
Abstract
The current study examined depression and physiological reactivity to a sexual threat task as longitudinal predictors of sexual revictimization in women with sexual victimization histories. The sample included 14 young adult women (Mage = 19.15) who reported child sexual abuse. Heart rate and root mean square of the successive differences were measured at baseline and during the presentation of sexual victimization–related words during an Emotional Stroop task. Results indicated that women who reported a greater history of childhood sexual abuse and adult sexual victimization were at increased risk for sexual revictimization 6 months after initial data collection. Furthermore, even after accounting for their childhood and adult sexual victimization histories and depression symptoms, women who exhibited reduced, or blunted, physiological activity during the sexual victimization stimuli of the Stroop task were more likely to report sexual revictimization during the 6-month follow-up. The findings suggest that sexual victimization survivors may benefit from interventions that address physiological blunting and the recognition of sexual threat cues in their environment.
Keywords
It is well documented that survivors of childhood sexual abuse (CSA) are at increased risk of short-term and long-term psychological, health, and interpersonal difficulties (Clements, Speck, Crane, & Faulkner, 2004; Felitti et al., 1998; Lang et al., 2003). Some long-term psychological effects include affective related disruptions, notably an increased depression risk (Maniglio, 2010; Neumann, Houskamp, Pollock, & Briere, 1996). Furthermore, CSA is a strong, consistently replicated predictor of later sexual victimization, which is called revictimization (Arata, 2000; Roodman & Clum, 2001; Tusher & Cook, 2010). Roodman and Clum (2001) conducted a meta-analysis and noted an effect size of .59 for the relationship between CSA and adult sexual victimization. Studies suggest that CSA survivors are 2 to 3 times more likely to be sexually victimized as adults than non-abused individuals (Abbey, Zawacki, Buck, Clinton, & McAuslan, 2004; Fleming, Mullen, Sibthorpe, & Bammer, 1999; Wyatt, Guthrie, & Notgrass, 1992). Walsh, Blaustein, Knight, Spinazzola, and van der Kolt (2007) noted that 75% of women with a history of CSA also reported an unwanted adult sexual experience. Prior research clearly documents that CSA survivors are at heightened risk of future victimization.
Previous researchers have attempted to explain why sexual revictimization occurs, including examining situational variables such as alcohol abuse, multiple sexual partners, differences among types of abuse, and separation from parents (Fisher, Cullen, & Turner, 2001; Siegel & Williams, 2003; Walsh et al., 2007). More recently, the inability to detect and respond to threat has been studied as a possible explanation of revictimization (Gidycz, McNamara, & Edwards, 2006; Meadows, Jaycox, Stafford, Hembree, & Foa, 1995; Messman-Moore & Brown, 2006; Patriquin, Wilson, Kelleher, & Scarpa, 2012; Soler-Baillo, Marx, & Sloan, 2005). By not recognizing threat, individuals may not react appropriately and find themselves in dangerous situations.
Lovallo, Farag, Sorocco, Cohoon, and Vincent (2012) looked at young, healthy adults with a history of adverse life events. Participants self-reported physical and sexual experiences as well as emotional adversity. Participants also completed a stress task while heart rate (HR) reactivity was measured. The researchers found that in both men and women, having greater early life adversity predicted a reduced physiological response to the stress task. This provides evidence of long-term physiological consequences following early adverse experiences.
In another study, Soler-Baillo and colleagues (2005) examined physiological recognition of threat in undergraduate females with or without histories of adolescent or adulthood sexual victimization. The researchers examined retrospective reports of sexual assault after the age of 14. The participants listened to the sounds of a sexual encounter between a man and woman that involved a date rape scenario while HR data were collected. They found that victims exhibited lessened HR reactivity to sexual threat cues compared with non-victims. The researchers suggested that by having a blunted response to sexual threat cues, the women might not detect risky situations or leave potentially threatening situations, and they proposed that therapeutic intervention could help survivors improve their recognition of potentially threatening cues. Therefore, physiological reactivity may function as a predictor of future sexual victimization events.
Related to physiological reactivity as a potential correlate of sexual victimization, Patriquin and colleagues (2012) found that college women with a history of CSA exhibited the highest sympathetic activation when compared with women sexually victimized in adulthood only, victimized in both childhood and adulthood (i.e., revictimized), or non-abused. These findings suggested that CSA survivors who avoided future victimization may have developed a defensive physiological response, which may have helped them to detect and avoid future risky situations. The women who reported sexual revictimization, however, evidenced lower sympathetic and parasympathetic reactivity during the sexual threat words than during baseline. The authors suggested that the physiological patterns among the revictimized women are suggestive of physiological blunting or reduced physiological reactivity (Berntson, Cacioppo, & Quigley, 1991; Simeon, Yehuda, Knutelska, & Schmeidler, 2008). Although these findings support the notion that attenuated threat detection is a possible predictor of revictimization, the findings were limited because the adulthood sexual victimization outcome data were collected retrospectively.
It is important to note that not all studies have found an association between risk perception and sexual revictimization (e.g., Breitenbecher, 1999). The method of assessing threat detection related to sexual victimization, however, may play a role in how participants respond. For example, Breitenbecher (1999) used video vignettes about acquaintance rape and had participants report recognition of threat. Attitudes toward actors, such as those based on race (Maeder, Mossière, & Cheung, 2013) or gender (Vandiver & Dupalo, 2013), may influence the participants’ responses. Other means of assessing threat, such as an emotionally threatening Stroop task (Field et al., 2001), may remove some of these problems associated with biases. Gidycz et al. (2006) noted that most studies have found an association between risk recognition and revictimization, and stressed the need to investigate various mechanisms underlying behavioral responses.
Current Study
Although Soler-Baillo et al. (2005) and Patriquin et al. (2012) found that victims displayed distinct physiological reactivity compared with non-victims, the implications of both studies were limited because they used cross-sectional designs and retrospective reports of victimization. In addition, Patriquin and colleagues (2012) noted that some survivors of CSA may have developed a heightened physiological response that protected them from future victimization. Conversely, some CSA survivors were revictimized in adulthood and these individuals demonstrated physiological blunting, which may be evidence of weakened threat detection. This latter finding suggests that there is variability in the physiological response of CSA survivors that may influence future victimization.
This pilot study sought to expand on the findings of Patriquin and colleagues (2012) and to inform future larger scale research by examining the impact of sexual victimization history and physiological reactivity during an emotional task on prospective reports of revictimization. The current study used a subset of the same participants as Patriquin and colleagues (2012), but incorporated the prospective victimization data that were not yet available for that study. To expand on that study and other previous literature, the current study used prospective revictimization data of female CSA survivors rather than relying on retrospective reports. College women were used in the current study because women report greater prevalence of sexual victimization than men, with young women at the highest risk—particularly college women (Kilpatrick, Resnick, Ruggiero, Conoscenti, & McCauley, 2007; Pereda, Guilera, Forns, & Gomez-Benito, 2009). For example, around 50% of female college students report sexual victimization and around 25% report attempted or completed rape (Abbey, Zawacki, Buck, Clinton, & McAuslan, 2001; Crowell & Burgess, 1996; Koss, 1988; Spitzberg, 1999).
The researchers used frequency domains of HR variability (i.e., HR and root mean square of the successive differences [RMSSD]) as indicators of sympathetic and parasympathetic activity of the heart. The cumulative number of different CSA incidents, HR, and RMSSD were examined as predictors of sexual revictimization. We defined CSA as an unwanted sexual abuse experience before 14 years of age. Revictimization was defined as an unwanted sexual experience that occurred in the adult women 6 months after participating in Time 1. We controlled for adult sexual victimization that may have occurred between the age of 18 years and Time 1, as these life events will likely also predict future victimization. Furthermore, we controlled for depressive symptoms as depression is often an aftereffect of victimization and associated with a dysregulation of cardiovascular activity (Brown, Barton, & Lambert, 2009). Orcutt, Cooper, and Garcia (2005) found that psychological distress, including depressive symptoms, partially mediated the relationship between CSA and revictimization. Survivors may engage in risky sexual behaviors as a means of coping to reduce psychological distress or may feel helpless in preventing future victimization. In sum, the examined predictors included history of CSA, history of adult sexual victimization, depression symptoms, and baseline and task HR and RMSSD.
In a typical “fight-flight” response, one would expect sympathetic activity (i.e., HR) to increase while parasympathetic activity (i.e., RMSSD) decreases (Berntson et al., 1991). We hypothesized that greater variety of CSA experiences or prior adult sexual victimization events reported at Time 1 would predict greater levels of sexual revictimization reported 6 months later at Time 3. Furthermore, we hypothesized that HR and RMSSD calculated during a sexual threat task at Time 2 would predict sexual revictimization at Time 3. Specifically, we expected women who demonstrated a heightened physiological response to sexual threat would be protected from sexual revictimization and thus report lower levels of prospective sexual revictimization at Time 3. Conversely, we expected women with a blunted physiological response (i.e., lower HR, lower RMSSD) to sexual threat stimuli to be at greater risk and therefore report greater levels of future sexual revictimization at Time 3.
Method
The current study was part of a larger longitudinal study, which included 2,892 undergraduate women at a large public university, examining cognitive and social characteristics associated with sexual revictimization. To be included in the current analyses, women had to have reported experiencing at least one CSA event and had to have participated in all three phases of the study (online screening, laboratory session, and follow-up online questionnaires). Of the 2,892 participants, 619 women reported experiencing at least one CSA event and of those 619, 14 individuals agreed to participate in all three phases of the study and had complete data for all phases (Mage = 19.15, SDage = 1.28). Participants who completed the second phase of the study were invited through email to participate in the follow-up online questionnaires (third phase). Participants were entered into a gift card raffle after completing the follow-up online questionnaires. Of note, participants were college students and the data were collected across semesters; thus, both the type of incentive and data collection across semesters likely contributed to the high rate of attrition of participants. Based on independent-samples t tests, the 14 sexual abuse survivors who completed all three phases of the study did not significantly differ on baseline or task physiology, depression symptoms, history of adult sexual victimization, number of CSA events, or rate of sexual revictimization from the CSA survivors who only completed one or two phases of the study. Of the 14 participants, 5 women reported an adult victimization event that occurred between Time 1 and Time 3. The women reported their ethnicity/race as White (n = 11), African American (n = 1), and Other (n = 1). One participant did not report her ethnicity/race.
Measures
Child abuse survey-modified
This seven-item instrument (Esposito & Clum, 2002) is a measure of CSA. The measure assesses incidents, including being kissed or hugged in a sexual way, the touching of sexual organs in a sexual way, vaginal penetration, and anal penetration. Participants reported on CSA experienced before the age of 14, which was defined as a sexual act involving bodily contact occurring during childhood by someone who was at least 5 years older than the child. This measure did not include sexual victimization that may have been perpetrated by peers. The participants were asked to respond to each item from 0 (never true) to 4 (very often true). For the purposes of this study, each item was scored as an absence or presence of each type of sexual victimization experience. These items were summed to create a total score of types of CSA experienced. To be included in the present analyses, participants had to indicate they had experienced at least one CSA incident. The child abuse variable was kurtotic (statistic = 4.98) and slightly skewed (statistic = 2.11). Therefore, the variable was log-transformed and was normally distributed after transformation (skewness statistic = 1.01, kurtosis statistic = .08).
Sexual experiences survey
The Sexual Experiences Survey (Koss & Oros, 1982) is a 10-item self-report instrument used to assess experiences of sexual hostility and victimization that may occur during adulthood. Participants were asked to indicate whether they had experienced various forms of sexual victimization using a yes−no format. The items assessed fondling, kissing, petting, and penetration. Scores were calculated by summing the 10 items, and scores ranged from 0 to 10. Participants completed this measure twice. First, participants completed the instrument in reference to any events that occurred between the age of 18 years to the time the women completed the Time 1 data collection. This represents the participants’ history of adult sexual victimization. The participants also completed the measure at Time 3 in reference to any sexual victimization that occurred during the 6 months between Time 1 and Time 3. This represents sexual revictimization. The revictimization variable was kurtotic (statistic = 4.59) and slightly skewed (statistic = 2.10). Therefore, this variable was log-transformed and was normally distributed after transformation (skewness statistic = 1.20, kurtosis statistic = .16).
Center for Epidemiological Studies of Depression Scale (CES-D)
The participants completed the CES-D (Radloff, 1977) at Time 1, which is a 20-item self-report screener of depression symptomatology. The women were asked to think about the past week and rate each of the 20 items from 0 (rarely or none of the time) to 3 (most or all of the time). Total scores on the CES-D can range from 0 to 60, with higher scores representing the presence of more depression symptomatology. Previous research has demonstrated high internal consistency (i.e., .87) for the CES-D when used in a college sample (Radloff, 1991). Typically, a cutoff score of 16 or higher is used to estimate the presence of clinically significant depression symptomatology. Based on this cut-off, 36% of the current sample reported clinically significant levels of depression symptoms. The Cronbach’s alpha for the CES-D in the current study was high (.93).
Emotional Stroop paradigm for sexual threat
The Stroop paradigm used in the current study was a computerized version based on the procedure used by Field and colleagues (2001). This task consisted of four types of stimuli presented via computer in the following order for all participants: (a) clusters of five X’s (control category), (b) “neutral” fruit category (emotionally neutral) containing 10 words (i.e., banana, peach, prune, pear, raisin, cherry, strawberry, grape, melon, apple), (c) general threat category containing 10 words (i.e., cancer, tumor, anxiety, coffin, guilt, death, panic, stress, nervous, funeral), and (d) sexual/victimization category containing 10 words (i.e., victim, abused, rape, molester, fondle, oral sex, erection, trapped, penetrate, force). The clusters of X’s or words in each category appeared in red, blue, green, or yellow on the computer screen. The inter-trial interval and word presentation time length were variable and depended on the participants’ response time to the stimuli. Color and content of the words were randomized so that no two successive words had the same color or definition. Research has demonstrated that this task is successful in activating previous memories of sexual victimization, which can significantly affect how one reacts toward sexual-related stimuli (Field et al., 2001)
Neutral baseline
Before completing the Stroop task, participants were shown a neutral baseline video. The baseline video, validated by Vella and Friedman (2007), was a 3-min segment of a video by Godfrey Reggio (co-produced by Francis Ford Coppola and George Lucas) titled Powaqqatsi: Life in Transformation. The Powaqqatsi video documents daily life events in different countries. This stimuli was used to establish a measure of baseline psychophysiology.
Polar S810i heart rate monitor
The Polar Heart Rate Monitor Model S810i (Polar monitor) is an ambulatory HR monitor that was used to collect heart period (HP) data during the baseline video and Emotional Stroop task. Research suggests that the Polar monitor provides a valid measure of HP during stationary laboratory tasks and provides results comparable with the electrocardiogram (Gamelin, Berthoin, & Bosquet, 2006).
Psychophysiological Data Reduction
HP data were collected continuously from the beginning of the 3-min baseline until after the Stroop task was completed. The Stroop task psychophysiology data analyzed here were collected during the 3-min epoch that coincided with the presentation of the sexual/victimization category words. R-waves were examined for validation. Following the artifact identification procedure outlined by deGeus, Willemsen, Klaver, and van Doornen (1995), all beats deviating more than 30% from the previous beat were deemed artifact and removed.
HR variability (HRV) measures were calculated using Kubios HRV Analysis Software (The Biomedical Signal Analysis Group, University of Kuopio, Finland) using RMSSD, which is an accepted measure of vagal, or parasympathetic, activity (De Meersman & Stein, 2007).
Procedure
The current study was part of a larger study involving measures that are not included in this article. At Time 1 of the study, women completed an hour-long online screening survey, during which they retrospectively reported on their CSA experiences, adulthood sexual victimization, and depression symptomatology.
At Time 2, after completing the online questionnaires, women were invited to complete a 1-hr laboratory session, which included the Emotional Stroop Paradigm and physiologic data collection. After participants provided informed consent, they were instructed on the attachment and use of the Polar monitor. Once the Polar monitor was in place, participants watched the Powaqqatsi baseline video for 3 min. Then, the researcher gave instructions on the Emotional Stroop task, which the participants subsequently completed. HP was recorded throughout the baseline video and entire Stroop task.
Approximately 6 months after Time 1, women were invited to complete Time 3 of the study, an online screening survey that inquired about sexual victimization that may have occurred during that 6-month period.
Institutional Review Board approval was obtained for each phase of the current study. Informed consent was also obtained from each participant for her participation in each phase of the study. Participants were compensated with extra credit points allotted toward their psychology courses for participating in Phases 1 and 2, and were entered into a raffle for participating in Phase 3.
Results
Descriptive Statistics and Correlations
The means, standard deviations, and Pearson product–moment correlations for all variables of interest are presented in Table 1. Baseline HR was positively correlated with task HR and negatively correlated with task RMSSD. Task HR was also negatively correlated with task RMSSD. History of adult sexual victimization was positively correlated with depression symptoms and revictimization.
Descriptive Statistics: Means, Standard Deviations (SD), and Inter-Correlations for all Variables of Interest (N = 14).
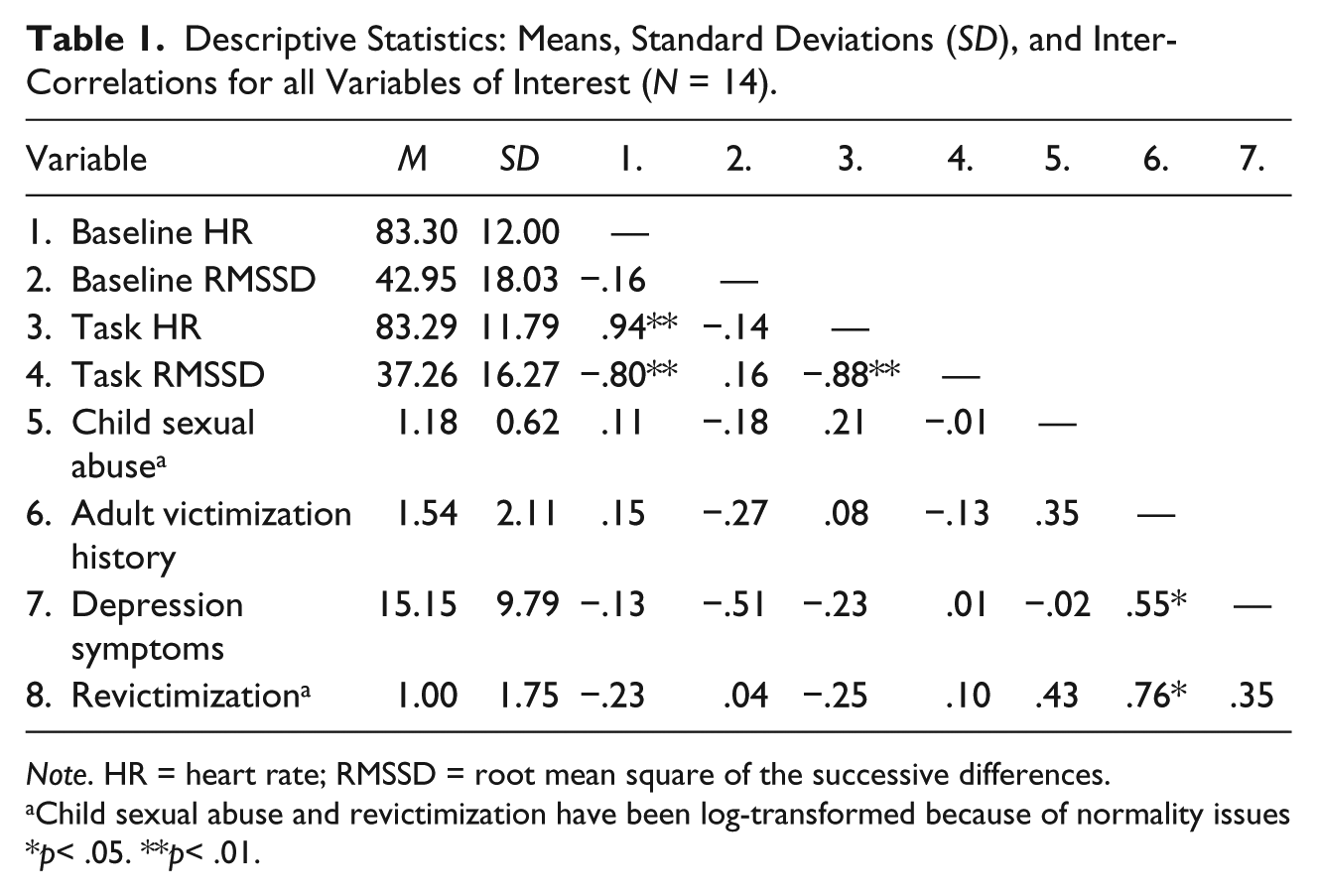
Note. HR = heart rate; RMSSD = root mean square of the successive differences.
Child sexual abuse and revictimization have been log-transformed because of normality issues
p< .05. **p< .01.
Because research consistently demonstrates strong inter-correlations between CSA, sexual victimization, psychopathology, and psychophysiology, it is likely more informative to examine partial correlations to test the relationship between task psychophysiology and revictimization. The partial correlation between task HR and revictimization, controlling for baseline HR, baseline RMSSD, task RMSSD, child abuse experiences, history of adult sexual victimization, and depression symptoms was statistically significant (r = −.77, p = .044). The partial correlation between task RMSSD and revictimization, controlling for baseline HR, baseline RMSSD, task HR, child abuse experiences, history of adult sexual victimization, and depression symptoms was statistically significant (r = −.76, p = .049).
Linear Regression
Linear regression analyses were used to test the main hypotheses (see Table 2). History of CSA and history of adult sexual victimization were entered in the first step of the regression to control for initial individual differences based on prior victimization, F(2, 10) = 7.73, p = .01, R2 = .61. History of adult sexual victimization was the only significant predictor in the first step (β = .69, p = .01). Baseline HR, baseline RMSSD, and depression symptoms were added in the second step of the regression, F(5, 7) = 5.44, p = .02, ΔR2 = .19. The only significant predictor in the second step was the history of adult sexual victimization (β = .80, p = .01). Task HR and task RMSSD were added in the third step of the linear regression, F(7, 5) = 10.12, p = .01, ΔR2 = .14. Task HR (β =−1.88, p = .04), task RMSSD (β = −1.06 p = .02), history of child sexual abuse (β = .54, p = .02), and history of adult sexual victimization (β = .72, p = .01) significantly predicted future victimization. The predictors accounted for 94% of the variance in prospective revictimization.
Linear Regression Analyses Testing Child Sexual Abuse History, History of Adult Sexual Victimization, Baseline Physiology, Depression Symptoms, and Task Physiology as Predictors of Prospective Reports of Sexual Revictimization (N = 14).
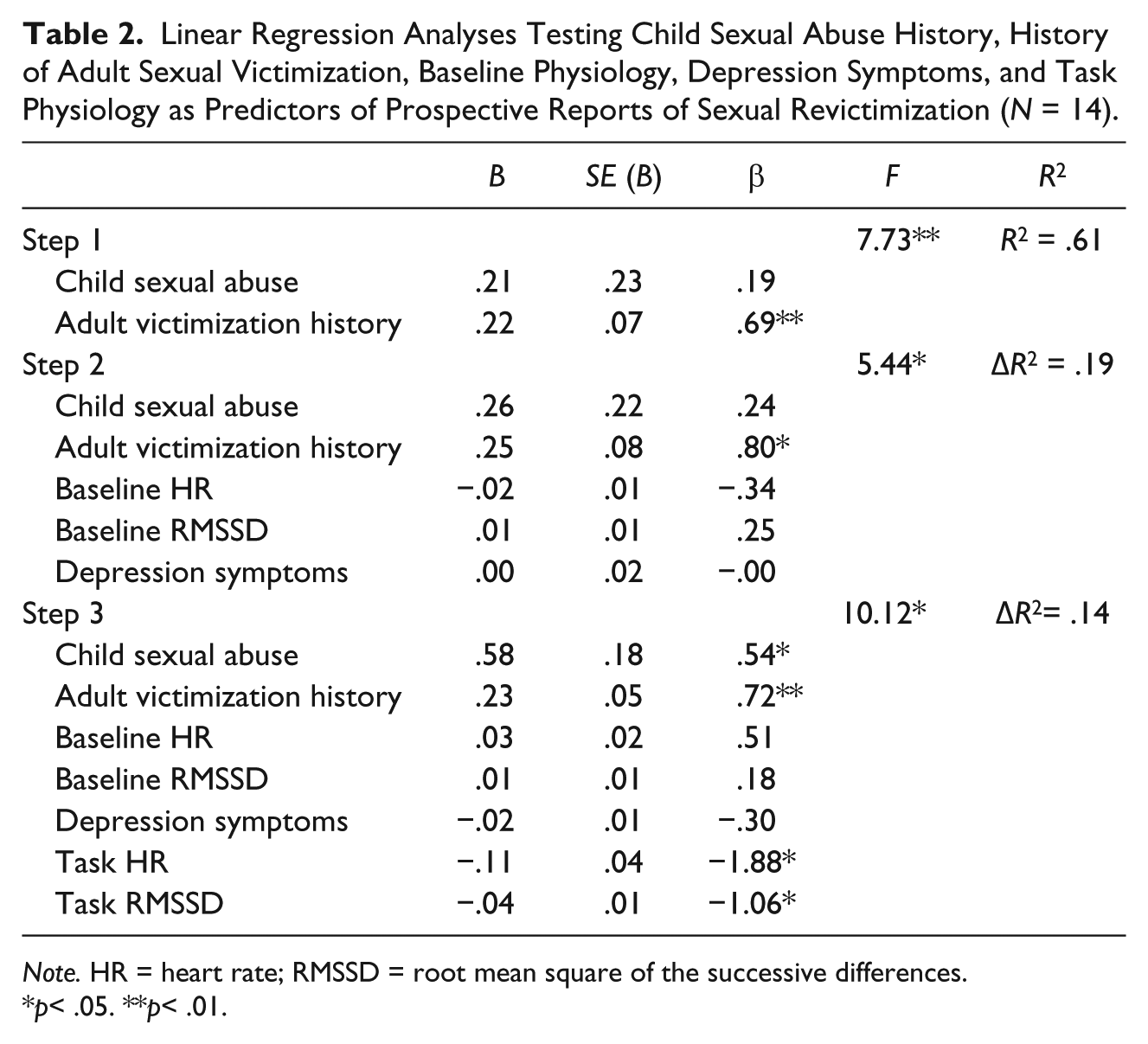
Note. HR = heart rate; RMSSD = root mean square of the successive differences.
p< .05. **p< .01.
Discussion
The present study examined victimization history, depression symptoms, and physiological reactivity to a sexual threat task as predictors of sexual revictimization. Overall, the results indicated several prospective predictors of adult sexual revictimization. After accounting for all predictors, greater number of CSA events measured at Time 1 was associated with greater adult sexual revictimization measured at Time 3. Experiencing more events as a child, therefore, increased the risk for adult revictimization. This finding is consistent with a large body of previous research that finds a history of child abuse to be associated with a greater likelihood of future victimization (Abbey et al., 2004; Fleming et al., 1999; Walsh et al., 2007; Wyatt et al., 1992).
The current study also found that, in CSA survivors, lower sympathetic and parasympathetic activity during a sexual threat task (measured at Time 2) were significantly related to increased incidences of sexual revictimization at Time 3. This result is indicative of physiological blunting across the autonomic nervous system (Simeon et al., 2008). Women who are not able to physiologically recognize sexual threat are at greater risk of sexual revictimization. Their lack of response to sexual cues may make these women unaware of threatening situations and therefore less likely to leave these situations. These results are similar to those found by previous researchers (e.g., Patriquin et al., 2012; Soler-Baillo et al., 2005). Interestingly, HR and RMSSD at baseline did not prospectively predict reports of revictimization. This indicates that responsivity and reactivity during exposure to sexual threat may be a more powerful variable in predicting future risk than baseline physiology. Conversely, due to the small sample, these analyses may have been underpowered. Future researchers who are interested in predicting victimization from physiological response should take into account the rate of attrition in this longitudinal study.
While depression has been linked to an increased risk for revictimization (Orcutt et al., 2005), it is important to note that the current study did not examine all psychiatric symptomatology related to revictimization (see Messman-Moore & Long, 2003, for review). Most notably, posttraumatic stress disorder (PTSD) is a common outcome of CSA that is considered a predictor of revictimization (Arata, 1999; Arata, 2000). PTSD, however, could not be examined as part of the current analyses because a measure of PTSD was not administered to all participants. This will be an important area in future investigations because physiological reactivity may be directly related to PTSD symptomatology. In fact, the most recent revision to the Diagnostic and Statistical Manual of Mental Disorders highlights the role of alterations to arousal following trauma as a required diagnostic criterion for diagnosis of PTSD (American Psychiatric Association, 2013). More specifically, research suggests that many individuals with PTSD experience heightened physiological reactivity to trauma-related stimuli (i.e., hyperarousal; Orr, Metzger, Miller, & Kaloupek, 2004; Pole, 2007). Conversely, many individuals with PTSD do not demonstrate this heightened response (Orr & Roth, 2000). It is unclear whether the results presented here would change if we were able to account for PTSD symptoms. However, it is clear that future research should include PTSD as a predictor to further our understanding of the impact of physiological blunting on revictimization.
There are limitations of the current study that should be highlighted. First, the external validity of the study is restricted because the sample included only college women and the participants were predominantly White. Future studies should examine community samples, as well as strive to include men and more culturally and ethnically diverse participants. Although the external validity was limited, college women were deemed appropriate due to a greater risk for sexual victimization compared with non-college women and men (Kilpatrick et al., 2007; Pereda, Guilera, Forns, & Gomez-Benito, 2009). Second, HR has both sympathetic and parasympathetic influences (De Meersman & Stein, 2007), so HR is not a precise measure of sympathetic activity. Third, there is debate in the literature regarding how to measure sexual victimization. Many researchers use dichotomous measures to assess for the absence or presence of victimization; however, many researchers prefer continuous measures because dichotomous instruments over-simplify the nature of the victimization. The current study used a continuous measure of the number of sexual victimization experiences and this methodology should be kept in mind when interpreting the results. Fourth, this study did not look at child abuse perpetrated by same-aged peers. The researchers recognize that peer victimization can be just as traumatic as abuse perpetrated by an adult. Previous research, however, has noted that child abuse perpetrated by an older individual may be associated with more negative outcomes than peer abuse (Maker, Kemmelmeier, & Peterson, 2001). Prior researchers have suggested that differences in power status might lead to more adverse long-term outcomes. It would be interesting to see if physiological responses play similar roles in peer abuse. Fifth, the Time 1 screening for child abuse and adult sexual victimization histories were collected retrospectively, which may have affected their accuracy. Last, the sample size is smaller than would be suggested based on an a priori power analysis (power analyses recommended 49 participants for a linear regression analysis using α = .05 and power = .80 to detect large effect sizes with seven predictors) and future research should attempt to replicate the findings in a larger and more diverse sample. Future researchers should take into account the attrition rate of the participants across the three phases of the study to recruit a larger sample size at Time 3. Also, future researchers should be aware of the large attrition of college student participants when conducting a study across semesters. Due to the small sample size, these results should be viewed as preliminary but offer important guidance for future investigation.
Despite these limitations, the study has several strengths that should be highlighted. First, the prospective design allowed us to examine predictors of future sexual revictimization. Second, despite the small sample size, the variables of interest accounted for 94% of the variance and suggest that the constructs studied evidenced large effect sizes. Third, we included objective measures (i.e., psychophysiology) as predictors of revictimization, which is beneficial because this type of measure is less prone to biases than self-report or questionnaire measures. Last, this study incorporated several well-established measures and built upon previous research findings.
Clinically, this study helps to inform mental health professionals about information that should be addressed during intervention following sexual victimization and when designing prevention programs. For example, psychoeducation could be an important stage of recovery to help women identify future potential threat cues. This could include training related to identifying and monitoring social cues, emotional cues, and/or physical cues associated with risky situations or people. Psychophysiological measurement could also be considered as a possible measure to monitor psychotherapy treatment progress, because HRV reactivity has been found to change in response to cognitive-behavioral therapy following trauma (Rabe, Dorfel, Zollner, & Maercker, 2006). The results also suggest that biofeedback may be an effective tool that should be considered for inclusion as part of a treatment plan.
Overall, the findings contribute to the field by examining predictors of adult sexual revictimization using a prospective design. Physiological reactivity, specifically physiological blunting, to a sexual threat was found to increase women’s risk of future revictimization. Clinically, this study demonstrates the need for interventions to incorporate information related to threat detection and reduced psychophysiological reactivity. This pilot study, despite its limitations, should be used to guide the designing of future investigations, improve intervention planning, and inform prevention programs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.