
Abstract
Childhood trauma is common among survivors and perpetrators of intimate partner violence (IPV). Although symptoms of posttraumatic stress disorder (PTSD) and dissociative disorders (DDs) are predictors of IPV victimization and perpetration, few studies explore IPV among those with DDs. The present study examined IPV and symptoms as predictors among participants in the Treatment of Patients With Dissociative Disorders (TOP DD) Network study, an educational intervention for individuals with DDs and their clinicians. Both clinicians and patients reported on patients’ history of physical, emotional, and sexual IPV as both victims and perpetrators. Patients self-reported dissociative, posttraumatic (PTSD), and emotion dysregulation symptoms, as well as IPV-specific dissociative symptoms. According to patients and clinicians, patients were frequently victims of IPV, most commonly emotional IPV. Dissociative symptoms predicted IPV exposure, whereas dissociative and emotion dysregulation symptoms predicted IPV-specific dissociative symptoms.
Intimate partner violence (IPV), including physical, sexual, emotional, and/or psychological abuse incurred from a current or former partner, is an endemic public health issue in the United States and worldwide. Globally, one in three women experiences physical and/or sexual violence in their lifetime (Garcia-Moreno et al., 2013). In the United States, a little above one third of women (37.3%) and a little less than one third of men (30.9%) report physical abuse, sexual abuse, and/or stalking by intimate partners during their lifetime, whereas about half of women (47.1%) and men (47.3%) experience psychological aggression by intimate partners (Smith et al., 2017). IPV victims, particularly women who experience physical and sexual abuse, are at increased risk of adverse health outcomes including depression, alcohol abuse, and contracting HIV or another sexually transmitted infection (Garcia-Moreno et al., 2013).
Childhood physical, sexual, and emotional abuse, as well as exposure to traumas such as familial domestic violence (DV) and neglect, are risk factors for IPV victimization and perpetration, although differences exist across victim gender and type of violence exposure (Eriksson & Mazerolle, 2015; McMahon et al., 2015; Milaniak & Widom, 2015; Millett, Kohl, Jonson-Reid, Drake, & Petra, 2013; Widom & Wilson, 2015). The developmental trajectory from childhood to adult abuse is important to address, given that childhood abuse occurs among 20% to 40% of all adults, with nearly one in three adults reporting childhood physical abuse and one in five adults reporting childhood sexual abuse (Felitti et al., 1998). The psychological outcomes of childhood trauma may increase risk of IPV, such as dissociation, a theorized coping mechanism for children experiencing severe and frequent physical and sexual abuse perpetrated by a trusted caregiver (Brand et al., 2013; Dalenberg et al., 2012; Foote, 2013; K. T. Putnam, Harris, & Putnam, 2013; Trickett, Noll, & Putnam, 2011).
Dissociation is a discontinuity and/or fragmentation in an individual’s identity, consciousness, memory, emotions, sensory perception, and/or bodily and motor control (Diagnostic and Statistical Manual of Mental Disorders [5th ed.; DSM-5]; American Psychiatric Association [APA], 2013). Dissociation is adaptive when used by children in abusive situations they cannot otherwise cope with or escape, but its continued use in adulthood becomes maladaptive and, if used excessively, can be a disorder when it is no longer needed to survive abuse. Dissociative disorders (DDs) are characterized by one or more core dissociative symptoms including amnesia, depersonalization (e.g., feeling oneself is unreal), derealization (e.g., feeling one’s surroundings are unreal), identity confusion, and identity alteration (e.g., experiencing oneself as having unintegrated identities; APA, 2013; Brand et al., 2009; Foote, 2013; International Society for the Study of Trauma and Dissociation, 2011).
A handful of studies have explored the role of dissociative symptoms in IPV, including as a predictor of adult interpersonal revictimization (Daisy, 2005; Iverson et al., 2013; Noll, Horowitz, Bonanno, Trickett, & Putnam, 2003), a mediator of the relationship between childhood abuse and adult IPV (Daisy & Hien, 2014), a mediator of the relationship between adult IPV and posttraumatic stress disorder (PTSD)-related dissociation (Fleming & Resick, 2016), and a predictor of PTSD symptoms among victims of IPV (Seedat, Stein, & Carey, 2005). In addition, high rates of dissociation and DDs have been found among IPV victims (Basu, 2010; Cuevas, Sabina, & Picard, 2010; Marchiori, Rossi, & Colombo, 2004; Stein, 2012; Temple, Weston, & Marshall, 2010) and perpetrators (Cuartas, 2002; Dutton, Fehr, & McEwen, 1982; LaMotte & Murphy, 2017; Lau & Stevens, 2012; Simoneti, Scott, & Murphy, 2000).
A smaller group of studies have examined IPV among those with DDs, typically via clinician report, with conflicting findings. Putnam, Guroff, Silberman, Barban, and Post (1986) found 29% of those with dissociative identity disorder (DID) reported homicidal behavior, 20% reported perpetrating rape, and 6% reported committing homicide. In an all-male sample, Loewenstein and Putnam (1990) reported criminal violent behavior and incarceration in 47% of those with DID, homicide in 19%, and rape perpetration in 13%. More recent studies of IPV among those with DDs suggest high rates of interpersonal victimization but lower rates of perpetration, compared with earlier studies. Using clinician reports of their patients, Webermann, Brand, and Chasson (2014) reported adult lifetime physical IPV rates of 29.6% (with 26.1% reporting victimization only without perpetration, and 3.5% reporting both victimization and perpetration) and adult lifetime emotional IPV rates of 58.8% (with 48.9% reporting victimization only without perpetration, and 9.9% reporting both victimization and perpetration). Assessing the same DD sample longitudinally over the prior 6 months, therapists reported physical IPV among 4.1% to 7.1% of patients, and emotional IPV among 29% to 36% (Myrick, Brand, & Putnam, 2013). Both the cross-sectional and longitudinal studies found that IPV was only perpetrated by those who were also victimized.
Krüger and Fletcher (2017) examined variables that predicted DDs including type of IPV (physical, emotional, and sexual abuse, and physical and emotional neglect) and relationship to perpetrator (biological family or intimate partner) among a psychiatric inpatient sample. They found emotional abuse was most predictive of DDs, including emotional neglect from biological family and emotional abuse from adult intimate partners. Notably, Myrick et al. (2013) and Webermann et al. (2014) assessed IPV through clinician reports, and no studies to date have obtained self-report IPV data from DD patients. This contrasts from other studies on trauma and IPV, where trauma and its symptomatology are assessed via self-report (Becker-Blease & Freyd, 2007; D. G. Dutton, 1995; Ellason & Ross, 1999; Hulnick, 1997; Leibowitz, 2007; Lewis, Yeager, Swica, Pincus, & Lewis, 1997; Ross, 2008; Simoneti et al., 2000). Comparing IPV reports from clinicians and patients would provide a better understanding of IPV and, possibly, highlight reporting discrepancies.
PTSD symptoms and emotion regulation may also play a role in IPV victimization and perpetration. A study of men in an abuser intervention program found that 77% reported at least one potentially traumatic event, 62% reported multiple traumatic events, and 11% screened above the cutoff indicating a possible PTSD diagnosis (Semiatin, Torres, LaMotte, Portnoy, & Murphy, 2017). In addition, other studies suggest PTSD symptoms predict IPV revictimization (e.g., Iverson et al., 2013; Kuijpers, van der Knaap, & Winkel, 2012; Matlow & DePrince, 2013). Others have identified emotion dysregulation as a predictor of IPV perpetration (Bliton et al., 2016; McNulty & Hellmuth, 2008), a mediator between proximal negative affect and physical IPV perpetration (Shorey, McNulty, Moore, & Stuart, 2015), a mediator between childhood maltreatment and IPV perpetration (Gratz, Paulson, Jakupcak, & Tull, 2009), and a mediator of PTSD symptoms among childhood abuse survivors (Lilly, London, & Bridgett, 2014). Importantly, although PTSD symptoms and emotion dysregulation are common among those with DDs, they have yet to be examined as risk factors for IPV among those with DDs.
The Present Study
Further examination of the role of dissociation in IPV, and IPV among those with DDs, is needed. Thus, the present study aims to examine the prevalence and typology of IPV among individuals with DDs through their self-report and clinicians’ reports, examine IPV-specific dissociative symptoms among patients with DDs through self-report, and assess predictors of IPV and IPV-specific dissociative symptoms among DD patients. We hypothesized the following:
Method
Participants
Clinician and patient participants were recruited from the Treatment of Patients With Dissociative Disorders (TOP DD) Network study, the second iteration of the TOP DD study (Brand et al., 2009; Brand et al., 2013). TOP DD Network was an online outpatient psychoeducational intervention of outpatients with DDs diagnosed with either DID or DD not otherwise specified/other specified DD. The TOP DD Network study included 237 clinicians and 242 of their patients who completed baseline measures, presented after the screen measures, which verified study eligibility. Both the patient and clinician providing psychotherapy were required to enroll together to ensure that all patients had professional assistance in case of crisis. The TOP DD Network study was approved by the Institutional Review Board of Towson University, and patient and clinician participants completed an informed consent process. TOP DD Network study patient participants were primarily female (88.6%), Caucasian (82.1%), middle aged (median = 41), highly educated (50.9% had a college diploma or more), and U.S. citizens (42.3%), although a sizable portion derived from Norway (27.5%) as well as a number of other countries (30.2%). Half of participants (55.2%) were either in a dating or married relationship. Patients were primarily diagnosed with DID (63.4%). This sample had high rates of childhood trauma, as reported by clinicians: 84% had been emotionally abused, 80.6% had been sexually abused, 64.1% had been physically abused, 62% had been neglected, and 43.9% had witnessed DV in their family of origin. This aligns with extant research on DDs, which suggests that severe and chronic childhood abuse may lead to dissociation and subsequent fragmenting of one’s identity. DD samples report rates of childhood abuse between 80% and 95% (e.g., Brand et al., 2009; Foote, 2013). Clinician participants were primarily female (80%) and Caucasian (91.3%). Most reported multiple years of experience as therapists (median = 15), as well as in treating trauma (median = 13) and dissociation (median = 8). Clinicians primarily worked in private practice (81.1%) or an outpatient clinic or hospital (41.6%).
A subset of 45 patient participants (18.6% of all patient participants) completed additional and optional self-report measures on IPV and IPV-related dissociative symptoms. The subsample was middle aged (median = 42) and Caucasian (83.7%), with a smaller subsample of Asian (9.3%) and African American (4.7%) participants, highly educated (51.1% with a college degree), and primarily female (76.7%). About half (58.1%) were in dating or married relationships. Therapists reported similar years of clinical experience (median = 15), treating trauma (median = 13), and treating dissociation (median = 8) as the larger therapist sample.
Procedures
Patient and clinician participants in the TOP DD Network study watched weekly 7- to 15-min psychoeducational and skills training videos, and patients completed written reflection and behavioral exercises. At the conclusion of the video for Week 24, patients were offered a survey titled “Optional Patient Survey” that contained the IPV and dissociative violence measures utilized in the present study. The prompt indicated to patients the potential emotional difficulty of the survey and emphasized that the completion of the survey was optional:
There is an optional 25-minute survey offered at week 24 that patients may opt to complete if they so choose. This optional survey asks brief questions about traumas, attachment and violence. This information may be useful for therapists to know about and process with the patient, so this survey might be useful to complete when the client is with the therapist.
The rationale of including the optional survey 24 weeks (i.e., 6 months) into the program was that patients would be acclimated to the Network program content and its surveys, and better equipped with symptom management skills to review and complete a potentially emotionally challenging survey. Data for the present study were collected from baseline surveys conducted on Qualtrics from March 2015 to December 2016.
Patient Measures
Relationship violence perpetration and victimization
Perpetration and victimization in adult romantic relationships were assessed through the Revised Conflict Tactics Scale Short Form (CTS2S; Straus & Douglas, 2004). The CTS2S is a 20-item, shortened version of the full 78-item Revised Conflicts Tactics Scale (CTS2; Straus, Hamby, Boney-McCoy, & Sugarman, 1996). Subscales include physical aggression (i.e., physical IPV), psychological aggression (i.e., emotional IPV), and sexual coercion (i.e., sexual IPV). Each subscale assesses minor and severe IPV, as well as both perpetration (e.g., I yelled at my partner) and victimization (e.g., my partner yelled at me). The CTS2S has concurrent and construct validity with the full CTS2 (r = .65-.94; Straus & Douglas, 2004). The measure was scored into dichotomous variables indicating any history of physical, sexual, or emotional IPV, as victims and/or victim–perpetrators. Internal consistency for the CTS2S in the present sample was α = .73.
Dissociative experiences during IPV perpetration
Peritraumatic dissociation occurring during an aggressive interpersonal episode was assessed through the nine-item Dissociative Partner Violence Scale (DPVS; Simoneti et al., 2000). The following dissociative symptoms were assessed: feeling as if someone else was being aggressive with your partner and not you, depersonalization (feeling yourself from a distance aggressing; feeling you were not real), derealization (feeling the other person was unreal), dissociative callousness (unable to show sympathy for your partner’s pain), amnesia for violent episodes (blackouts not due to drinking or drugs/accused of partner violence but don’t remember), and violence-related flashbacks (flashbacks of past violence; violent in ways you’ve only seen in a dream). Mantakos (2008) reported an internal consistency of α = .78, and criterion, convergent, and discriminant validity. Each item on the measure was summed to obtain a frequency score. Internal consistency for the DPVS in the present sample was α = .82.
Trait dissociation
The Dissociative Experiences Scale (DES; Carlson & Putnam, 1993) is a 28-item, 11-point scale (ranging from 0% to 100% of the time), where the participant indicates what percentage of the time a particular dissociative experience occurred in the past month. van Ijzendoorn and Schuengel (1996) demonstrated test–retest reliability of .78 to .93, α = .93, and convergent validity of r = .67. The measure was scored by adding the item frequency values and dividing by the total number of items, yielding an average summary score for each participant. Internal consistency for the DES in the present sample was α = .96.
Posttraumatic symptoms
The Posttraumatic Checklist–Civilian (PCL-C; Weathers, Litz, Huska, & Keane, 1994) is a 17-item measure of PTSD symptom severity mapping onto criteria for Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; APA, 2000) that encompasses re-experiencing, avoidance and numbing, and arousal, without reference to any specific trauma. Respondents indicate the degree to which symptoms have bothered them within the last month using a 5-point scale (1 = not at all to 5 = extremely). All items are summed, and a cutoff score of 50 is consistent with a PTSD diagnosis (Weathers & Ford, 1996). PCL-C has strong test–retest reliability and validity (Brand et al., 2009). Internal consistency for PCL-C in the present sample was α = .88.
Emotion dysregulation
The Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, 2004) is a 36-item measure of six types of emotion dysregulation: nonacceptance of emotions, difficulties engaging in goal-directed behavior, impulse control difficulties, lack of emotional awareness, limited emotion regulation strategies, and lack of emotional clarity. The DERS has strong internal consistency, construct validity with the Generalized Expectancy for Negative Mood Regulation Scale (a common measure of emotion regulation), and predictive validity for self-harm and partner abuse (Gratz & Roemer, 2004). Internal validity for the DERS in the present sample was α = .84.
Clinician Measures
IPV
Clinician reports of patients’ history of physical, emotional, and sexual IPV victimization and perpetration in adulthood were assessed through the following question: “Has the patient been in a(n) (physically, emotionally, or sexually) abusive relationship as an adult?” If the clinician responded yes to any question, they were asked whether the patient was the victim, perpetrator, or both (e.g., victim–perpetrators). In contrast to the patient IPV self-report measure (via the CTS2S), IPV was not behaviorally defined within the clinician IPV measure, or differentiated by severity. The measure was scored dichotomously into categorical variables that indicated the presence or absence of each type of IPV.
Analyses
Hypothesis 1, that emotional IPV would be the most prevalent type of IPV, was assessed through examining IPV frequencies reported by patients and clinicians. Hypothesis 2, that patients would report more IPV than clinicians, was assessed through Z tests comparing IPV prevalence proportions reported by clinicians and reported by patients. Hypotheses 3 and 4, that greater dissociative symptoms, but not PTSD and emotion regulation symptoms, would predict IPV as well as IPV-specific dissociative symptoms, were assessed through discriminant analyses examining whether severity of dissociative, PTSD, and emotion dysregulation symptoms (via the DES, PCL-C, and DERS, respectively) could predict patients with a history of IPV and/or a history of IPV-specific dissociative symptoms (via the CTS2S and therapist reports, and DPVS, respectively). IPV perpetrators and victims were merged in analyses because more than 90% of IPV reported involved victimization alone or both victimization and perpetration. Thus, the following should be interpreted as indicating a history of an abusive adult relationship, rather than an indication of IPV victimization or perpetration. To correct for inflation of Type I error, we applied an alpha correction through the false discovery rate (FDR) control procedure of αcritical = .019.
Results
Descriptive statistics for clinician and patient-reported IPV are listed in Tables 1 and 2.
Descriptive Statistics and Z Test Comparisons of Clinician and Patient Reports of IPV.

Note. IPV = intimate partner violence.
18.6% of total patient sample.
p < .05. **p < .01. ***p < .001.
Descriptive Statistics and Symptomatic Predictors of IPV-Specific Dissociative Symptoms (N = 44).
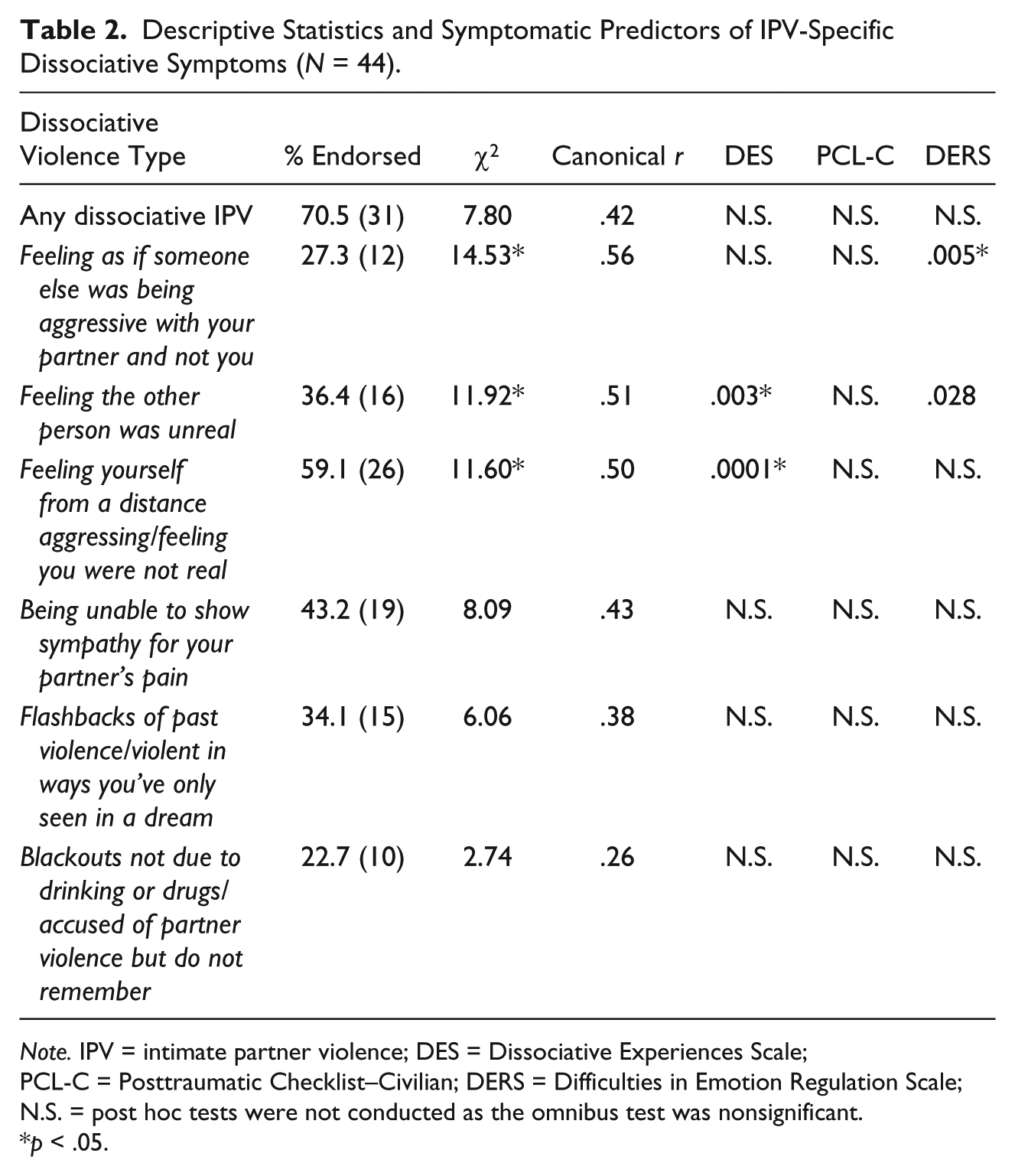
Note. IPV = intimate partner violence; DES = Dissociative Experiences Scale; PCL-C = Posttraumatic Checklist–Civilian; DERS = Difficulties in Emotion Regulation Scale; N.S. = post hoc tests were not conducted as the omnibus test was nonsignificant.
p < .05.
Comparison of Clinician- Versus Patient-Reported IPV Prevalence
Regarding DD patients’ rates of physical IPV, patients self-reported higher rates of total physical IPV (Z = 3.06, p < .001) and physical victimization–perpetration (Z = 5.98, p < .01) than their clinicians, but there were no differences in reports of physical victimization between clinicians and patients (Table 1). Regarding emotional IPV, differences in total emotional IPV were nonsignificant but trended toward significance (Z = 1.89, p = .06), whereas clinicians reported more emotional victimization (Z = 5.12, p < .001), and patients self-reported more victimization–perpetration (Z = 8.71, p < .001). Finally, there were no differences in clinician and patient reports of sexual IPV, including total sexual IPV (Z = 1.09, p = .28), sexual victimization (Z = 0.81, p = .42), and sexual victimization–perpetration (Z = 0.92, p = .36).
Symptomatic Predictors of Clinician-Reported IPV
Patient-reported trait dissociation differentiated DD patients with a history of clinician-reported physical IPV, χ2(1) = 22.20, p < .001, canonical r = .31, as well as clinician-reported sexual IPV, χ2(1) = 12.89, p < .005, canonical r = .24. Neither PTSD nor emotion dysregulation symptoms differentiated those who experienced physical or sexual IPV. Although patients with a history of adult emotional IPV had more severe trait dissociation (M = 39.92, SD = 21.27) than those without a history of emotional IPV (M = 37.23, SD = 18.79), trait dissociation did not differentiate DD patients with a history of emotional IPV, nor did PTSD and emotion dysregulation symptoms (Table 3).
Symptomatic Predictors of IPV (N = 45).
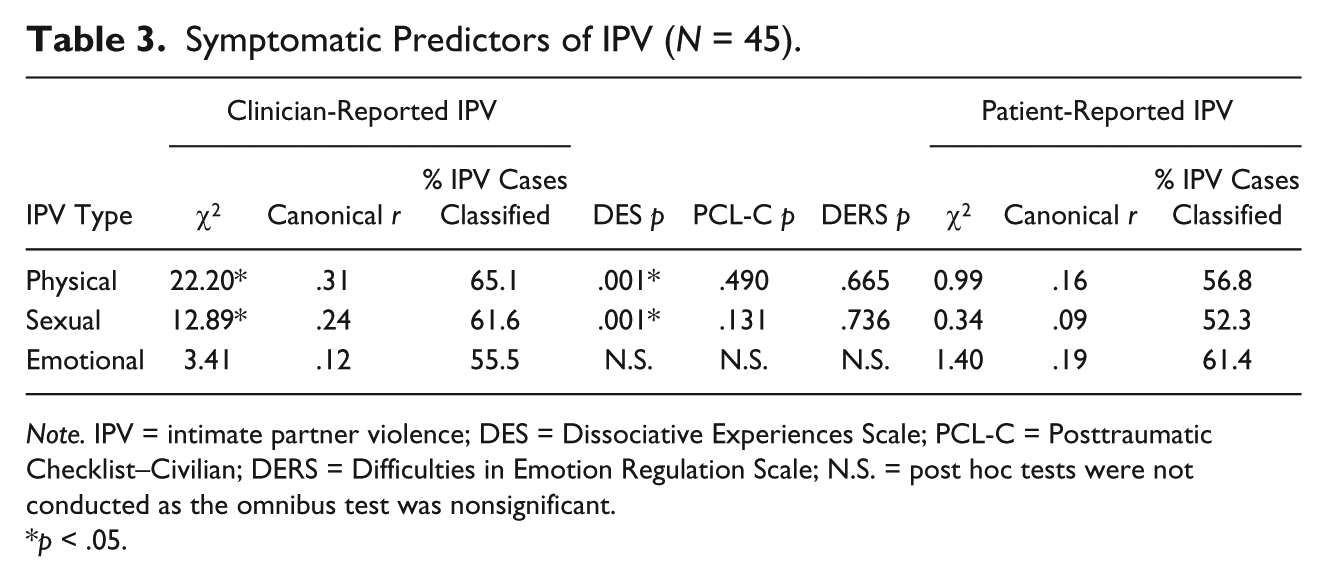
Note. IPV = intimate partner violence; DES = Dissociative Experiences Scale; PCL-C = Posttraumatic Checklist–Civilian; DERS = Difficulties in Emotion Regulation Scale; N.S. = post hoc tests were not conducted as the omnibus test was nonsignificant.
p < .05.
Symptomatic Predictors of Patient-Reported IPV
Trait dissociation did not differentiate which DD patients self-reported a history of physical, sexual, or emotional IPV via the CTS2S (Table 3). That is, although dissociative symptoms could differentiate which patients have a history of IPV as reported by clinicians, it could not differentiate which patients have a history of self-reported IPV (within the subsample of 18.6% of patients who completed the optional self-report measures), likely due to low power.
Symptomatic Predictors of Patient-Reported Dissociative Violence
A composite predictor variable of trait dissociation, PTSD, and emotion dysregulation predicted general IPV-specific dissociative symptoms, χ2(1) = 7.80, p < .05, canonical r = .42; feeling someone aggressing who wasn’t you, χ2(1) = 14.53, p < .005, canonical r = .56; IPV-specific derealization (feeling your partner was unreal), χ2(1) = 11.92, p < .01, canonical r = .51; IPV-specific depersonalization (seeing yourself from a distance aggressing and feeling disconnected from your body), χ2(1) = 11.60, p < .01, canonical r = .50; and IPV-specific dissociative callousness (unable to show sympathy for partners’ pain), χ2(1) = 8.09, p < .05, canonical r = .43. After applying the critical p value of .19, the composite predictor variable was no longer able to significantly predict general IPV-specific dissociative symptoms (p < .05) or IPV-specific dissociative callousness (p < .04). In post hoc ANOVAs for the significant dissociative IPV outcomes, only trait dissociation predicted IPV-specific derealization (p < .003) and IPV-specific depersonalization (p < .001), whereas only emotion dysregulation symptoms predicted feeling someone was aggressing who wasn’t you (p < .005).
Discussion
The present study contributes to the limited literature on dissociation and IPV within DD individuals by examining IPV prevalence, IPV-specific dissociation, and symptomatic predictors of both IPV and IPV-specific dissociation among individuals with DDs in the TOP DD Network study, an online outpatient psychoeducational intervention. According to participants with DDs and their clinicians, the majority of individuals with DDs have been involved in an abusive relationship as adults. Most participants (60.8%-75.6%) experienced emotional IPV, a little above one third (35.9%-44.4%) experienced sexual IPV, and about a quarter to a half (26.1%-48.9%) experienced physical IPV. These high rates of IPV underscore the importance of further understanding what contributes to IPV in this population. Our goal in this study was increase knowledge about the role of trait and IPV-specific dissociation in IPV, as well as the possible contribution of PTSD symptoms and emotion dysregulation to IPV in individuals with DD.
The first hypothesis, that emotional IPV would be the most frequent type of IPV, was supported. This echoes findings from the two previous studies of IPV among an earlier, naturalistic TOP DD study of DD patients (Myrick et al., 2013; Webermann et al., 2014), wherein emotional IPV was the most common type of IPV reported among patients with any adult history of IPV as well as those who had recently experienced IPV. The nearly universal experience of emotional IPV among those with DDs is of clinical significance given that psychological and emotional abuse, above and beyond physical abuse and sexual coercion, are predictive of PTSD symptoms among IPV survivors (Krüger & Fletcher, 2017; Mechanic, Weaver, & Resick, 2008; Norwood & Murphy, 2012). Other studies have found a link between IPV and PTSD among childhood trauma survivors, wherein trauma-related appraisals mediate or predict negative mental health outcomes for IPV survivors (Brown, 2016; Fleming & Resick, 2016), and betrayal trauma predicts ongoing IPV among IPV survivors (Babcock & DePrince, 2013).
The second hypothesis, that patients would self-report more IPV than their treating clinicians would report about them, was also supported. Significant differences were found in the proportion of total physical IPV, as well as physical and emotional victimization–perpetration (because all IPV perpetrators were also victims of IPV) reported by patients and clinicians. Studies on IPV victims and perpetrators in clinical samples typically rely on patient self-reports rather than clinician reports, but the few studies on IPV among patients with DDs used only clinician reports (Loewenstein & Putnam, 1990; Myrick et al., 2013; Putnam et al., 1986; Webermann et al., 2014). This is clinically relevant as clients may not disclose IPV in clinical settings due to fears of not being believed or helped, fears of negative consequences or retaliation, and feelings of shame and guilt (Howard, 2013; Mertin, Moyle, & Veremeenko, 2015; Othman, Goddard, & Piterman, 2014; Rose et al., 2011; Trevillion et al., 2014). In addition to these issues, patients may have reported more IPV due to methodological issues: The CTS2S is a behaviorally descriptive measure of both mild and severe IPV, whereas clinicians responded to a yes–no question about whether their patients had an IPV history as victims or perpetrators. A yes/no IPV assessment relies on clinicians’ understanding of the nature of IPV, and answers depend on what is considered abusive, whereas CTS2S asks about the incidence of “relationship behaviors.”
The third hypothesis, that trait dissociation, but not PTSD or emotion dysregulation symptoms, would predict IPV history, was partially supported. Only dissociation severity significantly predicted which patient participants had a history of clinician-reported physically and sexually abusive relationships, but not emotionally abusive relationships. In addition, PTSD and emotion regulation measures were not predictive of IPV. These findings lend credence to the notion that dissociation may increase risk of IPV (e.g., Basu, 2010; Cuartas, 2002; Cuevas et al., 2010; Daisy, 2005; D. Dutton et al., 1982; Iverson et al., 2013; Krüger & Fletcher, 2017; LaMotte & Murphy, 2017; Lau & Stevens, 2012; Marchiori et al., 2004; Simoneti et al., 2000; Stein, 2012; Temple et al., 2010). The present study suggests that those highest in trait dissociation, even among this highly dissociative sample, are at higher risk of IPV. This finding underscores the importance of addressing dissociation at the beginning, as well as throughout treatment, for individuals with DDs, a recommendation that is consistent with expert treatment guidelines (International Society for the Study of Trauma and Dissociation, 2011). Longitudinal research is needed to determine whether a decreasing dissociation over time in treatment causes a reduction in DD patients’ high rates of IPV.
Our finding that neither PTSD symptoms nor emotion regulation predicted IPV among those with childhood trauma aligns with literature, indicating that other trauma-related variables are more relevant to predicting IPV than are PTSD and emotion dysregulation, such as cognitive trauma-related appraisals (Brown, 2016; Fleming & Resick, 2016), coping style (Iverson et al., 2013), and betrayal trauma (Babock & DePrince, 2013). Although there is evidence that emotion regulation and PTSD symptoms may play a role in IPV, studies have been mixed, and rarely find a direct correlation or predictive relationship between PTSD and emotion regulation and IPV.
The fourth hypothesis, that only trait dissociation, but not PTSD or emotion dysregulation symptoms, would predict which patient participants had a history of IPV-specific dissociative symptoms, was partially supported. Both dissociation and emotion dysregulation predicted IPV-specific dissociative symptoms. Emotion dysregulation predicted which patient participants reported feeling someone else was aggressing against their partner and not them, whereas trait dissociation predicted derealization (feeling their partner was unreal) and depersonalization (feeling themselves aggressing from a distance/perceiving themselves as unreal). This contributes to the limited literature on IPV-specific dissociative symptoms (Cuartas, 2002; Fleming & Resick, 2016; LaMotte & Murphy, 2017; Simoneti et al., 2000). It is also noteworthy that 70.5% (n = 31) of the patient sample reported at least one instance of IPV-specific dissociation, the most common of which were depersonalization (feeling themselves aggressing from a distance/perceiving themselves as unreal; 59.1%, n = 26) and dissociative callousness (unable to show sympathy for their partner’s pain; 43.2%, n = 19). Given that those with DDs chronically dissociate during stressful and traumatic situations (e.g., Brand et al., 2009; Brand et al., 2013; Dalenberg et al., 2012; Foote, 2013), it follows that they would also dissociate during partner abuse experiences. In addition, the DES includes items measuring depersonalization (although not callousness), so a significant association between the measures is not surprising. That is, if an individual tends to frequently experience trait depersonalization, it is predictable that he or she would also be at risk of experiencing depersonalization during IPV.
Among survivors of childhood abuse who experience dissociation, trait dissociation might contribute to involvement in abusive relationships through the following mechanisms: emotional detachment from, and/or amnesia for, childhood abuse experiences, which might be reenacted in adult relationships, rather than being integrated into a coherent, organized trauma narrative; a fragmented sense of self that may interfere with more consistent empathy across situations for one’s partner; a lack of adaptive coping skills, which could leave an individual with limited communication skills and low tolerance for conflict; attachment to, and/or identification with, an abusive caregiver; and insecure attachment, which could increase risk of experiencing IPV (Byun, Brumariu, & Lyons-Ruth, 2016; Dalenberg et al., 2012; Kluft, 1989; Putnam, 1991).
Limitations
The present subsample of patients who completed the optional measures (the CTS2S and DPVS) was small (N = 44-45), thus limiting the power of analyses involving patient-reported IPV and IPV-related dissociative symptoms. This prevents us from conducting analyses to parse out victims and perpetrators, given the small number of patients who perpetrated IPV. In addition, the patient sample may not generalize to those with DDs not in outpatient treatment, or to more diverse DD populations. However, the TOP DD Network study is typical of DD clinical research populations (Brand et al., 2013). Finally, the measures assessing patients’ self-reported IPV and clinicians’ report of patients’ IPV history differed considerably in degree of specificity and behavioral descriptors. These methodological differences may likely have contributed to the discrepancies in rates of IPV reported by patients versus clinicians, although both clinicians and patients reported high rates of IPV victimization among patients.
Implications and Conclusion
The present study is the first known study to utilize DD patient self-reports of their IPV history and to assess DD patients’ self-reported IPV-related dissociative symptoms. This study both echoes and builds upon the findings of the limited literature on the intersections of dissociation and interpersonal violence. As it is well established that experiencing trauma often begets exposure to future trauma, and there is a developmental trajectory between childhood abuse and IPV among the general population and among individuals with DDs, it is crucial to screen for both IPV victimization and perpetration among DD individuals.
Research is needed to better understand the mechanisms by which trait dissociation increases risk of IPV. A qualitative study of individuals who experience trait dissociation and IPV might be particularly useful in illuminating potential mechanisms linking dissociation and IPV. Survivors of childhood trauma, including those with DDs, are an important population in which to study IPV, for the purposes of intervening and preventing further trauma among trauma survivors. The nearly universal experience of severe and chronic childhood victimization among those with DDs, with their elevated trait dissociation and comorbid diagnoses, provides an important group with whom to develop a better understanding of how childhood trauma contributes to IPV. Practitioners in the IPV field are encouraged to assess IPV victims and perpetrators for trauma and trauma-based symptomatology, as a trauma-informed approach is crucial to any intervention that aims to prevent IPV or treat its outcomes. In addition, trauma and dissociation clinicians are encouraged to assess patients for current or recent IPV, as there is mounting evidence that individuals with DDs are at heightened risk of IPV. In many ways, researchers, clinicians, and the general public continue to be eluded by the dual questions of how individuals can perpetrate abuse toward a partner they purport to care for, as well as how individuals endure years of severe abuse from their partners. Studying IPV within a specialized population who evidence multiple risk factors for IPV might offer further insights into what mechanisms enable IPV to continue at such high rates across the life span.
Footnotes
Acknowledgements
The authors warmly thank the patients and therapists who generously donated their time to participate in the TOP DD Network study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors declare that this research was funded by foundations (i.e., ANS Research, Constantinidas Family Foundation), private donations (including from Anne Bartello and family, Brad Foote, MD, and gifts made to Sheppard Pratt Health System’s Trauma Disorders Research Program and Towson University’s Foundation), and grants from Towson University.