
Abstract
Neighborhood factors such as instability and weakened social ties have been linked to both intimate partner violence (IPV) and poor mental health outcomes; however, research has not yet investigated the relationship between IPV and gentrification-specific change, including whether gentrification-related neighborhood factors affect mental health symptoms commonly associated with IPV. This study aims to determine if (a) perceptions of neighborhood connectedness and recent compositional changes (e.g., residential mobility, crime, and infrastructure) are associated with IPV exposure and (b) perceived neighborhood connectedness and compositional change moderates the relationship between IPV and mental health symptoms (i.e., psychological distress, suicidal ideation, suicide attempts). Data from the 2017 Survey of Police-Public Encounters were used, which is an online, cross-sectional, general population survey administered to male and female adults residing in New York City and Baltimore (N = 1,000). Findings suggest that higher levels of neighborhood disconnectedness were associated with higher levels of IPV, whereas higher levels of neighborhood compositional change were associated with lower levels of IPV. Neighborhood disconnectedness and compositional change worsened psychological distress symptoms and suicide risk most strongly among individuals exposed to IPV. Violence prevention and intervention approaches should consider the extent to which neighborhood instability, related to community connectedness and recent compositional change, impacts the safety and mental health of victims of IPV.
Introduction
As a leading cause of morbidity in the United States, intimate partner violence (IPV) remains a significant public health crisis affecting an estimated 1.5 million women and 834,700 men annually (Cronholm, Fogarty, Ambuel, & Harrison, 2011). IPV is characterized by acts of physical, sexual, and/or psychological violence by an intimate partner and its adverse health and mental health consequences are well-documented (Antai & Anthony, 2014; Black et al., 2011; Cronholm et al., 2011; Leiner, Compton, Houry, & Kaslow, 2008). Individuals exposed to IPV tend to report higher levels of psychological distress and suicidal ideation than those without IPV exposure (McLaughlin, O’Carroll, & O’Connor, 2012). Following exposure to IPV, research has shown that 47% of victims experience psychological distress and 8% attempt suicide (Cronholm et al., 2011). However, factors such as social support have been found to attenuate negative mental health symptoms associated with IPV (Coker, Watkins, Smith, & Brandt, 2003; Lanier & Maume, 2009; McLaughlin et al., 2012; Reviere et al., 2007), suggesting that feelings of connectedness and strong social ties may serve as a protective factor against the development of negative mental health sequelae following IPV exposure.
Few studies, however, have assessed neighborhood factors (i.e., resident perceptions) associated with IPV exposure, particularly the extent to which perceived neighborhood factors are related to mental health symptoms commonly associated with IPV. Existing research on IPV points to the influential role of neighborhoods, such as stability and connectedness, in understanding the etiology of IPV, particularly in urban settings (Cronholm et al., 2011; Leiner et al., 2008; Pinchevsky & Wright, 2012; Voith, 2019). Although IPV occurs within all types of neighborhoods and environments, individuals residing in urban areas have an increased likelihood of experiencing IPV in part due to poverty and socioeconomic disadvantage that disproportionately impacts urban communities (Burke, O’Campo, & Peak, 2006; Cronholm et al., 2011; Fox & Benson, 2006; Leiner et al., 2008). In addition, studies assessing the broad effects of perceived neighborhood factors (e.g., social cohesion, collective efficacy, social ties) on mental health suggest that a strong sense of neighborhood connectedness and stability may also act as protective mechanisms against depression and distress symptoms (Hill & Maimon, 2013; Lim et al., 2012). Yet, the extent to which neighborhood perceptions of connectedness and stability attenuates adverse mental health symptoms associated with IPV is not clearly understood.
Emerging research on the issue of neighborhood gentrification has investigated the impact of this phenomena on neighborhood stability in urban U.S. cities, including its potential to disrupt residents’ social ties and sense of neighborhood connectedness (Lim et al., 2017; Schlichtman, Patch, & Lamont Hill, 2017; Versey, 2018). Given that neighborhood connectedness and stability have been identified as protective mechanisms against both IPV and poor mental health (e.g., Beyer, Wallis, & Hamberger, 2015), understanding perceptions of neighborhood connectedness, in relation to recent changes due to gentrification, can be used to guide the development of urban public health interventions aimed at preventing violence and promoting neighborhood health. Furthermore, rapid neighborhood changes and subsequent disruptions in social ties due to gentrification may have unique implications for the safety and mental health of residents who have experienced IPV. Thus, identifying potential buffering effects of perceived neighborhood connectedness and stability on mental health symptoms associated with IPV exposure can assist IPV interventions in targeting protective mechanisms that reduce adverse mental health outcomes associated with IPV.
Using an urban, general population sample of men and women, this study sought to address the following primary research question: Do perceptions of gentrification-related neighborhood connectedness and recent compositional change (e.g., residential mobility, crime, and infrastructure) moderate the relationship between IPV and mental health symptoms (i.e., psychological distress, suicidal ideation, suicide attempts). We hypothesized that neighborhood connectedness would moderate the relationship between IPV and mental health symptoms, where higher levels of neighborhood disconnectedness would exacerbate mental health symptoms among individuals with IPV histories. In addition, based on prior literature highlighting the salient role of social support in mitigating poor mental health outcomes associated with IPV (e.g., Coker et al., 2003), we also assessed moderation effects of social isolation and loneliness (the antithesis of social support) on mental health symptoms associated with IPV (Hawkley & Cacioppo, 2010). Finally, based on prior studies linking neighborhood stability, social cohesion, and collective efficacy more broadly to IPV exposure (Beyer et al., 2015; Pinchevsky & Wright, 2012), we examined the relationship between IPV exposure and perceptions of gentrification-related neighborhood connectedness and compositional change (e.g., residential mobility, crime, and infrastructure).
Method
Study Sample and Procedures
Data were used from the second Survey of Police–Public Encounters (SPPE-II), which is an online, cross-sectional, general population survey administered in March 2017 (DeVylder et al., 2018). The survey was administered using Qualtrics to English-speaking adult residents of Baltimore City and New York City. Participants were recruited using Qualtrics Panels, an online sampling service comprised of panels of several million U.S. residents who consent to periodic survey research. Qualtrics Panels use a quota sampling methodology to recruit demographically representative samples (i.e., ±10% of 2010 census distributions for age, sex, and race/ethnicity within each city) based on geographic household data. Participants are not asked to complete the survey once quotas are met for their demographic group within the boundaries of each city. Monetary incentives were provided to participants who completed the survey at rates determined by Qualtrics. Institutional review board (IRB) approval was obtained from the sponsoring university, and an IRB waiver for written consent was granted. Participants were provided with information on the purpose of the study, and informed consent was obtained by agreeing to proceed to complete the survey online. A total of 1,221 adults agreed to participate in the survey. A total of 221 were excluded due to incorrectly responding to attention checks and discontinuation of the survey prior to completion resulting in a final sample size of 1,000 (81.9% participation rate).
Measures
Psychological distress
The K6 was used to assess clinically significant psychological distress symptoms in the past 4 weeks (Kessler et al., 2003). The K6 scale uses 5-point Likert-type response options (1 = all of the time, 2 = most of the time, 3 = some of the time, 4 = a little of the time, 5 = none of the time) asking participants to indicate how much of the time they felt the following: (a) so sad that nothing could cheer you up, (b) nervous, (c) restless or fidgety, (d) hopeless, (e) that everything was an effort, and (f) worthless. Items were reversed coded and summed (scores range from 0 to 24). Higher scores indicate greater levels of distress. Internal consistency and reliability of the K6 in this sample was excellent (α = .91).
Suicidal ideation and attempts
Past-year suicidal ideation and attempts were measured with two questions from the National Survey on Drug Use and Health (NSDUH) “In the past 12 months, have you ever seriously thought about committing suicide?” and “In the past 12 months have you ever attempted suicide?” (Miller et al., 2015). Response options included yes, no, or unsure, and were recoded into a dichotomous variable (yes or no). Responses of “unsure” to suicidal ideation (n = 23) and suicide attempts (n = 11) were recoded as “yes” to account for under-reporting of suicidal ideation and attempts in the population (Klonsky, May, & Saffer, 2016; Prinstein, 2008).
Perceived gentrification-related neighborhood connectedness and compositional change
The Neighborhood Change and Gentrification Scale (NCGS) is comprised of two sub-scales assessing perceived neighborhood connectedness and neighborhood compositional change in relation to recent gentrification-related neighborhood changes (DeVylder, Fedina, & Jun, in press). The NCGS uses a 5-point Likert-type scale and asks respondents to indicate their level of agreement with statements regarding recent changes to their neighborhood in the past several years (1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree). The neighborhood connectedness subscale is comprised of six items assessing recent changes related to one’s feelings of recent disconnectedness with their neighborhood: (a) I have felt increasingly “out of place” in my neighborhood, (b) I have seen a disruption of local community ties and social networks, (c) I have feared being “pushed out” of my neighborhood, (d), I have experienced or heard of others being harassed by their landlords to vacate an apartment, (e), I worry about feeling “unwelcome” in my neighborhood, and (f) I have observed changes to the sense of “community” in the neighborhood. Higher scores indicate higher levels of neighborhood disconnectedness. The neighborhood compositional change subscale is comprised of four items assessing recent changes in neighborhood composition related to affluence/resources, crime, residential mobility, and infrastructure: (a) I have experienced improved access to neighborhood amenities and city services, (b) Crime has decreased in my neighborhood, (c) I have seen an influx of affluent or nonminority residents moving into the neighborhood, and (d) I have observed a lot of renovation activity in the neighborhood. Higher scores indicate higher levels of neighborhood compositional change. Internal consistency and reliability of the neighborhood connectedness and compositional change subscales in this sample was acceptable (α = .83, .64, respectively).
Loneliness
The three-Item Loneliness Scale, which was adapted from the Revised University of California Los Angeles (R-UCLA) Loneliness Scale, was used to assess loneliness (Hughes, Waite, Hawkley, & Cacioppo, 2004). Items include (a) “how often do you feel that you lack companionship?” (b) “how often do you feel left out?” and (c) “how often do you feel isolated from others?” with a 3-point Likert-type scale (1 = hardly ever, 2 = some of the time, 3 = often). Items were summed and averaged, where higher scores indicate greater levels of loneliness (range = 1-3). Internal consistency and reliability in this sample was acceptable (α = .84).
IPV
IPV was assessed with 15 dichotomous items (yes/no) from the National Intimate Partner and Sexual Violence Survey (NISVS) measuring lifetime physical, sexual, and psychological violence by a romantic or sexual partner (Centers for Disease Control and Prevention, NISVS General Population Survey Raw Data). Internal consistency and reliability of the measure was excellent in this sample (α = .94). Each IPV indicator was summed into a single continuous variable ranging from 0 (no exposure) to 15 (exposure to all).
Sociodemographic factors
Sociodemographic control variables included age, race/ethnicity (non-Hispanic/Latino White, non-Hispanic/Latino Black or African American, Hispanic/Latino, and non-Hispanic/Latino Other [i.e., Asian American, American Indian/Alaska Native, or Native Hawaiian]), gender (male, female, or transgender), sexual orientation (lesbian/gay/bisexual or heterosexual), annual household income (in US$20,000 increments, up to US$100,000+), and education level (<high school, high school diploma or general equivalency diploma [GED], some college or technical school, college graduate, graduate or professional degree).
Data Analyses
Pearson correlations and t tests were used to assess bivariate relationships between IPV and main study variables, including mental health outcomes (i.e., psychological distress, past-year suicidal ideation, past-year suicide attempts) and perceived neighborhood factors (i.e., neighborhood disconnectedness, neighborhood compositional change). Ordinary least squares (OLS) and binary logistic regression analyses were used to model associations between IPV, neighborhood disconnectedness, neighborhood compositional change, and each mental health variable (i.e., psychological distress, suicidal ideation, suicide attempts), adjusting for sociodemographic factors and loneliness. Interaction terms were created and entered into the models to test moderation effects of neighborhood connectedness, neighborhood compositional change, and loneliness on IPV for each mental health outcome, controlling for other variables in the models. No missing cases were found for study variables due to the use of forced choice responding during survey administration. All analyses were tested at a significance level of .05 (α = .05, two-tailed) using Stata Version 13.1 (StataCorp, 2016).
Results
Sample Description
Descriptive statistics for study participants are presented in Table 1. The majority of participants were female (60.6%), non-Hispanic/non-Latino Black (39.0%), heterosexual (90.3%), and between the ages of 25 and 44 (47.4%) (M = 37.79, SD = 15.18, range = 18-95). A total of 49% of participants reported any lifetime exposure to physical, sexual, and/or psychological IPV. The range of IPV exposure in the study sample was 0 to 15, with an average exposure to approximately two IPV behaviors (M = 2.75, SD = 3.97).
Description of Sample Sociodemographic Characteristics and Main Study Variables (N = 1,000).
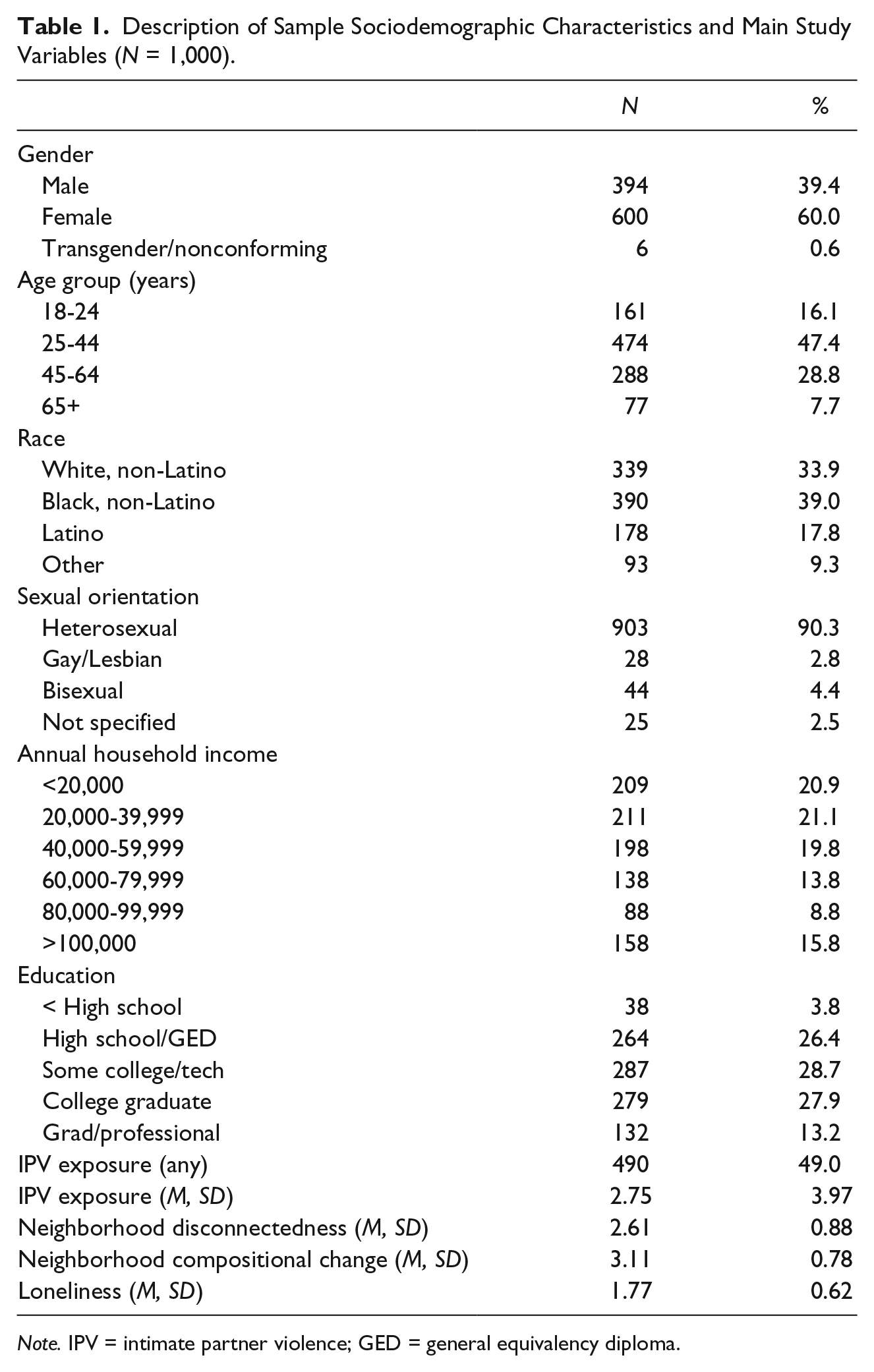
Note. IPV = intimate partner violence; GED = general equivalency diploma.
Correlations Between IPV and Main Study Variables
IPV exposure was positively correlated with psychological distress (r = .34, p < .001) and loneliness (r = .23, p < .001) at the bivariate level. Individuals with past-year suicidal ideation and attempts reported higher levels of IPV exposure (M = 6.13, SD = 4.66; M = 8.42, SD = 4.91, respectively) compared with those without past-year suicidal ideation and attempts (M = 2.41, SD = 3.73; M = 2.57, SD = 3.80, respectively) (t = −8.86, p < .001, t = −8.36, p < .001, respectively). IPV exposure was positively correlated with neighborhood disconnectedness (r = .15, p < .001) and negatively correlated with neighborhood compositional change (r = −.12, p < .001); that is, greater levels of IPV exposure were correlated with greater levels of neighborhood disconnectedness, and lower levels of IPV exposure were correlated with higher levels of neighborhood compositional change.
Multivariate Associations Between IPV and Mental Health Symptoms
Multivariate associations are presented for each model in Table 2. Regression analyses suggest a significant relationship between IPV and psychological distress (B = .33, p < .001, 95% confidence interval [CI] = [0.24, .41]), suicidal ideation (odds ratio [OR] = 1.15, p < .001, 95% CI = [1.10, 1.21]), and suicidal attempts (OR = 1.30, p < .001, 95% CI = [1.20, 1.41]), after accounting for sociodemographic factors, loneliness, neighborhood disconnectedness, and neighborhood compositional change in each model. In addition, higher levels of neighborhood disconnectedness (B = .82, p < .001, 95% CI = [0.43, 1.20]) and loneliness (B = 3.07, p < .001, 95% CI = [2.53, 3.62]) were significantly associated with increased psychological distress symptoms. Neighborhood compositional change was not significantly associated with psychological distress, after accounting for other variables in this model. In the model predicting suicidal ideation, loneliness was significantly associated with increased odds of suicidal ideation (OR = 2.87, p < .001, 95% CI = [1.90, 4.34]); however, neighborhood disconnectedness and compositional change were not significant in this model. Finally, in the model predicting suicide attempts, neighborhood compositional change was significantly associated with increased odds for suicide attempts (OR = 2.18, p < .01, 95% CI = [1.27, 3.74]). Neighborhood disconnectedness and loneliness were not associated with suicide attempts, after controlling for other variables in the model.
Multivariate Models for Perceived Neighborhood Factors, Loneliness, and IPV Predicting Mental Health Symptoms (N = 1,000).
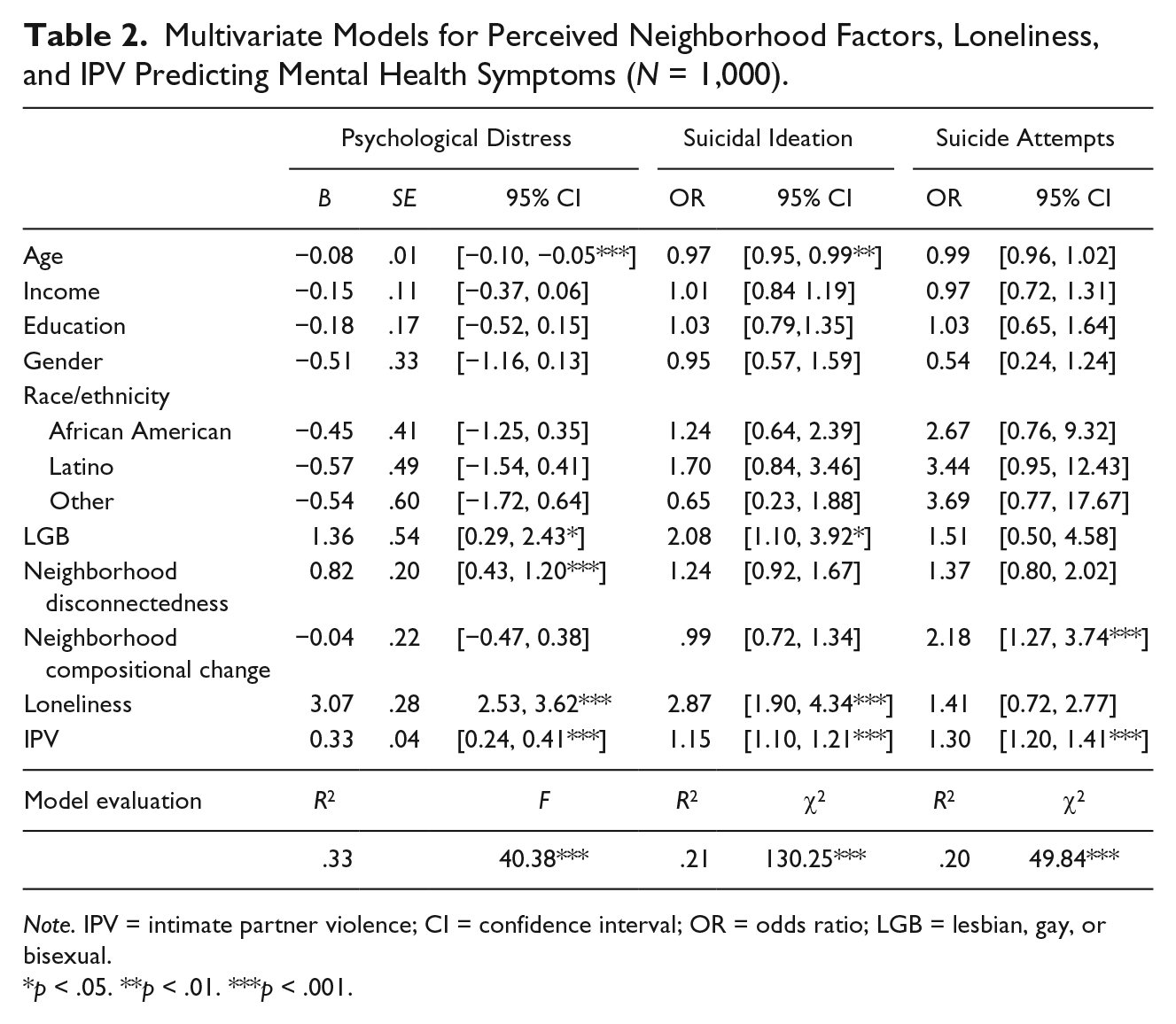
Note. IPV = intimate partner violence; CI = confidence interval; OR = odds ratio; LGB = lesbian, gay, or bisexual.
p < .05. **p < .01. ***p < .001.
Moderation Effects of Neighborhood Disconnectedness, Neighborhood Compositional Change, and Loneliness
Regression results suggest several significant interaction effects of perceived neighborhood characteristics on IPV and mental health symptoms, as presented in Figure 1. Neighborhood disconnectedness (B = .13, p < .01, 95% CI = [0.04, 0.22]) and neighborhood compositional change (B = .11, p < .05, 95% CI = [0.02, 0.20]) significantly moderated the relationship between IPV and psychological distress. Results indicate that the higher the level of neighborhood disconnectedness and neighborhood compositional change, the greater the effect of IPV on psychological distress (Figure 1a and 1b). Loneliness did not moderate the relationship between IPV and psychological distress. In the model predicting suicidal ideation, loneliness (OR = 0.85, p < .001, 95% CI = [0.78, 0.92]) and neighborhood compositional change (OR = 1.10, p < .01, 95% CI = [1.04, 1.17]) significantly moderated the relationship between IPV and suicidal ideation (Figure 1c and 1d). Results suggest that the higher the level of neighborhood compositional change, the greater the effect of IPV on suicidal ideation. However, interaction effects suggest that the higher the level of loneliness, the weaker the effect of IPV on suicidal ideation. Neighborhood disconnectedness did not moderate the relationship between IPV and suicidal ideation. In the model predicting suicide attempts, loneliness significantly moderated the relationship between IPV and suicide attempts (B = .88, p < .05, 95% CI = [0.78, 1.01]), where the higher the level of loneliness, the weaker the effect of IPV on suicidal attempts. Neighborhood disconnectedness and compositional change did not moderate the relationship between IPV and suicide attempts.
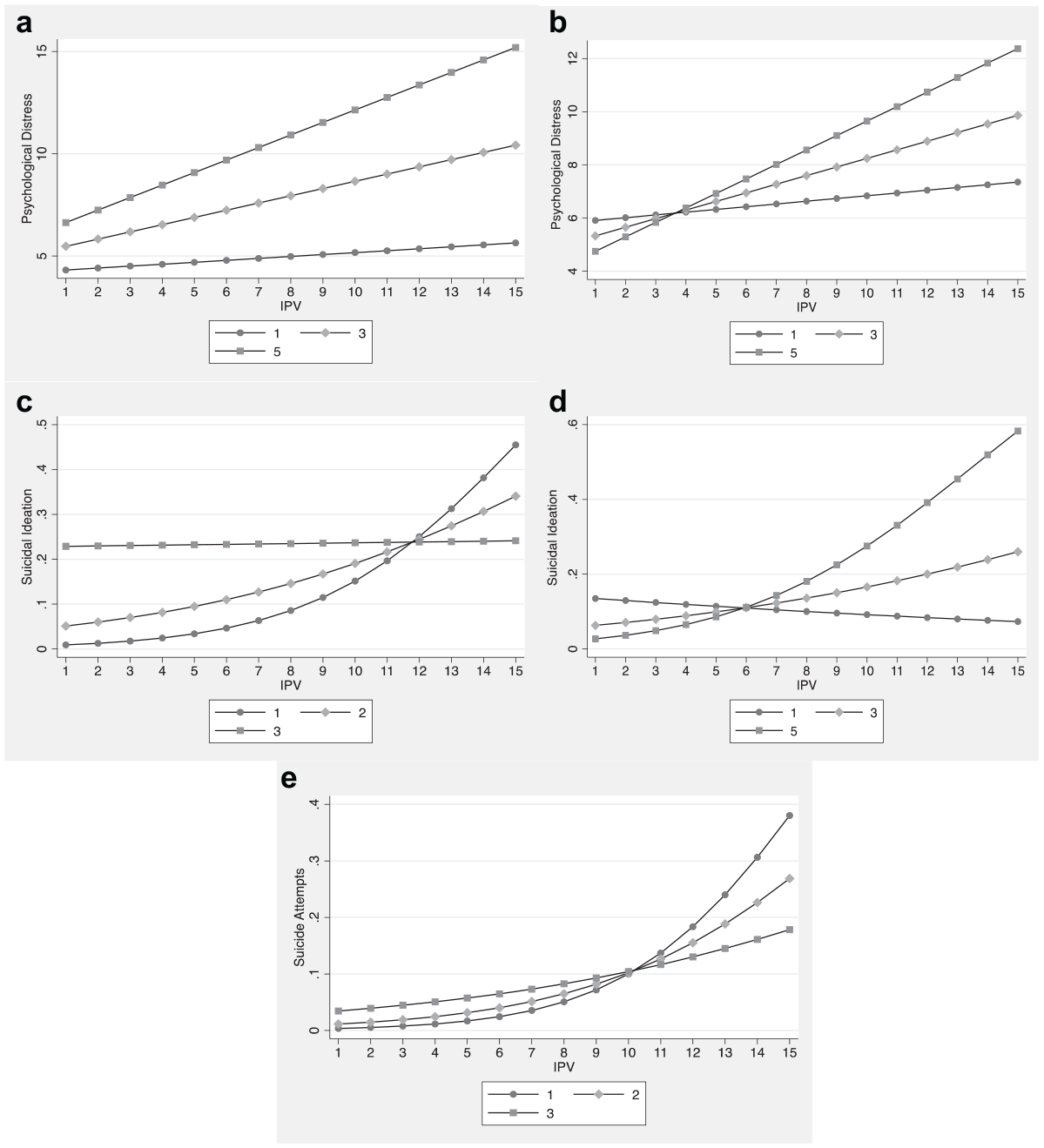
Significant interaction effects of (a) perceived neighborhood disconnectedness on IPV and psychological distress, (b) perceived neighborhood compositional change on IPV and psychological distress, (c) loneliness on IPV and suicidal ideation, (d) perceived neighborhood compositional change on IPV and suicidal ideation, and (e) loneliness on IPV and suicide attempts.
Discussion
This study examined the relationship between perceptions of gentrification-related neighborhood factors (i.e., neighborhood connectedness and neighborhood compositional change) and past histories of IPV, including the moderating role of these factors on IPV exposure and associated current mental health symptoms in a general population sample of urban U.S. male and female adults. This study demonstrates that neighborhood connectedness and neighborhood compositional change are broadly associated with past IPV exposure and current mental health of participants exposed to IPV, which have important implications for public health interventions aimed at disentangling the relationships between IPV, neighborhood factors, and adverse mental health outcomes. Findings from this study are consistent with emerging research broadly linking perceptions of neighborhood factors (e.g., neighborhood connectedness and stability) and IPV (Beyer et al., 2015). Our study extends knowledge in this area by investigating associations between IPV exposure and gentrification-specific perceptions of neighborhood disconnectedness and recent compositional change, suggesting that these factors worsen the effects of psychological distress and suicide risk among individuals exposed to IPV.
We hypothesized that neighborhood disconnectedness and neighborhood compositional change would moderate and worsen psychological distress symptoms, suicidal ideation, and suicide attempts among individuals exposed to IPV based on prior literature identifying strong links between perceived neighborhood factors (i.e., collective efficacy, social ties, stability) and the mental health of urban residents in the general population (Beyer et al., 2015; Steinmetz-Wood et al., 2017). This hypothesis was partially supported in this study. Both neighborhood disconnectedness and compositional change moderated the relationship between IPV and psychological distress, and neighborhood compositional change moderated the relationship between IPV and suicidal ideation. These findings suggest that at minimum, neighborhood disconnectedness and neighborhood compositional change worsens psychological distress symptoms and increases suicide risk (ideation), and that this relationship is even more pronounced for IPV victims. This implies that violence prevention approaches should consider the ways in which neighborhood change and instability, including residents’ sense of neighborhood connectedness, impacts IPV and subsequent mental health outcomes. In addition, community mental health interventions should be cognizant of the broad effects of neighborhood connectedness and compositional changes on mental health and that these factors may have particular implications for the safety and mental health of IPV victims.
This study also explored moderating effects of loneliness (the antithesis of social support) on mental health symptoms associated with IPV based on prior research (Hawkley & Cacioppo, 2010). We found that loneliness significantly moderated the relationship between IPV and suicidal ideation and suicide attempts; however, the nature of these interaction effects were somewhat unexpected. IPV and suicide were more strongly related for individuals experiencing low levels of loneliness, opposed to high levels of loneliness. These findings suggest that loneliness may be an important factor contributing to elevated suicide risk for urban residents in the general population; however, it may not be an especially salient risk factor for individuals with IPV histories. Individuals exposed to IPV had significantly higher odds of suicidal ideation and suicide attempts compared with individuals without IPV exposure, which is consistent with prior studies (Cronholm et al., 2011; Leiner et al., 2008; McLaughlin et al., 2008). However, additional factors, apart from social isolation or loneliness, may lead to elevated suicide risk among IPV victims, including neighborhood disconnectedness and compositional change, which was the case in this study’s findings. Individuals with IPV histories living in urban areas with high levels of neighborhood disconnectedness and rapid compositional change may face greater levels of distress, economic insecurity, weakened social ties, and risk for displacement, which may ultimately lead to increased risk for suicide.
We also explored the relationship between IPV and gentrification-related factors. Higher levels of IPV exposure were associated with higher levels of neighborhood disconnectedness, whereas lower levels of IPV were associated with higher levels of neighborhood compositional change. The positive relationship found between IPV and neighborhood disconnectedness may be explained by diminished collective efficacy and connectedness resulting from neighborhood changes due to gentrification, as well as socioeconomic disadvantage in neighborhoods where neighborhood disruption, as a consequence of gentrification, is more likely to be prevalent. In addition, the inverse relationship found between IPV and neighborhood compositional change may be explained by the benefits or positive neighborhood changes stemming from gentrification (e.g., decreased crime, increased affluence, greater investment in local amenities and services), where residents living in less gentrified areas continue to experience high crime, disinvestment, and limited amenities and services and, consequently, higher levels of IPV. Further investigation using prospective designs is needed to understand the mechanisms linking IPV to gentrification-related neighborhood change and disconnectedness, such as resident displacement and accessibility to services and amenities in gentrified neighborhoods (Freeman, 2005; Lim et al., 2017; Sullivan, 2014).
There are several limitations to be considered in the current study. First, survey data are limited in its cross-sectional design. Therefore, causality and temporal relationships between IPV exposure (which was measured as lifetime exposure in this study) and perceptions of neighborhood factors cannot be determined. Future studies should use prospective designs that can adequately assess whether perceived neighborhood factors, including connectedness and change, are predictive of future exposure to IPV. In addition, survey data were collected from Baltimore and New York City, which may not be generalizable to populations living in other U.S. cities. The study sample was limited to English-speaking participants, and thus, findings are not generalizable to non-English speaking populations. Relatedly, due to very small sample sizes of transgender/gender nonconforming participants, we were unable to adequately assess the effects of gender identity on outcome variables of interest. Challenges in achieving sampling quotas were encountered in the data collection process, resulting in oversampling of some populations (i.e., females in New York City and younger respondents in Baltimore). Finally, although this is one of the first studies to explore residents’ perceptions of neighborhood factors as they relate to IPV and mental health, no additional neighborhood data sources or measures (e.g., resident mobility, evictions, housing costs) were included in the analysis. Future studies should combine assessments of residents’ perceptions of neighborhood factors with other data sources to more fully capture the dynamic processes involving IPV, mental health symptoms, and neighborhood gentrification-related connectedness and change.
Despite these limitations, the current study addresses important gaps in research on perceived neighborhood factors related to neighborhood connectedness and neighborhood change and its relationship to IPV and mental health, in a large, diverse sample of both males and females. Findings from this study suggest that neighborhood disconnectedness and compositional change may worsen psychological distress symptoms and suicide risk most strongly among individuals exposed to IPV. Violence prevention and intervention approaches should consider the extent to which neighborhood instability, related to community connectedness and recent compositional change, impacts the safety and mental health of victims of IPV. Therefore, IPV and its adverse mental health symptoms should not be considered solely as a function of individual characteristics given that this study’s findings suggest that mental health outcomes are influenced by neighborhood factors related to connectedness and compositional change. This knowledge can inform future practice, policy, and research to consider the role of gentrification-related neighborhood connectedness and compositional change in both the etiology of IPV and preventing its health and mental health consequences.
Community-based programs aimed at both preventing violence and enhancing neighborhood social support, connectedness, and collective efficacy through economic, health, and mental health support services can mitigate the development of adverse mental health symptoms associated with IPV exposure. For example, several urban cities in the United States have implemented mixed-income housing demonstration projects that deliver an array of economic, health, and social support services aimed at preventing violence; however, low levels of neighborhood connectedness, trust, and collective efficacy may prevent families from utilizing these needed services (Hailey & Saxena, 2013). As such, these and other similar public health models focused on neighborhood health and violence prevention should include programs and activities that promote connectedness and trust among residents, which may protect against the development of adverse mental health symptoms due to IPV. Although future research is needed on their effectiveness, antidisplacement policies to counter the negative impacts of gentrification on neighborhood cohesion and connectedness can enhance and maintain social bonds and trust among residents (Rigolon & Németh, 2019). The effects of such policies may extend to the prevention of mental health risks commonly associated with IPV.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by internal funding from the University of Maryland School of Social Work, through the Competitive and Innovative Research (CIR) Award to DeVylder, Post-Doctoral Fellowship to Jun and Graduate Research Assistantship to Fedina.