
Abstract
Research suggests that the relationship between alcohol use and intimate partner violence (IPV) is moderated by a range of other factors. Therefore, we investigated the relationship between alcohol use, hostile sexism, and religious self-regulation with perpetration. Using a national sample of 255 men, we found that hostile sexism was associated with physical violence toward a partner and alcohol use was positively associated with psychological abuse toward a partner. With regard to religious self-regulation, we found that introjected religious self-regulation was positively associated with hostile sexism and positively associated with perpetrating physical IPV. Identified religious self-regulation was negatively associated with physical violence perpetration. We also found significant interactions among our independent measures on physical IPV perpetration. These analyses suggest that increased alcohol consumption elevates the risk for physical violence perpetration among men who are high in introjected religious self-regulation and low in hostile sexism, while reducing the risk for perpetration in men who are high in identified religious self-regulation and low in hostile sexism. Implications and limitations of the findings are discussed.
Research on risk factors for men’s intimate partner violence (IPV) perpetration has shown a high correlation with substance use, particularly alcohol use (Bennett & Bland, 2008; Chermack, Fuller, & Blow, 2000; Coker, Smith, McKeown, & King, 2000; Gondolf, 1999). However, Bennett and Bland (2008) cautioned that the relationship between alcohol use and IPV is neither simple nor necessarily direct. As they point out, most heavy drinkers do not perpetrate IPV, which suggests that IPV perpetration is influenced by additional factors that may interact with alcohol use. One such factor may be sexism, given that research has shown that the correlation between substance abuse and IPV perpetration is strongest among men who endorse male dominance and who believe that IPV is appropriate behavior in specific circumstances (Field, Caetano, & Nelson, 2004). Interestingly, one factor that some researchers have found to have a protective effect on both alcohol use and IPV perpetration is religiosity—that is, the intensity of commitment to a religion or faith tradition. In a systematic review of 97 alcohol studies, Johnson (2011) reported that in the majority of studies, the findings showed that high religiosity is associated with a lower likelihood of alcohol abuse (for contrary results, see (Brinkerhoff, Grandin, & Lupri, 1992; Cunradi, Caetano, & Schafer, 2002). Some researchers maintain that religiosity per se, whether high or low, is less functionally important than how adherents to a religion are religious (Hackney & Sanders, 2003; Payne, Bergin, Bielma, & Jenkins, 1991). Renzetti, DeWall, Messer, and Pond (2017), for example, found that men’s religious self-regulation style (i.e., the internalized motivations underlying their reported behavioral expressions of religiosity) has a greater influence on their risk of IPV perpetration than does their level of religiosity.
These findings, taken together, indicate that risk and protective factors for IPV perpetration do not influence behavior in a singular or linear fashion, but rather interact with one another in complex ways that contribute to deleterious or beneficial outcomes. The purpose of the present study, then, is to examine in a community sample of American men how several factors—alcohol use, sexism, and religious self-regulation—may interact to increase or reduce the risk of IPV perpetration.
Alcohol Use and IPV Perpetration
As noted, one of the most commonly cited contributing factors to IPV is problematic alcohol use (Bennett & Bland, 2008; Eckhardt, Parrott, & Sprunger, 2015; Foran & O’Leary, 2008a; Johnson, 2001). Studies that examine the role of alcohol use in IPV typically show that men who are heavy or problem drinkers, especially men who binge drink, are at significantly greater risk of perpetrating IPV than men who are light or moderate drinkers or who abstain from alcohol (Coker et al., 2000; Field et al., 2004; Johnson, 2001; Kantor & Straus, 1987; O’Leary & Schumacher, 2003; Peralta, Tuttle, & Steele, 2010; Shorey, Stuart, & Cornelius, 2011). Moreover, IPV perpetrated by men who abuse alcohol tends to be more frequent and more severe than IPV perpetrated by men who are not problem drinkers (Graham, Bernards, Wilsnack, & Gmel, 2011; Murphy, Winters, O’Farrell, Fals-Stewart, & Murphy, 2005; Testa, Quigley, & Leonard, 2003). Johnson (2001), for example, reported that the men in her study who drank heavily or were intoxicated at the time of the IPV incident were more likely than nondrinkers to use very serious forms of violence against their intimate partners (e.g., choking, threatening with a weapon, sexual assault) and were more likely to inflict physical injuries, including injuries that required medical attention.
Despite this evidence, researchers emphasize that demonstrating an association between alcohol use and IPV perpetration does not establish a causal link (Bennett & Bland, 2008). Kantor and Straus (1987), for example, analyzed data from a national probability sample of more than 6,000 households and found that alcohol was not involved in a majority (76%) of the IPV incidents. Gelles (1993) noted that some men begin drinking following an IPV incident, and others cite alcohol as an excuse or justification for their abusive behavior. Furthermore, as Bennett and Bland (2008) pointed out, the popular notion that abusive men are very drunk or out of control when they perpetrate IPV is simply inaccurate. Among the theories that have been developed to explain the mechanisms by which alcohol facilitates or increases the risk of IPV perpetration, some suggest that alcohol use may contribute to IPV perpetration more for some men than for others. The potential influence of such individual differences is taken into account by the multiple threshold model (Fals-Stewart, Leonard, & Birchler, 2005). The multiple threshold model posits that alcohol will have differential psychopharmacological or cognitive effects on likelihood of IPV perpetration for men with personality characteristics or relational tendencies (e.g., trait anger, state anger, irrational beliefs, hostile attributions, depression, low self-esteem, low perceived self-efficacy) that have been found to be associated with risk for IPV perpetration (Edleson & Tolman, 1992; Foran & O’Leary, 2008a; Holtzworth-Munroe & Meehan, 2004).
As Foran and O’Leary (2008a) explained, men with few or no IPV risk factors will evidence a low, if any, association between alcohol use and IPV perpetration because the psychopharmacological effects of the alcohol are not strong enough to increase their risk above the threshold at which they would aggress. Men with a moderate number of IPV risk factors, however, may experience a decrease in inhibition from drinking alcohol such that they exceed their threshold for perpetrating nonsevere IPV when drinking. And those men who are at greatest risk for IPV perpetration may engage in nonsevere IPV even when not drinking, so their risk for nonsevere IPV does not increase significantly when they drink, although their risk for severe IPV may increase with alcohol consumption. Experimental and cross-sectional research has provided some support for this model (e.g., Foran & O’Leary, 2008b; Parrott & Giancola, 2004), but Shorey, Brasfield, Zucosky, Febres, and Stuart (2015) called for further research that examines the moderating effects of a broader range of individual-level factors on the alcohol–IPV relationship. One such factor that studies indicate should receive additional research attention is adherence to sexist beliefs and attitudes.
Hostile Sexism and IPV Perpetration
Sexism is commonly defined as prejudice and discrimination, typically against women, on the basis of sex. Ambivalent sexism theory (Glick & Fiske, 2001), however, posits that this popular definition of sexism is incomplete because it captures only one dimension of a more complex construct. According to ambivalent sexism theory, there are at least two different types of sexism: hostile sexism and benevolent sexism. Hostile sexism refers to “antipathy toward women who are viewed as usurping men’s power,” whereas benevolent sexism is defined as “a subjectively favorable, chivalrous ideology that offers protection and affection to women who embrace conventional roles” (Glick & Fiske, 2001, p. 109). Researchers have long debated the effect of adherence to types of sexism on men’s likelihood of perpetrating IPV against women (Allen, Swan, & Raghavan, 2009; Lonsway & Fitzgerald, 1995). Although Glick, Sakalli-Ugurlu, Ferreira, and de Souza (2002) have argued that benevolent sexism and hostile sexism are “complementary tools of control,” whereby men’s protection of and affection toward women are contingent on women’s adherence to traditional gender norms, researchers have obtained inconsistent findings with regard to the relationship between benevolent sexism and IPV perpetration (Allen et al., 2009; Forbes & Adams-Curtis, 2001; Forbes, Jobe, White, Bloesch, & Adams-Curtis, 2005). Studies of hostile sexism, in contrast, have yielded relatively consistent findings with regard to its positive relationship to IPV. Men who hold hostile attitudes toward women have been found to be at greater risk for IPV perpetration (Anderson & Anderson, 2008; Glick et al., 2002; Holtzworth-Munroe, Meehan, Herron, Rehman, & Stuart, 2000). Anderson and Anderson (2008) reported, in fact, that men who are highly hostile toward women specifically target women for aggression. Nevertheless, it has been argued that in many societies today, blatantly hostile sexism is generally frowned upon (Swim, Aikin, Hall, & Hunter, 1995), which may have an inhibiting effect on the open expression of such attitudes and their manifestation in abusive behavior toward women, at least in specific situations or settings.
The multiple threshold model leads us to expect that alcohol use might interact with hostile sexism to affect risk of IPV perpetration. Indeed, Renzetti, Lynch, and DeWall (2018) found that heavy alcohol use was associated with increased physical IPV perpetration among men with high, low, and average scores on the Hostile Sexism subscale, but the greatest effects were for men who scored low in hostile sexism. When these men were heavy drinkers, their physical IPV perpetration reached levels comparable with men high in hostile sexism. Alcohol use, then, appears to interact with hostile sexism to increase risk of IPV perpetration.
The Role of Religiosity and Religious Self-Regulation
As noted earlier, religiosity has been found to have a protective effect for alcohol abuse and for IPV perpetration (Ellison & Anderson, 2001; Ellison, Trinitapoli, Anderson, & Johnson, 2007; Johnson, 2011). Ellison and Anderson (2001) reported, for instance, that among both men and women, those who attended religious services more often and more consistently—their measures of religiosity—were less likely to perpetrate IPV. The protective effect of religiosity held even after controlling for its effects on increasing social integration and social support, and decreasing substance abuse and various psychological problems. Moreover, religiosity’s protective effect remained significant regardless of whether the data on IPV were collected from self-reports of perpetrators or from partner reports of victimization. This is an especially noteworthy finding given research documenting the tendency for IPV perpetrators to underestimate the frequency and severity of their abuse (Dobash, Dobash, Cavanagh, & Lewis, 1998; Hamberger & Guse, 2002; Kimmel, 2002) and to overestimate the normativity of IPV perpetration (Neighbors et al., 2010).
Other studies, however, show less robust and consistent effects of religiosity on IPV perpetration, particularly when alcohol use is taken into account. For example, DeWall (2010), in a study of a large, nationally representative sample of married adults, measured alcohol consumption and used frequency of participation in religious services and participants’ self-assessed importance of religious beliefs in their daily lives as indicators of religiosity. His findings showed that heavy alcohol use was associated with greater IPV perpetration, but only among participants low in religiosity; high religiosity served as a protective factor against IPV perpetration while also appearing to break the commonly observed link between alcohol use and IPV. In contrast, Cunradi et al. (2002), who measured religiosity in terms of church attendance, found that while religiosity was associated with reduced IPV perpetration, it was less significant than alcohol consumption in predicting men’s likelihood of perpetrating IPV (see also Brinkerhoff et al., 1992).
Regardless of the specific findings, all these studies are limited by their rather narrow measures of religiosity. Religiosity is a complex and multifaceted construct that encompasses far more than attendance at religious services, religious affiliation, or self-proclaimed importance of religious beliefs (Dollahite, Marks, & Goodman, 2004). Moreover, social scientists have pointed out that the influence of religiosity on specific behavioral outcomes depends to some degree on the extent to which one’s religion is integrated into his or her everyday life (Pargament, 2002). In other words, to understand the potential impact of religiosity on behavior, researchers must consider not only such measures as religious affiliation, self-reported beliefs, or frequency of church attendance or prayer but also how individuals may use religion to actually regulate their behavior. This, social psychologists maintain, requires internalization of religious values (Blais, Sabourin, Boucher, & Vallerand, 1990). When religious values are internalized, the individual “takes them on” as his or her own and incorporates them into daily living; they then motivate the individual’s behavior. But internalization occurs in different ways and in differing degrees.
Drawing on self-determination theory (SDT), Ryan and Deci (2000) identified ways that external motivational factors, such as religion, may regulate an individual’s behavior. These ways of behavior motivation can be conceptualized along a continuum of internalization that manifests as behavioral self-regulation (see also Neyrinck, Vansteenkiste, Lens, Duriez, & Hutsebaut, 2006). At one end of the continuum are behaviors that are performed because others pressure or coerce the individual into performing them. For example, an individual may go to religious services every week because his or her spouse insists on it or because they feel guilty if not. In such cases, the religious motivation for the behavior really has not been internalized, but rather is overtly externally regulated. This type of behavioral self-regulation is referred to as introjected self-regulation (Neyrinck et al., 2006; Ryan & Deci, 2000). In contrast, when individuals perform a behavior, such as praying, because they see it as an important or valued activity to which they are personally committed, their motivation is more fully internalized and their action is more autonomous or freely chosen. This type of behavioral regulation is referred to as identified self-regulation (Neyrinck et al., 2006; Ryan & Deci, 2000).
Most relevant for the present study is research that examines the emotional and behavioral outcomes for each of these types of religious self-regulation. More specifically, those high in introjected regulation—what Neyrinck and colleagues (2006) aptly labeled non-self-determined motivation or “because I should” motivation (p. 325)—have higher rates of depression, lower self-esteem, lower perceived self-efficacy, and tend to use less adaptive coping strategies. In contrast, those high in identified regulation—that is, self-determined motivation or “for the pleasure of doing it” motivation (Neyrinck et al., 2006, p. 325)—are more likely to express greater life satisfaction, higher self-esteem, a greater sense of self-efficacy, and tend to use more positive and adaptive coping strategies (Neyrinck, Lens, & Vansteenkiste, 2005; Ryan, Rigby, & King, 1993). Importantly, research with men who have perpetrated IPV has found high rates of depression, low self-esteem and low perceived self-efficacy, and the tendency to use negative coping strategies (Edleson & Tolman 1992; Holtzworth-Munroe & Meehan 2004). Consequently, research examining the potential effects of religiosity on men’s likelihood of perpetrating IPV should include, in addition to standard measures of religiosity (e.g., frequency of church attendance, self-proclaimed importance of religion), measures of how men are religious in terms of their style of religious self-regulation. Indeed, Renzetti, DeWall, et al. (2017) found in their study using a national, community sample of men that men high in introjected religious self-regulation were more likely to perpetrate IPV, regardless of their reported level of religiosity; that is, introjected religious self-regulation had a strong, independent effect on the men’s IPV perpetration. However, Renzetti, DeWall, et al. (2017) did not examine the relationship between alcohol use and religious self-regulation. Nor did they consider how hostile sexism might interact with both alcohol use and religious self-regulation style to affect IPV perpetration, an interaction that is worthy of study.
The Present Study
The overall goals of the present study were to both build on and synthesize prior work in the IPV perpetration literature by investigating the interactive effects of alcohol use, hostile sexism, and religious self-regulation on male-perpetrated IPV. We used a national, community sample of men who were currently involved in a romantic relationship. Based on our review of the extant literature, we developed several hypotheses. First, because previous studies have produced contradictory findings with regard to the relationship between benevolent sexism and IPV perpetration, we focused on the relationship between hostile sexism and IPV perpetration, which has been fairly consistent and strong in the extant literature:
With regard to the alcohol–IPV relationship, we hypothesized that,
Based on the findings of Renzetti, DeWall, et al. (2017), we also expected that,
Although we did not find research in our literature review demonstrating a relationship between religious self-regulation style and hostile sexism, we did take note of research showing that religious beliefs may actually facilitate certain types of offending for some people (Topalli, Brezina, & Bernhardt, 2012) and that members of specific religious subgroups (e.g., fundamentalists) express greater approval of family violence, including acts of IPV, under certain circumstances (Koch & Ramirez, 2010). Consequently, we hypothesize that,
Based on the multiple threshold model, we expected participants’ alcohol use, hostile sexism, and religious self-regulation to have an interactive effect on participants’ IPV perpetration. Furthermore, Renzetti, Lynch, and DeWall (2018) found an Alcohol Use × Hostile Sexism interaction such that high levels of alcohol consumption had a greater impact on physical IPV perpetration for men low in hostile sexism than for men high in hostile sexism. Our predictions in Hypothesis 5 (H5) were largely based on the findings of this interaction. We also considered the possibility that religious self-regulation type could further moderate this two-way interaction given that religiosity may facilitate violence in some people (Topalli et al., 2012). Therefore, we predicted that,
Method
Participants
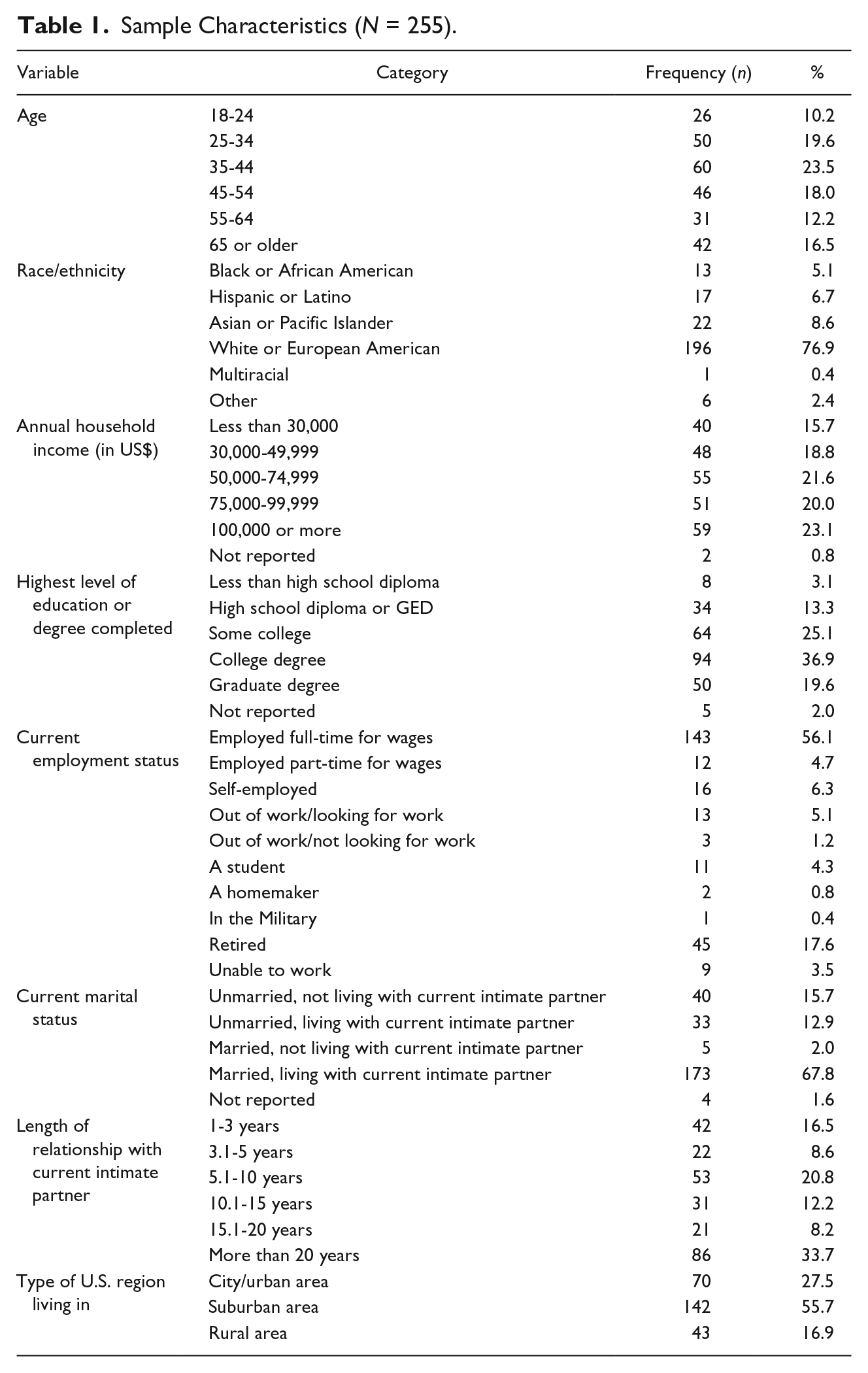
Our national, community sample consisted of 255 men who were recruited through the online sampling and survey administration service, SurveyMonkey. SurveyMonkey advertised the study to members of their respondent pool who met the following eligibility criteria: male, aged 18 or older, living in the United States, in a committed heterosexual intimate relationship with the same partner for at least 1 year, fluent in English, and without disabilities that would prevent them from completing an online survey. SurveyMonkey incentivized participants by making contributions to charities and by entering participants into sweepstakes drawings for each survey completed. The majority of participants were White or European American (76.9%), under the age of 45 (53.3%), had an annual income more than US$50,000 (64.6%), married and living with their spouse (67.8%), employed full-time (56.1%), and completed either some college (25.1%) or held a college degree (36.9%). A complete summary of our sample characteristics can be seen in Table 1.
Sample Characteristics (N = 255).
Procedure
Individuals interested in completing the survey followed the study link provided by SurveyMonkey. The link directed them to an online Informed Consent document that they were asked to read before deciding to complete the survey instrument. Following the study introduction, potential participants were asked to provide their informed consent if they wanted to participate. If a potential participant decided not to complete the study, he was automatically redirected to the SurveyMonkey homepage. If a potential participant consented to participate, he was directed to the online survey. All study procedures were approved by the Institutional Review Board of the authors’ academic institution.
Measures
Hostile sexism
Participants’ hostile sexism was measured using the Hostile Sexism subscale of the Ambivalent Sexism Scale (Glick & Fiske, 1996). The Hostile Sexism subscale asks participants to indicate their level of agreement with each of the 11 items using a 6-point Likert-type response scale (0 = disagree strongly; 1 = disagree somewhat; 2 = disagree slightly; 3 = agree slightly; 4 = agree somewhat; 5 = agree strongly). The items on the Hostile Sexism scale assess hostility toward women and support for dominance of men (e.g., “Once a woman gets a man to commit to her, she usually tries to put him on a tight leash.”). We found good reliability for the 11 hostile sexism items in our sample (α = .81).
Alcohol use
Alcohol use during the past 12 months was calculated by summing participants’ responses to three items from the Collaborative Studies on Genetics and Alcoholism (COGA) Study of the National Institute on Alcohol Abuse and Alcoholism (NIAAA). First, participants indicated how often they drank alcohol in the past 12 months (0 = never/not at all; 1 = 1 to 3 times; 2 = about 1 time per month; 3 = about 2 to 3 times per month; 4 = about 1 time per week; 5 = about 2 to 6 times per week; 6 = about 1 time per day; 7 = about 2 to 3 times per day; and 8 = about 4 times per day). Second, participants reported how many drinks they usually consumed each time they consumed alcohol in the past 12 months (0 = none/ I did not drink any alcohol in the past 12 months; 1 = one; 2 = two to three; and 4 = four or more). Third, participants indicated how many times they were drunk or high from alcohol in the last 12 months (0 = never/not at all; 1 = 1 to 3 times; 2 = about 1 time per month; 3 = about 2 to 3 times per month; 4 = about 1 time per week; 5 = about 2 to 3 times per week; 6 = about 4 or more times per week).
Religious self-regulation
Participants’ religious self-regulation was measured using the Religious Self-Regulation Questionnaire (RSQ; Ryan et al., 1993), which is composed of 12 items. Using a 7-point Likert-type scale (1 = not at all true, 7 = very true), six items measure introjected religious self-regulation (e.g., “One reason I think it’s important to actively share my faith with others is because I would feel bad about myself if I didn’t”) and six items measure identified religious self-regulation (e.g., “When I turn to God, I most often do it because I enjoy spending time with Him”). Although they are theoretically distinct, introjected and identified religious self-regulation were correlated in the present study (r = .68, p < .001).
IPV perpetration
The primary dependent variable, IPV perpetration, was measured using the Severity of Violence Against Women Scale (Marshall, 1992). For each item, participants provided the frequency of times they perpetrated the given behavior toward their partner in the past 12 months (0 = never; 1 = once; 2 = a few times; and 3 = many times). Our two primary dependent measures consisted of (a) psychological abuse perpetration and (b) physical violence perpetration. Participants’ responses to the 19 psychological abuse items were summed as were the responses to the 21 physical violence items to create separate psychological abuse and physical violence perpetration dependent measures.
Results
Descriptive Statistics
Hostile sexism, alcohol use, and religious self-regulation
The average score on the Hostile Sexism subscale was 2.58 (SD = .61; range = 0.92-4.38). The average alcohol consumption score was 6.0 (SD = 3.79; range = 1.00-18.00). The average introjected self-regulation score was 3.00 (SD = 1.60; range = 1.00-7.00) and the average identified self-regulation score was 4.12 (SD = 1.94; range = 1.00-7.00).
IPV perpetration
Physical violence perpetration scores ranged from 0 to 60, with a mean score of 1.89 (SD = 6.84); 19.6% of the men reported having perpetrated at least one physically violent behavior in the past 12 months. Psychological abuse perpetration was more common; scores on this measure ranged from 0 to 42, with a mean score of 3.42 (SD = 6.25) and 47.5% of men reported having perpetrated at least one psychologically abusive behavior in the past 12 months. Only 33 participants (13% of the total sample) reported perpetrating both physical violence and psychological abuse in the past 12 months.
Hypothesis Testing
To test our hypotheses, we ran a negative binomial regression for each of the (a) perpetration of psychological abuse, and (b) perpetration of physical abuse, in which we entered the Hostile Sexism subscale mean scores; alcohol use scores; the introjected religious self-regulation scale mean scores; the identified religious self-regulation scale mean scores; the two-way interaction terms involving hostile sexism, alcohol use, and the two religious self-regulation scales; and the three-way interaction terms, all while controlling for household income and race. We centered all predictor variables in both regression models and controlled for participant race, age, household income, education level, employment, and length of time in a relationship with their partner. The results of the regressions are shown in Table 2 and correlations among all measures in the models can be viewed online in the supplementary table. Overall, the models for both physical violence, χ2(17) = 319.742, p < .001, and psychological abuse, χ2(17) = 88.091, p < .001, perpetration were significant.
Negative Binomial Regression Results for Psychological and Physical IPV Perpetration Models (N = 255).

Note. Model results control for participant race, age, household income, education, employment, and length of time in their intimate relationship; all predictor variables were centered. CI = confidence interval.
p < .05. **p < .01, ***p < .001.
H1: Hostile Sexism and IPV
As predicted (H1a), higher hostile sexism scores were positively associated with perpetrating physically violent acts against a partner (B = 1.14, p < .001). Contrary to our hypothesis (H1b), we did not find support for our hypothesis that hostile sexism is associated with increased perpetration of psychological abuse (B = .16, p = .260).
H2: Alcohol Use and IPV
Contrary to our hypothesis (H2a), the main effect of alcohol use on the perpetration of physical violence was not significant (B = .00, p = .914). However, increased alcohol use was associated with increased perpetration of psychological abuse (B = .09, p < .001), which supports our hypothesis (H2b).
H3: Religious Self-Regulation and IPV
Supporting our hypothesis (H3a), introjected religious self-regulation was positively associated with perpetrating physical violence against a partner (B = 1.07, p < .001), but not psychological abuse (H3b; B = 0.12, p = .104). Identified religious self-regulation was negatively associated with physical violence perpetration (B = −0.85, p < .001), supporting our hypothesis (H3c). Contrary to our prediction (H3d), identified religious self-regulation was not significantly associated with psychological abuse perpetration (B = −0.02, p = .769), though the relationship between these two variables was in the predicted direction.
H4: Religious Self-Regulation and Hostile Sexism
Consistent with our hypothesis (H4a), introjected religious self-regulation was significantly, positively associated with hostile sexism (B = 0.08, p = .009, 95% confidence interval [.021, .147]). Though the relationship was in the predicted (negative) direction (H4b), identified religious self-regulation was not significantly associated with hostile sexism (B = −0.02, p = .500, 95% confidence interval [−.069, .034]).
H5: Interactions
Physical violence
To reduce redundancies and to describe the associations among the variables as accurately as possible, only the three-way (i.e., higher order) interactions will be probed. First, the three-way interaction of Hostile Sexism × Alcohol Use × Introjected Religious Self-Regulation was significant (B = −0.26, p < .001). As seen in Figure 1, the greatest increase in risk for perpetrating physical IPV was for participants who were high in introjected religious self-regulation and low in hostile sexism, while consuming higher levels of alcohol, t(240) = 6.12, p < .001. Though introjected religious self-regulation also significantly increased the likelihood of physical violence perpetration for participants who were high in hostile sexism and were heavy drinkers, t(240) = 4.99, p < .001, this increase was smaller than that seen in low hostile sexism heavy drinkers. With regard to those with lower alcohol consumption, a combination of high hostile sexism and high introjected self-regulation increased participants’ likelihood of perpetrating physical violence when they consumed less alcohol, t(240) = 3.34, p = .001. However, participants who were low in hostile sexism and consumed less alcohol did not significantly differ in their perpetration as a function of introjected religious self-regulation, t(240) = 1.68, p = .094.

Three-way interaction between hostile sexism, alcohol consumption, and introjected religious self-regulation.
Second, the three-way interaction of Hostile Sexism × Alcohol Use × Identified Religious Self-Regulation was also significant (B = 0.26, p < .001). As seen in Figure 2, consuming more alcohol significantly decreased highly identified participants’ risk for perpetrating physical violence when they were both high, t(240) = −4.71, p < .001, and low, t(240) = −5.80, p < .001, in hostile sexism—though this decline in risk was much stronger for those who were less hostilely sexist. Participants who were highly sexist and consumed less alcohol also showed a small, but significant decline in risk to perpetrate IPV when they were highly identified, t(240) = −2.73, p = .001. However, in participants who consumed less alcohol, there was no effect of identified religious self-regulation on perpetration for those who were less hostilely sexist, t(240) = −0.50, p = .620.
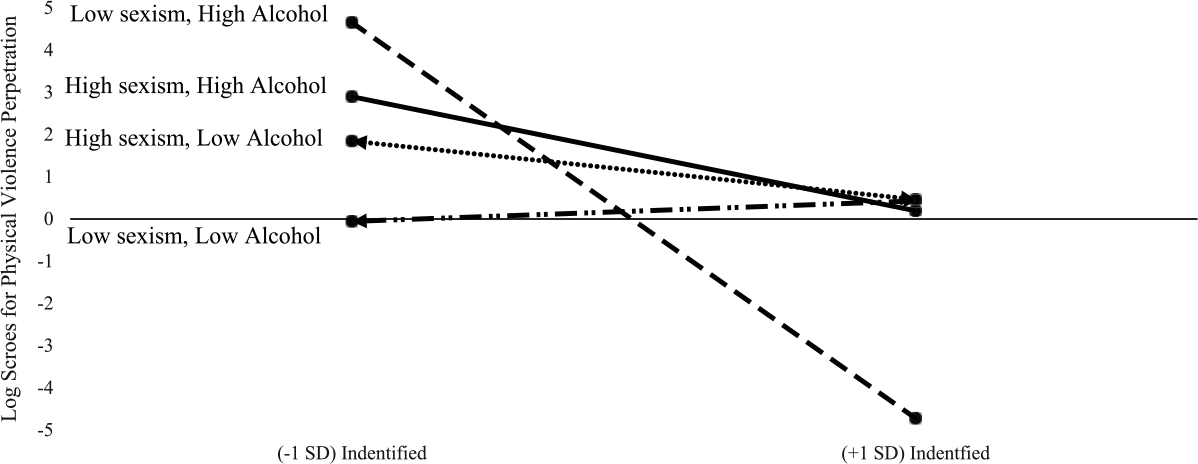
Three-way interaction between hostile sexism, alcohol consumption, and identified religious self-regulation.
Psychological abuse
As seen in Table 2, there were no significant interactions among the predictor variables for the model predicting psychological abuse perpetration.
Discussion
The results of our first two hypotheses partially mirror Renzetti, Lynch, and DeWall’s (2018) findings and support previous research investigating both sexist beliefs (e.g., Anderson & Anderson, 2008; Glick et al., 2002; Holtzworth-Munroe et al., 2000) and alcohol use (e.g., Foran & O’Leary, 2008a, 2008b; Johnson, 2001; Shorey et al., 2011) as IPV risk factors. Furthermore, our results for H3 are consistent with Renzetti, DeWall, et al.’s (2017) findings, wherein introjected religious self-regulation acts as a risk factor for IPV perpetration, while identified religious self-regulation acts as a protective factor for IPV perpetration. However, it is important to acknowledge that we found only partial support for all our hypotheses. To this end, some factors were associated with physical violence only, while others were associated only with the perpetration of psychological abuse. For example, we found that higher hostile sexism scores and introjected religious self-regulation were both significantly associated with the perpetration of physical violence but not psychological abuse perpetration. Relatedly, alcohol use was significantly associated with psychological abuse but not physical violence IPV perpetration. Given that Renzetti, Lynch, and DeWall (2018) found significant, positive associations between alcohol use and hostile sexism scores with both physical and psychological IPV perpetration, we expected to mirror such findings. However, Renzetti, Lynch, and DeWall (2018) did not include participants’ religious self-regulation scores in their investigation of the alcohol, sexism, and IPV perpetration link, and in the current study, participant religious self-regulation both accounted for a significant amount of variance in explaining IPV perpetration and interacted with alcohol and hostile sexism.
Arguably the most interesting findings in the present study that provide the greatest contribution to the literature consist of the 2 three-way interactions we found between alcohol use, sexism, and religious self-regulation. We predicted in H5 that we would find that participant religious self-regulation would further moderate the two-way interaction between alcohol use and hostile sexism that Renzetti, Lynch, and DeWall (2018) found. Indeed, we found that the interaction between alcohol use and hostile sexism was moderated by both introjected and identified religious self-regulation. This supports the notion that religious self-regulation style can both facilitate and impede IPV perpetration depending on the combination of participants’ drinking and sexist beliefs. Among high introjected religious self-regulation and low sexism participants, a higher level of alcohol consumption significantly elevates the risk to perpetrate physical violence in comparison with a lower level of alcohol consumption. This effect could perhaps be explained by the fact that less sexist participants had more room for an increase in IPV perpetration given their lower baseline rate of IPV perpetration in comparison with participants who were higher in hostile sexism. Among high identified religious self-regulation and low hostile sexism, consuming higher amounts of alcohol significantly reduces the risk of perpetrating physical violence against a partner compared with drinking less alcohol.
Thus, our results lend support to the multiple threshold model of the alcohol–IPV relationship, which suggests that alcohol will have differential effects on likelihood of IPV perpetration for men with characteristics or relational tendencies, such as beliefs or traits, that have been found to be associated with risk for IPV perpetration (Fals-Stewart et al., 2005). For example, alcohol may act as a disinhibitor to facilitate sexist views (Swim et al., 1995) or distortions in the behavior of a partner (Foran & O’Leary, 2008), which are then amplified in participants who are introjected self-regulators. On the contrary, the protective effect of identified religious self-regulation is strongest in combinations where alcohol consumption and sexism are not both high (i.e., higher alcohol consumption/low sexism and lower alcohol consumption/higher sexism). Thus, it would appear that identified religious self-regulation can act as a protective agent against IPV perpetration, but only to a certain point in participants who are also high in other risk factors for IPV (i.e., alcohol use and hostile sexism).
We should note that there were also no interactions among the independent variables for the perpetration of psychological abuse model. This may have been due to the fact that psychological abuse is unfortunately quite common in intimate relationships. For example, nearly 50% of the men in our study reported having perpetrated at least one psychologically abusive behavior in the previous 12 months, which was much higher than the percentage of men who reported perpetrating physical violence against their partners. Thus, there may have been limited variation across the comparison cells among the combination of independent variables when detecting moderation to explain variance in psychological IPV perpetration. Despite the general commonality of psychological abuse in relationships, we should note that the men in our sample engaged in relatively low levels of IPV and only about 13% of participants perpetrated both physical violence and psychological abuse toward their partners. Furthermore, very few participants reported perpetrating severe physical violence against an intimate partner, such as threatening to kill a partner, or sexual violence against a partner. This is likely due to the fact that our sample did not specifically target IPV perpetrators for participation, but rather was a general community sample. As highlighted by the work of Johnson (2006), different sample types (e.g., community survey vs. court/shelter) tap into different types of IPV (e.g., situational couple violence vs. intimate terrorism), which differ in severity, levels of violence and control, and gender patterns. It is noteworthy that although our sample was not a clinical one involving severe battering, we were still able to observe the increased risk for perpetration that alcohol may facilitate under certain dispositional characteristics.
Finally, our results revealed a significant positive relationship between introjected self-regulation and hostile sexism (H4). Though the relationship between identified self-regulation and hostile sexism was not significant, the direction of this relationship was in the predicted (negative) direction. These findings lend support to the notion that individuals with specific religious orientations tend to express greater approval of family violence (Koch & Ramirez, 2010). Furthermore, Topalli et al. (2012) emphasized that while religiosity may inhibit offending for many individuals, it may facilitate offending for certain subgroups. That introjected religious self-regulation had an additive effect on physical IPV perpetration in hostilely sexist participants—even when they were low in alcohol use—stresses the importance of better understanding the circumstances under which men who hold such beliefs may be at a higher risk to perpetrate IPV.
Limitations
The findings of the present study must be considered in light of several limitations. First, we were only able to analyze cross-sectional data. Consequently, we can identify associations among the variables of interest, but we cannot make any determination of temporality and, therefore, likely causation. Given that we did not measure the context of participants’ alcohol use, alcohol use problems, or reasons for using alcohol, we cannot make causal statements about how alcohol consumption affects men with varying levels of sexist attitudes and religious orientations. Future research, particularly using a longitudinal design, should include an examination of situational contexts, the development of problem drinking, and motivations for alcohol use, as well as how these variables change over time in relation to religious self-regulation and sexist attitudes. Relatedly, it would be valuable for future studies to replicate the findings of the present study using larger sample sizes and other sample types (e.g., clinical samples). Although our results lend support to the multiple threshold model of alcohol’s impact on IPV perpetration, our hypotheses were only partially supported and we observed no effects on psychological abuse. Therefore, the present study offers initial evidence of the moderated relationship between alcohol consumption, hostile sexism, and religious self-regulation in the context of IPV, but not definitive evidence of the complex associations among these variables.
Second, although we recruited a national, community-based sample, it was not a random probability sample. Researchers who use the SurveyMonkey sampling pool can specify eligibility criteria, but participants nevertheless self-select into the study. Therefore, it may be that only men with certain characteristics (e.g., those at low risk for IPV perpetration) chose to participate. However, our sampling strategy resulted in a relatively diverse sample with regard to the demographic characteristics we measured. In addition, evaluation of Internet sampling and data collection methods indicates that although these techniques have limitations, they also reduce some of the biases found in other types of samples, such as college student samples (Buhrmester, Kwang, & Gosling, 2011; Gosling, Vazire, Srivastava, & John, 2004). Rates of disclosure to sensitive items, such as questions about IPV perpetration and alcohol use, were similar to or higher than those reported by other types of samples (Heeren et al., 2008; Hines, Douglas, & Mahmood, 2010). Relatedly, our sample aimed to represent the general U.S. male population and was not a clinical sample, nor a subsample of IPV perpetrators. As a result, we cannot generalize our findings to men who perpetrate sexual or severe physical IPV. We should note that studies indicate that the risk factors for and the dynamics of sexual and severe IPV are different from and more complex than those investigated in the present study (Smith, Thornton, DeVellis, Earp, & Coker, 2002; Wegner, Pierce, & Abbey, 2014; White & Smith, 2009). Therefore, it would be valuable to examine in future work how alcohol use, sexism, and religious self-regulation may affect different types of IPV perpetration (e.g., sexual violence, severe violence).
Third, the present study only provides self-reports of IPV perpetration. This is of particular relevance in the present study given that research shows that men tend to underestimate and underreport IPV perpetration (Dobash et al., 1998; Hamberger & Guse, 2002; Kimmel, 2002). Consequently, researchers often warn that their findings are likely underestimates of IPV perpetration rates. It is also possible that this potential social desirability response bias may have reduced the likelihood for our participants to report sexual and severe IPV, although in the present study, the self-reported rates of psychological and physical abuse were comparable with those reported in other studies (Black et al., 2011; Schafer, Caetano, & Clark, 1998; Tjaden & Thoennes, 2000).
Fourth, our sample consisted only of men in heterosexual relationships, which limits the generalizability of our results to female-perpetrated IPV. Although some observers maintain that women are as likely as men to assault their intimate partners (see, for example, Archer, 2000; Dutton, 2006; Dutton, Corvo, & Hamel, 2009; Straus, 2007), there is a sizable body of research demonstrating that men’s IPV against women has different underlying motives (see Barnett, Lee, & Thelan, 1997; Dobash et al., 1998; Miller, 2001; Rajan & McCloskey, 2007) and has more serious consequences for victims, including injuries and even death (Archer, 2000; Fox & Zawitz, 2007; Hamberger & Guse, 2002; Menard, Anderson, & Godboldt, 2009; Tjaden & Thoennes, 2000). Therefore, it would be worthwhile to test the interactive effects that we found in the present study in a sample of nationally representative women to investigate the role of gender symmetry.
Future Directions and Conclusion
Our goal was to examine how two known risk factors—alcohol use and sexism—interact with religious self-regulation, which we thought, based on the literature, could act both as a risk and protective factor depending on the self-regulation type, for IPV perpetration. We did, indeed, find evidence to support our prediction that these three factors interact with one another in ways that both increase and decrease the likelihood of male-perpetrated physical IPV. The results of the present study shed light on the complex interplay between risk and protective factors for IPV perpetration and may hopefully contribute to a better understanding of effective violence intervention and prevention. For example, given that it is common for violence prevention and intervention programs to address sexism through social network and peer support models (e.g., Coker, 2014; Potter & Banyard, 2011), it may be worthwhile to also consider how positive peer support in the form of identified religious regulation may buffer against sexist attitudes held against women. Furthermore, it is possible that individuals who are higher in identified religious self-regulation may be less inclined to engage in problem drinking behavior (and vice versa for introjected regulators). More work is needed to better understand the characteristics and behaviors of those who are high and low in introjected/identified religious self-regulation, and how this is related to IPV perpetration.
It is also important for us to emphasize that there is a need for future research to further explore interactions among risk and protective factors to better understand the complex interplay of trait and situational characteristics in the context of IPV perpetration. Factors such as alcohol expectancies, emotion regulation, and relationship satisfaction, for example, may also play a moderating role in the link between alcohol use and IPV perpetration (Hammond & Overall, 2013; Shorey et al., 2015). Furthermore, given that introjected religious self-regulators and IPV perpetrators typically test high for negative traits and emotions (e.g., depression and low self-esteem; Edleson & Tolman, 1992; Holtzworth-Munroe & Meehan 2004), researchers may consider controlling for such measures in the future as a means to better understand how IPV intervention and prevention efforts can effectively target IPV perpetrators.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.