = Empowerment Scale; SMS = Stress Management Survey; SDMS = Self-Decision-Making Scale; FSQ = Feel Safe Questionnaire; PBSE = Protective Behavior Skills Evaluation; QLSPD = Quality of Life Scale for Persons With Disability; AAS = Abuse Awareness Scale; SSE = Safety Self Efficacy; SPB = Safety Promoting Behaviors; IES = Impact of Events; CFSEI = Culture-Free Self-Esteem Inventories; NAS = Novaco Anger Scale; BDI = Beck Depression Inventory; and CBI = Challenging Behavior Interview.
Classification of study designs from QATQS−EPHPP, 2013.
Not applicable.
Only significant results.
Based on QATQS.
Interventions
There were seven universal, one selected, and two indicated prevention interventions. The content of the interventions varied, ranging from respite care for carers, through training programs for service providers, to survivor groups and educational workshops for the carers of survivors. Four of the studies targeted sexual abuse; three, different types of abuse; one, physical abuse; one, all forms of child maltreatment; and one did not specify the type of abuse.
Country of study
Nine out of 10 studies were conducted in high-income countries—6 in the United States; 1 in the United Kingdom and Australia, respectively; and 1 in the Republic of Korea—and 1 in an upper-middle income country—South Africa.
Assessment of Risk of Bias
All studies received an overall rating of “weak” on QATQS. Not one study was rated as “strong” on selection bias and 70% of studies were rated “weak” on 50% or more of the six dimensions of QATQS.
Study designs
Three of these studies used randomized controlled designs; two, non-randomized designs with control groups and pre- and post-measures; one, non-randomized design, using a general population control group; three, designs with no control groups but pre- and post-measures; and one, a single-subject designs, with seven subjects (see Table 2).
Outcome measures
In only four studies were the outcome measures clearly supported by some evidence of validity (including face or content validity), and in seven studies they were supported by evidence of reliability. None of the eight studies evaluating the effectiveness of universal or selected interventions to prevent violence used a proximal outcome measure (i.e., a measure of actual violence). Instead they used measures of risk or protective factors for violence—such as measures of child abuse potential, sexual abuse attitudes, or evaluation of protective behavior skills.
Effectiveness of Interventions
Of the 10 interventions evaluated and not taking risk of bias into account, 7 were judged to be “effective,” 1 to have “unclear” results, and 2 to be “ineffective.” However, once risk of bias was taken into account, and effectiveness downgraded if studies were found to be “weak” on QATQS, no intervention remained “effective”: six were “unclear” and three, “ineffective.”
Discussion
The systematic search for evaluations of the effectiveness of interventions to prevent violence against persons with disabilities and mitigate its consequences identified 10 studies that met the inclusion criteria. Seven of them were evaluation of universal interventions. The content of the interventions and the type of violence targeted varied considerably. All but one study came from high-income countries and most focused on people with intellectual or developmental disabilities. All studies were judged to be at a high risk of bias: All were assessed as “weak” on the QATQS (QATQS-EPHPP, 2013). All measured risk factors for violence rather than actual violence as outcomes. When risk of bias was taken into account, not a single intervention was considered to be effective
Current evidence summarized in this review on the effectiveness of interventions to prevent and respond to violence against persons with disabilities only offers limited guidance to practitioners, policy makers, and persons with disabilities themselves. Despite deliberately broad criteria, the review identified only 10 studies that met its inclusion criteria and these studies reveal major gaps in the literature including the range of disabilities included—none focused on mental illness, physical, or sensory impairments; geographical regions—only one study comes from an upper-middle income country and none from a low-income country; and types of violence—none addressed neglect or institutional violence.
“Neglect” was included as a type of violence in our search terms but yielded no relevant results, yet children (<18 years of age) with a disability have been shown to be at a 4.56 higher risk of neglect than children without a disability (Jones et al., 2012). Our search found one result focusing on responses to violence in institutions, but it failed to meet the inclusion criteria (Robinson & Chenoweth, 2011). A UNICEF report on violence against disabled children confirmed that violence in institutions is particularly widespread, which may imply that deinstitutionalization would be an appropriate violence prevention strategy, but none of the studies focused on this area (UNICEF, 2005). The UNICEF report also highlights the prevalence of neglect in institutions. More research is needed on both these forms of violence against persons with disabilities.
For those types of disabilities addressed by these 10 studies, mainly intellectual and developmental disability, findings are weakened by a high risk of bias which further limits their usefulness as guidance. All studies were rated as “weak” on QATQS; none used a measure of actual violence as an outcome; and none provided calculations of sample size and statistical power, although 6 out 10 had total samples of less than 50. The absence of the use of measures of actual violence (either self-reported or from police, social work, or other official records) is probably due to the small sample sizes and relatively short follow-up periods used in these studies, and perhaps also due to the reluctance on the part of disabled people to divulge violence perpetrated by caregivers. The use of measures of actual violence would require much larger samples with longer follow-up periods, as violence is a relatively low-frequency occurence. Nonetheless, this limited evidence base can be viewed as a starting point from which to further research and evaluation of those interventions that appear promising.
A word is required, however, on how this much-needed research should be conducted. Since 1990, a vigorous disability rights critique of traditional research on disability has become evident. Rather than neutral, detached, positivist investigations, conducted predominantly by non-disabled people, scholars such as Oliver (1992) have stressed the potential of emancipatory research, managed by disabled people and conducted according to the social model of disability (Oliver, 1990). Other scholars have worked to empower people with intellectual disabilities and involve them fully in studies which concern them (Walmsley & Johnson, 2003). Emancipatory research paradigms aim not simply to understand, but also to improve the lives of disabled people. On the face of it, these approaches would appear to be in contradistinction to the public health emphasis on evidence-based policy, drawing usually on large-scale quantitative studies following clear criteria for scientific quality. Emancipatory research has proven more effective in giving voice to disabled people’s concerns than in shaping policy in the area of violence and hate crime (Roulstone & Mason-Bish, 2013, Shakespeare, 2013). Moreover, particularly in developed countries such as the United Kingdom, public health research and other health services research increasingly prioritizes “patient and public involvement” (Edwards & Elwyn, 2009). Where genuine, the resulting participation by disabled people in research has the potential to neutralize the disability rights critique and conform to the principles underlying emancipatory research.
Unlike previous reviews which mostly focused on persons with intellectual disabilities and specific types of violence (Barger et al., 2009; Doughty & Kane, 2010; Mahoney & Poling, 2011; Moore, 2001), this review included all forms of disabilities and types of violence. But, much like previous reviews, this review identified few studies. Barger et al. (2009) found only five articles in their review of research focusing on reducing sexual assault against women with intellectual disabilities. Doughty and Kane (2010) found six. Lund (2011), with broader criteria for inclusion, found 16. Lund who focused on community-based services and interventions for adults with all forms of disability who have experienced interpersonal violence, found, like this review, that research into sexual abuse against persons with intellectual disabilities dominated. The background literature shows that persons with intellectual disabilities are more at risk of violence and consequently a greater number of programs cater to this group. Like the current review, previous reviews are dominated by findings from the United Kingdom and United States.
This review has several limitations. First, while we did not apply any language restrictions in our search strategy, we did not search databases in other languages and have only one result in another language (Ahn, 2004 in Korean, which we had translated). Second, assessment of study eligibility was performed by one reviewer only, with a sub-sample checked by a second reviewer, potentially reducing the reliability of these assessments. Third, no uniform quantitative summary measure of treatment effect was used for all studies nor was a meta-analysis conducted, due to the extensive heterogeneity of types of disability, violence, and interventions, and of outcomes used in the studies included. Instead, a two-stage process of judgment, which incorporated risk of bias in the second stage, was used.
Conclusion
Violence against children and adults with disabilities is highly prevalent and represents a major human rights violation and public health problem. Yet, this review found only 10 studies that met its inclusion criteria, which were deliberately set broadly. It reveals major gaps in the research on interventions to prevent violence against persons with disabilities and highlights the serious methodological weakness of the studies included.
One option to strengthen the evidence base in this area is to test existing violence prevention strategies to see if they work for persons with disabilities. It is plausible that interventions of proven effectiveness in reducing violence against non-disabled adults and children might also be applicable to disabled people. The WHO publication Violence Prevention: The Evidence (WHO, 2009) reviews seven main strategies, with some evidence of effectiveness, for the prevention of interpersonal violence. These include, for instance, developing safe, stable, and nurturing relationships between children and their parents and caregivers; developing life skills in children and adolescents; reducing the availability and harmful use of alcohol; promoting gender equality to prevent violence against women; and changing cultural and social norms that support violence. Parenting programs such as the Positive Parenting Program (Triple P, 2013) or the home visiting program, the Nurse Family Partnership (NFP; 2013) have been shown to be effective for preventing child maltreatment and could be adapted and tested for parents of children with disabilities. Other such effective or promising violence prevention measures for non-disabled people could be adapted for persons with disabilities and then carefully evaluated.
The evidence base for the effectiveness of interventions to prevent violence against people with disability currently offers little clear guidance for practitioners and program commissioners faced with selecting such interventions. There is an urgent need in this area for research of higher quality. Researchers need to use samples that are more representative of the populations they are generalizing to; samples that are large enough to detect the expected effects; study designs with greater internal validity; measures of outcomes that are reliable and valid and also that more often measure actual violence rather than risk factors for violence; and above all, they should conduct outcome evaluation—of high quality—in low- and middle-income countries, where the majority of people with disabilities live.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.