
Abstract
Sexual assault is a common traumatic experience that can have a wide-ranging impact on psychological functioning, including experience of depressive symptoms. Although many studies have examined lifetime rates of depression among those with sexual assault history, less is known regarding risk factors for depressive symptoms following recent sexual assault. The study examined whether drug use history is uniquely related to depressive symptoms following recent assault. N = 65 individuals, 95.4% female; 73.8% White; M(SD)age = 28.89 (10.29), who had recently experienced sexual assault (less than 60 days) and completed a SAMFE (sexual assault medical forensic examination) were interviewed via phone and completed questionnaires regarding depressive and acute/post-traumatic stress symptoms and substance use history. Demographic information as well as information related to the assault was also collected. 68.7% of the sample reported clinically significant levels of depressive symptoms (PHQ-9, Patient Health Questionnaire, scores ⩾ 12). In a linear regression adjusted for acute/post-traumatic stress (b = 0.26, p < .01) and other variables, polydrug use was significantly associated with depressive symptoms (b = 3.26, p = .04). Single-drug use (b = 0.96), physically forced sexual assault (b = −1.11), victim–perpetrator relationship (b = 0.15), prior sexual assault (b = −1.02), alcohol misuse (b = −0.09), age (b = 0.07), race (b = 2.78), and days since assault (b = −0.02) were not significantly associated with depressive symptoms (all ps > .05). Results highlight the potential role of drug use history in increasing risk of experiencing clinically significant depressive symptoms following recent assault.
Sexual assault is reported by 17% to 25% of U.S. adults (Elliott, Mok, & Briere, 2004) and can have a wide-ranging impact on psychological functioning (Dworkin, Menon, Bystrynski, & Allen, 2017). Although post-trauma depressive symptoms have been associated with a poorer mental health trajectory (O’Donnell, Creamer, & Pattison, 2004), risk factors for depressive symptoms immediately following sexual assault are not well examined. Substance use history may be one such risk factor, as it often co-occurs with both sexual assault and depressive symptoms (Grice, Brady, Dustan, Malcolm, & Kilpatrick, 1995; Volkow, 2004). Although the risk of substance use (alcohol and drug use) following assault is well-studied (Langdon et al., 2017), less research has examined how substance use history may influence onset of depressive symptoms following a recent assault. To begin to address this gap, the current study reports on preliminary findings from a pilot study examining whether substance use history is uniquely related to depressive symptoms following recent sexual assault. These preliminary findings encourage future research in this area with the goal of informing appropriate screening in acute responses to sexual assault, such as during the sexual assault medical forensic examination (SAMFE), to improve early intervention and prevention of psychological sequelae following sexual assault.
Depression and Sexual Assault
Depressive symptoms are common after sexual assault (e.g., Kilpatrick et al., 2003), likely in part due to concerns related to self-blame, stigmatization and negative self-appraisal, and perceived lack of control (Koss & Figueredo, 2004). However, much of the research on depression among individuals who have experienced sexual assault has focused on lifetime depression, and there is less research examining depressive symptoms more acutely following recent assault (Mgoqi-Mbalo, Zhang, & Ntuli, 2017). Although natural recovery for depressive and other trauma-related symptoms can occur within the first 3 months post-trauma (Frank, Turner, & Stewart, 1980), many individuals continue to experience long-term symptoms. More severe depressive symptoms early in trauma recovery may be a risk factor for developing other issues, such as post-traumatic stress disorder (PTSD; O’Donnell et al., 2004). Much of the research on depression and sexual assault has focused on the comorbidity of PTSD and depression, and there is some debate over whether depression and traumatic stress symptoms are separate constructs (Grant, Beck, Marques, Palyo, & Clapp, 2008) or both part of a broader post-traumatic distress pathology (Au, Dickstein, Comer, Salters-Pedneault, & Litz, 2013). Thus, additional research on depressive symptoms within the early stages following assault while adjusting for acute post-traumatic stress symptoms is warranted.
Alcohol Use, Drug Use, and Depressive Symptoms
Individuals who have experienced sexual assault are at increased risk of alcohol and drug use disorders, likely in part due to experiencing PTSD and depressive symptoms (Kilpatrick et al., 2003). Moreover, there is evidence for a reflexive association between alcohol/drug use and depressive symptoms (e.g., Schuckit, 2006). For example, individuals may “self-medicate” with drugs or alcohol to cope with depressive symptoms or distress following traumatic or negative events (Langdon et al., 2017). Chronic substance use can also lead to neurobiological changes that increase vulnerability for depression (Volkow, 2004). Despite evidence for this reflexive association, sexual assault research has predominantly focused on alcohol and drug use post-assault or alcohol/drug use as a risk factor for experiencing sexual assault (Kilpatrick et al., 2003; Langdon et al., 2017). Less is known regarding how history of alcohol and drug use might influence risk of experiencing depressive symptoms in the early stages following a sexual assault. There is evidence that individuals with a history of substance use (i.e., alcohol and drug use) have lower distress tolerance and are more likely to rely on avoidant coping strategies in response to distress (Buckner, Keough, & Schmidt, 2007; Simons, Gaher, Correia, Hansen, & Christopher, 2005); thus, these factors may increase risk of experiencing depressive symptoms post-assault. Even further, those with a history of use may reinitiate or continue use post-assault and potentially exacerbate depressive symptoms and increase risk of a poorer or longer recovery (see Langdon et al., 2017). In fact, there is evidence that drug use prior to the assault is associated with substance abuse following the assault and increased risk of experiencing greater mental health symptoms related to post-rape stress (Resnick, Walsh, Schumacher, Kilpatrick, & Acierno, 2013; Walsh et al., 2017). The current study expands on these findings by exploring whether drug and alcohol use history may increase risk of experiencing post-assault depressive symptoms, in particular in the early stages following assault.
Characteristics of the Assault, Demographics, and Depressive Symptoms
Characteristics of the assault have also been shown to be associated with depressive symptoms. For example, sexual assaults involving physical injury, physical force, or threats of force are associated with particularly heightened risk of experiencing depressive symptoms (Carretta & Burgess, 2013; Zinzow et al., 2010). Furthermore, individuals who have a closer relationship with the perpetrator typically report greater depressive symptoms (Goldsmith, Chesney, Heath, & Barlow, 2013; Martin, Cromer, DePrince, & Freyd, 2013) perhaps due to greater self-blame and risk of ongoing abuse. Individuals with a prior sexual assault history may also be at heightened risk, as revictimization is associated with more severe lifetime depressive symptoms (Najdowski & Ullman, 2011). However, research to date has not yet examined the characteristics of a recent sexual assault as associated with post-assault depressive symptoms.
Individual demographics, such as age and race, are also related to more vulnerability for depressive symptoms. White women (Pegram & Abbey, 2019; Sigurvinsdottir & Ullman, 2015) as well as individuals who experience sexual assault at earlier ages (Dunn, Nishimi, Powers, & Bradley, 2017) reported more severe depressive symptoms. Again, it is unclear how demographic factors might be associated with depressive symptoms following a recent assault. Elucidating risk factors for post-assault depressive symptoms may inform secondary prevention efforts during, or immediately following a SAMFE in the emergency department (ED).
Current Study
The current study examined potential risk factors for post-assault depressive symptoms among individuals who received a recent SAMFE in the ED. Based on research examining associations between lifetime sexual assault and depressive symptoms, the current study examined alcohol and drug use (Kilpatrick et al., 2003), acute and post-traumatic stress symptoms (Dworkin et al., 2017), assault characteristics (Carretta & Burgess, 2013; Zinzow et al., 2010), and demographic factors (Dunn et al., 2017; Pegram & Abbey, 2019) as correlates of post-assault depressive symptoms. By examining depressive symptoms after a recent sexual assault, focused prevention efforts can be developed to reduce the likelihood or long-term impact of experiencing post-assault depression.
Specifically, we examined whether alcohol use, drug use history, acute or post-traumatic stress symptoms, assault characteristics (victim–perpetrator relationship and type of assault), and demographic factors were related to experiencing depressive symptoms. We hypothesized that individuals reporting history of alcohol misuse and more extensive drug use history (i.e., past history use of multiple drugs) would report more depressive symptoms based on findings that polydrug users often report more severe depression and anxiety compared with single-drug users (Malow, West, Corrigan, Pena, & Lott, 1992; McMahon, Malow, & Loewinger, 1999). We also hypothesized that drug use would be associated with depressive symptoms, even adjusting for other important variables, including characteristics of the assault, prior sexual assault history, and individual demographics, as described above.
Method
Participants and Procedure
Participants included individuals who indicated interest in behavioral and medical follow-up after receiving a SAMFE at the local ED within 120 hr of the assault. Follow-up screening calls were completed by postbaccalaureate-, masters-, and doctoral-level providers and supervised by a licensed clinical psychologist. Individuals were called up to 3 times with the first attempted call occurring within 10 days of the SAMFE. Only individuals who completed the routine clinical follow-up screen within 60 days of the assault and had complete data on study variables were included in the current study, N = 65; 95.4% female; 73.8% White; M(SD)age = 28.89 (10.29).
Measures
Demographic information
Participants were asked their racial/ethnic identity. Those who identified as White (1) were compared with those who were a racial/ethnic minority (0). Participant age at the time of the assault was calculated using medical records.
Sexual assault characteristics
Participants were asked the date of their assault and the days since assault were calculated. Participants were also asked if they knew the perpetrator (0 = no; 1 = yes) and whether they experienced forced sexual assault (0 = no; 1 = yes). Participants also reported on whether they previously experienced sexual assault (0 = no; 1 = yes).
Alcohol misuse
Individuals completed the Alcohol Use Disorders Identification Test—Consumption Questions (AUDIT-C; Bush, Kivlahan, McDonell, Fihn, & Bradley, 1998) to assess for problematic alcohol use. Three items assess quantity, frequency, and problems, with higher summed scores indicating more severe problem alcohol use (α = .80).
Drug use
Participants were asked about lifetime drug use (yes or no to any drug use for nonmedical reasons). Those who reported use also reported on type of drugs used. Participants were categorized as nondrug users, single-drug users, or polydrug users. Of note, all single-drug users reported only cannabis use, thus, this group can also be classified as cannabis-only users. Two dummy variables were created to compare polydrug use (1) and single-drug (or cannabis-only) use (1) to nonuse.
Depressive symptoms
The Patient Health Questionnaire (PHQ-9; Kroenke, Spitzer, & Williams, 2001) was used to assess depressive symptoms in the past 2 weeks. Participants rated nine items on a scale from 0 (not at all) to 3 (nearly every day). Total scores range from 0 to 27. Scores of 12 or higher are considered clinically significant (α = .86).
Acute and post-traumatic stress symptoms
The Post-traumatic Stress Disorder Checklist (PCL-5; Weathers et al., 2013) was used to assess both acute (within 30 days of the assault) and post-traumatic stress (after 30 days of the assault). Participants indicated how much they were bothered by 20 symptoms on a scale from 0 (not at all) to 4 (extremely), with total scores ranging from 0 to 80. Clinical cutoff score for PTSD is 33 (Bovin et al., 2016; α = .94).
Statistical Analyses
We conducted a linear regression using maximum likelihood (ML) estimation in SPSS 24.0 with depressive symptoms (PHQ-9) as the dependent variable. The following dichotomous variables were included: race, victim–perpetrator relationship, whether physical force was used, previous sexual assault history, single-drug use, and polydrug use. Age, days since assault, alcohol misuse, and acute/post-traumatic stress symptoms were entered as continuous variables. Only individuals with complete data were included in analyses (N = 65; n = 18 excluded for missing data).
Results
Preliminary Results
Across the sample, 69.7% (n = 53) reported clinically significant levels of depressive symptoms (i.e., PHQ-9 total score ⩾ 12). Only two individuals who completed the questionnaires more than 30 days after the assault reported nonclinical levels of depression, suggesting the majority of individuals did not experience natural recovery within 60 days post-assault. There was also high comorbidity among depression and acute/post-traumatic stress: 55.1% (n = 43) of individuals had significant depressive and acute/post-traumatic stress symptoms (Table 1).
Sample Demographics and Study Variable Descriptive Statistics.

Note. N = 65. Values are in terms of M(SD) or n(%). Depressed individuals are those with a PHQ-9 ⩾ 12. ϕc = Cramer’s V. Participants with complete data are shown. AUDIT-C = Alcohol Use Disorders Identification Test–Consumption Questions; PCL = Post-traumatic Stress Disorder Checklist; PHQ = Patient Health Questionnaire.
p < .05. **p < .01.
Linear Regression With Depressive Symptoms
Overall, 70% of the model variance was accounted for by the independent variables (R2 = .70). Polydrug use was significantly related to depressive symptoms (b = 3.26, p = .04), even adjusting for acute/post-traumatic stress (b = 0.26, p < .01) and other variables. Single-drug/cannabis-only use (b = 0.96), forced sexual assault (b = −1.11), victim–perpetrator relationship (b = 0.15), prior sexual assault (b = −1.02), alcohol misuse (b = −0.09), age (b = 0.07), race (b = 2.78), and days since assault (b = −0.02) were not significantly related to depressive symptoms (all ps > .05; Table 2).
Linear Regression Predicting Depressive Symptoms.
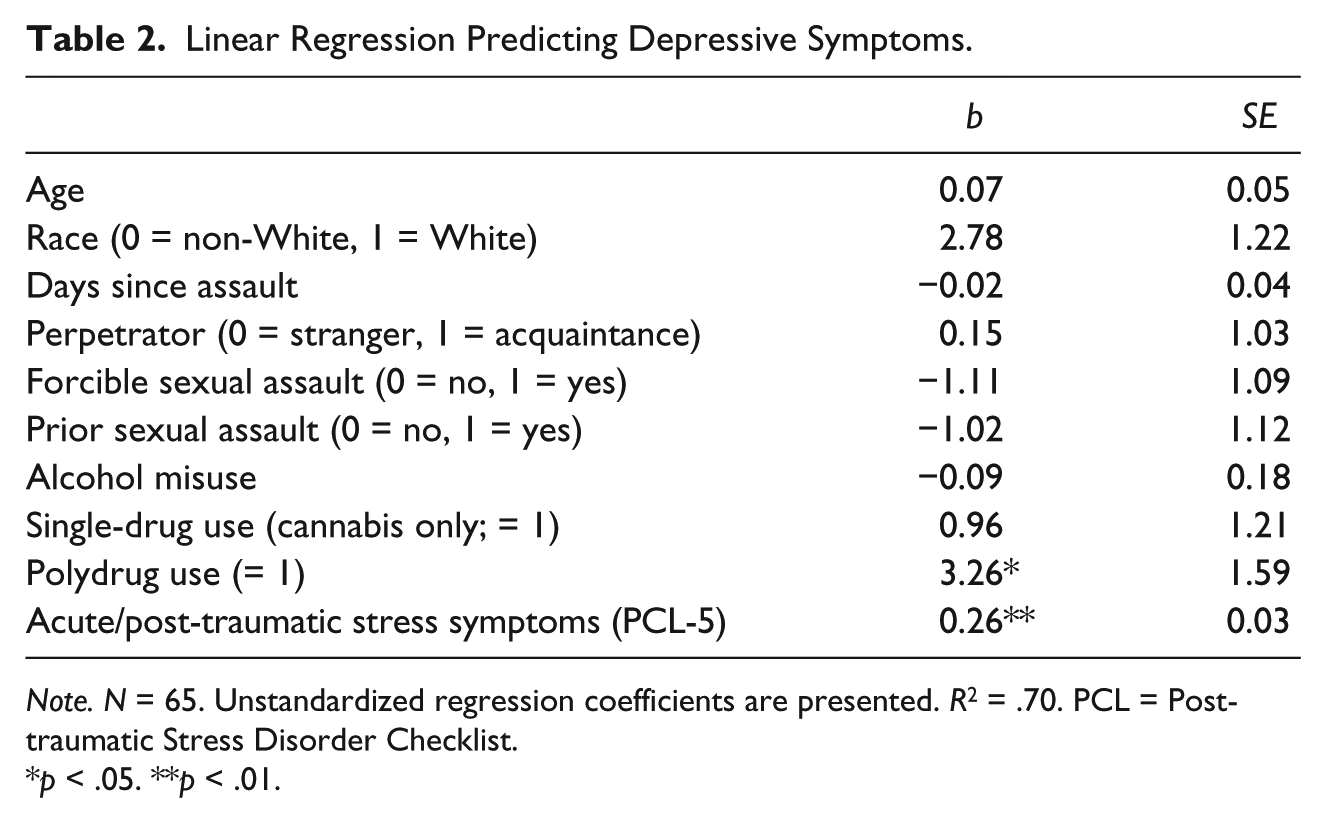
Note. N = 65. Unstandardized regression coefficients are presented. R2 = .70. PCL = Post-traumatic Stress Disorder Checklist.
p < .05. **p < .01.
Discussion
The current study examined whether history of drug use was related to experiencing post-assault depressive symptoms, as well as potential associations between acute or post-traumatic stress symptoms, alcohol misuse history, assault and demographic characteristics, and prior sexual assault history with post-assault depressive symptoms. History of drug use was associated with depressive symptoms, such that those who reported any lifetime use of multiple drugs reported more severe depressive symptoms following recent sexual assault. Acute/post-traumatic stress symptoms were also related to depressive symptoms. Furthermore, individuals who identified as White were also more likely to report depressive symptoms compared with racial/ethnic minorities. Neither age, days since assault, forced sexual assault, alcohol misuse history, nor victim–perpetrator relationship were uniquely associated with depressive symptoms.
Individuals with a history of polydrug use reported more severe depressive symptoms compared with non- and single-drug users. Although most studies examine risk of substance use (i.e., alcohol and drugs) following assault or risk of experiencing assault based on substance use, the current findings suggest that history of drug use may increase risk of experiencing significant depressive symptoms in the early recovery period following assault. Although the mechanisms for this are unclear, there are a few potential explanations. Drug use may be a sign of preexisting depressive symptoms, given their high comorbidity (Schuckit, 2006). There is also evidence for underlying traits related to both drug use and depressive disorders that may explain the association. Those who report history of drug use are more likely to report poorer coping skills, lower distress tolerance, and higher stress sensitivity, which may leave one more vulnerable to experiencing more severe depressive symptoms following an assault (e.g., Buckner et al., 2007). Still, regardless of the mechanism, these findings suggest drug use may be a marker for vulnerability to more severe distress pathology following an assault.
Also of note is that all single-drug users were cannabis users; these patterns of drug use may reflect the fact that cannabis is the most widely used drug in the United States (Substance Abuse and Mental Health Services Administration [SAMHSA], 2015) or these patterns may be unique to the sample. Discussion of specific effects of cannabis compared with other drugs in relation to depression risk is not possible from these results; further research is needed to examine potential unique relationships between specific drugs and depression risk. Nonetheless, we can postulate that findings might be related to previous evidence that the extent and severity of drug use (in this case, use of multiple drugs) is related to extent and severity of depressive symptoms (Malow et al., 1992).
These results are particularly important given the recency of sexual assault in the sample, as fewer studies have examined depressive symptoms before individuals can seek services or potential for experience post-assault recovery (Mgoqi-Mbalo et al., 2017). The study is cross-sectional, and thus, we do not know the long-term trajectory of symptoms; however, findings suggest the potential for early detection of potentially chronic possibly psychological distress following assault. Future research should examine the trajectory of depressive symptoms over time following assault.
This study is not without limitations. First, alcohol misuse, history of prior sexual assault, and other assault characteristics were not significantly related to depressive symptoms, contrary to existing evidence (Langdon et al., 2017). One reason for discrepant findings could be due to the small sample size, which limited power to detect significant effects. Second, the sample was predominantly White and female, thus we could not examine differences across other ethnic groups or gender differences. Third, drug use was assessed using an open-ended question as part of clinical care; we did not assess for onset of or current drug/alcohol use nor extent of drug/alcohol use problems. Future studies should include more comprehensive assessments of substance use disorders to determine relationships between substance use and depression.
Conclusion
Findings highlight the importance of assessing depressive symptoms postsexual assault as well as the potentially important role of history of drug use in increasing risk of depressive symptoms following assault. These preliminary results support the need for future research to better understand early depressive symptoms following sexual assault, such as incorporating screening for depression and drug use during the SAMFE to better triage individuals to needed care.
Footnotes
Acknowledgements
The authors would like to acknowledge the clinical staff, volunteers on the project, and individuals and community partners who assisted with project coordination, which include, but are not limited to Mollie Selmanoff, Dr. Kathleen Gill-Hopple, Dr. Gweneth Lazenby, Dr. Ryan Byrne, Dr. Rosaura Orengo-Aguayo, Karen Hughes, People Against Rape, and Dr. Heidi Resnick.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Manuscript preparation was partially supported by a grant from the National Institute on Drug Abuse (K23DA042935 to Dr. Gilmore) and by the South Carolina Clinical & Translation Research (SCTR) Institute, with an academic home at the Medical University of South Carolina NIH—NCATS Grant Number UL1 TR001450. This project was also supported by the National Institude on Mental Health (T32MH018869). This project is also supported by the Federal Formula Grant 2015 VA GX 0001, awarded by the Office of Victims of Crime, U.S. Department of Justice through the South Carolina Department of Public Safety to Dr. Gilmore. Any points of view or opinions contained within this document are those of the author and do not necessarily represent the official positions or policies of the U.S. Department of Justice.