
Abstract
Complex trauma (CT; for example, childhood abuse) has been associated with significant behavioral health problems (i.e., mental health and substance use disorders) and symptoms that are consistent with complex posttraumatic stress disorder (C-PTSD). CT is prevalent in adult forensic populations, and particularly important for women as they tend to report more adverse consequences of exposure to traumatic stressors and are entering the criminal justice system at a heightened rate compared with men. However, no studies have empirically tested the relationship among CT, C-PTSD, and behavioral health problems with gender among incarcerated adults. The present study examined the relationship between gender and childhood abuse history, C-PTSD symptom severity, and behavioral health problems in 497 incarcerated adults. Findings indicate that women were more likely to report a history of childhood abuse, and more severe C-PTSD symptoms and behavioral health problems than men. Childhood abuse history significantly accounted for the gender difference observed in C-PTSD symptom severity. C-PTSD partially mediated the gender difference in psychiatric morbidity and in risk of hard drug use. Implications for trauma-informed and gender-responsive services and research in the adult criminal justice system are discussed.
Research has primarily focused on posttraumatic stress disorder (PTSD) when referring to gender differences in the consequences of exposure to traumatic stressors (Tolin & Foa, 2006). This article extends prior studies by examining potential gender differences in what is referred to as “complex trauma” (CT) and “complex posttraumatic stress disorder” (C-PTSD) symptoms, as well as the relationship to mental health and substance use disorders. CT represents a subset of the larger domain of traumatic stressors that involve extreme forms of interpersonal victimization, which compromise an individual’s basic sense of trust in self, relationships, and social contact (e.g., childhood abuse by putatively protective caregivers or other adults, torture, genocide, kidnapping; Cook et al., 2005). CT has been associated with more complex reactions that may include symptoms consistent with C-PTSD (Herman, 1993), as well as associated mental health and substance use disorders, which could result in criminal prosecution. Forensic populations have high rates of exposure to CT and associated problems, especially among women, who tend to report more adverse traumatic experiences and consequences than men (Scoboria, Ford, Lin, & Frisman, 2008). However, reasons for these potential gender differences have not been examined for C-PTSD symptoms, or their relationships to behavioral health problems (i.e., mental health and substance use disorders) among incarcerated adults. C-PTSD symptoms are thought to reflect underlying deficits and disruptions associated with CT, which could manifest in diagnosable mental health and substance use disorders (Ford, 2015; Herman, 1993). Therefore, the goals of this study are to identify potential gender differences in C-PTSD symptoms, and examine the relationship between CT, C-PTSD, and behavioral health problems in a sample of incarcerated men and women.
CT can have adverse effects on psychobiological development and often results in complex posttraumatic stress reactions (Cook et al., 2005; Herman, 1993; van der Kolk, Roth, Pelcovitz, Sunday, & Spinazzola, 2005). Interpersonal violence in the form of childhood abuse (physical, sexual, or emotional) is a highly impactful form of CT because it occurs during a developmentally formative period, often over an extended period of time, and tends to involve betrayal of the protective nature of primary caregiving relationship(s) (Freyd, 1994; Herman, 1993). In addition, childhood abuse often occurs in the context of other adversities including parental substance abuse and family violence (Dong, Anda, Dube, Giles, & Felitti, 2003; Dong et al., 2004; Edwards, Holden, Felitti, & Anda, 2003). Childhood abuse is also associated with an increased risk of future victimization and symptom complexity in adulthood (Briere, Kaltman, & Green, 2008; Browne, Miller, & Maguin, 1999; Cloitre et al., 2009; Dong et al., 2003; Ports, Ford, & Merrick, 2016; Schumm, Briggs-Phillips, & Hobfoll, 2006).
CT has been associated with a wide variety of behavioral health problems that involve dysregulation of emotion (e.g., inability to cope with or recover from intense affective distress including anger and shame, as well as anxiety and dysphoria), behavior (e.g., reactive aggression toward self or others), and self/identity (e.g., pathological dissociation or self-hatred; Girieballa et al., 2006; Spitzer, Chevalier, Gillner, Freyberger, & Barnow, 2006; Trestman, Ford, Zhang, & Wiesbrock, 2007). Although these forms of trauma-related dysregulation involve symptoms that are similar to those of numerous psychiatric and substance use disorders, evidence is accumulating that implicates a distinct syndrome, which has been described as C-PTSD (i.e., affect, interpersonal, and self-dysregulation; Cloitre, Garvert, Brewin, Bryant, & Maercker, 2013; Ford, 2015; Herman, 1993). C-PTSD involves a set of symptoms that include features of affect dysregulation, dissociation, somatic dysregulation, and altered beliefs regarding self, relationships, and the world that extend beyond the primarily anxiety-based symptoms in Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association [APA], 1994) PTSD (Ford, 2015; Herman, 1993; van der Kolk et al., 2005).
CT exposure is of particular relevance for forensic populations, based on evidence that it may also increase individuals’ risk of criminal involvement (Cuadra, Jaffe, Thomas, & DiLillo, 2014; Widom, 1989; Widom & Ames, 1994). Past exposure to CT, particularly childhood abuse is highly prevalent in adult forensic populations, compared with community samples (Carlson & Shafer, 2010; Girieballa et al., 2006; Roe-Sepowitz, Bedard, & Pate, 2007; Spitzer et al., 2006). Incarcerated adults also have heightened rates of behavioral health problems and symptoms consistent with C-PTSD (Fazel & Seewald, 2012; Girieballa et al., 2006; Spitzer et al., 2006; Widom & White, 1997). This population tends to experience many challenging issues, which may be especially difficult for women, given what we know about trauma. However, few studies have investigated whether the sequelae of CT exposure (including C-PTSD and related behavioral health problems) differ based on gender in incarcerated adults.
There is some evidence to suggest that incarcerated women have higher rates of trauma exposure and suffer from greater psychiatric morbidity than incarcerated men, including PTSD, and borderline personality, anxiety, depression, and substance use disorders (Gunter, Chibnall, Antoniak, McCormick, & Black, 2012; Kim, Johnson, Goswami, & Puisis, 2011; Komarovskaya, Loper, Warren, & Jackson, 2011; Lewis, 2006; McClellan, Farabee, & Crouch, 1997; Trestman et al., 2007). Prior research with community samples indicate that women have a tendency to be more adversely affected by traumatic events than men. Women exposed to interpersonal violence and other traumatic stressors are more likely to report severe (Breslau, 2002; Ditlevsen & Elklit, 2012; Ghafoori, Barragan, & Palinkas, 2013; Tolin & Foa, 2006) and chronic (Holbrook, Hoyt, Stein, & Sieber, 2002) posttraumatic stress problems than men. Research comparing the differential effects of childhood abuse also suggests that women may experience more adverse consequences compared with men (MacMillan et al., 2001; Thompson, Kingree, & Desai, 2004), which include a wide range of behavioral health problems consistent with C-PTSD such as depressive (Horwitz, Widom, McLaughlin, & White, 2001; MacMillan et al., 2001; McClellan et al., 1997), anxiety (Zlotnick et al., 2008), and substance use disorders (Danielson et al., 2009; Horwitz et al., 2001; MacMillan et al., 2001; McClellan et al., 1997; Simpson & Miller, 2002; Widom & White, 1997), as well as behaviors that may lead to criminal involvement (McClellan et al., 1997; Widom & White, 1997).
One plausible explanation for these findings is differences in the amount and type of violence or trauma experienced by women, particularly their heightened rate compared with men of exposure to CT involving sexual abuse or assault (Arnow, Blasey, Hunkeler, Lee, & Hayward, 2011; Gunter et al., 2012; Higgins & McCabe, 2003; Koenen & Widom, 2009; Scher, Forde, McQuaid, & Stein, 2004; Silverman, Reinherz, & Giaconia, 1996; Stuber, Resnick, & Galea, 2006; Tolin & Foa, 2006) and multiple forms of child maltreatment (Scher et al., 2004; Silverman et al., 1996), all of which can result in severe and complex problems. However, types of trauma exposure can only partially account for these gender differences, as some studies demonstrate an elevated rate of adverse consequences in women compared with men after controlling for types of traumatic events (Koenen & Widom, 2009; Tolin & Foa, 2006). Whether gender differences can be accounted for by increased rates of CT exposure and/or severity of C-PTSD symptoms is an important question that has not been investigated to our knowledge.
This area of research is essential because women are becoming involved in the criminal justice system at an alarming rate (Harrison & Beck, 2005), but most research with incarcerated adults has been conducted with men and cannot necessarily be generalized to women (Fazel & Seewald, 2012; Spitzer et al., 2006). This is of particular concern given that incarcerated women often have history of CT, psychological distress, and substance abuse (Browne et al., 1999; Gunter et al., 2012; McClellan et al., 1997; Mejia, Zea, Romero, & Saldivar, 2015; Salina, Lesondak, Razzano, & Weilbaecher, 2007; Trestman et al., 2007; Zlotnick, 1997). Incarcerated women tend to report experiencing many social and economic challenges including homelessness, poverty, education, employment, transportation, child care, medical care, lack of social support (Kim et al., 2011; Salina, Lesondak, Razzano, & Parenti, 2011; Salina et al., 2007), and abusive relationships (Browne et al., 1999). They are also at risk for a range of adverse health outcomes such as eating disorders, suicidality, sexually transmitted diseases, prostitution, and other high-risk behaviors and chronic health problems (Gunter et al., 2012; Kim et al., 2011; Lewis, 2006; Messina & Grella, 2006; Salina et al., 2007). Furthermore, women’s past exposure to CT and related problems may increase their vulnerability to the traumatic effects of incarceration (e.g., sexual abuse by staff or other inmates, separation from their children) and exacerbate feelings of shame and helplessness (Lewis, 2006; Moloney, van den Bergh, & Moller, 2009; Wolff, Shi, & Siegel, 2009). Few evidence-based treatments have been developed for incarcerated women who have histories of interpersonal violence and meet criteria for PTSD (Ford, Chang, Levine, & Zhang, 2013). Further refinements of these interventions including their adaptation to more complex problems (e.g., comorbidity, severe C-PTSD symptoms) require empirical guidance from research that clarifies the impact of CT-related problems for women. A better understanding of these underlying issues may also help identify pathways to criminality and inform preventive techniques, programming, and policies to reduce recidivism.
Therefore, the goals of the current study are (a) to determine whether gender differences exist in rates of past exposure to childhood abuse, severity of C-PTSD symptoms, and behavioral health problems among incarcerated adults; (b) to determine the extent of gender’s role in the relationship between past childhood abuse and C-PTSD symptoms, and between C-PTSD symptoms and behavioral health problems; and (c) to examine the contribution of a history of childhood abuse to the relationship between gender and C-PTSD, and to determine whether the relationship of gender to behavioral health problems can be indirectly accounted for by C-PTSD symptoms. The study’s hypotheses are as follows:
Method
Procedure and Sample
This study was approved by the Institutional Review Board (IRB) at the University of Connecticut Health Center, with data from 497 newly incarcerated adults. Participants were selected using a random number algorithm from all new admissions (n = 8,497) to Connecticut’s five moderate to high security prisons (see Scoboria et al., 2008; Trestman et al., 2007). Approximately 26% of individuals admitted into prison (n = 2,196) were selected during the recruitment process and screened for eligibility. Some inmates refused to participate in the study (7%) or were unable to participate due to rapid discharge or transfer to another facility (53%). Participants were excluded if they were non-English speaking, or required acute care for problems related to injuries, substance abuse detoxification, suicidality, or psychosis (17%). The final sample consisted of a diverse group of men (n = 301) and women (n = 196), who were equally represented across racial categories (43.1% White, 34.8% Black, 21.5% Hispanic). The mean age was 31.64 years (SD = 9.29 years), with women being slightly older than men (M = 30.62 vs. 32.30). Reasons for incarceration consisted mainly of nonviolent offenses such as drug possession or violation of probation (84.1%), rather than violent offenses (15.9%), which was consistent with the distribution of offenses in the overall prison population. However, men were more likely than women to be incarcerated for a violent offense (19% vs. 11%), but no differences were observed for drug-related offenses. Approximately, one in three women met criteria for a current affective (32%) or anxiety (36%) disorder other than PTSD, and 21.5% met criteria for PTSD (Trestman et al., 2007). Fewer men than women met criteria for a current affective (14%) or anxiety (28%) disorder (other than PTSD), or for PTSD (6%; Trestman et al., 2007). Women were more likely than men to meet criteria for borderline personality disorder (24% vs. 14%) and for a comorbid current Axis I psychiatric disorder and an Axis II personality disorder (41% vs. 24%; Trestman et al., 2007).
Measures
Trauma history
The Traumatic Events Inventory (TEI) is a 15-item clinician-administered interview assessing lifetime trauma exposure, adapted from the Stressful Life Events Screening Questionnaire (SLESQ; Goodman, Corcoran, Turner, Yuan, & Green, 1998), Traumatic Event Screening Instrument (TESI; National Center for PTSD Dartmouth Child Trauma Research Group, 1999), and victimization screening questions (Resnick, Kilpatrick, Dansky, Saunders, & Best, 1993). Preliminary evidence on psychometric properties of TEI and information on similar instruments suggests good reliability such as high interrater agreement (κ = .87-1.00; Goodman et al., 1998; Scoboria et al., 2008). In the current study, various trauma types were coded dichotomously (0 = no or 1 = yes) for childhood abuse, interpersonal trauma in adulthood (family or community violence), noninterpersonal trauma in childhood or adulthood (accidental, disaster, or illness), traumatic loss/separation from caregivers in childhood, and witnessing traumatic events in adulthood.
Psychiatric diagnoses
The Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders (4th ed. text rev.; DSM-IV-TR; APA, 2000) Axis I (SCID-I) and the Structured Clinical Interview for DSM-IV-TR Axis II (SCID-II; First, Spitzer, Gibbon, & Williams, 1996) were used to assess lifetime Axis I (other than PTSD) and II diagnoses. Previous research has demonstrated the SCID-I to be reliable with kappa values above .70 for interrater agreement. Similarly, research on the SCID-II suggests acceptable reliability and validity in assessing personality disorders, with kappa values above .60 and diagnostic predictive utility of 0.85 or greater for five personality disorders (First & Gibbon, 2004). A more recent study found kappa values for Axis I disorders ranging from 0.61 to 0.83 and 0.77 to 0.94 for Axis II disorders, indicative of fair to excellent interrater reliability (Lobbestael, Leurgans, & Arntz, 2011). The number of psychiatric diagnoses (Axes I & II disorders) was used in the current study as an index of psychiatric morbidity.
The Clinician-Administered PTSD Scale (CAPS; Blake et al., 1995) assessed lifetime PTSD based on DSM-IV-TR diagnostic criteria. The CAPS demonstrates excellent psychometric properties across a variety of adult populations (Weathers, Keane, & Davidson, 2001). Interrater reliability is high for continuous scores, which has been at 0.90 and above. Test–retest reliabilities range from .77 to .96 for the three symptom clusters and from .90 to .98 for the 17-item core symptom scale (Blake et al., 1995; Weathers et al., 2001). Internal consistency was found to be high with alphas ranging from .80 to .90 for a PTSD diagnosis and individual symptom clusters (Weathers et al., 2001). The CAPS was found to have convergent validity based on agreement with other measures of PTSD, such as the Impact of Events Scale (IES), PTSD Checklist (PCL; Weathers et al., 2001), and the Structured Clinical Interview for DSM-IV-TR PTSD Module (SCID-I; Foa & Tolin, 2000). Its diagnostic utility has sensitivities and specificities above .80 and kappas above .70 (Weathers et al., 2001).
C-PTSD symptom severity
A revised version of the Structured Interview for Disorders of Extreme Stress (SIDES; Pelcovitz et al., 1997) was used to assess lifetime C-PTSD symptom severity on a 4-point severity scale. Items on the SIDES-R were re-worded in order to clarify item anchors, but content, intent of items, and scoring procedures were maintained (Ford & Kidd, 1998). The overall C-PTSD symptom severity score consisted of 32 items pertaining to the following categories: (a) affect regulation and impulses, (b) attention and consciousness, (c) self-perception, (d) relationships with others, and (e) systems of meaning. This included questions about revictimization, self-harm, suicidality, guilt and shame, difficulty managing emotions, and feelings of hopelessness and despair about the future. Responses were rated from 0 to 3 within each category and totaled into the overall C-PTSD severity score. Higher numbers were assigned to items that were more reflective of severe symptomatology, indicative of C-PTSD (see Courtois, 2004). For example, one question tapping into “affect regulation” inquires about the frequency of difficulty calming oneself or getting upset over small problems (Pelcovitz et al., 1997). Preliminary evidence on the SIDES-R suggests reasonable concurrent, convergent, and discriminant validity (Scoboria et al., 2008). In previous studies, the SIDES-R has demonstrated acceptable interrater reliability (.74-.93; Ford & Kidd, 1998), and internal consistency with alphas ranging from .77 to .87 (total score) and .64 to .80 (subscales).
Substance use disorder risk
Six questions from the Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST; WHO ASSIST Working Group, 2002) were used to assess risk of problematic use of alcohol, heroin, cocaine, marijuana, and “other” drugs. The ASSIST includes items related to frequency of use, strong desire or preoccupation with use, problems related to use, attempts to cut down, and others expressing concern over use. Each response has a corresponding numeric value that was totaled to calculate an overall risk score for each substance (range = 0-39), which would then be classified into a “risk” category (low, moderate, or high). Low risk (i.e., alcohol, 0-10; other substances, 0-3) indicates no current substance use problems or a low risk of developing problems in the future. Moderate risk (i.e., 11-26 alcohol, 4-26 other substances) reflects a reasonable risk of health and other problems, in which individuals may currently be experiencing problems, and continuing this type of use will likely lead to future problems and dependence. High risk (i.e., 27 or higher on any substance) reflects the presence of substance use–related problems (e.g., health, social, financial, legal, and interpersonal) and substance dependence. The more frequently and recently endorsed responses (i.e., daily use, within past 3 months) are associated with a higher risk of problematic substance use, meaning use is indicative of more severe substance dependency and associated problems. For data analysis purposes within the current study, risk of problematic substance use was categorized as either low or moderate/high. In previous studies, the ASSIST has demonstrated excellent concurrent, construct, predictive, and discriminant validity. It has effectively screened for low, moderate, and high risk use for various substances (WHO ASSIST Working Group, 2002). Studies report its internal consistency to be above .80 for most domains and items. The ASSIST has shown evidence of convergent validity based on agreement with similar measures that assess for problematic substance use, such as the Addiction Severity Index (ASI; McLellan, Luborsky, O’Brien, & Woody, 1980) and the Alcohol Use Disorders Identification Test (AUDIT; Humeniuk & Ali, 2006). For analyses in which substance use problems were used as an outcome, an aggregate variable classifying each participant as either low or moderate/high risk of hard drug use (i.e., heroin and/or crack/cocaine) was utilized.
Analysis
A secondary data analysis was accomplished by using SPSS version 20 and Mplus Version 6.1 software programs. Chi-square tests and independent samples t tests (with equal variances not assumed if the Levene, 1960, test for equality of variance was significant) were used to test for between-group (gender) differences. Hierarchal regressions were conducted, whereby gender was entered at the first step followed by child abuse when C-PTSD was the dependent variable, or by C-PTSD when behavioral health variables (i.e., psychiatric morbidity or substance use disorder risk) were the dependent variables. Logistic regression was used in the latter case, with substance use (i.e., heroin or crack/cocaine) disorder risk scored as a dichotomous dependent variable (low risk = 0, moderate/high risk = 1). In each regression, a third step was conducted to test for moderation by adding a term representing the interaction of the two independent variables. Finally, in order to assess for mediation, Mplus 6.1 was used with the bias correcting bootstrap method. Parameter estimates were evaluated for all direct and indirect effects for gender and child abuse with C-PTSD, and gender, child abuse, and C-PTSD with behavioral health problems.
Results
Bivariate Analyses: Gender Differences
Child abuse was the most frequently endorsed trauma type, with almost half (49%) of the sample reporting some form of abuse (physical, sexual, or emotional) during childhood. Although women reported experiencing more types of traumatic events than men, t(495) = 7.72, p < .001, d = .71, 95% CI = [0.52, 0.89], child abuse was the only trauma type that women more often reported than men, χ2(1, N = 497) = 16.57, p < .001, Φ = .183, 95% CI = [0.09, 0.27]. Women also reported higher levels of C-PTSD symptomatology than men, t(444) = 2.15, p = .032, d = .20, 95% CI = [−0.02, −0.38] (Table 1).
Gender Differences in Trauma History and C-PTSD Symptoms.
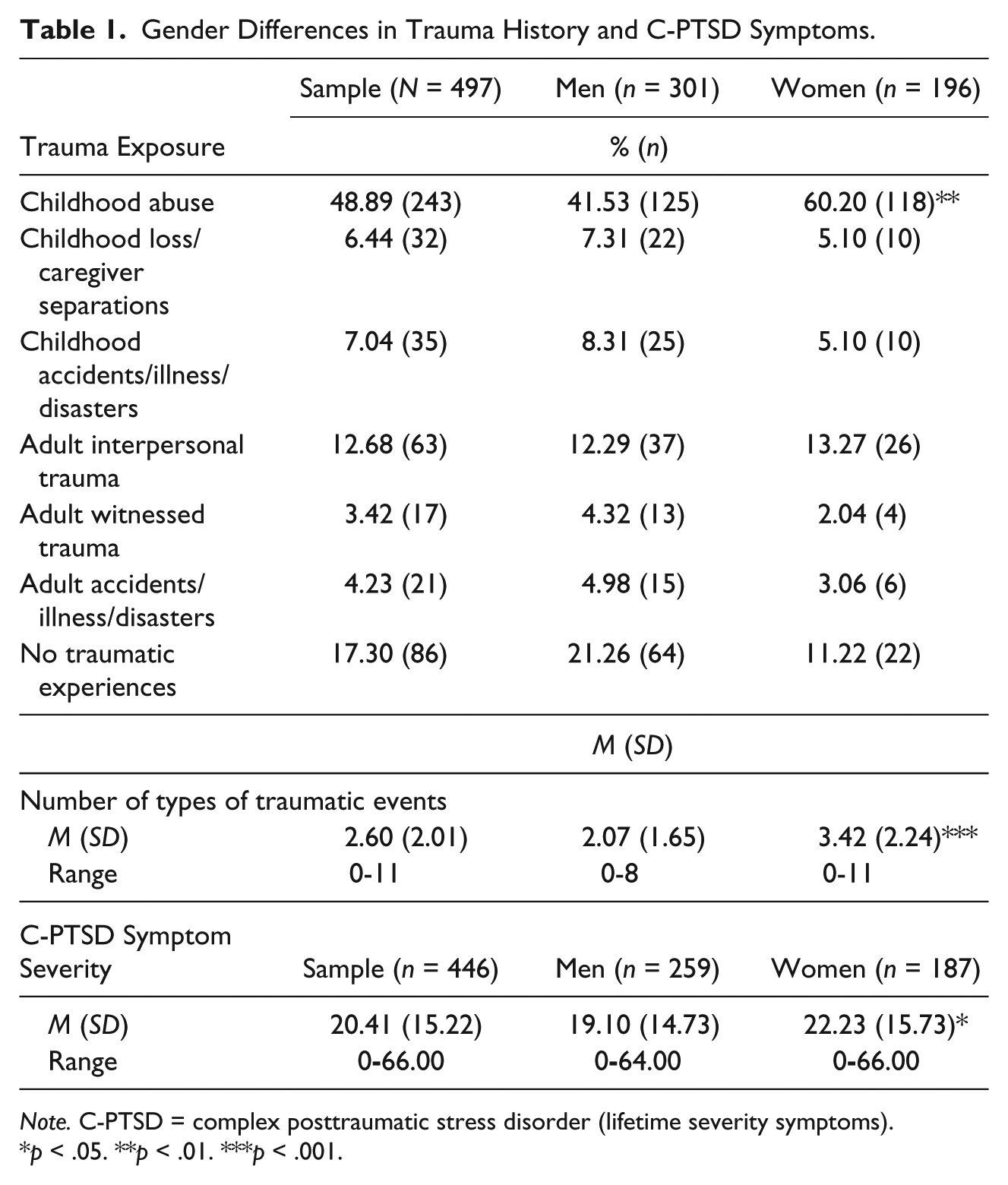
Note. C-PTSD = complex posttraumatic stress disorder (lifetime severity symptoms).
p < .05. **p < .01. ***p < .001.
Women met criteria for more total psychiatric diagnoses than men, t(380) = −4.194, p < .001, d = −.39, 95% CI = [−0.58, −0.21], with the difference in Axis I diagnoses being the major contributor to the overall difference, t(350) = −6.684, p < .001, d = −.64, 95% CI = [−0.82, −0.46] (Table 2). A chi-square test (with Yates Continuity Correction) indicated a significant relationship for gender and any diagnosis, χ2(1, N = 497) = 6.244, p = .012, Φ = −.116, 95% CI = [−0.03, −0.20], as well as for Axis I disorders, including depression, χ2(1, N = 497) = 43.32, p < .001, Φ = .300, 95% CI = [0.22, 0.38]; anxiety disorders, χ2(1, N = 497) = 23.46, p < .001, Φ = .222, 95% CI = [0.14, 0.30]; and PTSD, χ2(1, N = 484) = 21.53, p < .0051, Φ = .216, 95% CI = [0.13, 0.30]. This relationship was not observed for all Axis II disorders overall, but there were gender differences detected for antisocial personality disorder with men at greater risk, χ2(1, N = 497) = 7.78, p = .005, Φ = −.129, 95% CI = [−0.21, −0.04], whereas borderline personality disorder showed women to be at greater risk, χ2(1, N = 497) = 6.738, p = .009, Φ = .122, 95% CI = [0.03, 0.21].
Gender Differences in Psychiatric Diagnoses.
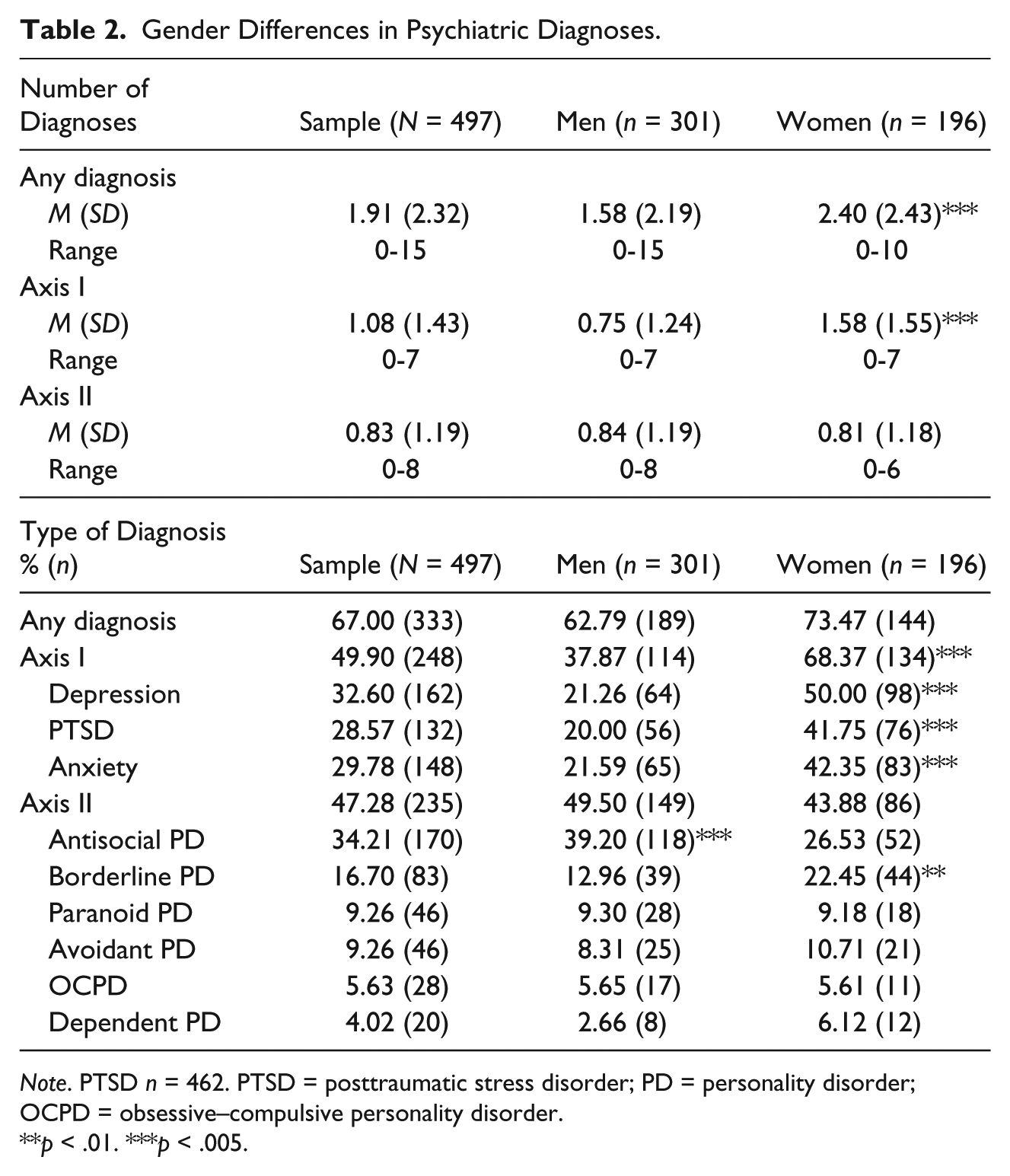
Note. PTSD n = 462. PTSD = posttraumatic stress disorder; PD = personality disorder; OCPD = obsessive–compulsive personality disorder.
p < .01. ***p < .005.
Substance use risk (low or moderate/high) for men and women within each type of substance (alcohol, marijuana, cocaine/crack, heroin, and other drugs) is displayed in Table 3. Chi-square analyses revealed that women were more likely than men to be moderate/high risk of cocaine/crack use, χ2(1, N = 293) = 5.44, p = .020, Φ = .144, 95% CI = [0.06, 0.23], and heroin use, χ2(1, N = 293) = 5.36, p = .021, Φ = .144, 95% CI = [0.06, 0.23]. In contrast, a higher percentage of men than women endorsed the moderate/high-risk category for marijuana χ2(1, N = 293) = 5.06, p = .025, Φ = −.139, 95% CI = [−0.22, −0.05].
Gender Differences in Risk of Problematic Substance Use.
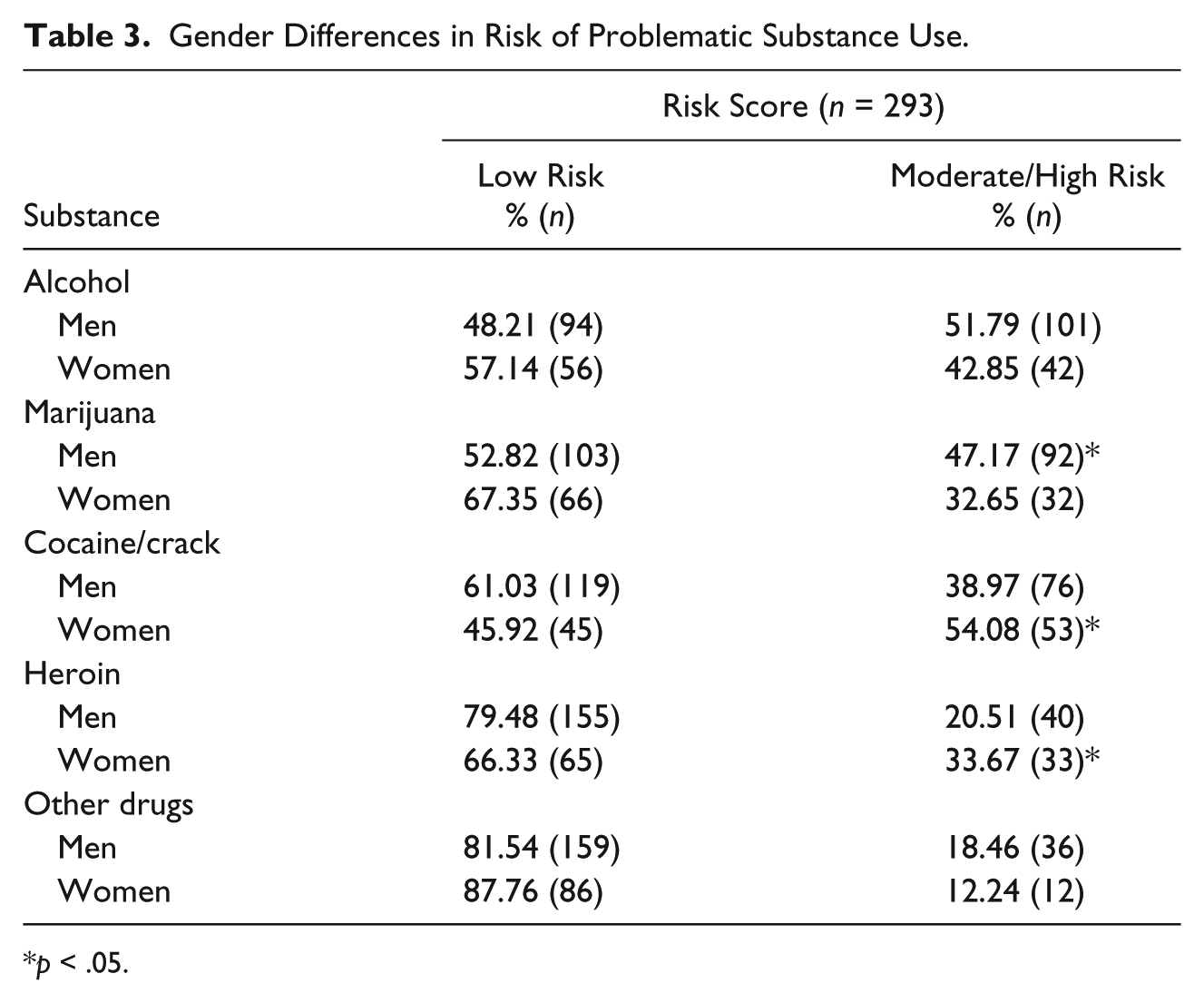
p < .05.
Regression Analyses: Multivariate Relationships of Gender, Child Abuse, C-PTSD, and Behavioral Health Problems
A hierarchical multiple regression using C-PTSD symptom severity as the dependent variable with child abuse and gender as the independent factors showed no significant effect for the interaction between gender and child abuse, suggesting that the influence of child abuse on C-PTSD symptoms was not moderated by gender (Table 4). Gender showed a significant effect as the first entry in the regression, R2 = .010, F(1, 444) = 4.627, p = .032, 95% CI = [0.000, 0.0366]. However, when child abuse was entered, gender was no longer significant, whereas the main effect for child abuse was significant and the model with gender and child abuse was significant, R2 = .105, F(2,443) = 25.12, p < .001, 95% CI = [0.0549, 0.1579]. Despite the significant overall main effect model and contribution of child abuse, substantial (>90%) variance in C-PTSD severity was not accounted for by child abuse or gender, or their interaction. Mediation analysis yielded an indirect effect that was significant, B = 1.76, p < .001, 99% CI = [0.789, 2.743], indicating that child abuse history fully mediated the association between gender and C-PTSD.
Multivariate Relationship of Gender, Childhood Abuse, and C-PTSD Symptoms.
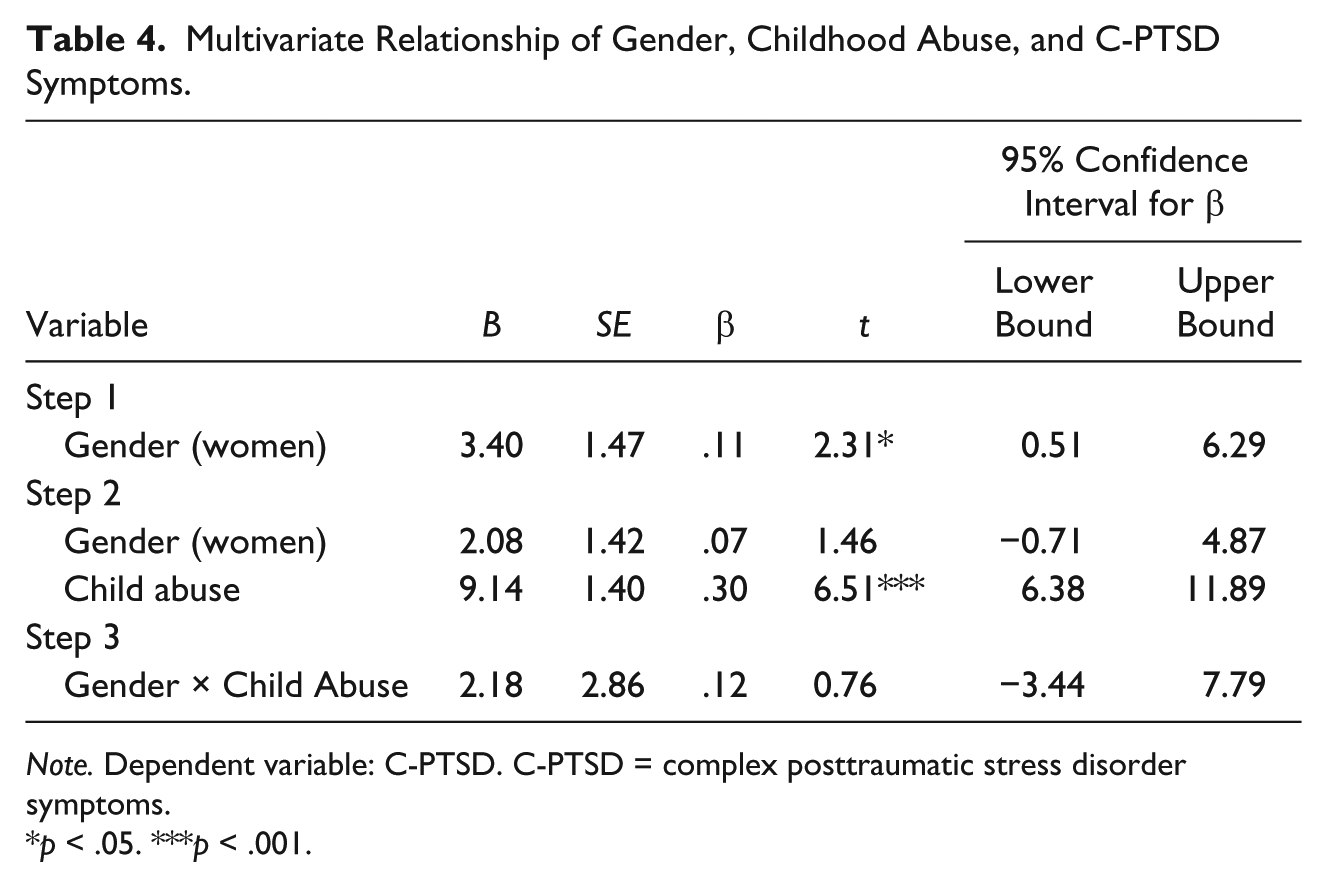
Note. Dependent variable: C-PTSD. C-PTSD = complex posttraumatic stress disorder symptoms.
p < .05. ***p < .001.
The second hierarchical multiple regression considered psychiatric morbidity (i.e., number of psychiatric disorders as dependent variable; see Table 5). The interaction of gender by C-PTSD was not significant, indicating that the association of C-PTSD symptom severity with the number of mental health disorders was not moderated by gender. Gender was significant in the first step, R2 = .021, F(1, 444) = 9.69, p = .002, 95% CI = [0.0029, 0.0547]. When C-PTSD was entered, the significance level of gender decreased, whereas the C-PTSD effect was highly significant, and the main effect model was also significant, R2 = .457, F(2, 443) = 186.239, p < .001, 95% CI = [0.392, 0.5113]. This model accounted for almost half (45.7%) of the variance in psychiatric morbidity. A mediation analysis yielded an indirect effect for gender that was significant, B = 0.387, p = .010, 95% CI = [0.086, 0.646]; however, the direct effect for gender remained significant at the .05 level, indicating that C-PTSD partially mediated the association between gender and psychiatric morbidity.
Multivariate Relationship of Gender, C-PTSD Symptoms, and Number of Psychiatric Diagnoses.

Note. Dependent variable: number of psychiatric diagnoses. C-PTSD = complex posttraumatic stress disorder symptoms.
p < .05. **p < .01. ***p < .001.
Finally, the relationship of gender, C-PTSD, and risk of problematic substance use was examined with multiple logistic regression (see Table 6). The interaction of gender and C-PTSD in Step 3 was nonsignificant, indicating that gender did not moderate the relationship between C-PTSD and substance use risk. Gender was significant at Step 1 but was no longer significant in Step 2 after C-PTSD symptom severity was included in the model. A mediation analysis of the relationship between gender and substance use risk yielded an indirect effect for gender that was marginally significant, B = 0.034, p < .09, 90% CI = [0.001, 0.067], suggesting partial mediation by C-PTSD of the association between gender and substance use risk.
Multivariate Relationship of Gender, C-PTSD Symptoms, and Drug (Cocaine/Crack or Heroin) Risk.
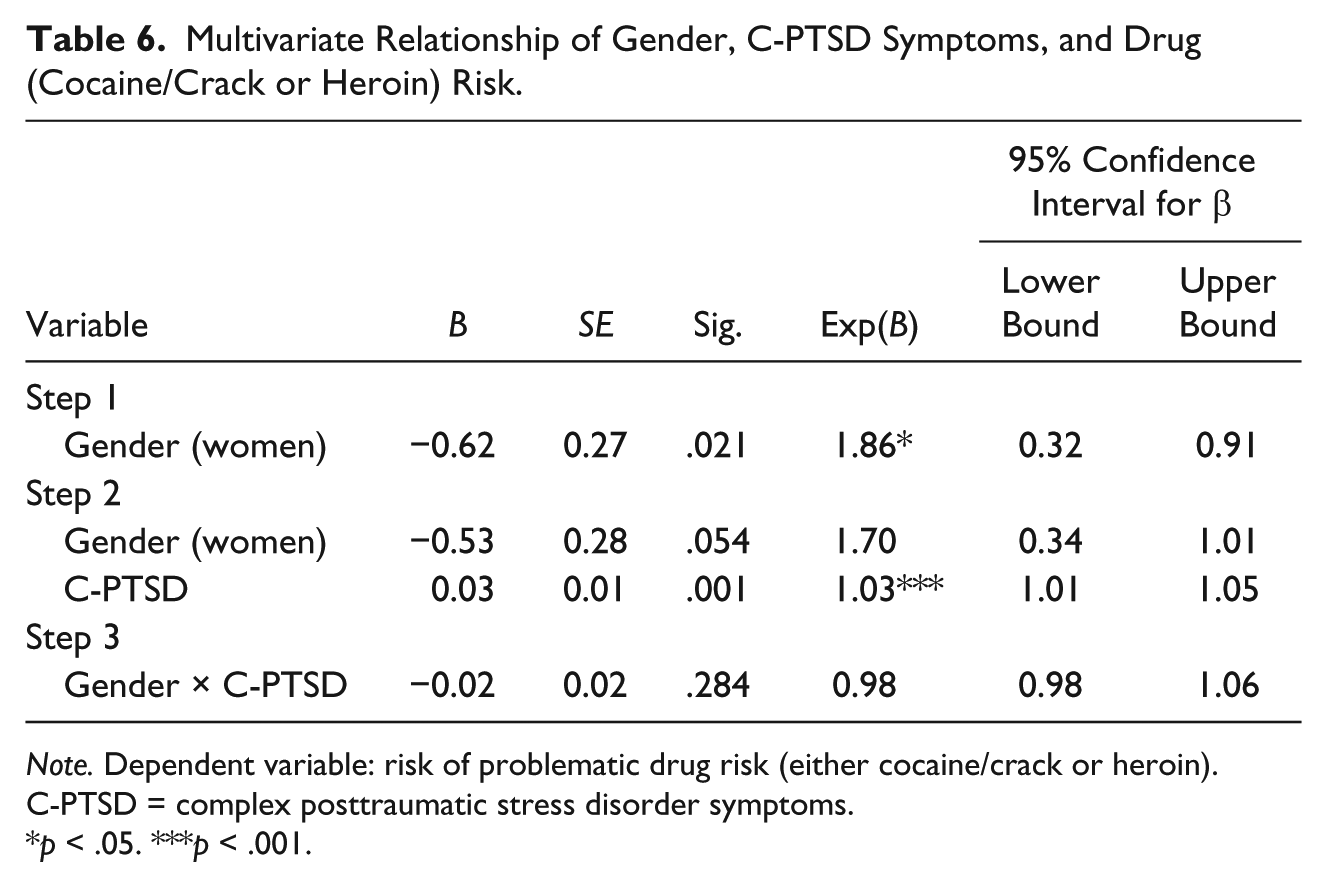
Note. Dependent variable: risk of problematic drug risk (either cocaine/crack or heroin). C-PTSD = complex posttraumatic stress disorder symptoms.
p < .05. ***p < .001.
Discussion
Consistent with prior research, both incarcerated men and women in the present study reported high rates of past exposure to childhood abuse (Carlson & Shafer, 2010; Girieballa et al., 2006; Roe-Sepowitz et al., 2007; Spitzer et al., 2006). Childhood abuse was associated with C-PTSD symptoms for both men and women, consistent with findings from prior clinical and community samples with nonincarcerated adults (Ford, 1999; van der Kolk et al., 2005). Also consistent with prior research with clinical and community samples (Higgins & McCabe, 2003; Koenen & Widom, 2009; Scher et al., 2004; Silverman et al., 1996; Tolin & Foa, 2006), incarcerated women were more likely to report a history of childhood abuse (although equally likely to report other types of childhood or past adulthood trauma exposure) compared with incarcerated men, and endorsed more severe C-PTSD symptoms. When the differential level of child abuse exposure was accounted for statistically, the gender difference in C-PTSD symptom severity became nonsignificant. Thus, differential CT exposure appears to play an important role in incarcerated women’s elevated levels of C-PTSD symptoms, as hypothesized.
C-PTSD symptoms were associated with increased risk of behavioral health problems in both incarcerated men and women. Here again, women endorsed more psychiatric problems, and greater risk of problematic substance use with hard drugs including heroin and cocaine, than men. C-PTSD accounted statistically for the gender difference in psychiatric morbidity, with evidence that the indirect effect of C-PTSD partially mediated the relationship of gender and psychiatric morbidity. Similarly, C-PTSD accounted partially for the gender difference in risk of hard drug use, although mediation was not confirmed. These findings suggest that apparent gender differences in behavioral health problems among incarcerated adults may be in part due to C-PTSD severity rather than gender per se. These findings held despite evidence that gender did not moderate the association between C-PTSD and behavioral health problems. Therefore, C-PTSD appears to be associated with behavioral health problems to a comparable degree for both incarcerated men and women, but incarcerated women’s higher levels of C-PTSD symptoms relative to men may contribute to the gender difference in severity of behavioral health problems.
Although childhood abuse, C-PTSD, and behavioral health problems were interrelated for both men and women, findings reveal greater past exposure of child abuse and more severe problems in women. These findings are consistent with prior research showing that women in prison are likely to experience difficulty with emotion regulation, behavioral self-control, interpersonal effectiveness, and feelings of shame and low self-esteem (Mullen, Martin, Anderson, Romans, & Herbison, 1996). The symptoms of C-PTSD also are associated with an increase in psychiatric morbidity and hard drug use, making women more susceptible to further victimization, socioeconomic disadvantage, and legal involvement (Moloney et al., 2009).
Study findings should be considered in the context of several methodological limitations. First, results cannot be generalized to clinical or community samples, or to populations of chronically incarcerated adults, because the sample was drawn from adults newly admitted to prison. Second, C-PTSD is a relatively new construct and more research needs to be conducted regarding its definition and measurement. Severity cut points for the SIDES-R have not been well established, making it difficult to draw conclusions about C-PTSD severity. Furthermore, use of a summary score for all SIDES-R symptoms may have obscured finer grain relationships between different aspects of C-PTSD (e.g., affect regulation, interpersonal relations, self-perceptions) and gender, child abuse history, or behavioral health problems. It is possible that we did not capture other indicators of CT-related problems with the SIDES-R. For example, in this sample, men were more likely than women to be incarcerated for a violent offense, which may be a reflection of affect dysregulation (e.g., aggression). There also existed high rates of personality disorders and PTSD in this sample. Therefore, it is unclear whether comorbidity of these disorders influenced or partially accounted for findings related to C-PTSD (see Ford & Courtois, 2014, for review). In addition, the DSM-IV-TR (APA, 2000) was used within this study to identify Axes I and II disorders, whereas the current version (Diagnostic and Statistical Manual of Mental Disorders, 5th ed. [DSM-5]; APA, 2013) now provides a definition of PTSD that includes several features of C-PTSD.
Due to high rates of endorsement of multiple types of past trauma exposure and overinclusive categories, it is unclear whether childhood abuse was the main contributor to C-PTSD severity, or whether this was attributable to a specific form of child abuse (e.g., sexual abuse) or an accumulation of multiple types of traumatic events including but not limited to child abuse (Cloitre et al., 2009). It is possible that sociological or contextual factors linked to gender may account for some of the observed differences in C-PTSD severity such as women’s role as a primary caregiver, or their elevated rate of sexual abuse and subsequent involvement in prostitution and sex trafficking (Kim et al., 2011). Women may also be more likely than men to internalize abusive experiences, which may lead to poorer outcomes (Simmons & Granvold, 2005). Finally, results could be attributable to gender-based reporting bias rather than differential rates, in which women may be more likely to report a history of childhood abuse and C-PTSD symptoms than men (Tolin & Foa, 2006).
Specific constructs within C-PTSD also need to be examined more closely in order to identify potential variations in ways in which C-PTSD might be manifested in both men and women. Given the heterogeneous nature of C-PTSD symptoms and biosocial aspects of gender, differences are likely to exist but may be difficult to detect at this level of analysis. Gender disparities have been commonly observed in the expression of depressive symptoms (Mirowsky & Ross, 1995), and rates of borderline (Ford & Courtois, 2014; Gunter et al., 2012) and antisocial (Zlotnick, 1999) personality disorders. This study revealed higher rates of anxiety, depression, borderline personality disorder, and PTSD for women, and antisocial personality disorder for men. However, further research is needed to clarify the role of C-PTSD in the development and maintenance of behavioral health problems for men and women, in light of findings indicating different patterns of risk and symptomatic presentation in psychiatric (Cavanaugh, Petras, & Martins, 2015; Gunter et al., 2012; MacMillan et al., 2001) and substance use (Horwitz et al., 2001; Lewis, 2006; McClellan et al., 1997) disorders. Identifying potential mediating factors linking childhood abuse to C-PTSD symptoms and adverse outcomes (e.g., psychiatric morbidity, hard drug use, and criminal behavior) with high-risk populations such as incarcerated adults is key, given the current study’s finding that C-PTSD symptoms and behavioral health problems cannot be fully explained by childhood abuse, gender, or their interaction. Finally, it is important to also consider ways in which C-PTSD symptoms might interfere with factors related to resiliency (e.g., social support, self-efficacy), and complicate behavioral health problems and their treatment and recovery.
Despite this study’s limitations, the findings indicate that incarcerated women’s particularly high rate of childhood abuse and severe C-PTSD symptoms compared with men warrants careful attention in research and services for incarcerated women’s behavioral health problems. Although childhood abuse and C-PTSD should be addressed in services for incarcerated men, the heightened severity of both childhood abuse and C-PTSD symptoms reported by incarcerated women places them at risk of particularly dangerous problems (i.e., multiple psychiatric disorders, severe drug use) that may be refractory to standard practice in behavioral health treatments. Women admitted into prisons should be assessed for CT and C-PTSD symptoms in standard behavioral health screening and follow-up assessments. Evidence-based psychosocial therapies for comorbid posttraumatic, psychiatric (Ford, Steinberg, & Zhang, 2011), and substance use (Frisman, Ford, Lin, Mallon, & Chang, 2008) disorders are needed on a systems-wide basis for incarcerated women, especially those with CT and C-PTSD symptoms who are at highest risk of subsequent criminal involvement (Ford et al., 2011; Moloney et al., 2009). Prevention and diversion programs that are informed by an understanding of childhood abuse/CT and C-PTSD also may contribute to earlier identification of women and girls who are at risk of criminal involvement and other high-risk behaviors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.