
Abstract
Intimate partner violence (IPV) against pregnant women is common with severe health consequences to women and their babies. The aim of the present study is to measure the association between IPV and signs of depression among pregnant women attending antenatal care in a semi-urban setting in northern Tanzania. A cross-sectional study was conducted from March 1, 2014, to May 30, 2015, among pregnant women attending routine antenatal care in Moshi Municipality, Tanzania. During their third trimester, self-reported exposure to IPV was assessed using a validated structured questionnaire adopted from the World Health Organization’s (WHO) Multi-Country Study on Women’s Health and Domestic Violence. Signs of depression were assessed using Edinburg Postpartum Depression Scale. A total of 1,116 pregnant women were included in the analysis. A total number of 433 (38.8%) reported to be exposed to at least one type of violence during their pregnancy, and 128 (11.5%) presented with signs of depression. The most common type of violence experienced was emotional violence (30.7%), followed by sexual violence (19.0%) and physical violence (10.0%). Exposure to at least one type of violence was the strongest predictor for depression (adjusted odds ratio [AOR] = 5.06; 95% confidence interval [CI] = [3.25, 7.86]), followed by women who reported their primary source of emotional support was individuals not related to their family as compared with support obtained from their male partner/husband (AOR = 2.25; 95% CI = [1.26, 4.02]). Positive HIV/AIDS status (AOR = 2.27; 95% CI = [1.01, 5.14]) and previous history of depression (AOR = 1.62; 95% CI = [1.00, 2.64]). After adjusting for other predictors and types of violence, physical violence was the strongest predictor for signs of depression (AOR = 4.42; 95% CI = [2.65, 7.37]). Signs of depression were commonly observed among pregnant women and strongly associated with exposure to any type of IPV. The present findings indicate an urgent need for screening depression and IPV to mitigate the adverse health outcomes related to both IPV and depression during pregnancy.
Introduction
Violence against women is a pandemic affecting all countries worldwide (García-Moreno & Heise, 2005). In the majority of cases, the violence is perpetrated by an intimate partner and is commonly defined as intimate partner violence (IPV). Globally, the reported prevalence of IPV is in the range of 15% to 71%, with high prevalence observed in, for example, Ethiopia (71%), Peru (69%), Bangladesh (62%), and Tanzania (56%), while the lowest prevalence reported in Japan (15%; García-Moreno & Heise, 2005). IPV is categorized into physical, emotional, and sexual violence and has been associated with a wide range of adverse health outcomes related to physical, mental, and reproductive health (Campbell, 2002).
Exposure to partner violence during a pregnancy increases the risk of a wide range of adverse health outcomes, including physical and psychological effects for both the mother and fetus (Lafaurie-Villamil, 2015; Mahenge, Likindikoki, Stöckl, & Mbwambo, 2013; Weobong et al., 2014). IPV can lead to unhealthy life styles (e.g., alcohol intake, smoking, poor nutrition which may result in inadequate weight gain), inconsistent prenatal care (Kaye, Mirembe, Bantebya, Johansson, & Ekstrom, 2006), and adverse neonatal outcomes like low birth weight, preterm birth, and small for gestational age (Grote et al., 2010).
The results of a systematic review on prevalence of IPV during pregnancy in sub-Saharan Africa indicated the prevalence of IPV to range from 2% to 57% with the prevalence of specific types violence ranging from 23% to 40% for physical violence, 25% to 41% for emotional violence, and 3% to 26% for sexual violence (Shamu, Abrahams, Temmerman, Musekiwa, & Zarowsky, 2011). In recent years, research has increasingly focused on depression during pregnancy in low-income countries of Sub-Saharan Africa with reported prevalence in eight African countries in the range of 4% to 17% and the main predictors for depression were reported to be lack of social support and marital conflicts (Sawyer, Ayers, & Smith, 2010).
Studies from developed countries also reported the occurrence of depression among pregnant women experiencing violence (Finnbogadóttir, Dykes, & Wann-Hansson, 2014; Flach et al., 2011; Grote et al., 2010). If depression is not managed during pregnancy, it can lead to postpartum depression (Ludermir, Lewis, Valongueiro, de Araújo, & Araya, 2010). Although the link between IPV during pregnancy and risk of depression during pregnancy has been documented, little is known regarding the association between specific types of violence and the occurrence of depression during pregnancy. A detailed assessment of the magnitude of IPV during pregnancy and the respective association with depression is crucial for informed decision making regarding appropriate interventions aiming at mitigating the IPV-related adverse effects on maternal and neonatal health.
The hypothesis of this study states that there is an association between IPV and depression to pregnant women. The purpose of the present study was to assess the association between specific types of IPV and depression during pregnancy among women attending antenatal care (ANC) in a semi-urban area in northern Tanzania.
Material and Method
The study was conducted from March 1, 2014, to May 30, 2015, among pregnant women attending two antenatal clinics located in a semi-urban area of Moshi Municipality, Kilimanjaro region, northern Tanzania. Moshi Municipality is situated in Kilimanjaro Region in the lower slope of Mount Kilimanjaro with an estimated population of 184,292 people with an annual population growth of 2.8%. The main ethnic groups are Chagga and Pare. The Municipal Council covers about 59 sq. km. Administratively, it is divided into 21 wards, and according to the 2012 census, the municipal has a total of 23 governmental health care facilities which offer antenatal services to pregnant women. The women were recruited from two antenatal care clinics, Majengo Clinic and Pasua Clinic, both having high attendance rates (approximately 4,000 women annually) which justify the selection of these two clinics for the present study. In Kilimanjaro Region, antenatal care coverage is 100%.
Study Design
The present study was nested in a cohort study, which was a study component in the research project “The Impact of Violence on Reproductive Health in Tanzania.” The overall aim of the research project was to assess the association between IPV and adverse pregnancy outcomes in semi-urban areas of Tanzania. In the present study, a cross-sectional study design was applied to assess the association between IPV and signs of depression during pregnancy.
Participants and Data Collection Procedure
As part of the routine ANC services, all pregnant women who attend ANC services in the two mentioned clinics were offered assessment of their gestational age and examination for HIV. All women aged 18 years and above with gestation age below 24 weeks, verified by ultrasound scanning, were invited to participate in the study. Women with multiple pregnancies and severe obvious signs of depression or other types of mental disease were excluded. On the day of enrollment, the first interview was performed at the ANC clinic where data on age, place of birth, place of upbringing, religion, and occupation and education level were recorded. In the same interview, data on previous history of past illnesses including depression, hypertension, and reproductive health characteristics were collected. At gestation age of 34 weeks, the women were invited for a second interview, which took place in a setting chosen by the participant (i.e., in the home of the woman or in a similar place where the participant felt comfortable to talk freely). During the second interview, we obtained information on signs of depression during present pregnancy, self-perceived HIV status (which was compared with the HIV status at the antenatal card without disclosure of the card information), and husband’s sex preference of the unborn child. The women were also asked whether they had been exposed to emotional, physical, and sexual violence exerted by their intimate partner during the present pregnancy. All the interviews (first and second interviews) were conducted by experienced nurses who were specifically trained in conducting interviews covering sensitive topics.
Questionnaire and Interviews
IPV experiences were assessed using a modified Swahili version of the WHO Multi-Country Study on Women Health and Domestic Violence Against Women (García-Moreno & Heise, 2005) tool previously used in Tanzania. The measurement of physical violence was addressed in six questions where the woman was asked whether the partner had slapped, pushed, hit, kicked, chocked, or threatened to use or actually used things like gun, knife, or other weapon that could hurt her. Measurement of emotional violence was based on four questions and focused on whether the woman had been insulted, humiliated, and intimidated or whether the partner had threatened to hurt her or someone she cares about. Measurement of sexual violence was based on questions on whether the partner had used physical force to have sexual intercourse, having sexual intercourse without consent, or being forced to engage in humiliating or degrading sexual acts.
Depression is defined by the World Health Organization (WHO) as a state of mental disorder, characterized by feeling of sadness, feelings of guilt and of being unimportant, loss of interest or pleasure, disturbed sleep pattern, loss of appetite, feelings of tiredness, and poor concentration which may lead to suicidal thoughts (WHO, 2012). To capture these signs of depression, Edinburg Postpartum Depression Scale (EPDS) was used for measurement of signs of depression during pregnancy. EPDS is a widely used self-reported questionnaire for assessment of postpartum depression but has also been applied for measurement of antenatal depression (Fisher et al., 2013; Matijasevich et al., 2014). EPDS is based on a 10-item questionnaire; each item is scored on a 4-point scale (0-3), with total sum of score of all items ranging from 0 to 30. The questions address the mood of the women in the past 7 days prior to the interview in relation to guilt, anxiety, sleep disturbance, and suicidal ideation. A high EPDS score indicates increased risk of depression. In the present study, a cutoff point of ≥13 was used to define signs of depression. The EPDS cutoff point used in the present study has previously been applied in Tanzania to assess depressive symptoms among pregnant women (Rwakarema, Premji, Nyanza, Riziki, & Palacios-Derflingher, 2015). All the EPDS questions were read by the interviewer.
Measurement of emotional support was based on questions where the woman was asked to point out the most important person with whom she felt that she could rely on to share her thoughts and feelings (Sigalla et al., 2017). The answer options were categorized into husband/partner, parents, in-laws, and nonrelated persons. Previous history of depression was assessed by asking the participants directly if they had previously been diagnosed with depression at any given time prior to the enrolment in the present study.
Other variables included sociodemographic (age, occupation, educational level, religion, place of birth/upbringing, number of pregnancies) and health-related characteristics (history of depression and hypertension, HIV status, and fathers’ preference regarding sex of the unborn children).
Statistical Analysis
All data were double-entered in Epi Data (Version 3.1), and discrepancies were identified and subsequently corrected according to the original data forms. All statistical analyses were performed using the STATA software package (version 12). Groups were compared using chi-square tests. Bivariate analyses were used to calculate the crude strength of statistical associations between exposure to IPV and signs of depression during pregnancy. A backward regression model, which included all statically significant variables from the bivariate analyses, was used to adjust for possible confounding. Predictor variables with a p value of ≥.1 were excluded at each step in the regression and all those with a value of <.05 were retained in the final model. The strength of all associations was presented as odds ratios (ORs) with a 95% confidence interval (CI). Assessment of effect modification in the data was performed by separate stratified analyses. In case of effect modification stratum, specific ORs were reported.
Ethical Statement
The WHO guidelines for ethical and safety for researching sensitive issues regarding intimate relationships and violence (WHO, 2001) were followed. At the end of the interview, women received information and contact details about available social support within Moshi Municipal regardless of whether they reported violence or not. The study was approved by the Kilimanjaro Christian Medical University College Research Ethical Committee (Approval no. 664).
Results
A total of 1,116 pregnant women were included in the study. The sociodemographic characteristics of the women who were included in the study are presented in Table 1. Almost half (47.9%) of the women were aged 25 to 34 years, whereas a smaller proportion was 35 years or above (13.1%). The majority of the women had a paid job (61.7%), and had completed primary education or higher (63.8%). More than half of the women were Christians (56.4%), and more than one third (38.5%) were primigravida.
Descriptive Sociodemographic Characteristics of Study Participants (N = 1,116).

Higher education means any education after secondary school education.
The overall prevalence of signs of depression among pregnant women attending ANCs in Moshi Municipality was 11.5%. A total of 433 women (38.8%) reported that they had been exposed to at least one type of violence during their pregnancy. The distribution of reported signs of depression in the various groups and the results of the analysis of the association between self-reported exposure to at least one type of violence and the signs of depression are shown in Table 2. We accept the hypothesis which states that there is an association between IPV and depression to pregnant women. The results of the multivariate analyses indicate that exposure to at least one type of violence exerted by the intimate partner was the strongest statistically significant predictor for signs of depression during pregnancy (adjusted odds ratio [AOR] = 5.06; 95% CI = [3.25, 7.86]). Hence, the odds of signs of depression during pregnancy was 5 times higher among women exposed to at least one type of violence as compared with women who did not report any partner violence. Other significant predictors for depression were women who reported that their primary source of emotional support was individuals not related to their family as compared with support obtained from their male partner/husband (AOR = 2.25; 95% CI = [1.26, 4.02]). Emotional support from biological relatives or in-law’s family was not associated with depression during pregnancy. Other significant predictors were HIV/AIDS diagnosis (AOR = 2.27; 95% CI = [1.01, 5.14]) and previous history of depression (AOR = 1.62; 95% CI = [1.00, 2.64]). The associations between the three specific types of violence and signs of depression during pregnancy are shown in Table 3. The most common type of violence experienced during pregnancy was emotional violence (30.7%), followed by sexual violence (19.0%) and then by physical violence (10.0%). After adjusting for the previously observed statistically significant predictors and other types of violence, physical violence was the strongest significant predictor for signs of depression (AOR = 4.42; 95% CI = [2.65, 7.37]), followed by sexual (AOR = 2.53; 95% CI = [1.60, 4.00]) and emotional violence (AOR = 2.16; 95% CI = [1.35, 3.44]).
Results of Bivariate and Multivariate Analyses (N = 1,116).

Note. The associations between sociodemographic characteristics, history of depression and hypertension, HIV status, fathers’ preference regarding sex of unborn children, emotional support, exposure to at least one type of violence, and signs of depression during pregnancy. OR = odds ratio; CI = confidence interval; AOR = adjusted odds ratio.
ORs have been adjusted for age, educational level, religion, reported history of depression, HIV/AIDS status, emotional support, and exposure to at least one type of violence.
Higher education means any education after secondary school education.
Primary source of emotional support means the most important person on whom the woman can rely on.
The Associations Between Specific Types of Violence and Signs of Depression During Pregnancy: Results of Bivariate and Multivariate Analyses (N = 1,116).
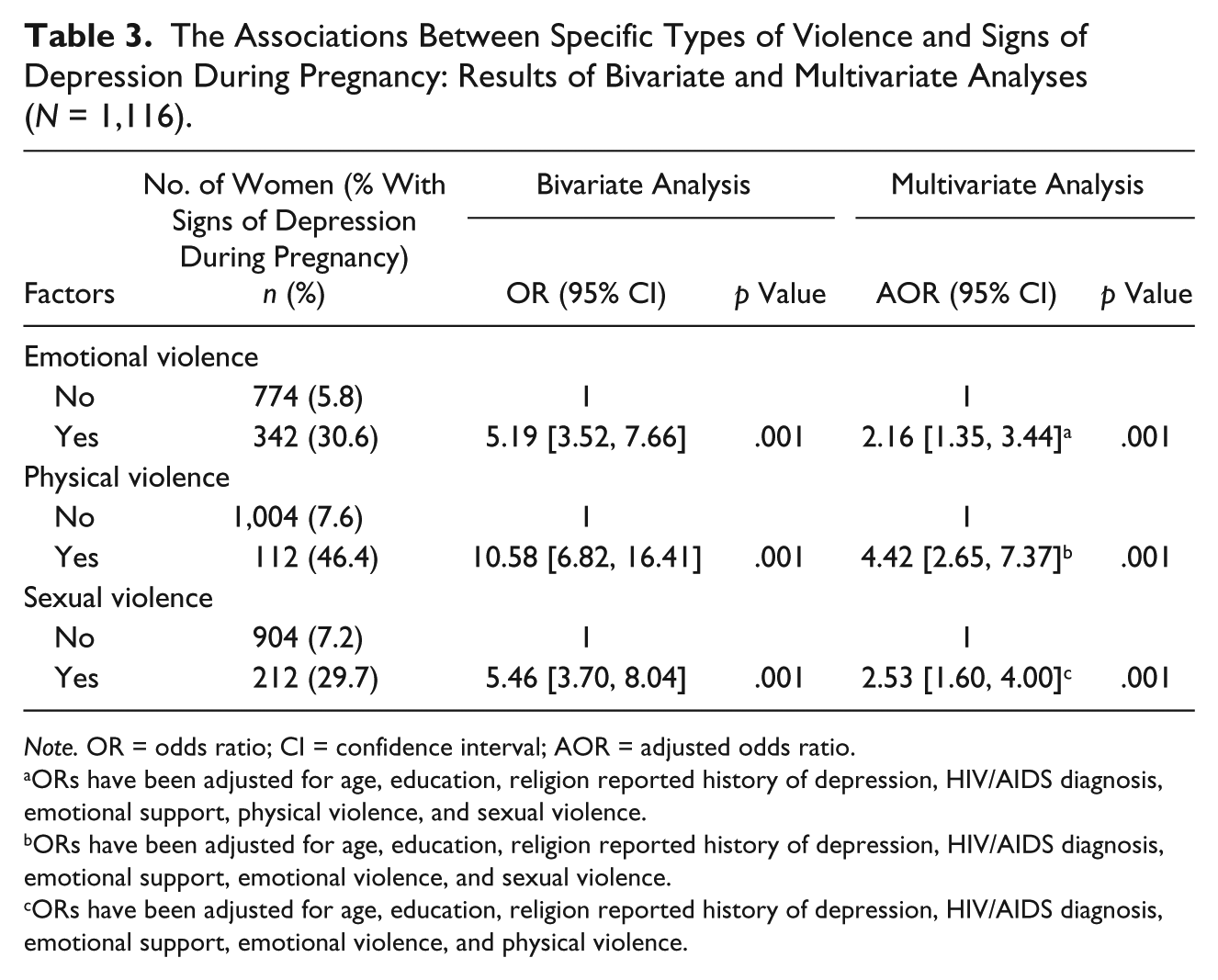
Note. OR = odds ratio; CI = confidence interval; AOR = adjusted odds ratio.
ORs have been adjusted for age, education, religion reported history of depression, HIV/AIDS diagnosis, emotional support, physical violence, and sexual violence.
ORs have been adjusted for age, education, religion reported history of depression, HIV/AIDS diagnosis, emotional support, emotional violence, and sexual violence.
ORs have been adjusted for age, education, religion reported history of depression, HIV/AIDS diagnosis, emotional support, emotional violence, and physical violence.
HIV/AIDS was identified as an effect modifier of the association between emotional violence and signs of depression. A separate stratified multivariate analysis was performed. The result showed that exposure to emotional violence increased the odds of signs of depression by 3 times among women with HIV/AIDS (OR = 2.61; 95% CI = [1.62, 4.20]), whereas there was no statistically significant association between emotional violence and signs of depression among women who do not have HIV/AIDS (OR = 0.09; 95% CI = [0.00, 3.16]).
Discussion
The overall prevalence of signs of depression during pregnancy was found to be 11.5%; 38.8% of the women experienced at least one type of violence during their pregnancy. Emotional violence was the most common type of reported violence and experienced by 30.6% of the pregnant women.
This is the first study in Tanzania to use a validated Swahili version of the EPDS to assess the association between specific types of IPV and signs depression among pregnant women attending ANC clinics. In the present study, 11.5% of all women recruited in the study presented with signs of depression during their pregnancy. This finding is in line with a systematic review of data from eight African countries which reported a weighted mean prevalence of depression of 11.3% (Sawyer et al., 2010). However, more recent findings from two studies performed in Tanzania indicated that the prevalence of depression during pregnancy was 13% (Mahenge et al., 2013) and 39.5% (Rwakarema et al., 2015). The reason for this disparity may be due to different definitions and measurements of depression.
The results of a systematic review of 13 African studies indicated a large variation in the prevalence of IPV during pregnancy ranging from 2% to 57% (Shamu, 2011). However, the prevalence of IPV during pregnancy in the present study (38.3%) was found to be higher compared with a recent study performed among pregnant women in a hospital setting in an urban area of Dar-es-Salaam, Tanzania, which reported a prevalence of 27% (Mahenge et al., 2013). This difference may reflect a higher degree of heterogeneity among the women in the latter study as compared with the study population in the present study.
The results of the multivariate analyses showed that reported exposure to physical violence seems to be the strongest predictor of depression (AOR = 4.42), whereas sexual and emotional violence seem to be of almost similar importance when it comes to prevention of sign of depression in this population. However, our findings differed from other studies where emotional violence were reported to be stronger predictor of depression during pregnancy (Ludermir et al., 2010).
The results of the present study further indicate that pregnant women who seek emotional support from other people than their close family members are more likely to present with signs of depression as compared with those who have access to emotional support obtained from close family members. One possible interpretation is that women who live in a relationship where they cannot expect emotional support from their intimate partner are more prone to develop depression during their pregnancy. Previous studies indicate that emotional support in general plays an important role for the individual in coping with depression (Snell-rood, 2015). Therefore, the finding in the present cross-sectional study may also suggest that lack of emotional support from the partner will make it more difficult for the women, who already have developed a depression, to seek support from her partner.
Limitations
The vast majority of women who were invited to participate in the study gave their consent and were subsequently interviewed (99.4%). This suggests that selection bias during recruitment most likely did not influence the results. Hence, we assume we managed to include most of the pregnant women who attended ANC during the study period. The overall prevalence of women who attend antenatal care in Moshi Municipality is 100% (TDHS, 2010). However, the women recruited from the two ANC clinics comprise only a proportion of pregnant women in Moshi Municipality, and the convenience sampling approach may therefore have influenced the ability to generalize the results to other pregnant women in this specific area. Due to large cultural differences between communities (125 tribes) in Tanzania, the ability to generalize the findings to communities outside Kilimanjaro Region is probably limited.
The cross-sectional study design used in present study to measure the IPV and depression at the same time could lead to difficulty in interpreting the direction of causality.
IPV is a sensitive issue; therefore, it is likely that some women may underreport the occurrence of violence, which may have resulted in an under- or overestimation of the strength of the association between specific types of IPV and depression during pregnancy.
Our study used EPDS to measure signs of depression. However, there was no validation by a psychiatrist to set an EPDS cutoff score which confirms depression.
Conclusions and Recommendations
Signs of depression were found to occur commonly among pregnant women in Moshi Municipality, Tanzania, and were highly associated with IPV. This indicates the need for screening for depression and IPV experiences among pregnant women as part of the routine antenatal services to detect women who are at high risk of depression and offer supportive counseling and/or referral to appropriate services.
Formation of formal community social support services may help to offer professional advice for women who cannot get support from their close family members and may reduce the signs of depression among pregnant women who are victims of IPV.
Footnotes
Acknowledgements
The authors would like to register their appreciation to all the women from Majengo and Pasua Clinics who participated in this study without whom this research would not have been possible and all research assistants who how interviewed the women.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study was funded by DANIDA (the Danish International Development Agency grant number 12-006KU), as part of a larger research project, “The Impact of Violence on Reproductive Health in Tanzania and Vietnam,” with the overall aim of assessing the associations between intimate partner violence (IPV) and women’s reproductive health in semi-urban areas of Tanzania and Vietnam.