
Abstract
It is widely known that sexual assault disproportionately affects women, and college-aged women are particularly at risk. Sexual assault can occur at any age and may have a varying range of emotional consequences for survivors, including pathological coping mechanisms such as disordered eating behaviors. This study examined the mediating effect of resilience on the relationship between posttraumatic stress disorder (PTSD) symptoms and disordered eating behavior in a sample of women who reported experiencing sexual assault in adulthood. The sample included 312 undergraduate women who identified as majority White (81.4%) and heterosexual (77.9%). Participants completed measures assessing history of sexual experiences, PTSD symptoms, disordered eating behavior, and resilience. Only those who reported experiences of sexual victimization since age 14+ were included in analyses. Results confirmed the hypothesis, as resilience significantly mediated the relationship between PTSD symptoms and disordered eating behavior in a sample of women with a history of sexual victimization. These results highlight the importance of resilience as a mitigating factor in recovery from sexual trauma. Other research indicates that resilience may have emotion-regulatory benefits that mitigate the development of disordered eating behavior. However, the specific functionality of resilience as a protective factor after sexual victimization is unclear. Further research should focus on ways to foster resilience in a clinical setting for those with a history of sexual victimization. Limitations of this study include underrepresentation of racial and ethnic minorities, as well as use of entirely self-report measures.
Approximately 44% of women report unwanted sexual experiences in their lifetime (Breiding et al., 2014), and the occurrence of sexual assault among college-aged women is especially high compared with women of other ages (Bureau of Justice Statistics, 2014). The consequences of sexual assault are numerous, but posttraumatic stress disorder (PTSD) is among the most pervasive psychopathologies experienced by survivors (Dworkin et al., 2017). Existing research indicates that sexual assault survivors may be more likely to develop PTSD symptoms than are survivors of other types of assault (Foa & Riggs, 1995; Faravelli et al., 2004). In addition, disordered eating (DE) has been found to commonly co-occur with PTSD symptoms in women who have experienced sexual trauma (Dubosc et al., 2012; Holzer et al., 2008). However, little is known about what factors may influence the relation between PTSD symptoms and DE. There is a paucity of research on the role of resilience in the relationship between PTSD symptoms and DE behaviors in women who have experienced sexual trauma. The aim of this study was to examine how PTSD symptoms and resilience associate with DE behaviors in a sample of undergraduate women.
Sexual Trauma Definitions and Operationalization
Sexual assault is classified as “sexual contact or behavior that occurs without explicit consent of the victim” (Rape, Abuse & Incest National Network [RAINN], n.d.); therefore, not all sexual assault qualifies as rape. Rape is legally defined as “The penetration, no matter how slight, of the vagina or anus with any body part or object, or oral penetration by a sex organ of another person, without the consent of the victim” (U.S. Department of Justice, 2012). For the purposes of this study, the terms sexual assault and sexual victimization will be used interchangeably to broadly refer to any physical assault for which the purpose was to obtain a sexual act, which may or may not include penetration (i.e., rape).
Sexual Trauma and PTSD
According to the National Intimate Partner and Sexual Violence Survey, 19.3% of women have been raped during their lifetime, and 43.9% of women have had some other form of unwanted sexual experience, such as sexual coercion or unwanted sexual touching (Breiding et al., 2014). College-age women (18–24 years) experience sexual assault at rates three to four times greater than women of other ages (Bureau of Justice Statistics, 2014). The risk imposed upon college-age women is further heightened considering that sexual assault is a notorious risk factor for numerous psychopathologies, such as substance use disorder, PTSD, and eating and mood disorders (Dworkin et al., 2017; Faravelli et al., 2004). A recent meta-analysis of psychopathology following sexual assault included 204 studies from 1970 to 2014 in which one or more psychopathologies with onset following sexual assault were examined (Dworkin et al., 2017). Trauma- and stressor-related conditions, such as PTSD, were among the most common psychopathologies to occur in survivors post-assault with an effect size of g = .71 (p < .01) (Dworkin et al., 2017). Results also suggested that PTSD may have a uniquely pervasive relationship with sexual victimization (Dworkin et al., 2017). Additional research supports this notion; for example, Foa and Riggs (1995) found that survivors of rape demonstrated more pervasive and persistent PTSD symptoms compared with a sample of nonsexual assault survivors. Approximately 16% to 30% more participants in the sexual assault group met criteria for PTSD than did the nonsexual assault group at each time point (Foa and Riggs, 1995). Although the sample utilized in this study was unique in that all participants had reported their assaults to the police, findings consistently support that survivors of sexual assault may be more likely to develop PTSD symptoms compared with survivors of other types of assault (Faravelli et al., 2004; Frazier et al., 2009).
Frazier and colleagues (2009) found PTSD symptoms to be most probable and prevalent among survivors of sexual assault compared with survivors of nonsexual assaults in a study of psychological impact of lifetime trauma in a college sample. In this study, participants were asked to rate their worst potentially traumatic life events at two time-points (T1 and T2) across a 2-month period during college. Of those who nominated sexual assaults their worst event at T1 (n = 87), 13% had probable PTSD, which was two to six times greater than the rate of probable PTSD compared with other top-ranking worst events (e.g., unexpected death of a loved one, accident, other’s life threat, unwanted sexual attention, and family violence; Frazier et al., 2009). Of those who reported experiencing sexual assault between T1 and T2 who also nominated sexual assault as their worst event in that time period (n = 7), 43% had probable PTSD. Although this rate was in stark contrast to probable PTSD rates for other top-ranking worst events that ranged from 0% to 13%, other worst events had notably larger occurrence between T1 and T2 (Frazier et al., 2009). Each of the described studies demonstrates a higher prevalence of PTSD symptomology compared with other types of trauma, including other physical traumas. However, the body of literature offering explanation for why PTSD and sexual victimization appear to have a uniquely pervasive relationship is lacking.
Sexual Assault and DE
The transdiagnostic nature of emotion regulation difficulties in eating disorder diagnoses lends DE behavior as a maladaptive emotion-regulatory mechanism; this offers a possible explanation for DE behavior as a likely comorbid psychopathology with PTSD following sexual assault. For example, Holzer and colleagues (2008) found significant relationships between trauma history and PTSD, trauma history and DE behavior, as well as PTSD symptoms significantly mediating the relationship between sexual victimization history and DE behavior. Furthermore, Holzer et al. (2008) found full mediation of specific PTSD symptoms; for example, arousal symptoms significantly mediated the relationship between sexual victimization and DE behavior. Comparable results were yielded when including avoidance in the statistical model, revealing avoidance as a mediator in the relationship between trauma and DE behavior (Holzer et al., 2008). Holzer et al. (2008) posit that those who experience PTSD with particularly high arousal and/or with significant social avoidance may be at higher risk of developing an eating disorder as a mechanism by which they can regulate and/or avoid negative affect. In light of the association between sexual victimization and PTSD, as well as the associations between PTSD symptoms and DE behavior, DE behavior in a sexually victimized sample is warranted.
The association of childhood sexual abuse and DE has been empirically established (e.g., Sanci et al., 2008). Given that first victimization is a strong predictor of revictimization (e.g., Haskell, 1999), one might expect that history of childhood sexual abuse in survivors of multiple instances of abuse would conflate the association between sexual abuse and DE in adult samples; however, several studies have demonstrated that this is not necessarily so. For example, in one study, a matched sample of women with no history of childhood sexual abuse who were survivors of rape, as decided by a court of law, in the 4 to 9 months preceding the study (n = 40), was compared with a control group of women who had experienced life-threatening, nonsexual violence (n = 32; Faravelli et al., 2004). Results showed that women who experienced adult sexual violence displayed greater PTSD symptoms and DE symptoms than the control group (Faravelli et al., 2004). The significant difference between presentation of PTSD and DE symptoms between the sexual assault group and the nonsexual assault group support the idea that sexual assault is a particularly pervasive risk factor for PTSD and DE. Moreover, by excluding survivors of childhood sexual abuse, the results demonstrate that adult sexual victimization is linked to significant DE symptomology.
In addition, another study controlled for childhood abuse in DE outcomes of female survivors of adult sexual assault and found that (a) childhood emotional abuse was the only significant predictor of present eating disorder symptoms when controlling for childhood sexual and physical abuse and (2) sexual assault in adulthood was significantly related to DE, even when controlling for childhood emotional abuse (Fischer et al., 2010). By controlling for childhood abuse, these studies established that psychopathological response to adult sexual assault is distinct from residual psychological difficulty from negative childhood abuse. The unique association of sexual violence and increased DE behavior remains robust across age of victimization (e.g., Ackard & Neumark-Sztainer, 2002; Faravelli et al., 2004; Sanci et al., 2008), and this association significantly differs from that of nonsexual violence and DE (Faravelli et al., 2004). Nonetheless, it remains to be understood why some survivors of sexual abuse develop DE and others do not. There are many factors that may moderate individual outcomes following sexual abuse, for example, resilience to adversity.
Resilience to Trauma
Although resilience can be defined in many ways, the present study conceptualized it in terms of Smith and colleagues’ (2008) definition—that resilience is the ability to bounce back or recover from stress. This theory of resilience posits that personality characteristics that may aid one in recovering from adversity are resilience resources, rather than an assessment of resilience itself. Smith et al. (2008) emphasize that concepts such as maintenance of equilibrium or functioning in spite of adversity should not be conflated with resilience itself (i.e., a return to normal functioning after stress). This definition of resilience is pertinent to researching the relationship among traumatic events and posttrauma psychopathologies because individuals’ response to trauma varies greatly. Understanding resilience as one’s ability to bounce back or recover from stress provides a simple framework from which to assess differences in response to trauma as it is related to resilience.
Existing research supports that resilience plays an important role in the relationship between trauma and later psychopathology. In a study of predominantly low income, African American adults who experienced trauma, both childhood abuse and other trauma influenced depression severity as expected and that resilience significantly moderated this relationship (Wingo et al., 2010). A study of affective recovery from anticipated threats showed that resilient people are capable of inhibiting negative affect, which researchers suppose might protect from rumination on negative feelings (Waugh et al., 2008). One study demonstrated resilience as a protective factor against fear-potentiated depressive symptoms following nonsexual trauma (Zhou et al., 2016). Bonanno and colleagues (2007) indicated that highly resilient people may experience healthier adjustment in the aftermath of disaster than do less resilient people.
These studies indicate that resilience may mitigate the negative impact of trauma. However, few studies have investigated the relationship of sexual trauma, psychopathology, and resilience. Given the empirical links among sexual victimization and PTSD, as well as PTSD and DE behavior, sexual victimization and DE behavior may be linked via pathway of trauma. Because resilience has been demonstrated to alter relationships between trauma and other psychopathology (e.g., Bonanno et al., 2007; Waugh et al., 2008; Wingo et al., 2010; Zhou et al., 2016), resilience may alter the pathway between PTSD symptoms due to sexual victimization and DE behavior.
The Current Study
Given the prevalence of sexual victimization among college-age women (RAINN, n.d.), the relationship between sexual victimization and PTSD symptoms (Foa & Riggs, 1995), the comorbidity of PTSD symptoms and DE behavior (Faravelli et al., 2004), as well as the protective role of resilience (e.g., Bonanno et al., 2007), empirical examination of these constructs in conjunction with each other is warranted. If resilience significantly influences the effect of PTSD symptoms related to sexual victimization on DE behaviors, then resilience could have clinical implications, such as development of resilience-informed trauma care. The current study hypothesized that resilience would mediate the relationship between PTSD symptoms and DE behavior in a sample of undergraduate women who reported experiences of sexual victimization in adulthood
Method
Participants
Eight hundred twelve undergraduate students identifying as women completed a survey and were screened for inclusion in this study. To be included, participants must have been between 18 and 25 years of age and have reported at least once experience of sexual assault or rape since the age of 14. Overall, 336 participants reported having at least one experience of completed or attempted sexual assault or rape in adulthood (ages 14+). These age ranges were determined based on the results of a study that found that experiences of sexual victimization in adolescence (ages 14–17) were more characteristically and contextually similar to those of adulthood (ages 18+) than to those of childhood (Livingston et al., 2007). Participants who reported experiences of sexual assault or rape that occurred exclusively in childhood (n = 24) did not meet inclusion criteria for the study and were not included in the selected sample. In addition, participants who reported experiences of sexual coercion, but not experiences of attempted or completed sexual assault or rape, were not included in the selected sample.
The selected sample included 336 undergraduate women recruited from a mid-sized university in the southcentral United States with an average age of 19.3 years (SD = 1.6). The majority of participants identified as heterosexual (77.9%) and White (81.4%). The remaining participants identified as bisexual (15.7%), homosexual (2.2%), or Other (3.2%), as well as Black/African American (9.9%), multi-ethnic (2.9%), Hispanic/Latinx (3.5%), Asian (1.6%), or Other (0.6%). T-test and chi-square analyses demonstrated no significant difference in mean age (t = −1.89, p > .05) or ethnicity, χ2(5) = 3.12, p > .05, among those included versus excluded from the study sample. Chi-square analysis indicated a significant difference in sexual orientation, χ2(794) = 27.4, p < .001, such that the included group had a slightly lower representation of heterosexual individuals and a greater representation of bisexual individuals than the excluded group (see Table 1).
Mean Scores, Standard Deviations, and Coefficient Alphas for Quantitative Measures.
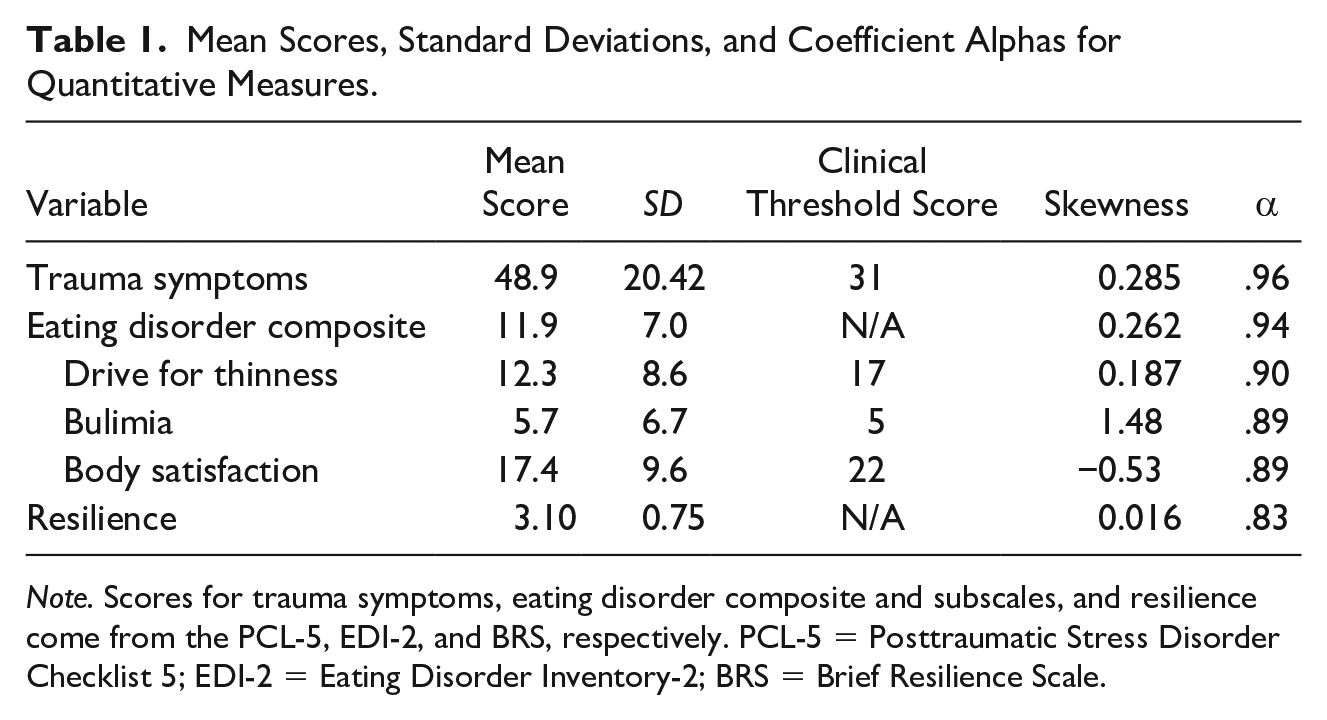
Note. Scores for trauma symptoms, eating disorder composite and subscales, and resilience come from the PCL-5, EDI-2, and BRS, respectively. PCL-5 = Posttraumatic Stress Disorder Checklist 5; EDI-2 = Eating Disorder Inventory-2; BRS = Brief Resilience Scale.
Procedures
The university Institutional Review Board reviewed ethical and methodological concerns and granted approval for this study. Respondents were recruited via an online university study board and completed an online self-report survey. The survey was posted to the university’s Study Board site, and students enrolled in psychology or psychological sciences courses received class credit for their participation. In addition, linked access to the survey was distributed via email list-servs for both the university Gender & Women’s Studies department and the university Panhellenic sorority list-serv. The recruitment email informed respondents that they would be asked to participate in a 20-minute survey regarding women’s health, mental health, and risk behaviors. After following the attached link, participants read the informed consent document which explicitly stated that they would be asked questions regarding their trauma history, eating behaviors, and resilience.
Participants completed online informed consent documents prior to beginning the survey and reviewed an online debriefing document following conclusion of the survey. The debriefing page included phone numbers and web-links to the university counseling center, Texting Crisis Support Line, National Suicide Prevention Lifeline, a local sexual trauma recovery center, and RAINN National Sexual Assault Hotline.
Anonymity was maintained by assigning computer-generated random identification numbers to each participants’ responses. In addition, the survey included skip-logic that presented pop-up boxes with the crisis hotline number for the local sexual trauma recovery center and a link to RAINN webchat for participants who reported a history of sexual assault.
Measures
Sexual Experiences Survey
Koss and Oros’ (1982) Sexual Experiences Survey (SES) is a 13-item qualitative assessment of participants’ experiences with various forms of sexual assault and harassment, including coercion, attempted assault and rape, and completed assault and rape. An empirical review of the SES found acceptable internal consistency (α = .74) and good test–retest reliability (r = .73) in female participants’ responses to a self-report measure and a researcher-administered interview (Koss & Gidycz, 1985).
In this measure, coercive experiences, such as circumstances in which the aggressor used verbal or emotional manipulation to coerce the victim to give consent to any type of sexual act, were assessed in questions such as “Have you ever found out that someone had obtained sexual intercourse with you by saying things they didn’t really mean?” and “Have you ever had sexual intercourse with someone when you didn’t really want to because you felt pressured by their continual arguments?” (Koss & Oros, 1982). Attempted sexual assault and rape were assessed via questions such “Have you ever been in a situation where someone tried to get sexual intercourse with you when you didn’t want to by threatening to use physical force (twisting your arm, holding you down, etc.) if you didn’t cooperate, but for various reasons sexual intercourse did not occur?” (Koss & Oros, 1982).
Next, assessment of completed sexual assault and rape was measured in questions such as “Have you ever been in a situation where someone used some degree of physical force (twisting your arm, holding you down, etc.) to try to make you engage in kissing or petting when you didn’t want to?” and “Have you ever had sexual intercourse with someone when you didn’t want to because they used some degree of physical force?” (Koss & Oros, 1982). Although the previous question alluded to the legal definition of rape without using the word rape, the survey concluded with the question, “Have you ever been raped?” (Koss & Oros, 1982). For each question to which a participant answered yes, skip-logic ensued with the follow-up questions: “How many times?” and “How old were you?” (Koss & Oros, 1982).
The SES included 13 questions that warranted dichotomous yes and no responses (yes = 1, no = 0). In the event of a yes response, the follow-up response for number of occasions remained a numeric response. The follow-up response for age was qualified into one of three categories: childhood (ages 1–13), adulthood (ages 14+), and both (multiple occasions across lifespan).
Posttraumatic Stress Disorder Checklist 5 (PCL-5)
The PCL-5 (American Psychiatric Association, 2013), was used to assess participants’ present PTSD symptoms (Weathers et al., 2013). Validity studies of this measure revealed high internal consistency (a = .94) and high test–retest reliability (r = .82) (Blevins et al., 2015). Reliability analysis from the present study showed Cronbach’s alpha of .96 (see Table 1). The PCL-5 includes 20 items that ask participants to report how much they are bothered, in the previous month, by symptoms such as “Repeated, disturbing, and unwanted memories of the stressful experience,” “Feeling very upset when something reminds [them] of the stressful experience,” and “Trouble remembering important parts of the stressful experience” (Weathers et al., 2013). Participants report how much they are bothered on a 5-point Likert-type scale from 0 = not at all to 4 = extremely. Responses for each are coded accordingly and summed to create composite scores, composed of subscales for each of the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) criteria categories for PTSD, that reflect degree of PTSD symptoms experienced. However, it does not provide conclusive diagnostic information. Total scores from the PCL-5 were used in the current study as a measure of overall PTSD symptoms.
Brief Resilience Scale (BRS)
The BRS is a six-item assessment of participants’ perceived ability to recover from adversity (Smith et al., 2008). An evaluation of this measure found good test–retest reliability in two samples of participants who were given the BRS twice, revealing in intraclass correlation of .69 for one group and .62 for the other (Smith et al., 2008). The same evaluation also found high internal validity with Cronbach’s alpha ranging from .80 to .91 among four samples of participants (Smith et al., 2008). Reliability analysis from the present study revealed Cronbach’s alpha of .83 (see Table 1). Respondents reported their level of endorsement for six statements about their personal resilience on a Likert-type scale of five possible responses, ranging from strongly disagree to strongly agree, to statements such as “I tend to bounce back quickly after hard times” and “I have a hard time making it through stressful events” (Smith et al., 2008). Responses to the six-item questionnaire were scored on a 1 to 5 scale, with responses indicating lowest resilience scoring 1, and responses indicating highest resilience scoring 5. Mean scores are calculated and higher scores indicate greater resilience.
Eating Disorder Inventory-2 (EDI-2)
The EDI-2 assessed participants’ DE behaviors using the subscales of drive for thinness, bulimic behavior, and body dissatisfaction, which comprise the eating disorder composite score (Garner, 1991). An empirical evaluation of this measure found good internal consistency (a = .82–.93) (Thiel & Paul, 2006). Reliability analysis from the present study report Cronbach’s alpha of .94 for the eating disorder composite score (see Table 1). The composite score includes 23 items across the three subscales that ask participants to report their level of endorsement to statements from each subscale. For example, sample items for drive for thinness, bulimic behavior, and body dissatisfaction, respectively, are as follows: “I think about dieting,” “I have gone on eating binges where I have felt that I could not stop,” and “I think that my thighs are just the right size” (Garner, 1991). Participants reported endorsement on a 6-point Likert-type scale that ranged from 1 = never to 6 = always. Answers are scored so that responses in the symptomatic direction for each item are weighted. The weighted responses are summed for each subscale scores, and the subscale scores are summed for the eating disorder composite score; higher scores indicate greater DE behavior. Within this sample, 36.3% of participants met or exceeded the threshold score for clinical levels of drive for thinness, 42.5% met or exceeded the threshold score for clinical levels of bulimic behaviors, and 36.5% met or exceeded the threshold score for clinical levels of body dissatisfaction. These scores reflect only symptoms of DE behavior and are not used for diagnostic purposes.
Results
Only participants who had complete and valid data on all study variables were included in analyses, which resulted in a sample size of 275 participants. To test the hypothesis that resilience would mediate the relationship between PTSD symptoms and DE symptoms, the bootstrap mediation analysis function in Process (Hayes, 2013) for SPSS was used. The total score from the PCL-5 was entered as the independent variable (trauma symptoms), the total score from the BRS was entered as the mediator (resilience), and the eating disorder composite score was entered as the dependent variable. Process reports unstandardized coefficients. The analysis confirmed a significant negative relationship between trauma symptoms and resilience (B = −0.014, SE = 0.002, p < .001), and the overall model was significant, F(1, 273) = 51.3, p < .001, R2 = .16. There was a significant direct effect between trauma symptoms and eating disorder symptoms (B = 0.0104, SE = 0.003, p < .001) and the overall model was significant, F(2, 272) = 23.99, p < .001, R2 = .08. After factoring in resilience, the relationship between trauma symptoms and eating disorder symptoms decreased in strength, but remained significant (B = 0.012, SE = 0.003, p < .001), and the overall model was significant. In the full mediation model, analysis also confirmed a significant negative relationship between resilience and eating disorder symptoms (B = −0.167, SE = 0.08, p = .04). The test of the indirect effect supported significant mediation (indirect effect = .002, 95% confidence interval [CI] = [0.002, 0.005]), as the CI did not include zero. This result indicates an indirect effect of resilience in the relationship between PTSD symptoms and DE outcomes in women with sexual victimization in adulthood (see Figure 1).
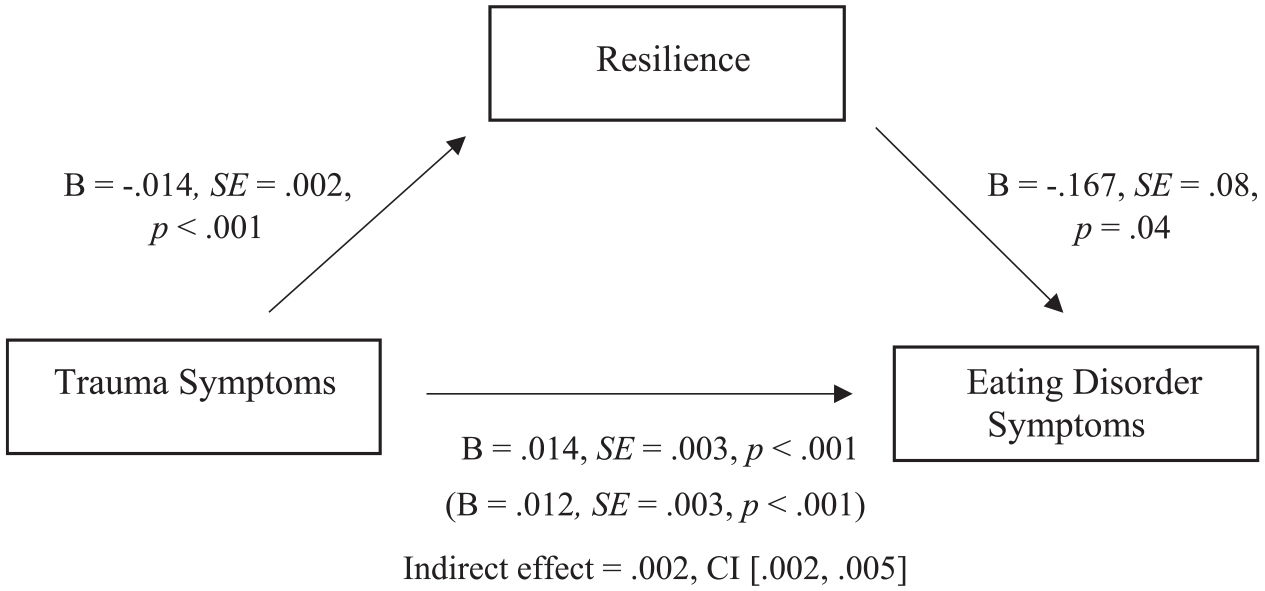
Resilience as a mediator of the relationship between trauma symptoms and eating disorder symptoms.
Exploratory analyses were also run to determine whether resilience was a significant mediator in the relationships between trauma and specific DE symptoms; three additional mediation models were run with each EDI-2 subscale as the outcome variable. Next, the total score from the PCL-5 was entered as the independent variable (trauma symptoms), the total score from the BRS was entered as the mediator (resilience), and the drive for thinness subscale score from the EDI-2 was entered as the dependent variable. The analysis confirmed a significant negative relationship between trauma symptoms and resilience (B = −0.014, SE = 0.002, p < .001), and the overall model was significant, F(1, 287) = 50.8, p < .001, R2 = .15. There was a significant direct effect between trauma symptoms and drive for thinness symptoms (B = 0.0113, SE = 0.004, p < .01) and the overall model was significant, F(2, 286) = 8.24, p < .001, R2 = .05. After factoring in resilience, the relationship between trauma symptoms and drive for thinness symptoms remained significant (B = 0.013, SE = 0.004, p < .001), and the overall model was significant. However, in the full mediation model, analysis did not confirm a significant negative relationship between resilience and drive for thinness symptoms (B = −0.141, SE = 0.106, p > .05). The test of the indirect effect did not support significant mediation (indirect effect = .002, 95% CI = [−0.0005, 0.0039]), as the CI included zero.
The next mediation model was run with the bulimia subscale score from the EDI-2 as the dependent variable. The analysis confirmed a significant negative relationship between trauma symptoms and resilience (B = −0.014, SE = 0.002, p < .001), and the overall model was significant, F(1, 296) = 55.5, p < .001, R2 = .16. There was a significant direct effect between trauma symptoms and bulimic symptoms (B = 0.0136, SE = 0.003, p < .001), and the overall model was significant, F(2, 295) = 17.9, p < .001, R2 = .11. After factoring in resilience, the relationship between trauma symptoms and bulimic symptom remained significant (B = 0.015, SE = 0.026, p < .001), and the overall model was significant. In the full mediation model, analysis did not confirm a significant negative relationship between resilience and bulimic symptoms (B = −0.101, SE = 0.078, p > .05). The test of the indirect effect did not support significant mediation (indirect effect = .001, 95% CI = [−0.0004, 0.0036]), as the CI included zero.
In the final mediation analyses, the body dissatisfaction subscale score from the EDI-2 was entered as the dependent variable. The analysis confirmed a significant negative relationship between trauma symptoms and resilience (B = −0.014, SE = 0.002, p < .001), and the overall model was significant, F (1, 288) = 53.8, p < .001, R2 = .16. There was a significant direct effect between trauma symptoms and body dissatisfaction (B = 0.009, SE = 0.003, p < .01) and the overall model was significant, F (2, 287) = 14.7, p < .001, R2 = .09. After factoring in resilience, the relationship between trauma symptoms and body dissatisfaction remained significant (B = 0.013, SE = 0.003, p < .001), and the overall model was significant. In the full mediation model, analysis confirmed a significant negative relationship between resilience and body dissatisfaction (B = −0.275, SE = 0.089, p < .01). The test of the indirect effect supported significant mediation (indirect effect = .004, 95% CI = [0.0013, 0.0068]), as the CI did not include zero. This result indicates an indirect effect of resilience in the relationship between PTSD symptoms and body dissatisfaction in women with sexual victimization in adulthood
Discussion
The primary goal of this study was to examine the role of resilience in the relationship between PTSD symptoms and DE in a sample of women with sexual victimization history. Results supported the hypothesis that resilience would mediate the association between PTSD symptoms and eating disorder behavior among women with a history of adulthood sexual victimization. When utilizing subscale scores for DE behavior, further analyses indicated that resilience had a significant indirect effect on the association between PTSD symptoms and body dissatisfaction, but not on drive for thinness (anorexia symptoms) or bulimic symptoms. All eating disorder subscales had significant relationships with trauma, but only body dissatisfaction was associated with resilience and had significant mediation.
What remains undetermined by the current study is the functionality of resilience within its mediating role between PTSD symptoms and eating disorder symptoms. Some research suggests that resilience may have regulatory benefits. Previous results demonstrated the ability of highly resilient people to inhibit negative affect, which is an emotion-regulatory function (Waugh et al., 2008). Another study identified emotion regulation difficulties as a transdiagnostic risk factor for DE with binge-related disorders, like bulimia nervosa or binge-eating disorder, showing greater emotion regulation difficulty than restrictive disorders like anorexia nervosa (Mallorquí-Bagué et al., 2018). However, there was not a significant indirect effect of resilience in the relationship between PTSD symptoms and bulimic symptoms in this study. In light of previous research, one might expect that resilience may have a greater mediating effect between PTSD symptoms and bulimic symptoms specifically, but results of this study did not support such a relationship. Although understanding the role of emotion regulation is outside the scope of this study, future research should include assessment for emotion regulation difficulties when assessing DE and resilience. Moreover, investigation of this relationship should include assessment for interactions of resilience and specific characteristics of DE, such as inhibition of negative affect and rumination. Comparison of resilience functions in DE behavior and other psychopathologies may reveal divergent pathways of mitigation.
Also, resilience had a significant indirect effect in the relation between PTSD symptoms and body dissatisfaction. This may indicate that resilience mitigated the negative impact of PTSD symptoms on body satisfaction in this sample of sexually victimized college-age women. This result aligns with previous research that found resilience to be a protective factor against body dissatisfaction in college-age women (McGrath et al., 2009). A literature review of the relationship between sexual trauma and eating disorders identified body perceptions as a pathway between sexual trauma and onset of DE behavior (Madowitz et al., 2015). Specifically, body dissatisfaction was directly linked to DE behavior in survivors of sexual assault (Madowitz et al., 2015). In the present study, the mediating effect of resilience on body dissatisfaction and overall DE symptoms, but not anorexic or bulimic behavior specifically, could indicate that body dissatisfaction is both a consequence of sexual assault and an underlying mechanism to DE behavior that is mitigated by resilience. However, further research must be done to support this point. Future research could examine the effects of body dissatisfaction in survivors of sexual assault to further explicate this relationship.
A strength of this study lies in the variability of DE behaviors reported in the sample. Participants demonstrated a greater range of DE risk than subthreshold or asymptomatic behavior. Limitations of this study include utilization of self-report measures, as well as online data collection, due to the possibility of obtaining false information from participants. In addition, the sexual experience history assessment did not account for assault during incapacitation—doing so may have provided more insight regarding situational effects on survivors’ psychological outcomes. For example, having been assaulted while incapacitated could alter the way an individual conceptualizes and reports their experience. The results of this study are limited due to lack of diversity in the sample, as a whole. Although racial and ethnic minorities were underrepresented compared with national data, racial and ethnic representation in the sample was proportionate to minority representation at the university. Importantly, bisexual women were overrepresented in the final analyses, which the authors consider a strength of the study. This is not surprising, as bisexual women are at higher risk of sexual victimization than both heterosexual and lesbian women (Walters et al., 2013). Because the data are cross-sectional and the questionnaire did not request participants to report the date of last assault, temporal effects could not be examined in analyses. However, because inclusion criteria required that participants be between ages 18 and 25 at the time of participation, and because analysis included only those who reported history of victimization since age 14+, reported experiences of sexual victimization can be expected to have occurred within a limited time frame. Finally, the cross-sectional nature of the current study made it impossible to observe the dynamism of resilience as it relates to psychological well-being. Further study should observe these relationships longitudinally with control for time precedence of first sexual victimization and onset of DE behavior, as well as differentiation among groups of survivors.
Given the high prevalence of sexual victimization within women college students, it is important to identify factors that may account for the relationship between sexual assault and negative outcomes that are often associated with experiencing this type of trauma. The current study examined resilience as one such factor that may mediate the relationship between trauma symptoms and DE. Results from the current study did show that trauma symptoms were indirectly associated with DE severity through resilience. More trauma symptoms were associated with lower resilience, which in turn was associated with more DE. These findings are helpful in understanding how treatments for victims of sexual trauma might be enhanced to improve effectiveness. Treatments that include components of identifying and building aspects of resilience and recovering from adversity may be helpful for victims of sexual trauma. Additional research is necessary to determine the functionality of resilience in those specific relationships and as a protective factor, in general.
Footnotes
Acknowledgments
The authors would like to acknowledge Western Kentucky University’s Office of Research and Creative Activity and Office of Scholar Development for supporting this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.