
Abstract
Victims of intimate partner violence (IPV) are frequent attendees at health care facilities. Although most literature on this subject focuses on developed or Western countries, there is a dearth of information from Asian countries. This study aims to estimate the prevalence of IPV among women attending urban primary care services in Malaysia and to identify the risk factors associated with IPV. Six out of 15 available public primary care clinics in the federal territory of Kuala Lumpur, Malaysia, were randomly selected. The sampling size for each clinic was conducted proportionate to the clinic’s average daily patient attendance. A total of 882 women participated in this study via a self-administered questionnaire. We administered the women’s experience with battering scale (WEB-scale) to estimate the prevalence of psychological violence and included a screening question for physical and sexual assault. The results showed that 22.0% of the women surveyed reported experiencing IPV. Ethnicity appears to be a significant predictor, with Chinese and Indian women reporting IPV at a higher rate than Malay women. Women with IPV are more likely to come from lower income households, have witnessed parental IPV, receive less social support, and have poorer psychological well-being. Our findings indicate that the prevalence of IPV among women attending urban public primary care clinics is high. Health care providers should pay close attention during clinical encounters for any sign of IPV, particularly among those presenting with risk factors.
Intimate partner violence (IPV) is a major public health problem with serious health consequences for women and children, both acutely and in the long term (Chan, Tiwari, Fong, & Ho, 2010; Coker, Sanderson, & Dong, 2004; Fanslow, 2017; Othman, Goddard, & Piterman, 2014). It refers to any behavior that causes physical, psychological, or sexual harm by one partner in an intimate relationship toward another. The term “battering” relates to a severe and escalating form of partner violence characterised by multiple forms of abuse, terrorisation and threats, and increasingly possessive and controlling behavior on the part of the abuser (Heise et al., 1999, p. 5). The prevalence of IPV varies among countries. An analysis conducted by the World Health Organization (WHO) based on existing data from over 80 countries reported that almost one third (30%) of all women who have been in a relationship experienced some form of physical and/or sexual violence from their intimate partner (WHO, 2016). A population study in Malaysia reported that 14.5% of women are estimated to experience violence at the hands of a partner at some time in their lives (Shuib et al., 2013).
Several studies of IPV in Malaysia have explored various aspects of the issue. These include the prevalence and social determinants of IPV (Awang & Hariharan, 2011; Yut-Lin & Othman, 2008), the impact of IPV (Ali, Tengku Hassan, Salleh, & Yusoff, 2012; Saddki, Suhaimi, & Daud, 2010), coping mechanisms of survivors (Oon et al., 2016), patterns of help-seeking behavior and barriers among survivors (Othman et al., 2014; Tengku Hassan, Ali, & Salleh, 2015), perspectives of health care providers regarding IPV (Colombini, Mayhew, Ali, Shuib, & Watts, 2013; Othman & Mat Adenan, 2008), and the process and policy of health models for violence response as well as the strengths and challenges of those models (Colombini, Ali, Watts, & Mayhew, 2011; Colombini, Mayhew, Ali, Shuib, & Watts, 2012).
The Domestic Violence Act 1994 (amended in 2017) provides protection for IPV victims. Unlike child abuse, there is no mandatory reporting for IPV cases (Domestic Violence Act [Amendment], 2017). In the Malaysian health care system, the one-stop-crisis center (OSCC) provides prompt and comprehensive support for the victims using a violence-response model. Nearly all government-funded hospitals have an OSCC located in the emergency department (Colombini et al., 2011). These OSCCs receive referrals from other health care providers, including primary care facilities.
The prevalence of IPV recorded in primary care settings varies, depending on the definition and the tools used for screening (Hegarty, Gunn, Chondros, & Small, 2004; Moghaddam Hosseini, Asadi, Akaberi, & Hashemian, 2013; Ruiz-Pérez, Plazaola-Castaño, & del Río-Lozano, 2007; Yut-Lin & Othman, 2008).
Common tools used to screen for IPV in primary care practice include the conflict tactics scale (CTS; Straus, 1979), the index of spouse abuse (ISA; Hudson & McIntosh, 1981), the abuse assessment screen (AAS; McCauley et al., 1995), the partner violence screen (PVS; Feldhaus et al., 1997), and the women abuse screening tool (WAST; Brown, Lent, Schmidt, & Sas, 2000). These tools were developed to allow IPV screening in clinical settings and for research purposes. They have been tested for their psychometric properties and accuracy in identifying IPV (Nelson, Bougatsos, & Blazina, 2012).
The prevalence of IPV varies across countries, but several factors associated with an increased risk of IPV are consistent. These include young age, low education status of either partner, low socioeconomic status, substance or alcohol use (Abramsky et al., 2011; Ali, Ali, Khuwaja, & Nanji, 2014; Ali & Bustamante, 2007; Pandey, Dutt, & Banerjee, 2009), smoking status (Ali et al., 2014), and attitudes that condone partner abuse or controlling behavior (Abramsky et al., 2011; Pandey et al., 2009). Other contributing factors include past experience of childhood abuse and growing up within a household where domestic violence occurred (Abramsky et al., 2011; Fanslow, 2017; Pandey et al., 2009). The results of some studies suggest that formal marriage reduces IPV while having extramarital relations and marital dissatisfaction further contribute to IPV (Abramsky et al., 2011; Vameghi, Amir Ali Akbari, Alavi Majd, Sajedi, & Sajjadi, 2018). Several other studies also indicate that women with no or less social support were more likely to be exposed to IPV (Djikanovic, Jansen, & Otasevic, 2010; Tiwari et al., 2010; Vameghi et al., 2018).
Women living in abusive relationships frequently present to health care facilities (Gass, Stein, Williams, & Seedat, 2010; Othman et al., 2014; Ulrich et al., 2003). These women may present with symptoms associated with abuse, including physical injuries, mental health symptoms, and relationship issues (Fanslow & Robinson, 2011; Hankin, Smith, Daugherty, & Houry, 2010; Pigeon et al., 2011; Ruiz-Pérez et al., 2007; Saddki et al., 2010). However, disclosing abusive relationships is difficult for many women, due to cultural beliefs that relationship problems are a private matter, fear of their husbands, or lack of courage to leave the relationship. Women may have low expectation for support from health services in situations where they received inappropriate responses from health care providers (Othman et al., 2014). The women’s presentation may be subtle, and without attentive screening, health care providers may miss discovering patients’ IPV backgrounds and histories of abuse. A systematic review on screening women for IPV reported beneficial evidence for health care providers to screen female patients for IPV in health care settings, as this will increase victim identification (Nelson et al., 2012). Failure to identify women with IPV backgrounds who come to health care facilities will only lead them to return to their abusive relationships unsupported (Astbury et al., 2000; Tengku Hassan et al., 2015), rendering them vulnerable to further abuse.
The aim of this study is to assess the prevalence of IPV among women attending urban primary care clinics and to examine the associated risk factors. This study focuses on primary care settings, as local information regarding IPV from these settings is still lacking. An urban location was chosen, as 73.7% of the Malaysian population resides in urban areas (Department of Statistics Malaysia, 2010). We hope that the information gathered may assist in the development of appropriate intervention strategies in primary care settings concerning the management of women with experience of IPV.
Method
Study Design and Sample
The study was conducted in Kuala Lumpur, which is the capital city of Malaysia. There are 15 public primary care clinics in Kuala Lumpur. The health care system of Malaysia consists of public and private sectors. The public sector is heavily subsidized by the government, and its populace can access primary health care services at minimal cost (RM 1 = US$0.25). In this study, six out of 15 available public primary care clinics were randomly selected. The number of patients attending these six clinics varies according to the size of the clinic. To ensure a greater representation from each clinic, the total number of participants recruited from each clinic was proportionate to that clinic’s size.
Participants were considered eligible if they were women aged 16 years or older, had previously been or were currently in an intimate relationship, were able to read and write, and were not accompanied by a partner. The recruitment for each clinic ceased when the maximum sample size estimated for each clinic was achieved.
The total sample size required for this study was calculated based on the previous reported prevalence of IPV of 6.0% (Yut-Lin & Othman, 2008) in a similar setting with 95% confidence interval (95% CI). This gave a sample size of 750. The sample size was then inflated by 20% for nonrespondents to give a final sample size of approximately 900.
Data Collection
Data collection was conducted over a period of 2 months. Every third patient attending the selected clinics who met the eligibility criteria was invited to participate in the study. Once verbal consent was obtained, a self-administered questionnaire was given to the respondent. Participants completed their questionnaires while waiting for consultation with the doctors. A room was available if participants felt that they needed some privacy to answer the questionnaire. The completed questionnaires were placed in a locked box to maximize patients’ privacy. The average time to complete the questionnaire was approximately 10 min to 15 min. The collected questionnaires were kept safe and accessible only by the researchers and authorized personnel. After completing the questionnaire, informational leaflets on IPV and services available to battered women and children, such as the Women’s Aid Organisation (WAO), were offered to the participants.
Measurement
The participants self-administered a questionnaire entitled “Women’s Wellness Questionnaire.” Participants were asked about their sociodemography, IPV experience, perceived relationship problems, safety issues, background of parental IPV, help-seeking behaviors, psychological health, and perceived social support (Goldberg et al., 1997; Smith, Earp, & DeVellis, 1995; Zimet, Dahlem, Zimet, & Farley, 1988). The following tools were used for measurement:
a. IPV: Participants were screened for experience of IPV in the past 12 months. A 10-item women’s experience with battering scale (WEB-scale; Q1-Q10) was used. The WEB-scale is a unique measure that operationalizes the experiences of battered women rather than the nature of the physical or psychological abuse they encounter (Smith et al., 1995; Smith, Smith, & Earp, 1999). This scale has been shown to be able to identify more women experiencing partner violence and thus have its clinical value (Coker, Pope, Smith, Sanderson, & Hussey, 2001). In this scale, “battering” is defined as women’s continuous perceptions of susceptibility to physical and psychological danger and loss of power and control in a relationship with a male partner. It has good internal consistency, with a reported Cronbach’s alpha coefficient of .95 (Coker et al., 2007). In the current study, the Cronbach’s alpha coefficient was .93. The responses to the WEB-scale in this study were simplified by limiting the response options to “agree” or “disagree” for each of the 10 items. A validation analysis for this modified scale showed high sensitivity (79.8%), specificity (99.4%), and positive predictive value (96.6%) compared with the full scale of responses (Coker et al., 2007). Participants were also screened for assault (Q11), defined as experiencing either physical abuse, sexual abuse, or both. The question on assault states
Is (was) this partner physically violent towards you? Physically violent means (did) he punch, kick, hit, shove, slap, choke, or physically attack you in other ways that could result in an injury? It also means being to do sexual acts when you don’t want to.
Participants who responded affirmatively to two or more of the WEB-scale items (Q1-Q10) were considered WEB-positive or positive for battering (Coker et al., 2007). Participants were considered to have experienced assault if they answered yes to the question on assault (Q11). Participants were grouped as having positive IPV experience if they were screened WEB-positive or answered yes to the assault question. In addition, participants were asked “Do (did) you feel that violence or abuse is (was) a problem in your relationship with this partner?” to clarify their perception of violence as a problem in a relationship (Q12; Coker et al., 2007).
b. Social support: The multidimensional scale of perceived social support (MSPSS) was used to provide an assessment of the social support available to the participants from three sources: family, friends, or significant others (Zimet et al., 1988). The MSPSS scale consists of 12 items, with item responses ranging from 1 to 7 (very strongly disagree to very strongly agree), and the scores are average item scores. The MSPSS has good internal reliability, with a Cronbach’s alpha coefficient of .91 (Ng, Amer Siddiq, Aida, Zainal, & Koh, 2010; Zimet et al., 1988). The Cronbach’s alpha coefficient for the current study was .92. Higher scores indicate greater social support from the various possible sources.
c. Health status: The 12-item general health questionnaire (GHQ-12) developed by Goldberg et al. (1997) was used to assess psychological well-being or detect general psychiatric morbidities. The GHQ-12 has good internal reliability, sensitivity, and specificity in detecting more common psychiatric disorders (Navarro et al., 2007; Yusoff, 2010). A binary scoring system with responses coded as 0–0–1–1 and a total score ranging from 0 to 12 were used. The cut-off point of 3/4 to discriminate between poor (score ≥ 4) or normal (score 0-3) psychological well-being were used.
d. Perceived danger: Participants were asked about perceived dangers to their lives and those of their children and offered a selection of possible reasons for this perception. They were also asked whether they had ever been physically abusive to their children, with a selection of possible reasons.
e. Witnessing parental IPV: Participants were considered to have past experience of witnessing parental IPV if they responded affirmatively to questions regarding witnessing physical, emotional, or sexual abuse between their parents.
f. Help-seeking behaviors: To understand help-seeking behaviors, participants were asked whether they had ever asked for any assistance related to their relationship, the types of assistance, and the person from whom they have sought assistance.
The study questionnaire was first developed in English and was pilot-tested for face and content validation on 30 patients. It was then back-translated from English into three languages: Bahasa Malaysia, Tamil, and Mandarin and vice versa.
Key Variables
The dependent variable in this study was current IPV, which was defined as violence by a current partner or ex-partner within the past 12 months. Two types of IPV that were screened for in this study were psychological violence and assault. The independent variables were sociodemographics, witnessing parental IPV, social support systems, and psychological health. The sociodemographic components included age, ethnicity, education level, employment, and household income, which were used as proxies for socioeconomic status and included total number of children.
Ethical Consideration
This study was approved by the University of Malaya Medical Ethical Committee Institutional Review Board (Approval Number 751.5) and the Malaysian Medical Research and Ethics Committee (Reference Number NMRR-09-1102-5023). We explained to potential respondents that participation in the study was on a voluntary basis and refusal to participate would not in any way influence their current or future consultation or medical treatment. Completion and return of the questionnaire indicated the participant’s consent to participate in the research. Each participant was offered written information about available counseling and support services. No complaints were received, and, to the best of the researchers’ knowledge, no adverse events were encountered during the conduct of this study.
Data Analysis
Data were analyzed using SPSS Version 22.0. Descriptive analyses were performed to obtain frequency and proportions. Numerical variables were tested for normality using the Kolmogorov–Smirnov goodness-of-fit test. Most numerical variables were not normally distributed and were analyzed using nonparametric tests such as the Mann–Whitney U test. Chi-square tests were performed to determine significant differences of categorical variables. Bivariate analyses between each independent variable and each outcome variable were conducted independently to identify associated factors. Only significant variables from the bivariate analysis were considered and entered into a regression model. Multiple logistic regression was used to analyze factors affecting current IPV and assess goodness of fit using a multicollinearity test, the LR test for possible two-way interaction, the Hosmer–Lemeshow goodness-of-fit test, and a receiver operating characteristic (ROC) curve. The final model included all variables with p < .05. An adjusted odd ratio (AOR) and 95% CIs were reported.
Results
Participants’ Characteristics
Of the 904 women approached, 884 women agreed to participate in this study, giving a response rate of 97.8%. Reasons for refusal include being in a rush, not interested, or feeling uncomfortable. Data from two participants were excluded in view of incomplete answers for the IPV screening section. Of the 882 participants, 439 (49.8%) were Malay, 196 (22.2%) were Chinese, and 247 (28.0 %) were Indian. The mean age was 43.8 years (± 12.7 years) with a range from 16 years to 80 years. Nearly one third (n = 251, 28.5%) of the participants had received a primary education, 436 (49.4%) a secondary education, and 195 (22.1%) had received a higher education. Less than half of the participants (n = 379, 42.9%) were employed at the time of the study. The majority of the participants (n = 632, 72.6%) have a low household income of RM 3,000 or less (US$1 = RM 4.28).
IPV Among Women Attending Primary Care Clinics
The prevalence of IPV in the past 12 months among women attending public primary care clinics was estimated to be 22.0% (n = 194). Approximately 13% of them experienced psychological violence only, 0.7% reported assault only, and 8.6% experienced both. Table 1 presents the various types of IPV.
Prevalence of IPV and Types of IPV Reported in the Past 12 Months Among Women Attending Public Primary Care Clinic in Federal Territory, Malaysia (n = 882).
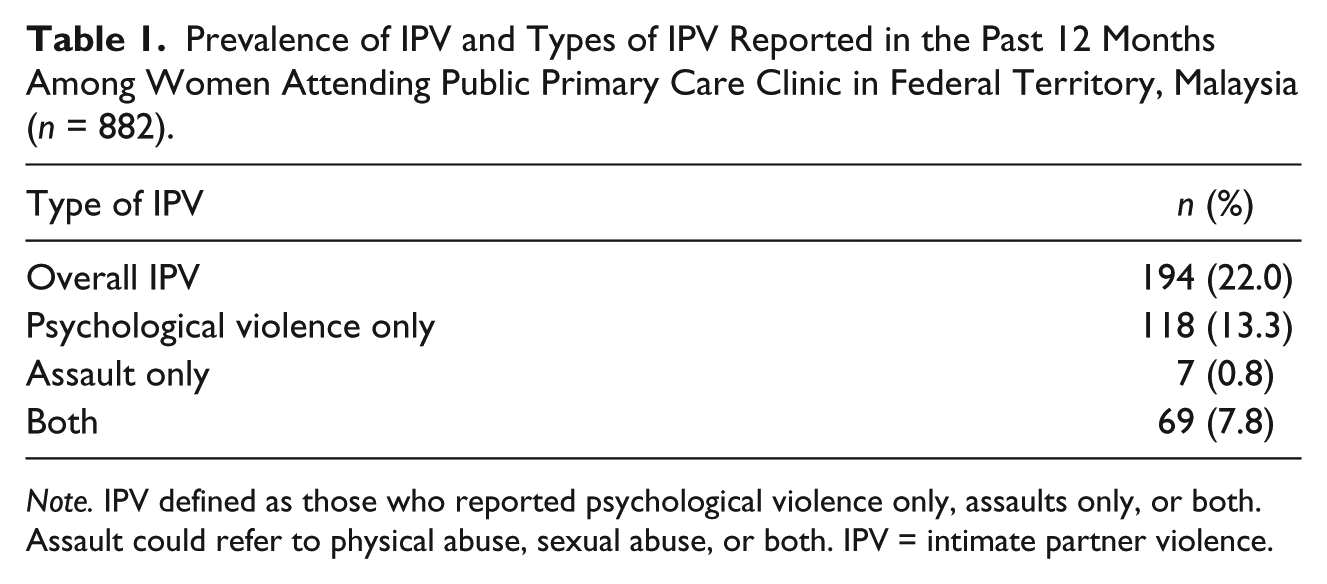
Note. IPV defined as those who reported psychological violence only, assaults only, or both. Assault could refer to physical abuse, sexual abuse, or both. IPV = intimate partner violence.
Profile of Victims’ Help-Seeking Behaviors
One third of those who screened positive for IPV (n = 65, 33.5%) have sought some assistance in their relationship. The types and sources of assistance are reported in Table 2. Half of those who sought help (n = 33, 50.8%) have talked to someone regarding their experiences, and 27 (41.5%) have sought assistance in obtaining a divorce. Seeking assistance for a temporary shelter was reported by 10 (15.4%) women. The main source of assistance was reported as coming from family members (63.1%).
Types and Source of Assistance Sought by Women Reported IPV (n = 65).
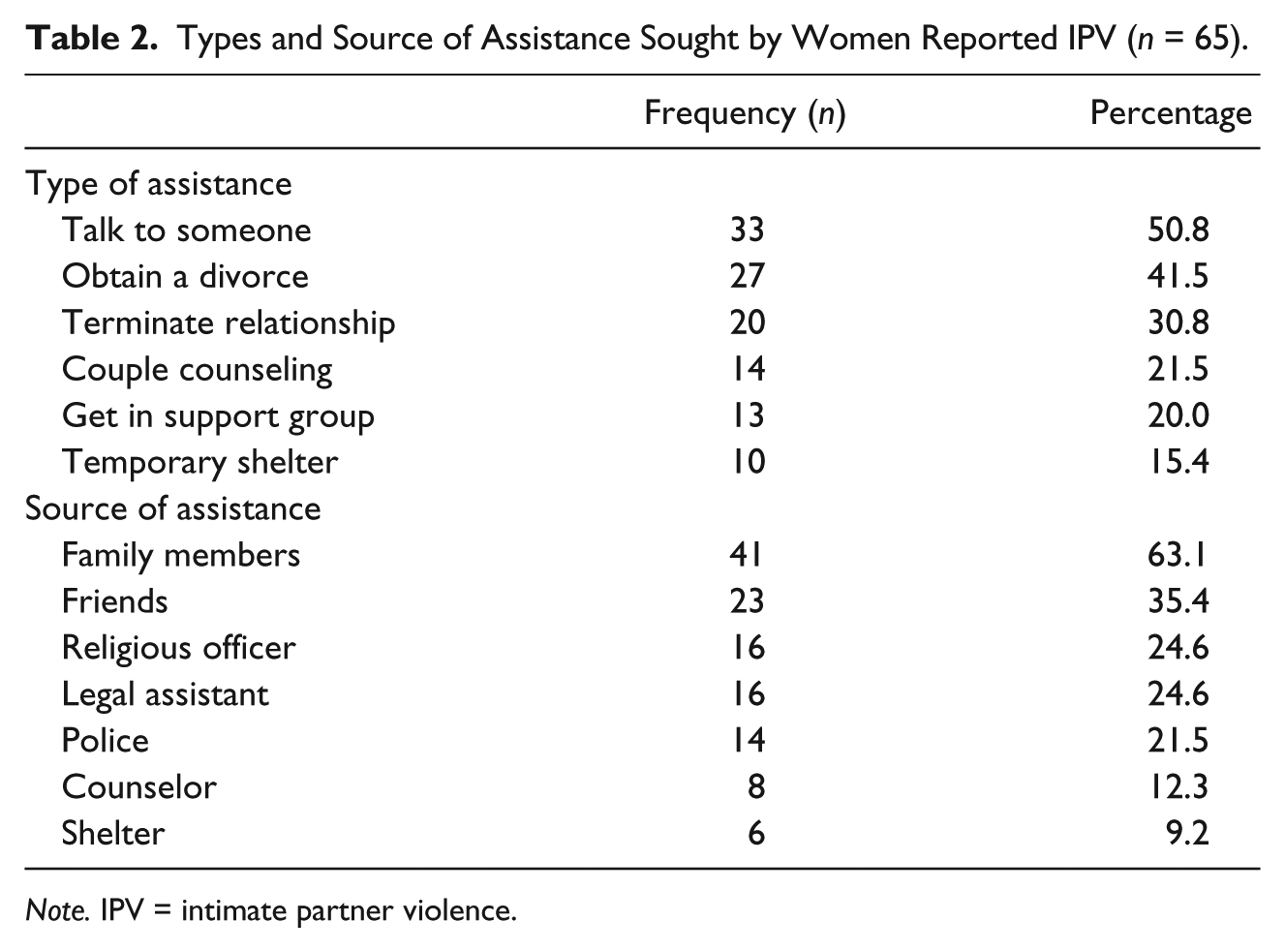
Note. IPV = intimate partner violence.
A total of 46 (23.7%) women with IPV experience reported leaving the relationship temporarily and subsequently returning to their partner. Reasons given include perception of wrongdoing for leaving the relationship from the religious point of view (43.3%), the partner requested them to come back and promised to change (41.8%), concern about leaving their children without a father figure (35.8%), financial problems (25.4%), and being advised by their friends and relatives to stay in the relationship (17.6%).
Safety at Home
When asked whether they felt their life or their children’s lives to be in danger, there was a significant difference in responses between women experiencing IPV and nonvictims. More women experiencing IPV perceived their life or their children’s lives to be in danger (n = 33, 17.1%) compared with women who do not experience IPV (n = 4, 0.6%; p < .001). The reasons for perceived danger to children expressed by women with IPV include worsening of abuse episodes (34.4%), partner abusing the children (28.1%), partner murder threats (25.0%), and partner use of a weapon (12.5%). When asked whether the participants had ever abused their children, more women with IPV reported having abused their children compared with nonvictims (9.8% vs. 0.3%, p < .001).
Risk Factors Associated With IPV
Table 3 presents the results for the association of various sociodemographic backgrounds and other factors with the experience of current IPV among women. There are significant differences between women with IPV and women without IPV in relation to age, ethnicity, education levels, household income, witnessing parental IPV, psychological well-being, and social support systems. Women with IPV experience were much younger, had a lower education level, and tended to come from a low monthly household income. More women with IPV had witnessed parental IPV, received lower social support, and had a poor psychological well-being.
Demographic Characteristics of Women With Current IPV Compared with Non-IPV.
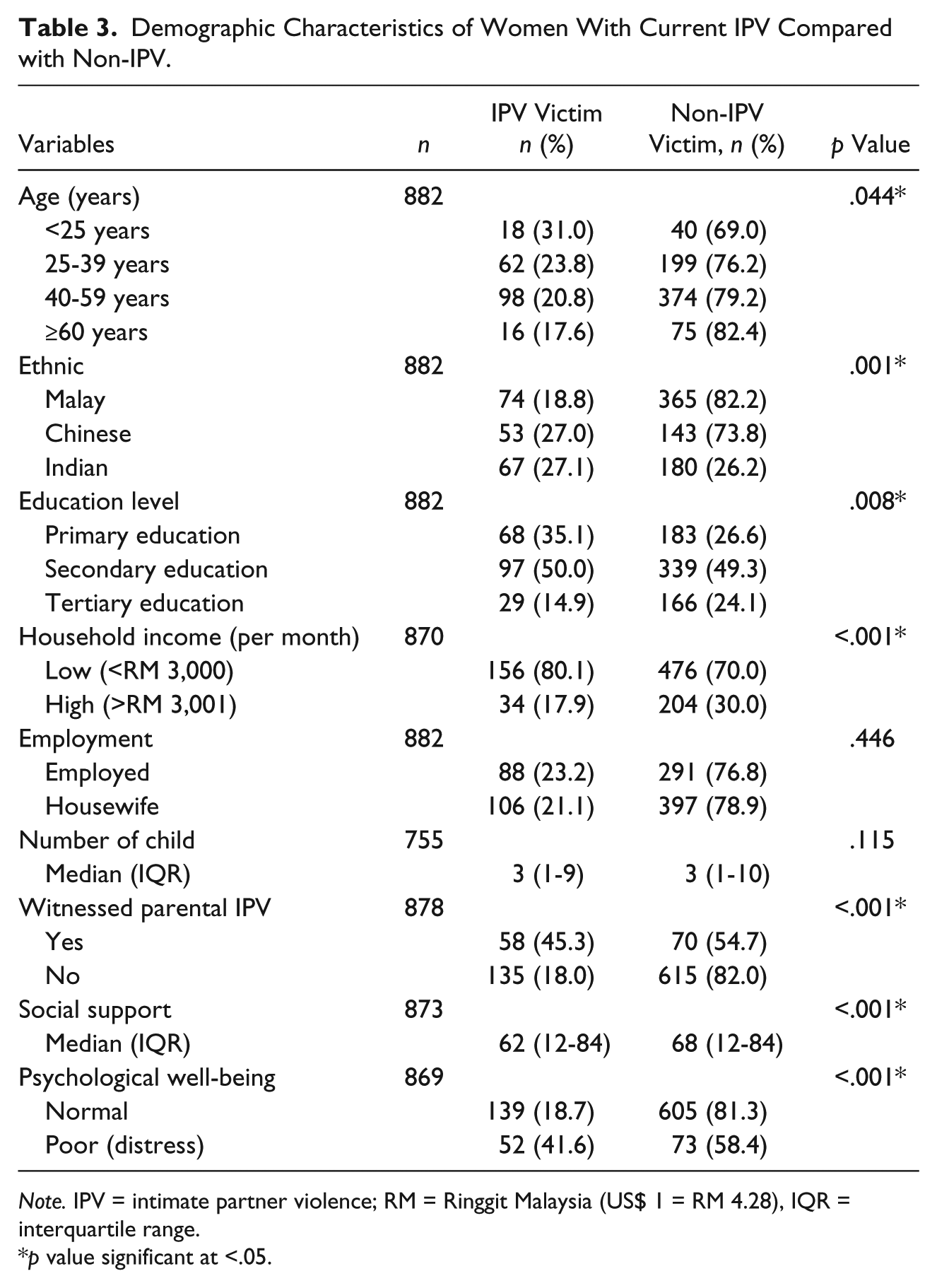
Note. IPV = intimate partner violence; RM = Ringgit Malaysia (US$ 1 = RM 4.28), IQR = interquartile range.
p value significant at <.05.
After adjusting all factors in the multivariate logistic regression model, five independent variables correctly (79.6%) classified of the data set (Table 4). Ethnicity, household income, parental IPV, social support, and psychological well-being were significantly associated with IPV. Women of Chinese ethnicity are 2 times more likely to experience IPV compared with women of Malay ethnicity (AOR = 2.02, 95% CI = [1.30, 3.12]). Household income of RM 3,000 or less was associated with IPV (AOR = 2.04; 95% CI = [1.32, 3.16]). Women who have witnessed parental IPV (AOR = 3.52; 95% CI = [2.29, 5.41]), have less social support (AOR = 0.985; 95% CI = [0.973, 0.997]), or experience poor psychological well-being (AOR = 2.16; 95% CI = [1.38, 3.38]) have a higher likelihood of experiencing IPV.
Factor Associated With IPV (Multiple Logistic Regression).
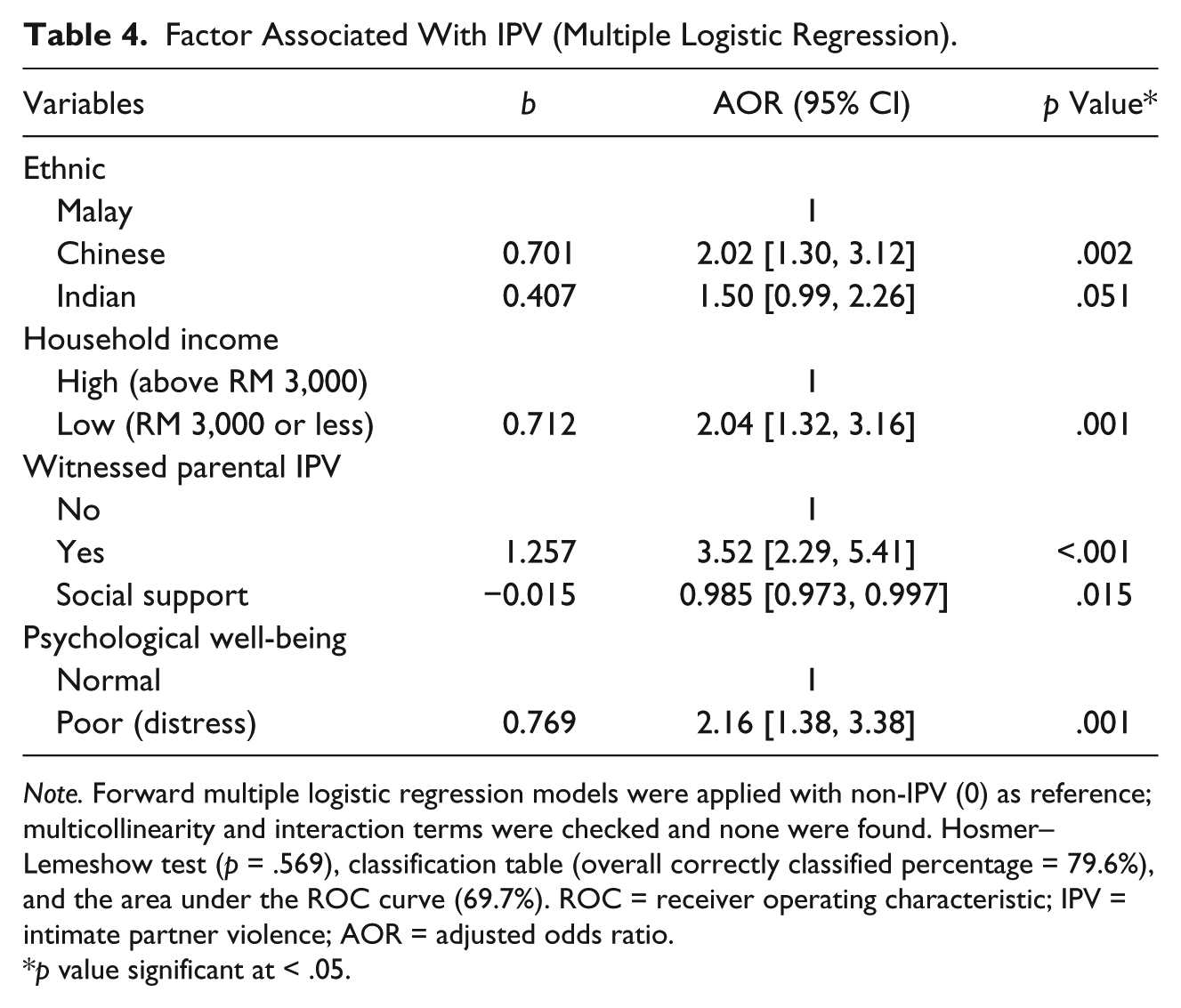
Note. Forward multiple logistic regression models were applied with non-IPV (0) as reference; multicollinearity and interaction terms were checked and none were found. Hosmer–Lemeshow test (p = .569), classification table (overall correctly classified percentage = 79.6%), and the area under the ROC curve (69.7%). ROC = receiver operating characteristic; IPV = intimate partner violence; AOR = adjusted odds ratio.
p value significant at < .05.
Discussion
This study found that one in five women attending urban public primary care clinics had experienced IPV in the past 12 months. The prevalence of IPV was nearly 4 times higher in this study when compared with a previous local study at a primary care setting (Yut-Lin & Othman, 2008). Unlike the previous study, where women were interviewed face-to-face by the enumerators, the current study used a self-administered questionnaire. This increased the likelihood that participants would report any experience of abuse. Self-administered questionnaires have been shown to be more effective in identifying victims compared with face-to-face interviews, particularly in the area of interpersonal violence (Canterino, VanHorn, Harrigan, Ananth, & Vintzileos, 1999; Kataoka, Yaju, Eto, & Horiuchi, 2010; Webster & Holt, 2004). Cultural values such as privacy of marriage (Bailey, 2012; Siegel, 1996) and maintaining the family’s reputation (Tengku Hassan et al., 2015) make open communication with others regarding abuse experience difficult among women. The prevalence of this study falls in the range of other countries by the WHO (15.0%-71.0%; Garcia-Moreno et al., 2006). The 22.0% IPV prevalence in the past 12 months in this study is reported to be much higher than studies in the United States (up to 19.9% IPV prevalence; Coker et al., 2007; McCloskey et al., 2005; Sprague et al., 2014), but lower than the findings in Australia (up to 28.9%; Hegarty et al., 2004; Mazza, Dennerstein, & Ryan, 1996). This could be due to the different screening tools used, the definition of IPV given, and the approach used in getting the information. Although the study by Coker et al. (2007) used a WEB-scale that focused on battering experience, the rest of the different screening tools in other studies identify IPV victimization based on the actual abusive behaviors experienced by victims.
Among women identified as experiencing IPV, those of Malay ethnicity have the lowest percentage of IPV compared with Indian and Chinese women. After adjusting for other factors in the multivariate logistic regression model, Chinese women were twice as likely to be victims of IPV compared with Malay women. There was no significant difference between Indian women’s odds of being victimized and those of Malay women. This finding may indicate the actual prevalence of IPV among these groups. However, it is also possible that the Malay respondents were not disclosing their relationship problems, as they are known to be relatively less forthcoming about personal relationships (Oon et al., 2016; Tengku Hassan et al., 2015).
Similar to other studies (Ellsberg, Winkvist, Pena, & Stenlund, 2001; Garcia-Moreno et al., 2006), nearly one fifth of the IPV victims in this study have left their partner, but later returned to the relationship. The most common reason for returning to the relationship was reported as perceived wrongdoing from a religious point of view by leaving the husband. Some women view marriage as a religious commitment and feel that it is their obligation to maintain the relationship (National Resource Center on Domestic Violence, 2007). According to Lindgren and Renck (2008), the process of leaving an abusive relationship has a few phases that are influenced by several factors, including fears. Different forms of fear can have the effect of either preventing women from leaving, or encouraging them to do so. In terms of seeking assistance, a local study by Oon et al. (2016) supported the finding that most women confide in someone close to them regarding relationship issues.
The majority of the women victims in this study had children under their care during the study period, and they reported concern for the safety of their life and the lives of their children. The safety of the victims is at risk particularly from escalation of the abuse, the perpetrator abusing the children, and death threats by their partner (Ferguson, 2009). Findings also showed that more women victims reported abusing their children compared with nonvictims. Appel and Holden (1998) described a sequential perpetrator abuse model where the female partner suffers abuse by her male partner, and abuses her child at the same time.
This study found that women with lower household income are twice as likely to experience IPV. Poverty limits the choices and resources for women victims (Goodman, Smyth, Borges, & Singer, 2009; Vest, Catlin, Chen, & Brownson, 2002). It is also possible that IPV affects the productivity of victims, and thus their employability (Anderberg, Rainer, Wadsworth, & Wilson, 2016). Women who have witnessed parental IPV were 3 times more likely to experience IPV themselves. Intergenerational transmission of violence has been postulated to explain the link between witnessing IPV and IPV in subsequent relationships (Black, Sussman, & Unger, 2010; Djikanovic et al., 2010).
This study found that better social support acts as a protective factor against IPV experience among women. Women living in abusive relationships tend to be isolated and have difficulty accessing support, often as a consequence of the controlling behavior of their relationship partner (Hegarty & Taft, 2001). Women identified as having psychological distress are twice as likely to be IPV victims. Several studies have shown the close association between IPV and victims’ mental health (de Barros et al., 2016; Hegarty et al., 2004; Vest et al., 2002).
Study Limitations and Strengths
Interpretation of the results requires some consideration due to certain limitations in this study. A short duration of data collection is one of the limiting factors in this study. Related incidences, if present during the data collection period, may influence the overall findings of the study. This could include special media coverage on IPV, a change in IPV-related public policy, or an environmental disaster. There was a concern for missing IPV victims by excluding women who were unable to read or write, and those who came to the clinic with their partner. Illiteracy has been associated with low household income (Martinez & Fernandez, 2010), which is correlated with IPV. Women who came with their partner were not recruited for this study as a measure of safety. Unfortunately, we did not capture the information regarding the number of patients, which were excluded due to these two situations. As a result, underreporting of IPV may occur, and as a result, these findings may underestimate the actual prevalence of IPV.
The IPV experiences reported by participants in this study were based on self-report, and thus may be prone to recall bias. Physical abuse and sexual abuse were measured using only one question, which did not distinguish the two types of abuse. Furthermore, a single question was unable to identify the degree of severity of the assault. The relationship between IPV and risk factors cannot be shown to be causative based on cross-sectional data. The generalizability of the study is limited to those attending public health facilities only, and those who were literate. There is a possibility that the study may have missed those who are severely abused and have no access to health care. Out of consideration for women’s safety, women who attended the practice with their partners were not interviewed in this study. IPV is a sensitive topic, and thus social desirability bias may exist. However, the self-administered questionnaire and anonymity might increase participants’ honest answers. Evidence has shown that women are more comfortable with self-administered questionnaires than with a face-to-face approach. In addition, self-administered questionnaires yield less missing data (MacMillan et al., 2006). Self-administered questionnaires were also found to have identified more instances of IPV when compared with face-to-face interviews (Kataoka et al., 2010). The major advantage of this study is the high response rate (98.5%) from the participants.
Conclusions and Implications
IPV is a significant problem identified among women attending urban Malaysian public primary care clinics. Women with IPV experience were more likely to come from lower household incomes, have witnessed parental IPV, have less social support, and experience poor psychological well-being. Women who self-identified as having experienced IPV were concerned not only for their own safety but also for that of their children as well. Health care providers should have a high level of awareness of IPV among women with risk factors to offer assistance to these women. This study contributes to the growing literature demonstrating the need to encourage screening of at-risk women among health care providers in primary care clinics in Asia. The prevalence rates of IPV among women are a sign of the necessity for local awareness and prevention programs in preventing chronic and serious effects on women and their children. More research is needed to more accurately specify how health care providers should proceed in assisting women to improve their safety and social support resources.
Footnotes
Acknowledgements
The authors acknowledge the contribution of Jeyaswari R. Kutty, Geeta, Angie, Yeoh, and Lee Sian Boy for their assistance in data collection.
Declarations of Conflicting Interest
The author(s) declare no potential conflicts of interests with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the University of Malaya (Grant Number: RG074/09HTM).