
Abstract
Community norms provide social scripts and pathways to accruing social capital that can alter a woman’s risk of experiencing sexual intimate partner violence (IPV). These norms are in turn influenced by the structural environment in which they exist. Missing from the literature is an understanding of how an individual’s departure from community norms—positive deviance—influences the risk of sexual IPV and how this effect may vary across structural environments. Demographic and Health Survey data from 32 low- and middle-income countries (LMIC) were stratified into six structural environments by two fundamental structural factors: level of gender inequality and prevalence of sexual IPV. To examine how transcending community norms shape the odds of reporting sexual IPV across environments, six identical multilevel models were fit including statistical deviation from 13 community norms as key covariates. Positive deviance from community norms is associated with both increased and decreased odds of reporting sexual IPV and the nature of these relationships vary by structural environment. Positive deviance had a greater effect on reporting sexual IPV in highly unequal societies. Positive deviance from fertility preferences and controlling behavior was associated with increased odds of sexual IPV across contexts. The accrual of social capital and differences in female autonomy across environments may be two ways positive deviance alters sexual IPV risk. A better understanding of how the salience of community norms varies by structural environment and how transcending these norms shapes the risk for sexual violence may help highlight pathways for interventions to change restrictive social norms and increase female empowerment without increasing the risk of sexual IPV.
Introduction
Sexual intimate partner violence (IPV) is a serious global health concern that has been linked to poor reproductive and sexual health outcomes such as unwanted pregnancy, sexually transmitted infections, and cervical cancer (Centers for Disease Control and Prevention, 2017; World Health Organization, 2013). Sexual IPV is also linked to physical trauma (Centers for Disease Control and Prevention, 2017; World Health Organization, 2013) and negative mental health outcomes, including depression, anxiety, and posttraumatic stress disorder (Centers for Disease Control and Prevention, 2017; Warshaw et al., 2009; World Health Organization, 2013). While the World Health Organization estimates more than one third of women globally will experience physical and/or sexual IPV in their lifetimes (World Health Organization, 2013), the legal and social barriers to reporting sexual IPV mean this is likely an underestimate of the true prevalence. Sexual IPV is also often experienced alongside physical and emotional violence, potentially compounding its negative effects (Naved, 2013; Puri et al., 2011).
While the negative implications of sexual IPV are well-founded, patriarchal notions of marriage as de facto and permanent consent for sex remain pervasive in many contexts (Yllö & Torres, 2016). Only in the past 25 years has sexual violence within marriage begun to be criminalized in low- and middle-income countries (LMIC—a World Bank designation based on per capita gross national income (The World Bank Group, 2019; Yllö & Torres, 2016). The United Nations estimates more than 600 million women still live in countries where sexual IPV within union is legal (UN Women, 2015). A lack of governmental and policy-level support in many LMIC makes the primary prevention of sexual IPV through social norms change especially important. By indirectly reducing its prevalence through changing the factors that shape the risk for sexual IPV, the incidence of sexual IPV may decrease without directly addressing this often politically charged topic. Hence, a better understanding of the risk factors for sexual IPV is needed to develop strategies that will be effective in reducing the prevalence of sexual abuse within marriages in low- and middle-income countries.
Global health research on sexual IPV has primarily examined individual-level risk factors (i.e., age, education, rurality, wealth, parity, occupation, autonomy; Abrahams et al., 2004; Coker et al., 2000; Gage & Hutchinson, 2006). This is despite decades of evidence from studies grounded in social-ecological theory that the norms of a person’s community also have an effect on the risk for all types of IPV (Batchelder et al., 2015; Bronfenbrenner, 1992; Campbell et al., 2009; Carlson, 1984; Flake, 2005; Heise, 1998; McLaren & Hawe, 2005). For example, evidence from low- and middle-income countries suggests that living in a community that is wealthier (Stephenson et al., 2008), has more egalitarian gender norms (Beyer et al., 2015; Pallitto & O’Campo, 2005), and greater female autonomy (Koski et al., 2011; World Health Organization/London School of Hygiene and Tropical Medicine, 2010) is associated with a woman’s reduced odds of IPV overall. Taken together, the community effects literature suggests that living in a place that provides more social and economic opportunities for women may reduce IPV (Beyer et al., 2015; VanderEnde et al., 2012).
Even studies that use a social-ecological approach often lack a holistic view of how social-ecological levels interact with each other to shape the risk of IPV. First, individual characteristics or the characteristics of the household in which a woman lives (i.e., those below the level of the community) may moderate the effect of community norms on an individual woman’s risk for IPV by empowering her to move beyond restrictive, gendered expectations. For example, a woman whose family places a high value on female education may be encouraged to complete secondary school, deviating from the community norm of leaving school early for marriage. The self-efficacy needed to transcend the prevailing community norms may also stem from nonfamilial social networks that create a sense of agency, such as when secondary schooling exposes a woman to others who have lower fertility preferences (Goldenberg & Stephenson, 2017). Second, structural norms (i.e., above the level of the community) may influence which community norms shape the risk for IPV, and to what extent. For example, it may be difficult for a community or household norm to exist that encourages women to continue their education if that community exists in a society in which women are prohibited from attending secondary school. Examining how the community interplays with other levels of the environment is critical for understanding how community factors shape the risk for sexual IPV.
This study applies the concept of positive deviance to examine the association between transcending the norms of one’s community and the reporting of sexual IPV. Initially used to study variations in malnutrition among Vietnamese children despite nearly identical living situations (M. F. Zeitlin et al., 1990), positive deviance is an asset-based approach to understanding what is already working among some members of a community to achieve a desired health outcome (Positive Deviance Initiative, 2017). In the foundational positive deviance study, the children of mothers who fed their children protein-rich shrimp found in rice paddies had better nutritional outcomes, though the mothers were deviating from the prevailing community norm that these and other shellfish were unclean (M. Zeitlin, 1991). Positive deviance studies use a strength-based lens to examine the behaviors and characteristics of those who obtain better outcomes on a given indicator than others in their community even though they have similar access to resources and are exposed to the same community and structural norms (Walker et al., 2007). In this study, positive deviance is quantified statistically as being different, by a standard measure, from the community mean in a demonstrably advantageous way, for example, by attaining a higher level of education or by reducing parity from expected norms. By applying this to sexual IPV, it may be possible to understand which behaviors are already present in the community that can contribute to a lowered risk for violence.
Social-ecological and feminist theories of IPV suggest two structural factors are essential for IPV to occur (Jewkes, 2002). Differences in (a) the degree of gender inequality and (b) the normalization of IPV may alter how community norms are formed and which community norms are most salient to shaping the risk for sexual IPV. To examine the interaction between community norms and their structural environment, this study situates countries (and the communities therein) according to levels of IPV prevalence and gender equality. This allows for comparison of how the interactions between the individual and community levels (e.g., positive deviance) vary by structural environment. This has the potential to uncover how different structural environments affect how positive deviance from community norms shapes the risk for sexual IPV.
It is hypothesized that individual positive deviance from most community norms will be significantly associated with a lower odds of reporting sexual IPV due to the protective effects of higher levels of things like education (female and male), wealth, and decision-making power known from previous IPV literature (World Health Organization, 2013). However, positive deviance from some norms may be seen as challenging deep-seated community norms, increasing the risk of sexual IPV as a way to restore the traditional gender roles (Blanc, 2001). Considering that positive deviance may be rarer in environments with stricter gender norms, we also hypothesize that positive deviance will have a larger effect (in both directions) in structural environments of high IPV and high gender inequality than in settings with lower levels of IPV and gender inequality. A more nuanced understanding of how macrosocial contexts alter how transcending community norms is associated with the risk of sexual IPV has the potential to highlight novel, modifiable factors present across countries that can be leveraged as pathways to reduce sexual IPV.
Materials and Methods
This analysis used data from the Demographic and Health Surveys, the largest repository of IPV-related data in LMIC (ICF International, 2017). The women’s questionnaire from all Demographic and Health Surveys (DHS) collected from 2010 to 2016 that included sexual IPV questions were used (n = 32). The DHS is conducted using a two-stage sampling design to ensure adequate representation at the national, regional, and community levels (ICF International, 2017). First, the most recent census data from each country is used to create geographic demarcations called Primary Sampling Units (PSUs). Twenty to 30 households are then interviewed from each PSU.
A percentage (between 50% and 80% in most countries) of these respondents are randomly selected to answer the Domestic Violence Module. Of these, only ever-married women (those who are currently married or divorced) aged 15 to 49 are asked questions about current or past sexual IPV. Following international standards for interviewing women about this highly sensitive topic (Ellsberg et al., 2001; Ellsberg & Watts, n.d.), exclusion criteria included not having a private space for the interview and interview interruption upon interruption by a third party. Therefore, this analysis includes all respondents aged 15 to 49 who answered all questions regarding sexual IPV and the other covariates from 32 LMIC representing all six World Health Organization (WHO) regions. Samples ranged from 1,448 (Namibia) to 34,681 respondents (Colombia).
To assess whether the association between positive deviance and sexual IPV varies by structural environment, all 32 countries were pooled into separate data sets (n = 6) containing countries with “high” (>10%), “medium” (5%–10%), and “low” (0%–5%) levels of IPV prevalence as well as “high” (>0.6), “medium” (0.5–0.6), and “low” (<0.5) levels of gender inequality according to the United Nations Development Programme’s Gender Inequality Index (GII) (see Table 1; United Nations Development Programme, 2015). The GII uses measures of reproductive health, female empowerment, and female economic status to measure gender equality on a 0 to 1 scale, with a lower score indicating a lower level of inequality. The three countries without a recent GII score were pooled using countries with similar Human Development Index (HDI) rankings as benchmarks (United Nations Development Program, 2016). Final sample sizes for each structural environment are listed in Table 3.
Sample Size, IPV Prevalence, and Gender Inequality Index in 32 Low- and Middle-Income Countries.
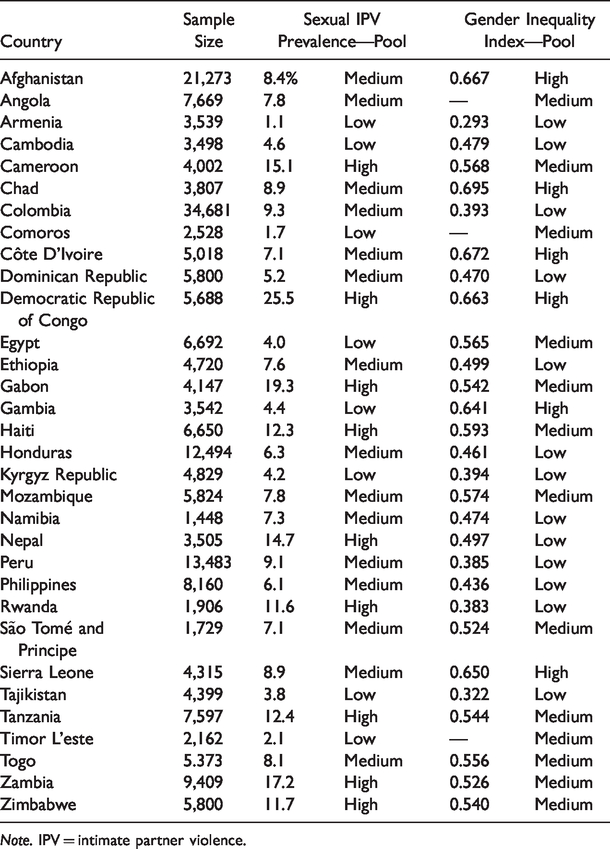
Note. IPV = intimate partner violence.
Key Covariates of Positive Deviance From Community Norms.

Note. IPV = intimate partner violence.
Not measured in all countries.
Associations Between Community Norms, Positive Deviance, and Sexual IPV Among 32 Low- and Middle-Income Countries Pooled by Structural Environment.

Note. Data are presented as adjusted odds ratio, 95% confidence interval, and p value. IPV = intimate partner violence; GII = gender inequality index.
Statistically significant at p < .05. ***Only one country in this pool reported this variable so it was removed from this model.
Outcome
The outcome variable measured lifetime experience of sexual IPV and was coded 1 if the respondent indicated that a husband or male partner had ever committed sexual violence after the age of 15 (“did your husband/partner ever force you to have sexual intercourse with him when you did not want to?” and “did your husband/partner ever physically force you to perform any other sexual acts you did not want to?”).
Key Covariates
Key covariates included 11 binary variables measuring positive deviance from community norms (see Table 2). Since the DHS does not collect community-level data, methods used in previous studies were employed to proxy community-level norms from individual-level data (Metheny & Stephenson, 2017; Stephenson et al., 2013). First, data from all respondents in the analysis sample in each PSU were aggregated to create a community mean (for continuous variables) or proportion (for binary variables). Using only ever-married women (and not all women in the survey) to create community norms ensures that respondents are only compared with women in similar circumstances. To calculate positive deviance for continuous variables, the difference between each woman’s response and the community’s mean was calculated and standardized to a z-score. Respondents whose z-scores were at least one standard deviation above or below the community mean (depending on the directionality of positive deviance) were coded as a positive deviant. For binary variables, respondents were considered positive deviants if they exhibited a positive deviance characteristic and the proportion of women in the community who also exhibited this characteristic was less than or equal to the national average for each country.
Demographic norms and fertility preferences
Community norms and social scripts that reinforce a younger age at marriage, higher fertility, and lower education have been shown to be associated with increased odds of experiencing IPV among LMIC women (Watts & Seeley, 2014). These norms were measured using questions from the DHS on age at first cohabitation (“How old were you when you first started living with him [the male partner]”), ideal number of children (“if you could choose how many children to have in your whole life, how many would that be?”), and education level (“what is the highest level of school you attended? [primary, secondary, or higher]”). Similarly, the degree of difference between partners on these indicators has also been associated with increased odds of experiencing IPV. Stemming from a power imbalance that arises from inequality in these key indicators, violence is often used to reset the balance of power in the relationship, regardless of which partner is older, more educated, or desires more children (Ackerson et al., 2008). The study uses questions from within the DHS that ask women to report on their partner’s age (“How old was your [husband/partner] on his last birthday?”), level of education (“what was the highest level of schooling he [the male partner] attended?), and fertility preferences (“Does your [husband/partner] want the same number of children that you want, or does he want more or fewer than you want?) to assess dyadic differences. Positive deviance is classified as an older age at marriage, desiring fewer children, and having more years of education than the community mean. Similarly, those respondents who have parity in age, education, and fertility preferences with their male partners when this is uncommon in the community would be considered positive deviants.
Socioeconomic norms
A lack of basic resources and the stress of poverty may act as a trigger for inciting IPV (World Health Organization/London School of Hygiene and Tropical Medicine, 2010). In many LMIC, frustration and stress over a man’s inability to live up his prescribed gender role as sole provider for his family may overflow into acts of violence (World Health Organization/London School of Hygiene and Tropical Medicine, 2010). Therefore, while IPV exists across all socioeconomic strata and there are notable exceptions (Kishor & Johnson, 2005, 2006), there is a strong negative relationship between household wealth and IPV (Gibbs et al., 2017). To calculate wealth, this study used the DHS index of durable goods and assets as translated into wealth quintiles. Based on answers to the asset index (which are country-specific), DHS places each respondent into wealth quintiles (poorest, poor, middle richer, richest). Women whose household wealth was above the average for their community were considered positive deviants.
Gender and inequality norms
Normative gender roles and gender inequality are associated with increased IPV due to long-standing patriarchal norms of male dominance and female subordination (Hatcher et al., 2013; World Health Organization/London School of Hygiene and Tropical Medicine, 2010) These norms perpetuate hierarchical gender roles and socialize violence as an acceptable way to assert dominance when these structures are threatened (Jewkes, 2002; Jewkes et al., 2010; Mishra & Tripathi, 2011). Therefore, greater decision-making autonomy, decreased normalization of IPV, and lower levels of gender inequality at a structural level are all associated with decreased odds of experiencing IPV (World Health Organization, 2013).
These structures play out at the dyadic level through controlling behavior by male partners and by women justifying the IPV they experience as warranted, both of which are associated with increased odds of experiencing IPV (Capaldi et al., 2012; Jesmin, 2015; World Health Organization, 2013). Women were assessed for whether their partners exhibited controlling behavior by indicating whether any of the following apply to their relationship (“he is very angry/jealous if you talk to other men”, “he frequently accuses you of being unfaithful”, “he does not permit you to meet with female friends”, “he tries to limit your contact with family”, “he insists on knowing where you are at all times”). If the respondent indicated “yes” to any of these scenarios, she was determined to experience controlling behavior.
The measure of IPV justification was created using five scenarios found in all 32 DHS data sets (“In your opinion, is a husband justified in hitting or beating his wife in the following situations: if she goes out without telling him, if she neglects the children, if she argues with him, if she refuses to have sex with him, and if she burns the food”). Each response was coded 1 if the respondent indicated “yes”. These five scenarios were then added together to create a scale of physical IPV justification. Similarly, a scale of household decision-making autonomy was created using four scenarios found in all 32 DHS data sets (“who usually decides how the money you earn will be used?; who usually decides how your husband/partner’s money will be used?; who usually makes decisions about health care for yourself?; and “who usually makes decisions about major household purchases?”). Women could respond to each question about decision-making by stating they made the decision alone, they made it jointly with their partner, their partner made the decision alone, or the decision was made by someone else. These categories were collapsed so that the question was coded 1 if the woman indicated she had any say in the decision (i.e., made the decision alone or jointly with her husband/partner). These were added together to create a 4-point scale of household decision-making autonomy. Women who did not experience controlling behavior in communities where this was common or had scores on the IPV justification or decision-making autonomy scales that were at least one standard deviation above average for their communities were classified as positive deviants.
Analysis
The nesting of respondents within communities (PSUs) and communities within countries means that the data have a three-level nested structure, necessitating the use of multilevel modeling in this analysis (Assari, 2013). Compared with standard logistic regression analyses, multilevel modeling corrects for the downward bias in standard errors created by the nonindependent nature of nested data and introduces an error term that captures the effects of unobserved covariates (Assari, 2013).
Six multilevel logistic regression models were fit, one for each structural environment. Models were identical in each context and included the 13 positive deviance covariates as well as measures of these variables at the individual and community levels and rural/urban status. Two additional variables were included at the individual or community levels based on their prominence in the literature as indicators of violence. Rurality was included at the individual level to control for the disparate levels of violence between rural/urban communities commonly seen in LMIC (Madhivanan et al., 2014; Pronyk et al., 2008; Stephenson et al., 2016). Women’s employment outside the home was also included at the individual level and at the community level to control for the access to financial resources and social capital (individual level) and more progressive social norms (community level) this may provide (Chaudhary et al., 2009; Flake, 2005; Hindin & Adair, 2002). However, because employment outside the home may not be of the woman’s volition or be undertaken due to financial strain, there was no way to determine which direction was demonstrably advantageous to women in LMIC generally. For this reason, it was not included as a positive deviance variable.
In these data sets, respondents are nested within communities (PSUs) and communities are clustered within countries. However, sparseness in higher-order clusters (defined as 50 clusters or fewer) widens confidence intervals and increases the chance of a Type I error (Bell et al., 2008). As the maximum number of level-three clusters in any one data set was 12, country was instead added as a fixed effect at level one to account for the nesting of participants by country. The domestic violence weights were also included per the DHS Guide to Statistics (Macro International, 1996) to account for sampling error present in the analysis.
Results
The reported lifetime prevalence of sexual IPV varied widely across countries, from 1.1% in Armenia to 25.5% in the Democratic Republic of Congo (DRC) (see Table 1). Across structural environments, results at the individual and household levels are largely consistent with those found in previous literature (World Health Organization, 2013). More educated women, those who marry at an older age, and those with more decision-making autonomy had significantly lower odds of reporting sexual IPV across contexts than less educated women, those who marry at a younger age, and those with less decision-making power. Likewise, women who more often justify IPV are employed outside the home and report controlling behavior had significantly greater odds of experiencing sexual IPV than women who did not work outside the home, and did not report controlling behavior (see Table 3).
Demographic Norms and Fertility Preferences
Positive deviance from community norms of education was associated with significantly lower odds of reporting sexual IPV in countries with medium and high levels of gender inequality (adjusted odds ratio [aOR]: 0.91 and 0.83, respectively). Marrying at an older age than is average for the community was also associated with significantly lower odds of reporting sexual IPV in medium GII countries (aOR: 0.87) and high IPV countries (aOR: 0.84). Being a positive deviant on dyadic age difference was associated with significantly greater odds of reporting sexual IPV in countries with high gender inequality (aOR: 1.07) and a high prevalence of sexual IPV (aOR: 1.12). Positive deviance on fertility preferences was associated with a significantly greater odds of reporting sexual IPV across contexts, with significant findings in Low IPV (aOR: 1.53), Low GII (aOR: 1.28), and Medium GII countries (aOR: 1.12), and High IPV Countries (aOR: 1.15) (see Table 3).
Socioeconomic Norms
A higher household income than is average for the community was associated with a significantly lower odds of reporting sexual IPV in countries with the highest levels of gender inequality (0.89) and significantly greater odds in Low GII countries (aOR: 1.28)(see Table 3).
Gender and Inequality Norms
Justifying IPV in fewer circumstances than the community norm was associated with significantly lower odds of reporting sexual IPV in High IPV countries (aOR:0.86) and Low GII countries (aOR:0.70). Positive deviance from experiences of controlling behavior was associated with significantly lower odds of reporting sexual IPV in High IPV countries (aOR: 0.35) and High GII countries (aOR: 0.28)(see Table 3).
Discussion
The results support the hypothesis that structural context alters how positive deviance from community norms is associated with sexual IPV, highlighting the need to recognize the structural environment in which positive deviance behaviors are enabled to occur. Overall, settings characterized by greater gender equity and lower IPV prevalence show weaker associations between positive deviance behaviors and reporting sexual IPV than contexts of higher inequality and IPV prevalence. Drawing on existing literature of social norms and IPV (What Works to Prevent Violence, 2019; World Health Organization, 2009a, 2010), we hypothesize that positive deviance may represent less of a challenge to social expectations in more egalitarian societies. This may make positive deviance less impactful than it is for those who live in more unequal contexts due to the less stringent gender norms commonly present in areas with lower IPV and gender inequality (European Institute on Gender Equality, 2015; World Health Organization, 2009b).
Two potential pathways emerged from the results of this study for how positive deviance from community norms may mediate the risk for sexual IPV. First, a woman’s accrual of social capital may provide insight into the observed relationships between positive deviance and the reporting of sexual IPV. Social capital is commonly defined as access to community resources and social networks, and may be formal (i.e., education or employment) or informal (i.e., networks of friends who can provide access to support and information) (Zolotor & Runyan, 2006). Positive deviance behaviors could provide access to formal social capital, which may also lead to the accrual of more informal forms of social capital such as social networks or differing perspectives on gender roles. Women who accrue social capital through positive deviance behaviors may also experience increased financial contributions and increased exposure to alternative social norms outside of the home that could shift their perceived value within the household, further altering their risk for sexual IPV.
These direct relationships between opportunities to accrue social capital and decreases in IPV are not new (Naved & Persson, 2008; Sambisa et al., 2010; Stephenson & Tsui, 2003). However, positive deviance may also indirectly shape the relationship between social capital and sexual IPV. Across contexts, women who were positively deviant to education and age at marriage, and therefore may be able to accrue formal social capital, had lower odds of reporting sexual IPV. However, positive deviance from dyadic differences in age and education were associated with significantly greater odds of reporting sexual IPV across contexts. It is possible that positive deviance behaviors that lead to the accrual of formal social capital generally may be less likely to be associated with an increased risk of sexual IPV than those that directly challenge male partners’ sense of control within the household or status in the community. In this way, some positive deviance behaviors may lead to reductions in social capital, which then increase the risk for sexual violence to restore power dynamics that favor males (Blanc, 2001; World Health Organization/London School of Hygiene and Tropical Medicine, 2010).
A second potential pathway between positive deviance and sexual violence may be partially explained by changes in female autonomy. Women who can marry later than the norm for their community may have greater autonomy in decisions around when to marry, and this autonomy may translate into increased equity and reduced violence within the marriage. Like the proposed explanation for the indirect role of social capital in shaping the risk of sexual IPV, women whose families allow (or encourage) an older age at marriage than the community norm may also hold less restrictive expectations and values for women. These are in turn linked to a lower risk of violence (Hadley et al., 2010). Positive deviance from norms of decision-making autonomy may be evidence of the role of autonomy in transcending social norms and reducing a woman’s risk of sexual IPV. These results suggest interventions that work to transcend social expectations via increasing autonomy may be a useful pathway to reducing violence.
Two exceptions to the proposed pathways were observed. First, the association between positive deviance from fertility preferences and increased odds of reporting sexual IPV was significant across contexts. This may be because women feel pressure to conform to the fertility norms of their community both in low-fertility (Billari et al., 2009) and high-fertility (Paek et al., 2008) settings. Second, women who reported less controlling behavior than was average for their community also had an increased odds of reporting sexual IPV across contexts. While this may seem counterintuitive, the way controlling behavior is defined in the DHS may mask more subversive forms of control. That is, men who place fewer restrictions on their partners’ movements and social associations may assert control in more private (i.e., less outwardly noticeable) ways.
Another explanation for this finding may be that women with fewer restrictions on their movement and social associations may also have wider social networks that give them a broader view of what constitutes violence, and these women are more likely to report sexual violence. Sexual violence within marriage is still commonly misunderstood across structural contexts, and the view that consent is permanently granted upon entering into a marriage is still widespread (UN Women, 2015). For example, six of the countries in this study have no law against marital rape at all (UN Women, 2015). While the reasons behind these two findings are likely to vary by country, the consistency of the results shows the universality of patriarchal norms and represents the gendered expectations for women across structural contexts.
There are several limitations to this analysis. First, any study of the factors associated with IPV victimization runs the risk of implicitly placing some of the blame of IPV on those who experience it. While this is certainly not the intention of this analysis, it bears noting that the forces that shape IPV victimization are the result of a complex, multilevel interplay of forces at the individual, dyadic, community, and structural levels, none of which emanate from the survivor him or herself. The cross-sectional nature of DHS data precludes inferences of causality between positive deviance and reporting of sexual IPV and allows for the possibility of a temporal disjuncture between positive deviance status and sexual IPV. It also makes it impossible to approximate community norms at the exact time that sexual IPV may have occurred. That is, because this study uses a lifetime report of IPV, it is possible that community norms (and therefore the respondent’s positive deviance status) have changed since the reported instances of sexual violence.
The DHS also samples only ever-married women for the Domestic Violence Module, introducing a potential selection bias against partnered, nonmarried women who may also experience sexual IPV. This may compound the already low prevalence of sexual IPV—one that is widely seen to be greatly underreported. As in previous studies of community norms using DHS data, the PSU was used as a proxy for the community. While this is the best approximation currently available, it is a purely geographical measure and may not fully correspond to the concept of community in terms of cultural context. As the sample includes women who are currently in a relationship as well as those who are divorced/separated, it is possible that the information reported about the male partner is not relevant to the respondent’s current marital status. Finally, the clustering of countries by structural environment inherently diminishes community- and country-level variation. For this reason, the results of this analysis should be viewed as a broad and exploratory analysis of how structural context may change the relationships between positive deviance from community norms and the risk for sexual IPV.
Conclusion
The associations identified between positive deviance and the reporting of sexual IPV vary by the country-level context of gender inequality and prevalence of IPV. Macro-social contexts alter the salience of positive deviance from some community norms, but are remarkably consistent for fertility preferences and controlling behavior. These associations may be explained through one, or a combination of two, pathways: the accrual of social capital and gains in autonomy that allow women to alter their risk of sexual IPV. The identification of positive deviance behaviors that are linked to lowered reporting of sexual IPV provides insight into the ways in which women can transcend patriarchal norms without the unintended consequence of sexual IPV. In turn, these positive deviance behaviors may form the framework for developing local, community-specific interventions that use behaviors already present in the community to tackle the structural norms and inequalities that place women at risks for sexual violence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.