
Abstract
Previous research suggests a diathesis-stress model of posttraumatic stress disorder (PTSD), wherein individuals with high levels of neuroticism who are exposed to traumatic events subsequently develop PTSD. Although studies have established relationships between neuroticism and neurological functioning in various brain regions for healthy and depressed individuals, the specific neural correlates of neuroticism for individuals with PTSD are yet unknown. This relationship is particularly relevant for women, given that their increased risk for PTSD is partially accounted for by their higher baseline levels of neuroticism. The current study examined previously established neural correlates of neuroticism in 61 women (48 women with interpersonal violence [IPV]/PTSD and 13 healthy controls). A specific region of interest map, including the amygdala, hippocampus, parahippocampus, anterior cingulate cortex (ACC), and dorsal medial prefrontal cortex (dmPFC), was examined while participants completed an emotional conflict task. Results showed that the PTSD group had significantly higher neuroticism scores than the healthy control group (t = 6.90, p < .001). Higher neuroticism scores were associated with increased neural activity in the right dmPFC when participants were instructed to directly attend to faces with negative emotional valences. Significant trends between higher neuroticism scores and greater right amygdala and right ACC activation also emerged for this condition. Finally, neuroticism was found to be associated with right amygdala and right parahippocampal activity when participants were instructed to ignore faces with negative emotional valences. The results of this study lend further evidence to the proposed diathesis-stress model of neuroticism and PTSD. Moreover, findings suggest a significant association between neuroticism and neural activity in brain regions associated with fear and emotion regulation for women with IPV and subsequent PTSD.
Posttraumatic stress disorder (PTSD) is a chronic disorder characterized by the onset of debilitating avoidance, hyperarousal, and reexperiencing symptoms subsequent to experiencing a traumatic event. Estimates indicate that PTSD affects 6% to 10% of the general population across the life span, with women experiencing substantially greater rates than men (9.7% vs. 3.6%) due in part to higher rates of interpersonal violence (IPV; for example, rape, sexual assault, physical assault; Breslau, Davis, Andreski, & Peterson, 1991; Iverson et al., 2013; Kessler, Chiu, Demler, & Walters, 2005; Kessler, Petukhova, Sampson, Zaslavsky, & Wittchen, 2012; National Comorbidity Survey, 2005). A significant number of negative outcomes have been linked to PTSD, including poor emotional functioning and increased risk of suicide (Bruce et al., 2012; Ilgen et al., 2012; Pittman, Goldsmith, Lemmer, Kilmer, & Baker, 2012). As such, efforts to increase our understanding of the underlying mechanisms associated with PTSD development are critical to strengthen prevention and intervention strategies.
One underlying mechanism that appears to be associated with PTSD is neuroticism, defined as the degree to which an individual is predisposed to experience aversive emotional states (Eysenck & Eysenck, 1964). Individuals with high neuroticism levels tend to respond less favorably to difficult situations and emotional content, which has been shown to result in more frequent worry, more anxiety/unease, and higher levels of negative emotionality than those with average and low levels of neuroticism (McCrae & Costa, 1999). Importantly, previous literature has reported significant gender differences in neuroticism, with women consistently reporting higher levels of neuroticism than men, even across varying cultures (Costa, Terracciano, & McCrae, 2001; Ormel et al., 2013). Thus, an examination of the relationship that neuroticism has on women with PTSD is an important area for further study.
A growing body of evidence suggests that a high level of neuroticism serves as a diathesis in the development of PTSD (Breslau et al., 1991; Breslau & Schultz, 2013; Christiansen & Hansen, 2015; Parslow, Jorm, & Christensen, 2006). For example, in a study consisting of 1,007 young adult participants, Breslau and colleagues (1991) showed that a high level of neuroticism was associated with a greater risk for developing PTSD. Moreover, Breslau and Schultz (2013) provided further evidence for this relationship between neuroticism and PTSD in a recent follow-up investigation that used the same sample of individuals from Breslau et al.’s (1991) study. Longitudinal data were collected from 899 participants of the original sample over the course of 10 years. Of the individuals who experienced a traumatic event over the course of this 10-year investigation, the authors found that those with higher levels of pretrauma neuroticism were at a significantly greater risk for subsequent development of PTSD than those with lower levels of pretrauma neuroticism. Neuroticism levels thus appear to serve as a greater risk factor for women than men in the development of PTSD, which partially accounts for their higher rates of PTSD onset subsequent to interpersonal trauma (Breslau, Davis, Andreski, Peterson, & Schultz, 1997; Christiansen & Hansen, 2015).
This body of prior research suggests that individuals with higher levels of neuroticism are more susceptible to the onset of PTSD symptomatology following a trauma. This area needs further exploration, though, as this interaction is not yet fully understood. Brain imaging techniques present one avenue through which neuroticism’s influence can be further examined, as little is yet known about the ways in which traits such as neuroticism affect the patterns of neural activity associated with PTSD.
Neural Correlates of Neuroticism
Recent studies have examined the neural correlates of neuroticism in a depressed sample; however, researchers have yet to investigate the neural correlates of neuroticism in women with PTSD (Servaas et al., 2013; Sutin, Beason-Held, Dotson, Resnick, & Costa, 2010). Given the transdiagnostic nature of neuroticism, as well as the high comorbidity between PTSD and depression, it is likely that neuroimaging research on neuroticism in depressed individuals provides a basis for examining neuroticism in women with PTSD (Campbell et al., 2007). These studies have noted an association between high levels of neuroticism and activation in brain areas such as the hippocampus, parahippocampus, dorsal medial prefrontal cortex (dmPFC), anterior cingulate cortex (ACC), and amygdala (Canli et al., 2001; Chan, Norbury, Goodwin, & Harmer, 2008; Coen et al., 2011; Haas, Constable, & Canli, 2008; Hooker, Verosky, Miyakawa, Knight, & D’Esposito, 2008).
Research examining fear conditioning in male and female samples has found that hippocampal and parahippocampal regions of the brain are involved in fear learning and expression (Feng, Feng, & Chen, 2013; Hooker et al., 2008; Maren & Hobin, 2007). One study demonstrated that greater activation in the parahippocampal brain region was associated with higher levels of neuroticism in participants viewing threatening stimuli contrasted to neutral stimuli, and another investigation found that higher levels of neuroticism were associated with greater activation in the amygdala–hippocampal complex during fear learning contrasted to neutral learning (Coen et al., 2011; Tzschoppe et al., 2014). Neuroticism thus appears to modulate activation in these brain regions, prompting researchers to hypothesize that the brain’s fear learning system may be overactive in individuals with higher neuroticism levels (Servaas et al., 2013).
Prior research has also established the amygdala as playing an integral role in the processing of emotion, the consolidation of emotion-laden memories, and the social recognition of emotions, particularly fear (Dalgleish, 2004; Meunier, Bachevalier, Murray, Málková, & Mishkin, 1999). High levels of neuroticism were previously correlated with increased activation in this region when individuals were presented with ambiguous fearful versus happy facial expressions (Chan et al., 2008). Similarly, Brück, Kreifelts, Kaza, Lotze, and Wildgruber (2011) found that neuroticism scores were positively correlated with amygdala activation when individuals were presented with emotionally laden auditory stimuli. These findings are consistent with theories suggesting that amygdala sensitivity in relation to negative information is indicative of higher levels of neuroticism (Canli, 2008).
Another important region of interest (ROI) is the dmPFC, a brain region believed to process and regulate emotion (Hofmann, Ellard, & Siegle, 2012; Ochsner & Gross, 2006; Servaas et al., 2013). In a study in which participants were asked to reappraise their thoughts while responding to threatening stimuli, Goldin, Manber, Hakimi, Canli, and Gross (2009) found that increased dmPFC activation occurred during regulatory efforts. Furthermore, regarding the influence of neuroticism levels on this brain structure, Cremers et al. (2010) found that higher neuroticism scores predicted greater activation in the dmPFC in response to faces with fearful expressions compared with neutral expressions. Importantly, it has been hypothesized that increased amygdala activation and impaired prefrontal control may account for the disrupted fear and threat-related processing in PTSD; however, increased dmPFC activation may be expected of those high in neuroticism due to their tendency to engage in worry (Cremers et al., 2010; Rauch, Shin, & Phelps, 2006). The combination of these findings led Servaas et al. (2013) to propose that hyperactivity in the dmPFC is representative of the debilitating impact that neuroticism has on emotion regulation, as highly neurotic individuals struggle to employ adaptive approaches to emotion processing and regulation, such as reappraisal.
Finally, previous studies also indicate a relationship between neuroticism and activity in the ACC, a structure proposed to be involved in the anticipation of aversive stimuli, emotion regulation, and diminution of unconditioned responses (Dunsmoor, Bandettini, & Knight, 2008; Hofmann et al., 2012; Servaas et al., 2013). Findings regarding the nature of this relationship have thus far been inconsistent, as some research has indicated that higher levels of neuroticism lead to greater activation in the ACC during emotional conflict, whereas other studies have demonstrated a negative relationship between neuroticism and ACC activation during anticipation of negative stimuli (Haas, Omura, Constable, & Canli, 2007; Kumari, Das, Wilson, Goswami, & Sharma, 2007). Given these conflicting findings, the current study sought to clarify the role of neuroticism as it relates to the ACC in women with PTSD.
It is important to note that the majority of the findings discussed thus far were based on studies with both male and female participants (Coen et al., 2011; Cremers et al., 2010; Dunsmoor et al., 2008; Hooker et al., 2008; Servaas et al., 2013; Tzschoppe et al., 2014). Preliminary research examining differences in brain activation across gender indicates that discrepancies exist. Specifically, men appear to demonstrate more extensive brain activation in response to angry, sad, and happy stimuli, whereas women have been found to have more widespread brain activation in response to fearful facial stimuli (Weisenbach et al., 2014). Moreover, differing degrees of brain activation have been shown to exist between men and women with PTSD, as a recent study by Felmingham and colleagues (2010) indicated that men with PTSD demonstrate greater hippocampal activity in response to fearful stimuli than women with PTSD (Felmingham et al., 2010). As such, although current research informs us about the influence of neuroticism on various brain regions, it is likely that findings from a sample of women with PTSD may result in some divergence from previous studies (Ormel et al., 2013).
The purpose of the current study was to examine the neural correlates of neuroticism in a PTSD sample of women who have experienced an interpersonal trauma. Based on previous studies outlined above, we hypothesized that women with PTSD would endorse significantly higher neuroticism scores than a nontrauma exposed healthy control sample. Furthermore, we hypothesized that the association between neuroticism and brain activation in specific brain regions (parahippocampus, hippocampus, dmPFC, ACC, amygdala) would be higher in the PTSD group compared with the healthy control group.
Method
Participants
Participants were recruited via a university-based trauma center as part of a larger neuroimaging study. The sample was comprised of 61 right-handed, English-speaking women, including 48 women with PTSD and 13 nontrauma exposed healthy controls. Participants’ demographic and clinical characteristics, as well as trauma history, are reported in Table 1. Sexual traumas included childhood sexual abuse, rape, and sexual assault, whereas physical traumas included childhood physical abuse, domestic violence, and physical assault. A large number of participants with PTSD (60%) reported experiencing multiple traumas in their lives.
Participant Demographics.
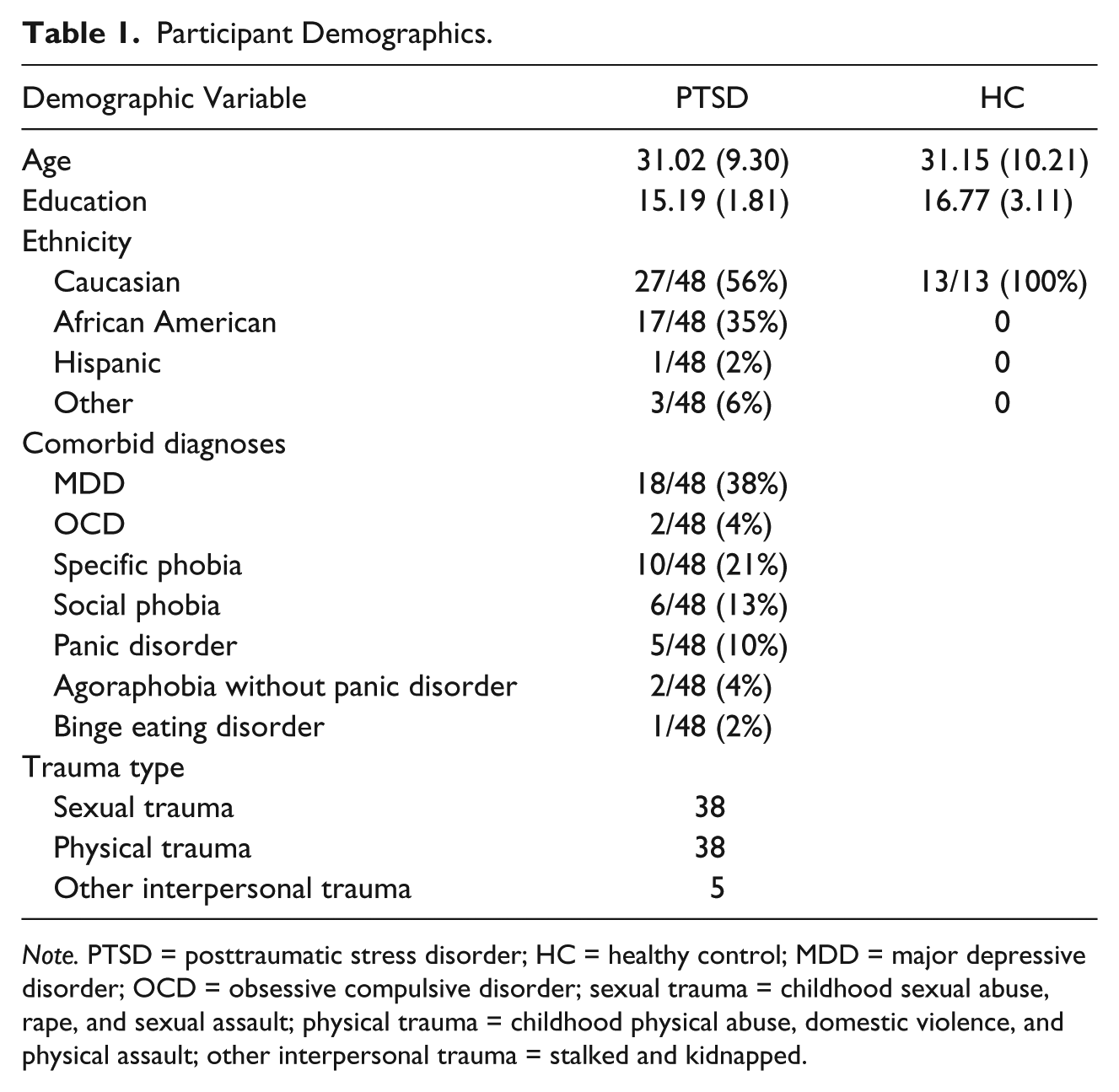
Note. PTSD = posttraumatic stress disorder; HC = healthy control; MDD = major depressive disorder; OCD = obsessive compulsive disorder; sexual trauma = childhood sexual abuse, rape, and sexual assault; physical trauma = childhood physical abuse, domestic violence, and physical assault; other interpersonal trauma = stalked and kidnapped.
Women were included in the PTSD group if they met Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000) diagnosis of PTSD that resulted from an interpersonal trauma. Trained assessors employed the Clinician Administered Posttraumatic Stress Disorder Scale (CAPS) to determine each participant’s PTSD diagnosis. Individuals in the PTSD group with a primary diagnosis of PTSD and a CAPS score of 45 or higher were included in the analysis to ensure participants had clinically significant symptoms. For inclusion in the nontraumatized healthy control group, participants were neither required to have experienced a Criterion A event in their lifetime nor could they have a current diagnosis of a mood or anxiety disorder. Individuals with psychosis, bipolar disorder (current or previous), current psychotropic medication use, current diagnoses of either substance or alcohol abuse, history of head trauma or other neurological disorders, and functional magnetic resonance imaging (fMRI) contraindications were excluded from both the PTSD and healthy control groups.
Procedure
Participants were recruited for this study via online advertisements on Craigslist, postings in university newspapers, and advertisement flyers throughout the community. Each participant engaged in standard informed consent procedures and agreed to participate. Phone intakes and in-person assessments were carried out by clinical research assistants. Eligible participants were scheduled for magnetic resonance imaging (MRI) scans subsequent to their initial assessments. The stimuli presented in the emotion conflict task were projected onto a screen behind the imaging chamber, and a mirror allowed each participant to view the material. Task instructions were given to participants both prior to and during the scan. Those women in the PTSD group were offered free trauma-focused therapy for their participation in the study.
Measures
CAPS
The CAPS (Blake et al., 1995) is a semistructured, clinician-administered interview that is regarded by many as the “gold standard” measure for assessing PTSD (Weathers, Keane, & Davidson, 2001). The measure includes 25 two-part items that determine the frequency and intensity of posttraumatic stress symptoms listed in the DSM-IV-TR diagnostic criteria. Frequency and intensity are both scored on rating scale of 0 to 4 for every item, with higher ratings indicating greater symptom frequency/intensity. The CAPS has exhibited good internal consistency (with coefficient αs ranging from .64 to .88) and test–retest reliability (with correlation coefficients ranging from .86 to .95; Weathers et al., 2001). During the initial in-person assessment, each participant was asked about both past month and lifetime symptoms of PTSD, though only past month scores were used in the analysis. A symptom was indicated by a frequency rating of one or more in conjunction with an intensity rating of two or more (Weathers et al., 2001).
Structured Clinical Interview for the DSM-IV (SCID)
The SCID is a semistructured, clinician-administered interview that assesses for the current or previous presence of psychological disorders based on criteria from the DSM-IV-TR. The initial assessment entailed the administration of the Mood, Psychotic, Anxiety, Somatic, and Eating Disorders modules of this measure, to determine participant eligibility. The SCID has exhibited good interrater and test–retest reliability (Lobbestael, Leurgans, & Arntz, 2011; Zanarini & Frankenburg, 2001).
Eysenck Personality Questionnaire (EPQ)
The EPQ is a 100-item self-report that assesses individuals on dimensions of extraversion, neuroticism, and psychoticism (Eysenck & Eysenck, 1964). Individuals are asked to respond “yes” or “no” to questions such as “Does your mood often go up and down?” and “Do you worry about awful things that might happen?” The EPQ has been shown to have good internal consistency for neuroticism (.82; Loo, 1979).
Emotion conflict task
Stimuli were presented using the PsyScope program, and each participant’s behavioral data were tracked using a fiber-optic key press equipped with the PsyScope Button box. Each stimulus consisted of four pictures (two faces and two houses) ordered in vertical and horizontal pairs (Figure 1). A total of 20 faces (10 fearful and 10 neutral) and 20 houses were sequentially presented to the participants on a gray background.

Sample image from the emotional conflict task.
The event-related task entailed four blocks of 52 trials, with the order of the blocks being counterbalanced. Blocks were comprised of 13 trials from four different conditions: attend fear (AF), ignore fear (IF), attend neutral (AN), and ignore neutral (IN). During the AF and AN conditions, the participant must decide whether the pair of faces, either both neutral or both fearful, matched or differed; this condition also involves ignoring the pair of houses being presented. During the IF and IN conditions, the participant must decide whether the pair of houses match or differ; pairs of fearful or neutral faces serve as distractors in this condition.
Each block began by informing participants which pair of images that they should attend to throughout (i.e., vertical or horizontal). Each individual trial initially displayed a fixation cross for 1,000 ms, followed by the pairs of houses and faces for 250 ms. Participants were instructed to decide whether the images of the cued pair matched or differed, and then indicate their choice by pressing one of two buttons on their handheld box. Intertrial jittering was randomly varied between 2,150, 4,660, 7,170, 9,680, and 12,190 ms. Participants were asked to maintain fixation on a crosshair fixation throughout the trials and to attend to the stimulus pair in just the relevant locations. Previous studies may be consulted for additional information on the emotion conflict task (Bruce et al., 2012; Fales et al., 2008).
Image Acquisition and Processing
Functional and structural MRI data were collected using a 3T Siemens Trio Trim whole-body scanner with a 12-channel head coil. fMRI data were acquired using an asymmetric spin-echo sequence sensitive to blood-oxygenation-level-dependent (BOLD) T2* contrast (4 × 4 × 4 mm voxel size, Repitition Time (TR) = 2,200 ms, Echo Time (TE) = 27 ms, Field of view (FOV) = 384 mm, flip angle = 90°, 64 × 64 matrix, 36 slices). Structural MR images were acquired using a high-resolution three-dimensional (3D) magnetization prepared rapid gradient echo (MPRAGE) sequence in the sagittal orientation (1 × 1 × 1 mm voxel size, TR = 2,400 ms, Inversion Time (TI) = 1,000 ms, TE = 3.13 ms, flip angle = 8°, FOV = 256 mm, 256 × 176 matrix, 176 slices).
Imaging data were preprocessed in Statistical Parametric Mapping Software, Version 12 Beta (SPM12b; Wellcome Department of Cognitive Neurology, London, UK). First, images were realigned to correct for head movement and then corrected for interslice temporal differences using slice time correction. Next, coregistration between structural and mean functional images was implemented followed by segmentation of the newly coregistered structural image (Ashburner & Friston, 2005). Using deformation fields, these images were then wrapped into Montreal Neurological Institute (MNI) coordinate space and smoothed with an 8-mm full-width at half maximum (FWHM) Gaussian kernel. For further quality control, movement and signal outliers were identified using the Artifact Detection Tool (ART; http://web.mit.edu/swg/art/art.pdf) software package. A Z value above three for the differential scan global signal threshold and a between scan movement threshold above 1 mm were defined as outliers. The identified outliers were submitted into each participant’s first-level general linear model (GLM), described below, as regressors of no interest. Participants having less than three fMRI scanning sessions and/or having more than 20% outliers per session were not included in second-level analyses (PTSD: n = 3 of original sample of 51, Controls [CON]: n = 1 of original sample of 17).
Statistical Analysis
An independent-samples t test was conducted to examine whether neuroticism levels were significantly greater for participants with PTSD than for healthy controls. In addition, a Cohen’s d statistic was calculated to demonstrate the effect size of group membership on neuroticism levels. A Pearson’s r correlation coefficient was calculated to test the degree of linear dependence between neuroticism levels and brain activation in the ROIs for both AF and IF conditions. Effect sizes were based on previously established standards (Cohen, 1992). Several exploratory analyses were performed on a subsection of individuals to test for group differences on behavioral task performance. Specifically, average accuracy scores and response times were calculated, and then independent-samples t tests were used to see whether the groups differed in performance across AF and IF conditions.
fMRI statistical analyses
SPM12b was also utilized for first- and second-level analyses. For first-level analyses, neural responses during each condition of the emotion conflict task were modeled with delta functions and then convolved with a canonical hemodynamic response function (HRF). The Statistical Parametric Mapping (SPM) default high pass filter cutoff of 128 s was used to account for slow signal drift. Serial correlations were accounted for with an autoregressive (AR(1)) model.
ROIs were identified a priori and included the parahippocampus, hippocampus, dmPFC, ACC, and amygdala. These regions were defined by Tzourio-Mazoyer et al. (2002) and created in the Wake Forest University PickAtlas toolbox (Maldjian, Laurienti, Kraft, & Burdette, 2003). Second-level group analyses began with generating unbiased activation maps in each ROI for the entire sample (PTSD and controls) for both the AF and IF conditions. This was accomplished using two-sample t tests with contrast images from the first-level models (AF and IF, separately) and an equally weighted T-contrast (e.g., [.5, .5]). Results were considered significant at a voxel-extent threshold of p < .05 corrected for family-wise error (FWE; Friston, Worsley, Frackowiak, Mazziotta, & Evans, 1994). To investigate whether PTSD and control groups have similar and/or different correlations between neuroticism scores and ROI activation during AF and IF conditions, average magnitude estimates were then extracted from statistically significant clusters of activation in the ROIs from the two-sample t tests described above for each individual participant using MarsBar (Brett, Anton, Valabregue, & Poline, 2002; http://marsbar.sourceforge.net). The extracted magnitude estimates were analyzed in SPSS statistics, Version 21, using bivariate correlations for both the PTSD and control groups, and were considered significant at p < .05.
fMRI data acquisition
A Siemens 3 TrioTim MRI scanner (Erlangen, Germany) was used to conduct all participant scans. In addition to functional images, localizer images and an MPRAGE were collected. A sagittal 3D T1-weighted sequence (TR = 2.4, TE = 3.13 ms, flip angle = 8°, FOV = 256 cm, TI = 1,000 ms, resolution = 1 × 1 × 1) was used to obtain structural scans. For functional images, an asymmetric spin-echo echo-planar sequence with a volume TR of 2.2 s (TE = 27 ms, flip angle = 90°, FOV = 256 cm) was utilized. A single acquisition included 36 transverse slices with a width of 4 mm (no gap) and a 4 × 4 mm in-plane resolution. Functional imaging sequences included 180 acquisitions and three initial volume images that were not analyzed.
Imaging analysis
Preparation of functional images for data analysis was conducted using SPM12b. Head motion was controlled for by aligning images to a participant-specific mean fMRI image. To account for interslice temporal differences, images were slice time corrected. Coregistration of the participants’ structural and functional images was conducted, and the coregistered structural images were segmented using the New Segment tool for SPM12b (Ashburner & Friston, 2005). Normalization of MRI data to MNI space was conducted utilizing deformation fields. An 8-mm FWHM Gaussian kernel was used to filter normalized images, and movement outliers were identified by the ART (Whitfield-Gabrieli, 2011) software package.
ROIs identification
ROIs analysis was utilized to test specific hypotheses regarding the neural correlates of neuroticism in individuals with PTSD. The Wake Forest University PickAtlas toolbox (http://www.nitrc.org/projects/wfu_pickatlas) for SPM12b was used to anatomically define the ROIs. ROIs for the current analysis included the left and right parahippocampus, hippocampus, dmPFC, ACC, and amygdala.
Results
Neuroticism and Group Membership
The average neuroticism score for the group of participants with PTSD was 16.71, whereas the average neuroticism score for the nontrauma exposed control group was 7.39. Results of an independent-samples t test revealed that the PTSD group had significantly higher neuroticism scores than the control group (t = 6.90, p < .001; Cohen’s d = 4.48).
Behavioral Task Performance
A series of statistical analyses were performed on a subsample of individuals to examine the influence of group membership and neuroticism levels on behavioral task performance. An independent-samples t test revealed that the control group’s overall mean accuracy (81%) was significantly higher than the overall accuracy of the PTSD group (73%; t = 2.33, p = .02). Furthermore, within the PTSD group, mean accuracy was significantly higher for the IF condition (76%) than the AF condition (71%; t = −3.05, p = .003). Again, for the PTSD group, mean response time was significantly lower for the IF condition (845.45 ms) than for the AF condition (927.03 ms; t = 3.98, p < .001).
AF Correlation Analyses
A series of correlation analyses were completed for each group to examine whether or not neuroticism scores were associated with activation in the brain ROIs when participants had to attend to fearful faces. For participants in the PTSD group attending to fearful faces, neuroticism scores were significantly associated with activation in the right dmPFC (r = .35, p = .02; see Figure 2). Furthermore, significant trends emerged between neuroticism scores and activation in the right amygdala (r = .27, p = .07) and the right ACC (r = .25, p = .09). No significant association was found between neuroticism scores and activation in the left parahippocampus, right parahippocampus, left hippocampus, right hippocampus, left dmPFC, left ACC, or left amygdala for the PTSD group. As for participants in the control group attending to fearful faces, no significant correlations or significant trends emerged between neuroticism scores and activation in any of the brain ROIs.
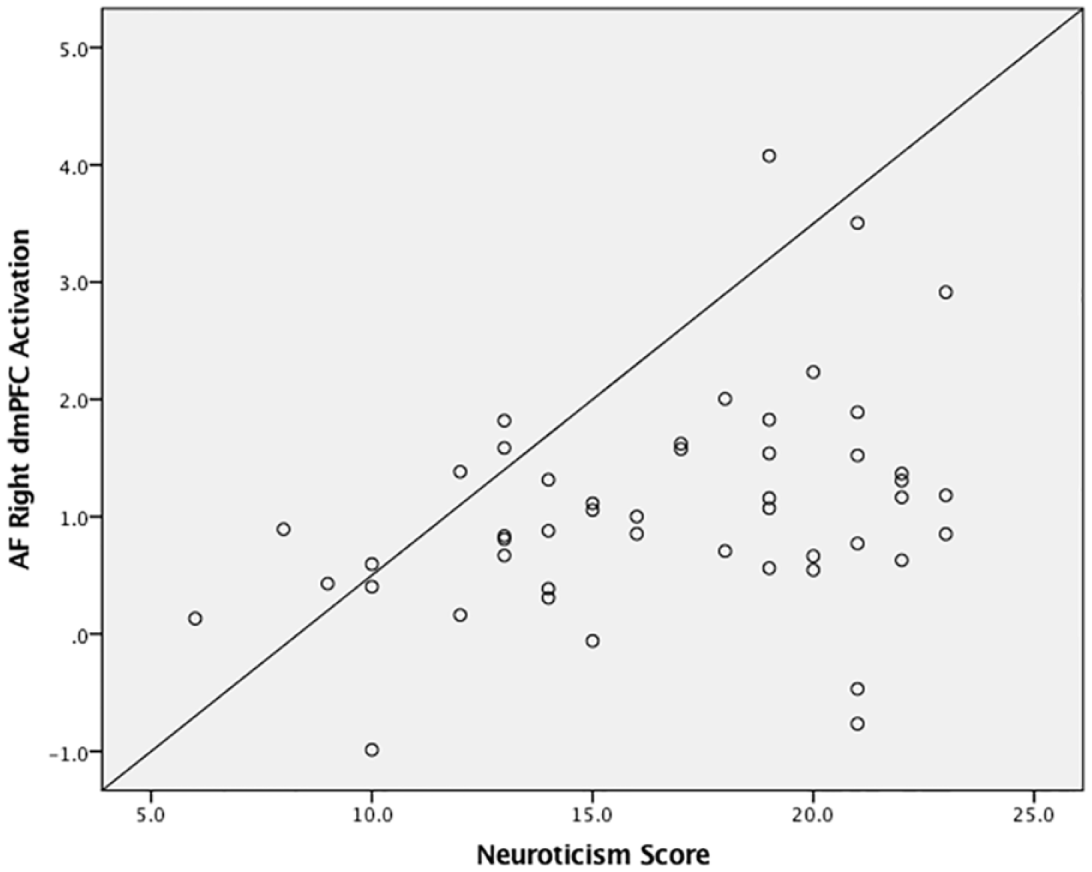
Scatterplot illustrating the relationship found in the PTSD group between right dmPFC activation and neuroticism for the AF condition.
IF Correlation Analyses
A series of correlation analyses were completed for each group to examine whether or not neuroticism scores were associated with activation in the brain ROIs when participants had to ignore fearful faces. For participants in the PTSD group ignoring fearful faces, neuroticism scores were significantly associated with activation in the right parahippocampus (r = .29, p = .05; see Figure 3) and right amygdala (r = .34, p = .02; see Figure 4). No significant trends or associations were found between neuroticism scores and activation in the left parahippocampus, left hippocampus, right hippocampus, left dmPFC, right dmPFC, left ACC, right ACC, or left amygdala for the PTSD group. Again, with regard to participants in the control group ignoring fearful faces, no significant correlations or significant trends emerged between neuroticism scores and activation in any of the brain ROIs.

Scatterplot illustrating the relationship found in the PTSD group between right parahippocampus activation and neuroticism for the IF condition.

Scatterplot illustrating the relationship found in the PTSD group between right amygdala activation and neuroticism for the IF condition.
Discussion
Results of this study indicate that women with PTSD endorsed substantially higher levels of neuroticism than psychologically healthy women without a trauma history, thus providing additional evidence for neuroticism’s role in the proposed diathesis-stress model of PTSD development. Results of the behavioral task performance revealed further differences between the two groups of women, as the control group was significantly better at discerning briefly presented facial pairs than the PTSD group. The PTSD group also demonstrated worse accuracy and longer response times when attending to fearful faces than when ignoring fearful faces. PTSD symptomatology thus appears to disrupt performance on tasks involving exposure to negatively affective stimuli, and in particular, tasks in which individuals are asked to directly attend to faces with a negative emotional valence.
With respect to specific brain activation, results indicated that women with PTSD had a significant association between high neuroticism scores and increased activity in the right dmPFC for the AF condition. Individuals prone to experiencing negative emotion, presumably stemming from a combination of elevated PTSD symptoms and elevated neuroticism, are thus expending considerable executive functioning capacity to modulate their emotions. As suggested by Servaas et al. (2013), these individuals may require greater levels of dmPFC activation to successfully engage in effective regulatory processes (e.g., reappraisal) aimed at reducing the perceived threat of stimuli. This notion also supports the trending relationship between neuroticism and ACC activation for the AF condition, given the ACC’s proposed role in emotion regulation (Hofmann et al., 2012). Thus, findings suggest that establishing control of one’s emotional state was most difficult for participants with PTSD when they were instructed to attend to faces demonstrating negative affect.
The PTSD group also demonstrated a significant association between high neuroticism scores and increased right parahippocampal activation for the IF condition. This finding was consistent with previous research that has demonstrated a relationship between high levels of parahippocampal activation and neuroticism when healthy individuals were exposed to a situation in which they expected an emotionally aversive stimulus based on prior experience (Coen et al., 2011). However, hippocampal activation was not associated with higher neuroticism in the PTSD group, an inconsistent finding with previous research (Hooker et al., 2008). These divergent results may be due to differences in study sample, as Hooker et al.’s (2008) investigation was comprised of healthy males and females. Indeed, previous research examining brain activity in men and women with PTSD found that men exhibited greater hippocampal activation than women in response to fearful facial stimuli (Felmingham et al., 2010). It is thus possible that neuroticism is related to parahippocampal activation regardless of PTSD diagnosis, while the relationship between hippocampal activation and neuroticism is not present in females with PTSD.
Finally, higher neuroticism scores were found to be associated with greater right amygdala activation in the IF condition for individuals in the PTSD group. Furthermore, a statistical trend emerged within the PTSD group between higher neuroticism scores and greater right amygdala activation in the AF condition. This finding is largely consistent with previous research demonstrating the amygdala’s role in recognition of emotions, as well as research exhibiting the relationship between amygdala activation and neuroticism (Chan et al., 2008; Dalgleish, 2004; Meunier et al., 1999). Moreover, our results provide further support of the generalized role of emotional processing that the amygdala plays, as well as the increased emotional sensitivity demonstrated by highly neurotic individuals (Canli, 2008). It also extends our prior findings demonstrating greater amygdala activation in the IF condition in major depression, a disorder that has a large overlap with neuroticism traits (Fales et al., 2008; Sheline et al., 2001).
This study is not without limitations. Within the conflict task, neutral faces were used as a comparison with more emotionally laden faces. However, it is possible that neutral faces could be viewed by PTSD participants as more negative than previously thought. For example, recent research on neutral stimuli showed that participants with depressive symptoms were more likely to perceive the stimuli as negative (Nejad, Fossati, & Lemogne, 2013). Furthermore, given that our healthy control group was nontrauma exposed, it cannot be determined whether differences in outcomes related to neuroticism and brain functioning were associated with IPV exposure or PTSD development subsequent to IPV. Finally, due to our sample size, we were not able to control for the neurological and behavioral effects of the comorbid diagnoses in our sample. Thus, generalizability to women with only PTSD is limited. However, given the high rates of comorbid psychopathology usually found in individuals with PTSD (Kessler, Sonnega, Bromet, Hughes, & Nelson, 1995), it is likely that this information would yield limited meaning and further decrease external validity.
Despite these limitations, results of this study provide further understanding of the relationship between neuroticism and PTSD in women with a history of IPV. To our knowledge, this is the first study to examine the neural correlates of neuroticism within the context of PTSD. Overall, our findings indicate a strong association between neuroticism and increased activation in brain regions associated with PTSD. It appears that women with high levels of neuroticism, in concert with PTSD symptomatology, demonstrate dysregulation within brain structures that are believed to influence emotional processing and regulation. It is promising that recent studies have shown neuroticism to be less stable than once believed, as this presents an opportunity to directly target neuroticism in treatment (Nivard, Middeldorp, Dolan, & Boomsma, 2015; Renner, Penninx, Peeters, Cuijpers, & Huibers, 2013). Indeed, treatments incorporating psychoeducation about reactions to negative emotions, as well as training in behavior modification when responding to stressful situations (e.g., emotion regulation skills) have demonstrated success (Barlow, Sauer-Zavala, Carl, Bullis, & Ellard, 2014; Carl, Gallagher, Sauer-Zavala, Bentley, & Barlow, 2014). Moreover, serotonergic pharmacological agents have been shown to decrease amygdala activation in response to fearful facial stimuli, thus indirectly exhibiting the neurological effect that treatment may have on neuroticism (Soskin, Carl, Alpert, & Fava, 2012). Future research should continue to explore the neural effects of neuroticism on the development and maintenance of PTSD. These findings should be replicated in a sample of both male and female participants, as previous research suggests sex differences in emotional processing (Felmingham et al., 2010; Weisenbach et al., 2014). Nevertheless, our results indicate that neuroticism plays a role in neural functioning in women with PTSD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Grants NIMH 1K23 MH090366-01 and NIMH 1RC1 MH089704-01.