
Abstract
Early sexual behavior plays a vital role in female reproductive health. Victimization experiences such as sexual harassment may have a unique impact on girls’ sexual health. We examined the prospective associations between sexual harassment during adolescence and high-risk sexual activity in early adulthood. Using mixed-effects logistic regression models, we tested associations between sexual harassment at ages 13 to 15 years and sexual risk behaviors at ages 16 to 20 years, controlling for depression and peer victimization. We used a community sample in Pittsburgh, PA. Through the Pittsburgh Girls Study, 2,450 girls were recruited when they were between the ages of 5 and 8 years, with approximately equal numbers in each of the four age groups. Approximately half of the girls sampled were African American (52%), and 41% were European American. The remaining girls were described as multiracial or representing another race. Data were collected via an annual nonclinician administered interview. Results indicated that participants who experienced sexual harassment as adolescents (21%) were more likely to have multiple sexual partners and more likely to have contracted a sexually transmitted infection (STI) in early adulthood. Sexually active 16-year-olds who had been sexually harassed were over 3 times more likely to have had two or more partners in the past 30 days. These effects were maintained controlling for other types of peer victimization and depression. Sexual harassment was not significantly associated with birth control use. These results suggest that sexual harassment has downstream effects on women’s health.
Introduction
Sexual victimization can take broad and varied forms. For girls, the most severe forms of sexual victimization can have immediate and negative outcomes, including medical (e.g., urinary tract infections, sexually transmitted infections [STIs], pregnancy), behavioral, and emotional problems (Frothingham et al., 2000; Messina & Grella, 2006; Newman et al., 2000; Wekerle & Wolfe, 2003). Sexual victimization also affects how girls express their sexuality. Theoretically, early victimization may create maladaptive schemas or narratives around sexual activity. Dunlap, Golub, and Johnson (2003) described a model in which sexual victimization creates a perception or assumption that sexual activity is a normative part of any relationship and further is a way to establish and keep affection, intimacy, and perhaps material objects. This in turn may lead girls to initiate sex earlier, more often, with more people, and with less consistent condom use for fear of sabotaging the attempt for closeness (Browning & Laumann, 1997; Coker et al., 1994). Although there are many factors involved in sexual decision making for adolescent girls, with such a strong link between severe forms of sexual victimization and high-risk sexual outcomes, we posited that less overt but common forms of sexual victimization in adolescence, such as sexual harassment, may also have harmful implications for reproductive health and wellness.
Peer victimization (also referred to as harassment or bullying) is broadly defined as overt or covert victimization where the child/adolescent is threatened or physically hurt by a peer (Cole, Maxwell, Dukewich, & Yosick, 2010; Crick, Casas, & Ku, 1999). The 2017 Youth Risk Behavior Survey found that 19.0% of high school students nationwide were bullied on school property during the 12 months before the survey (Kann et al., 2018). Other reports of bullying cite between 40% and 80% of school-age children experiencing peer victimization at some point during their school careers (Sanders & Phye, 2004). Sexual harassment is defined by the U.S. Equal Employment Opportunity Commission as “unwelcome sexual advances, requests for sexual favors, and other verbal or physical harassment of a sexual nature.” Sexual harassment is often considered in the context of the workplace, but reports of school bullying demonstrate that this type of sexual victimization and harassment also occurs among school-aged peers. As is the case with research around sexual victimization, these experiences have been referred to using various names in the literature. These experiences have sometimes been referred to in publications by the American Association of University Women (AAUW) as peer sexual harassment victimization (PSHV; AAUW, 2001) and have included a range of behaviors such as verbal comments, being brushed up against, being flashed, having sexual rumors spread about you, or being physically touched in a sexual way. Brion-Meisels and Raveche Garnett (2016) used the term relational youth violence to describe behaviors (physical, relational, sexual, verbal, or psychological) and policies (formal or informal) that are intentionally or unintentionally harmful to a young person or group of young people, based on real or perceived power imbalances that reflect larger social structures of equity and power.
Relational youth violence is proposed as an umbrella term that represents the intersectional nature of peer violence in adolescence that may be helpful when developing prevention strategies. Some authors have suggested that behaviors that include gender and sex are best separated from bullying and referred to as sexual harassment. Duncan (1998) used the term “sexual bullying” to describe bullying during adolescence, including verbal forms such as sexual name-calling and offensive remarks and sexual rumors and physical forms such as unwanted touching (Duncan, 1998; Page, Shute, & McLachlan, 2015; Shute, Owens, & Slee, 2008). In this work, however, the authors use the term sexual harassment to refer to unwanted sexual touching, comments, and advances in adolescence.
Research on sexual harassment in adolescence has been mostly conducted in the school environment. Reports show sexual harassment is a pervasive issue for adolescents, with 81% of high school students reporting experiencing some form of sexual harassment in their school lives (AAUW, 2001). In a longitudinal study of sexual harassment in adolescence, 30% of ninth-grade girls reported being “touched, grabbed, or pinched in a sexual way” (Petersen & Hyde, 2009). A survey of 250 female high school students from four school districts in Minnesota found that approximately half of the girls had been verbally and physically sexually harassed at school by a peer (Strauss & Espeland, 1992). Results from a survey of seventh- to 12th-grade adolescents conducted by the AAUW revealed that 56% of girls reported being sexually harassed, and half of that group reported that they did nothing afterward in response to being sexually harassed (Hill & Kearl, 2011). Both boys and girls can experience sexual harassment, but their experiences differ. Girls experience more severe forms of sexual harassment and experience them more often than their male counterparts (AAUW, 2001). Girls are more likely to be objectified, put down, and treated differently, whereas boys experience vulgar, aggressive, and homophobic comments based on asserting a toxic masculinity common in our culture (McMaster, Connolly, Pepler, & Craig, 2002). Female victims of sexual harassment in schools reported a range of outcomes, including feeling cheap and degraded, and feelings of guilt, confusion, helplessness, and fear. They also reported that these experiences caused humiliation and diminished self-esteem due to the lack of control they felt in the moments of harassment (Fineran & Bennett, 1998). Additional outcomes include behavior problems, educational problems, difficulty concentrating, absenteeism, and poor academic performance (Hill & Kearl, 2011). In a look at how sexual harassment affects risk of future harassment, victimization, and adjustment, Chiodo et al. (2009) found that sexually harassed ninth-grade boys were at increased risk of physical dating violence victimization, physical peer violence victimization, and peer relational victimization. For ninth-grade girls, sexual harassment similarly increased risk of physical dating violence victimization and physical peer violence victimization, but not peer relational victimization. To date, no study has tested the impact of sexual harassment by peers on reproductive health and sexual risk-taking in a community sample of girls. Given the link between more serious forms of sexual victimization and such behaviors, it seems prudent to test whether common, albeit less serious forms of sexual victimization distinct from peer victimization also confer risk of sexual risk-taking behaviors.
In the present study, we test the hypothesis that experiences of sexual harassment during adolescence would uniquely contribute to more frequent sexual risk-taking behavior in early adulthood (e.g., number of partners, frequency of STI infection, and lack of contraceptive use) while controlling for nonsexual forms of peer victimization and depression.
Method
Participants
Participants consisted of adolescent girls enrolled in the Pittsburgh Girls Study (PGS; Keenan et al., 2010). The PGS, started in 1999, is a multiple cohort, multi-informant, prospective study designed to investigate the developmental precursors and risk factors for behavioral and emotional problems. The PGS used a stratified random sampling design, with oversampling of households in low-income neighborhoods, to identify girls between the ages of 5 and 8 years. Through enumeration of households, 2,992 families were identified, with 2,875 families successfully contacted for participation. A final number of 2,450 families agreed to participate in the PGS. Approximately half of the girls were African American (52%), 41% were European American, and the remaining girls were described as multiracial or representing another race (7%). 1 Retention of the sample in each year has been very high, ranging from a high of 97.2% to 84.5% in the most recent year. Some of the variability in retention from year to year is due to difficulty tracking participants; a minority of families have refused to participate over the years. Comparisons of those assessed and those not assessed at each age were conducted using chi-square tests. Girls lost to attrition were more likely to be from families not receiving public assistance and were more likely to be European American.
Procedures
Approval for all study procedures was obtained from the University of Pittsburgh Institutional Review Board. Written informed consent from the caregiver and verbal assent from the child were obtained prior to data collection. Annual interviews are conducted separately for the parent and child in the home by trained interviewers. When girls reached the age of 18 years, they provided written informed consent. Families were compensated for their participation. The PGS uses an accelerated longitudinal design, with relatively equal numbers of girls at ages 5, 6, 7, and 8 years being enrolled in the study at Wave 1. Data are then aligned by age for longitudinal analyses.
Measures
Outcome: Sexual behavior
Sexual behaviors and sexual risk-taking were assessed using the Adolescent Sexual Activity Index (ASAI, Hansen, Paskett, & Carter, 1999) and an addendum developed for the PGS. The 12 items assessed the presence or absence of presexual and sexual behaviors. Girls reported on whether they have had sex with a boy or a girl in the past year, on the number of sexual partners, and whether they had been diagnosed with or treated for an STI in the past year. Girls reporting no sexual activity in the past year were coded as not engaging in sexual risk-taking.
The ASAI is a reliable measure of presexual and sexual behaviors and has been validated and shown to be internally consistent. For the purposes of this study, we used responses of adolescent participants (ages 16-20) about intercourse, STIs, contraceptive used during last intercourse in the past year, and number of partners in the last 30 days to better capture the occurrence of low base rate behaviors.
Independent variable: Sexual harassment
Sexual harassment was assessed by girls’ yes/no endorsement to the question, “In the past year, have there been times when other kids have grabbed your breasts or bottom when you didn’t want them to, like when you were walking in the hallway at school or when you were out in public such as at a mall or on a bus?” Participants were asked this question starting at age 13 years. This question was developed in response to reports made by girls in earlier waves of the PGS study when asked about their abuse experiences.
Control variables
Depression
Symptoms of major depressive disorder (MDD) were measured using the Childhood Symptom Inventory (CSI-4; Gadow & Sprafkin, 1994) based on parent and child report. The PGS administered the CSI-4 annually to parent and child (beginning at 7 years). The CSI-Norms Manual reported adequate 6-week test–retest reliability of the symptom count and severity of MDD (r = .43, r = .56, respectively; p < .0001). Response choices are “never,” “sometimes,” “often,” and “very often.” For the purposes of the current study, the nine items measuring Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000) symptoms of depression that were endorsed at the level of “a lot,” “all the time,” or “yes,” by either parent or child, were summed to generate symptom counts for ages 13 to 15 years. Estimates of minor depressive disorder and MDD were then generated using DSM-IV-TR criteria for symptom thresholds (APA, 2000). A little less than a third (30.9%) of the girls met criteria for depression (minor or major) between ages 13 and 15 years.
Peer victimization
Starting at age 7, participants responded to nine items assessing frequency of victimization during the past 3 months using the Peer Victimization Scale (PVS; Vernberg, Jacobs, & Hershberger, 1999). Internal consistency of victimization was high (α = .85; StataCorp. 2017). The PVS queries about verbal, physical, and psychological peer violence with three items each. Nine items such as “A student hit, kicked or pushed me in a mean way” and “a kid teased me in a mean way” were measured on a 5-point scale (0 = never, 1 = once or twice, 2 = a few times, 3 = about once a week, 4 = several times a week, and 5 = a few times a week). For the purposes of this study, total scores from responses of participants at ages 13 to 15 years were used. The average peer victimization score and standard deviation for the total sample were 2.46 and 2.81, respectively (N = 2,251).
Data Analysis Plan
Mixed-effects (random intercept, random slope) logistic regression models, with sexual harassment in adolescence and age (i.e., 16-20) as independent variables, were fit. The age by sexual harassment interaction was tested. It was removed from the final model if not statistically significant. We also tested whether peer victimization or depression during adolescence moderated associations between sexual harassment and later sexual behavioral health. Models included average peer victimization score from ages 13 to 15 and depression (minor or major diagnosis between ages 13 and 15). Separate regressions were computed for each of the following dependent variables: (a) intercourse, (b) STI, (c) contraceptive used during last intercourse, and (d) number of sexual partners. Statistical analyses were performed using Stata 15 (Hansen et al., 1999).
Results
Twenty-one percent of the sample reported sexual harassment between ages 13 and 15 years. At age 16, the rate of sex in the last year was 31%, increasing to 74.6% at age 20. At age 16, the rate of STIs in the last year was 3.1%, increasing to 5.9% at age 20. The rate of more than one partner in the last month was 6.2% at age 16 and 4.9% at age 20.
Those who had been sexually harassed were more likely to report sex in the past year compared with those who had not been sexually harassed (odds ratio [OR] = 7.6, 95% confidence interval [CI] = [4.9, 11.7]); this effect was maintained at each age (see Figure 1, Table 1a). Girls who had been sexually harassed were more likely to report an STI diagnosis (see Figure 2, Table 1b). This increase was significant when compared with those who had not been sexually harassed (OR = 1.9, 95% CI = [1.3, 2.8]). At the age of 16 years, 13% of sexually active girls who had been sexually harassed reported more than one partner in the last 30 days, versus 2% of those who had not been harassed (mixed model p = .007). This effect was attenuated at older ages (interaction p = .003, Table 1c).
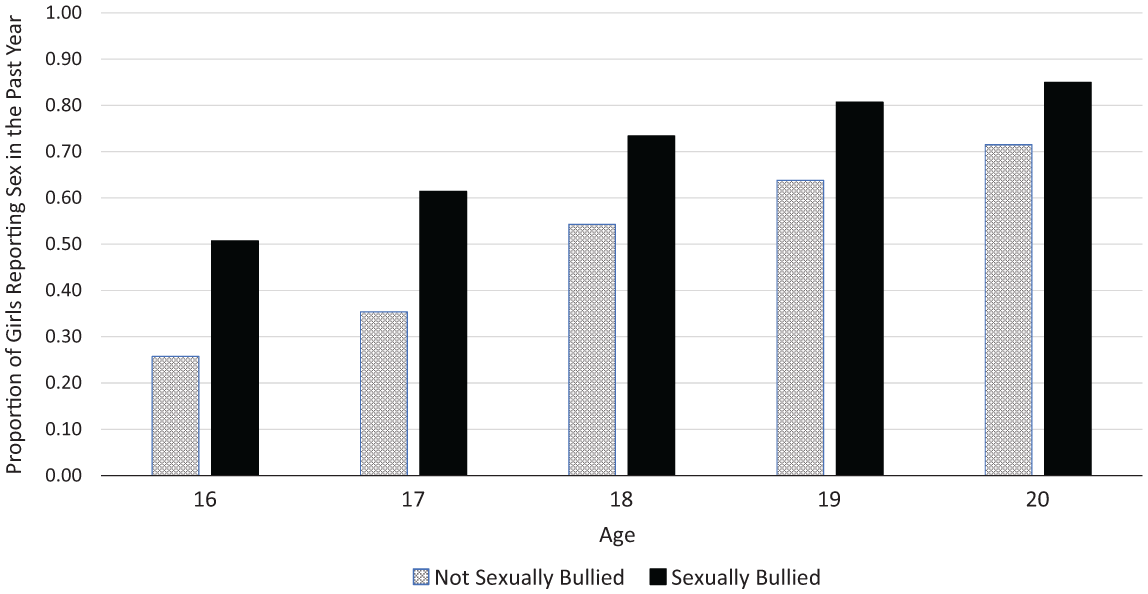
Prospective association between sexual bullying and sexual activity in past year.
Association Between Sexual Harassment in Adolescence and Sexual Behavior in Young Adulthood.

Note. OR = odds ratio; CI = confidence interval.

Prospective association between sexual bullying and sexually transmitted infections (STIs) past year.
The association between sexual harassment and peer victimization during adolescence was moderate and statistically significant: The difference in average victimization scores between the two groups was 1.7 (95% CI = [1.4, 2.0]), p < .001. Peer victimization, however, did not moderate the associations between sexual harassment and later sexual behavior: p values range from .28 for STI diagnosis to .77 for more than one partner.
Discussion
We hypothesized that physical bullying of a sexual nature during adolescence would be prospectively associated with girls’ sexual risk-taking as they enter early adulthood. Our results supported this hypothesis, showing a link between reports of sexual harassment and frequency of sex, acquisition of STIs, and the number of partners. These associations remained after controlling for other nonsexual forms of peer victimization and depression. In addition, although peer victimization and sexual harassment were significantly associated, they did not influence each other when predicting later behavior. These results prompt the use of a wider lens when considering gendered victimization and its negative impact on health. Revealing the impact of this type of peer victimization on girls’ behavior and health may provide an opportunity for targeting early manifestations of behaviors potentially viewed as minor, but fall within the spectrum of sexual assault. Unpacking bullying into that which contains sexual content whether it is homophobic verbal assaults (Espelage, Basile, De La Rue, & Hamburger, 2015, 2012) or unwanted sexual touching is important because it predicts uniquely onto outcomes for adolescent behavior. This particular bullying phenotype is important to capture because it seems to have important associations for sexual behavior as teens develop.
In addition, further research targeting the mechanisms by which sexual harassment increases sexual risk-taking may help to reveal potential protective factors. For example, this type of victimization may weaken the capacity to advocate for oneself or withstand pressure from partners in intimate situations. Understanding this relationship better may help us develop intervention and prevention efforts to protect girls who have had such experiences prior to engaging in more advanced sexual behaviors. These results can also serve as a reminder to pediatricians and gynecologists about the importance of screening for all types of harassment and victimization when meeting with girls. Validating girls’ reports of sexual harassment may help them to engage in a discussion about self-advocacy and encourage them to communicate with caregivers about sexual health and safe sex practices.
Limitations
The current study aimed to explore a potential link between sexual harassment and the reproductive health and wellness of adolescent girls. Research into sexual assault has been limited in its conclusions due to the varied definition of sexual assault used across the research. The current study is also limited by its measurement of sexual harassment. Other studies of sexual harassment have used the Sexual Experiences Questionnaire–Revised (SEQ-R; Fitzgerald, Drasgow, Hulin, Gelfand, & Magley, 1997). The current study did not set out to explore sexual harassment and included the measured question only after research staff noticed girls were reporting these experiences on their own at high frequency. Finally, nearly all participants were at mid to late Tanner’s (1962) stages of breast development by age 13. Thus, we were unable to examine the impact of stage of breast development on experiences of sexual harassment. It is possible that the strength of associations between sexual harassment and later sexual risk-taking may be stronger when experiences occur earlier, particularly if off-time pubertal development increases the likelihood of sexual harassment. Future studies would benefit from including earlier assessments of pubertal development and sexual harassment. This current study demonstrates an original finding and is meant to provide evidence and motivation for further research into the mechanisms through which early encounters with gender-based harassment and violence affect the lives of girls and women.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from National Institute of Mental Health (MH56630) and a Faculty Diversity Career Advancement Grant from the University of Chicago.