
Abstract
Objectives
Claims that the diversity of social ties matters more for health than the sheer number of ties have largely gone untested. This study accordingly compared the unique associations of number versus diversity of social ties with key health-related outcomes: functional limitations and leisure activities. Additionally, positive and ambivalent ties were distinguished.
Methods
Social networks, health, and leisure activities were assessed in a national sample of older adults (N = 874; ages 65–91).
Results
Regression analyses revealed that number of ties related to each outcome at a magnitude comparable to, or exceeding, that of diversity in most models. For positive ties, number related more strongly than diversity to greater leisure activities. For ambivalent ties, number related more strongly than diversity to worse functional limitations.
Discussion
Contrary to prevailing views, diversity of ties is not necessarily more important than number of ties. Findings extend scientific understanding and approaches to interventions.
Evidence demonstrating the power of social relationships to influence health and well-being has grown substantially in recent decades (Holt-Lunstad et al., 2010). Remarkably, being integrated in a large and diverse social network, in which a person participates in an array of social roles, was found to be associated with a 91% increase in survival odds in a meta-analysis (Holt-Lunstad et al., 2010). Older adults who are more socially integrated experience fewer functional declines (Avlund et al., 2004) and greater leisure activity engagement (Lee & Payne, 2015; Sasidharan et al., 2006)—both of which have been described as key components of successful aging (Rowe & Kahn, 1997). Researchers have yet to determine, however, whether the diversity of social ties contributes more to healthy and active aging than does the sheer number of social ties. The current study sought to determine which of these social network characteristics—diversity or number of ties—might best account for such health-related outcomes.
Despite documented benefits of both large and diverse networks, theoretical perspectives have increasingly emphasized diversity as essential to good health (Berkman et al., 2000; Chin & Cohen, 2020; Cohen & Janicki-Deverts, 2009). This emphasis dovetails with functional specificity theory (Weiss, 1969), which posits that different types of social ties perform specific functions for which they are optimally suited and, therefore, are not readily interchangeable. In later adulthood, family members often serve as key sources of instrumental support, whereas friends often serve as key sources of companionship, but less often vice versa (e.g., Rook et al., 2011). Close partners, in contrast, are less specialized and tend to perform multiple functions. In Weiss’s view, therefore, having a diverse social network that includes close partners, family members, and friends is essential for well-being. Diversity of social ties is commonly conceptualized as participation in a broad range of role relationships (e.g., spouse/partner, friend, parent, co-worker, neighbor; Cohen et al., 1997). Having diverse social roles is believed to enhance health and activity engagement by providing access to a broader range of support functions (Berkman et al., 2000; Cohen, 2021). Therefore, it is important to construe diversity in terms of key social network members who perform these functions. Common approaches to investigating the diversity of social ties, however, are often agnostic regarding function, and analyses of links with health-related outcomes rarely adjust for the sheer number of ties.
Furthermore, role relationships do not inevitably serve as sources of positive functions. Most studies, however, implicitly assume that a diverse network is comprised of exclusively positive ties (Holt-Lunstad et al., 2010), without accounting for potentially mixed, or ambivalent, relationships. Therefore, further research is needed to disentangle number versus diversity of ambivalent ties, as well as positive ties.
A Closer Look at the Importance of Diversity of Social Ties
Disentangling the unique health-related implications of number versus diversity of social ties is important for both scientific and practical reasons. Failure to differentiate between the two kinds of ties limits scientific understanding of which social network characteristics are most important for promoting healthy and active aging. Additionally, without a strong evidence base, suggestions that interventions should emphasize diversity (e.g., Cohen & Janicki-Deverts, 2009; Rhee et al., 2021) might be premature. Indeed, providing opportunities for older adults to develop ties, not necessarily diverse ties, may be crucial when combatting loneliness or isolation (Hawkley & Cacioppo, 2010; Stevens et al., 2006). Nonetheless, claims about the unique importance of diversity relative to number have been reasserted over the years, even though evidence for this claim is sparse, highlighting the need for further examination.
Diversity of Social Ties and Physical Health
An influential study by Cohen et al. (1997) in which healthy volunteers (ages 18–55) were exposed to a common cold virus revealed that greater diversity of social ties was related to lower cold susceptibility, even after adjusting for number of ties. Number of ties itself was unrelated to cold susceptibility. The authors concluded that diversity of ties matters most for health. Given this conclusion, a person with seven social ties that reflect three role relationships (e.g., spouse/partner, friends, parents) would be expected to have access to a broader range of support functions and to experience better health than would someone with seven ties that reflect only one role (e.g., friends). To our knowledge, however, there has been no replication of this explicit comparison between number and diversity of social ties in older age groups or with regard to outcomes other than cold susceptibility.
One study found that number and diversity of social ties each predicted mortality risk among older adults (Ellwardt et al., 2015), but it did not compare the relative magnitude of each effect. Other studies (Fingerman et al., 2020; Fiori et al., 2007; Rhee et al., 2021) have found diverse social ties to be important for various aspects of well-being in later life but, again, have not demonstrated the unique contribution of diversity independent of the sheer number of social ties (as such a comparison was not a central goal of these studies). No studies have compared their unique effects on functional limitations (i.e., difficulty with essential tasks of daily living), a health outcome crucial to older adults’ independence (Avlund et al., 2004). Therefore, the current study investigated whether number or diversity of social ties would exhibit a stronger unique association with this important aspect of physical health in later life.
Diversity of Social Ties and Leisure Activities
Research is also beginning to elucidate the characteristics of social integration that are linked to engagement in leisure activities among older adults. Leisure activities are broadly defined as enjoyable, voluntary activities engaged in during free time, such as hobbies, entertainment, or social visits (Adams et al., 2011; Kelly, 1996). Engaging in leisure activities predicts greater happiness and reduced mortality among older adults (Lee & Payne, 2015; Menec, 2003; Rowe & Kahn, 1997). The importance of social relationships for leisure activities is well established, with social support being key in helping older adults maintain active lifestyles (Franke et al., 2013; Sasidharan et al., 2006). Researchers speculate that having diverse social ties, in particular, may provide greater opportunities for social experiences (Cohen & Lemay, 2007), stimulate more novel and varied conversations (Keller-Cohen et al., 2006), and allow greater freedom to participate in varied activities and roles (Fiori et al., 2007).
As these speculations continue to pique interest, a few studies have begun to test these predictions directly. A recent study using ecological momentary assessment (Fingerman et al., 2020) found that older adults who had more diverse social contacts engaged in a greater variety of daily behaviors (including leisure activities) than did older adults who had less diverse social contacts throughout the day. These analyses, however, were not structured to examine whether the increase in activities was indeed due to the diversity, as opposed to the sheer number, of participants’ social contacts. In other words, do individuals with more diverse ties simply have more ties, with the latter driving increases in leisure activities?
Leisure activities are not always associated with exclusively positive social ties, however. Obligatory or unwanted social contacts can prompt leisure participation (Coleman & Iso-Ahola, 1993). For example, obligations to in-laws might prompt family gatherings. Such findings highlight the need to distinguish number and diversity of mixed (ambivalent) ties as well as positive ties.
Ambivalent Social Ties: An Overlooked Aspect of Diversity of Social Ties
Some social ties that provide support and companionship may simultaneously serve as sources of strain or conflict—reflecting relationships that are “mixed” or ambivalent in nature (Holt-Lunstad & Uchino, 2019; Rook et al., 2012). Ambivalent ties comprise as much as 27% of older adults’ social networks and tend to be family members (Fingerman et al., 2004). Thus, studies examining diverse social ties may unintentionally include some ambivalent ties in their overall assessment of participants’ social networks. Failure to differentiate positive and ambivalent ties can lead to misconstrued findings (Holt-Lunstad & Uchino, 2019), given their opposite associations with health.
Ambivalent ties have been consistently associated with adverse health outcomes (see reviews Holt-Lunstad & Uchino, 2019; Ross et al., 2019), including more functional limitations among older adults (Rook et al., 2012), but their association with leisure activities is less clear. Older adults may selectively avoid activities with such ties. It is also possible that contact with ambivalent ties focuses on more practical tasks (e.g., household chores) or passive activities (e.g., watching television), rather than active leisure engagement. Alternatively, because ambivalent ties have positive as well as negative components, it is possible they could be beneficial in some respects. Rook et al. (2012) examined this possibility but found that positive exchanges with ambivalent ties were unrelated to older adults’ health and well-being. However, that study focused on the functions performed by ambivalent ties, rather than the number or diversity of these ties. No studies, to our knowledge, have explicitly contrasted the effects of number versus diversity of ambivalent ties on health and leisure activity engagement. An additional goal of the current study, accordingly, was to contrast the implications of number versus diversity of ambivalent ties, as well as positive ties.
Current Study
A widespread view in the literature states that having diverse social ties matters more for health and well-being than does having numerous social ties. The empirical basis for this view is rather limited, however, and ambivalent ties are rarely considered. The current study examined whether number and diversity of social ties exhibit unique associations with older adults’ functional limitations and leisure activities (key markers of healthy and active aging), and we compared those associations separately for positive and ambivalent ties.
Method
Sample
Participants were drawn from the baseline sample of a larger study, the Later Life Study of Social Exchanges, a national survey of older adults spanning a 2-year period (see Sorkin & Rook, 2004 for study details). Probability sampling was used to select a representative sample of older adults, ages 65 and older, living in the coterminous United States. Participants were randomly selected from a 5% sample of the Medicare Beneficiary Eligibility List provided by the Centers for Medicare and Medicaid Services. This list includes all older adults in the U.S., regardless of Social Security benefit status; however, no information is released for individuals over 100 years old or non-legal residents. Participants received an initial invitation by mail, followed by a phone call or in-person visit. Of those who could be contacted and met eligibility criteria, 53% consented to participate in the study. Participants received monetary compensation (up to a total of $75) for the interviews that they completed across the study period. All study participants were noninstitutionalized, English-speaking, and cognitively functional. Eighty-three percent were non-Hispanic White and 17% belonged to a racial or ethnic minority group (including Black or African American, Hispanic or Latino/a/x, and mixed or other race/ethnicity). At baseline, the total sample consisted of 916 adults ages 65 to 91, and closely resembled the older adult (65+) U.S. population (U.S. Census Bureau, 2002).
Procedure
The current study used data from the baseline in-person interview (lasting approximately 70 minutes), which included questions about demographic characteristics, social networks, physical health, and leisure activities. Questions were read to the participant, with the interviewer recording their responses. Data were collected by Harris Interactive, Inc., a major survey research firm with extensive experience conducting public polls and social science surveys, including with older adults. Written informed consent was obtained from all participants in the study. All study procedures were approved by a university Institutional Review Board (approval number HS 96-257).
Measures
Social Network Characteristics
We used a three-step process to identify the number and diversity of social network members who functioned as positive or ambivalent ties. First, participants reported on positive and negative social exchanges they had experienced in the past month (see Newsom et al., 2005 for additional information). Twelve items assessed four domains of positive exchanges (three items per domain): receiving emotional support, instrumental support, and informational support from others, and experiencing companionship with others. Twelve additional items assessed four corresponding domains of negative exchanges (three items per domain): insensitivity or criticism by others, being let down in times of need, receiving unwanted or unsound advice, and experiencing rejection or neglect by others.
Second, for each domain of social exchanges, participants were asked to provide names (first name, last initial) of people involved in those exchanges (McCallister & Fischer, 1978), as well as their role relationship with each person (Cohen et al., 1997). Network members were classified into 13 distinct role relationships: spouse/partner, adult children, siblings, parents, grandchildren, other relatives, in-laws, friends, neighbors, co-workers, acquaintances, home aides, or other non-relatives.
The final step involved calculation of the number and diversity of participants’ social ties. Number of positive ties was calculated as the simple tally of people who were named for positive exchanges only, and diversity of positive ties was calculated as the number of distinct role relationships reflected in these ties. For example, a participant who named six positive ties comprised of four friends, one adult child, and a spouse would receive a number score of six and a diversity score of three (reflecting three distinct role relationships). Number of ambivalent ties was calculated as the simple tally of people who were named for both positive and negative exchanges, 1 and diversity of ambivalent ties was calculated as the number of distinct role relationships reflected in these ties. Participants whose networks did not contain any positive ties were necessarily excluded from the models of positive ties to avoid confounding the “number versus diversity” of existing positive ties with the “presence or absence” of positive ties. Moreover, role relationships cannot be defined for absent ties, and the primary goal of the study was to examine the characteristics of existing ties. For the same reasons, participants whose networks did not contain any ambivalent ties were necessarily excluded from the models of ambivalent ties. In addition, some participants (n = 42) had incomplete social network data or lacked both positive and ambivalent ties, and were accordingly excluded from all analyses, leaving a total of 874 participants in the current study.
The current study did not examine negative ties because they were extremely rare, comprising only 8% of participants’ social ties, on average. Moreover, our study aim was to evaluate prevailing views that diversity is more beneficial than number, and the diversity of purely negative ties has not been posited to benefit either of our outcomes. Whether diverse negative ties harm health and well-being to a lesser extent than do numerous negative ties is an interesting question that is beyond the scope of the current study.
Functional Limitations
Functional limitations were assessed using a 15-item self-report scale about basic activities of daily living, instrumental activities of daily living, upper extremity strength, and mobility (e.g., bathing, managing finances, lifting 15-pound objects, climbing stairs; e.g., Lawton & Brody, 1969). Participants indicated how difficult it would be for them to do each activity by themselves, using a response scale of 0 (Not At All Difficult) to 3 (Very Difficult). All items were averaged, with higher scores indicating greater functional limitations (Cronbach’s α = .92).
Leisure Activities
Frequency of leisure activities was assessed using a 9-item self-report scale similar to previous studies of leisure activities among older adults (cf. Adams et al., 2011). Activities likely to be freely chosen and undertaken for enjoyment or meaning were included (i.e., attend meetings of clubs/organizations, get together/talk on the phone with friends, get together/talk on the phone with family, work on a hobby, play cards/bingo/similar games, go out to a movie/restaurant/sporting event, go out shopping, go on trips, and do volunteer work). Participants were asked how often in the past month they did each activity. Response options ranged from 0 (Never) to 5 (Daily). All items were averaged, with higher scores indicating more frequent engagement in leisure activities. Unlike a summed score, an average takes into account potential individual differences in access or resources to engage in a broad range of activities, as well as preferences to engage in few, rather than many, activities. Internal consistency was moderate (Cronbach’s α = .62), consistent with evidence that participation in different leisure activities tends not to be strongly correlated (Adams et al., 2011).
Analytic Strategy
As an initial test of whether number or diversity is more strongly related to each outcome (functional limitations and leisure activities), difference tests of dependent correlations were conducted using zero-order correlation coefficients (Lee & Preacher, 2013; Meng et al., 1992). We then examined whether these differences were robust to the inclusion of covariates using a series of multiple regression models in SPSS Version 24. First, a set of sociodemographic and health variables known to be theoretically and empirically related to our outcomes (e.g., Antonucci et al., 2010) were evaluated as potential covariates in models without the social network predictor variables. The following covariates were considered: age, sex, education, ethnic/racial minority status, employment status, marital status, and number of chronic health conditions. Covariates that were significantly associated (p < .05) with a target outcome were retained in the final model for that specific outcome.
To examine whether number and diversity of positive ties exhibit unique associations with each outcome, multiple regression models were conducted using participants whose networks contained positive ties (n = 854; including 574 who had exclusively positive ties and 280 who had both positive and ambivalent ties).To examine the relative magnitude of their unique associations, confidence intervals (CI; bootstrapped with 5,000 resamples) for the regression coefficients were compared for number versus diversity of positive ties from each model (Greenland et al., 2016). These steps were repeated to compare number versus diversity of ambivalent ties, focusing on participants whose networks contained ambivalent ties (n = 300; including 20 who had exclusively ambivalent ties and 280 who had both positive and ambivalent ties). The 280 participants who had both positive and ambivalent ties were necessarily included in both sets of analyses. Outcomes and social network predictor variables were standardized prior to entry using the corresponding n for each model to account for the different ranges in scores and permit CI comparisons.
Means, Standard Deviations, and Intercorrelations for the Study Variables.
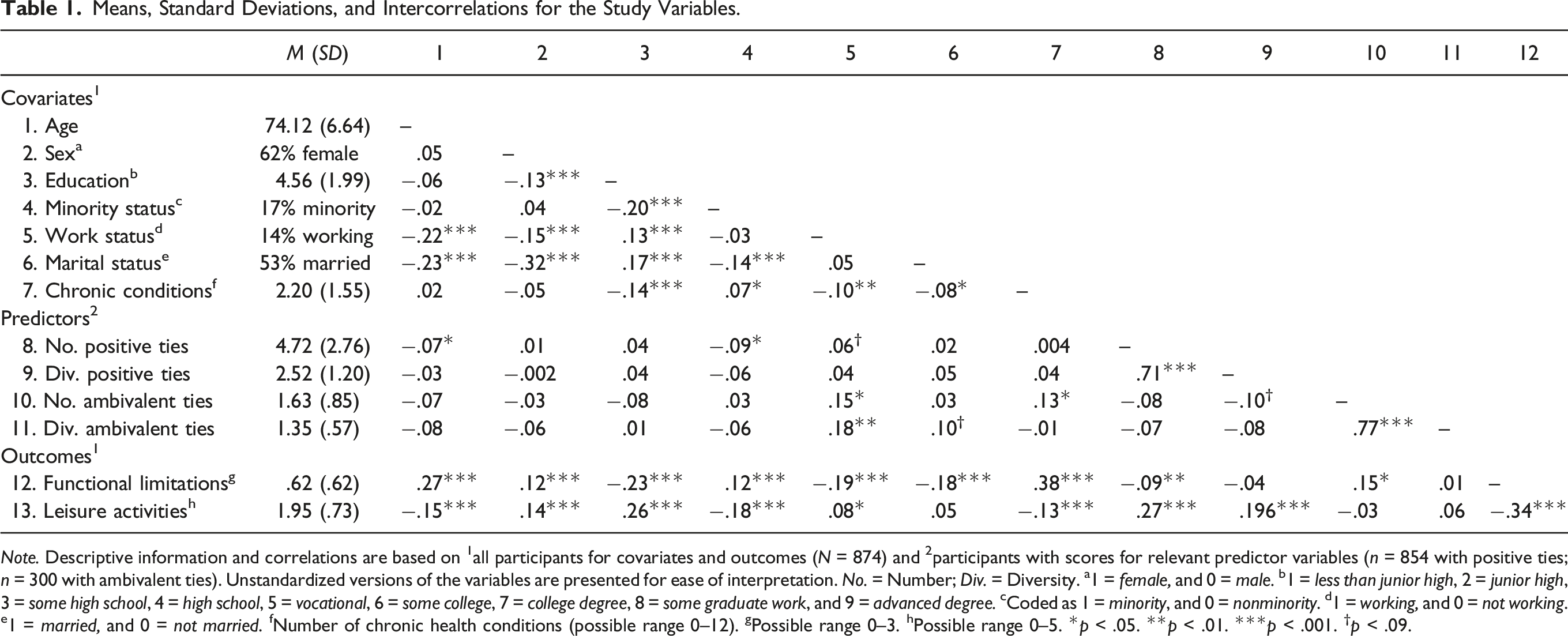
Note. Descriptive information and correlations are based on 1all participants for covariates and outcomes (N = 874) and 2participants with scores for relevant predictor variables (n = 854 with positive ties; n = 300 with ambivalent ties). Unstandardized versions of the variables are presented for ease of interpretation. No. = Number; Div. = Diversity. a1 = female, and 0 = male. b1 = less than junior high, 2 = junior high, 3 = some high school, 4 = high school, 5 = vocational, 6 = some college, 7 = college degree, 8 = some graduate work, and 9 = advanced degree. cCoded as 1 = minority, and 0 = nonminority. d1 = working, and 0 = not working. e1 = married, and 0 = not married. fNumber of chronic health conditions (possible range 0–12). gPossible range 0–3. hPossible range 0–5. *p < .05. **p < .01. ***p < .001. †p < .09.
Results
Initial Analyses
Demographic information and means, standard deviations, and correlations among all study variables are shown in Table 1. As an initial test of whether number or diversity was more strongly related to each outcome, difference tests of dependent correlations were conducted using zero-order correlation coefficients (Lee & Preacher, 2013; Meng et al., 1992). The difference test approach compares the magnitude of two correlations that share one variable in common (in this case, functional limitations or leisure activities), while accounting for the association between the unshared variables (in this case, number and diversity of ties), but does not account for covariates. For correlations with functional limitations, number of positive ties was marginally stronger than diversity of positive ties (Z = |1.92|, p = .055); similarly, number of ambivalent ties was significantly stronger than diversity of ambivalent ties (Z = |3.58|, p < .001). For correlations with leisure activities, number of positive ties was again stronger than diversity of positive ties (Z = |2.93|, p < .01); conversely, number of ambivalent ties was weaker than diversity of ambivalent ties (Z = |2.29|, p = .02). These difference tests provided a rough understanding of these comparisons; however, further tests were needed to determine whether these comparisons were robust to the inclusion of covariates.
Covariate Testing
Functional Limitations Regressed on Number and Diversity of Ties.

Note. Each panel shows results from separate multiple regression models. Potential covariates not included due to non-significance: minority status and marital status (model of positive ties); sex, education, work status, and marital status (model of ambivalent ties). Social network predictors and functional limitations were standardized prior to entry using corresponding n for each model. B regression coefficient; CI confidence interval bootstrapped. a1 = female, and 0 = male. b1 = less than junior high, 2 = junior high, 3 = some high school, 4 = high school, 5 = vocational, 6 = some college, 7 = college degree, 8 = some graduate work, and 9 = advanced degree. c1 = working, and 0 = not working. dNumber of chronic health conditions (possible range 0–12). eCoded as 1 = minority, and 0 = nonminority. *p < .05. **p < .01. ***p < .001. †p = .09.
Leisure Activities Regressed on Number and Diversity of Ties.

Note. Each panel shows results from separate multiple regression models. Potential covariates not included due to non-significance: work status and marital status (model of positive ties); age, minority status, work status, and marital status (model of ambivalent ties). Social network predictors and leisure activities were standardized prior to entry using corresponding n for each model. B regression coefficient; CI confidence interval bootstrapped. a1 = female, and 0 = male. b1 = less than junior high, 2 = junior high, 3 = some high school, 4 = high school, 5 = vocational, 6 = some college, 7 = college degree, 8 = some graduate work, and 9 = advanced degree. cCoded as 1 = minority, and 0 = nonminority. dNumber of chronic health conditions (possible range 0–12). *p < .05. **p < .01. ***p < .001. †p < .09.
Number versus Diversity of Social Ties and Functional Limitations
Positive Ties and Functional Limitations
A multiple regression model adjusting for relevant covariates examined the associations of number and diversity of positive ties with functional limitations (see Table 2, top panel). Number of positive ties exhibited a marginally significant unique association with fewer functional limitations [β = −.07, t(815) = −1.69, p = .09], whereas diversity of positive ties did not exhibit a unique association [β = .003, t(815) = .08, p = .94]. The CIs for each standardized regression coefficient contained the point estimate of the other, indicating that the unique (albeit non-significant) associations of number and diversity of positive ties with functional limitations were comparable in magnitude (see Figure 1, left panel). Comparing Confidence Intervals of Point Estimates for Functional Limitations Regressed on Number versus Diversity of Ties. Note. Each panel shows the standardized regression coefficients (β) and their 95% confidence intervals (CI) from separate multiple regression models in which functional limitations was regressed on number and diversity of positive ties (left panel, n = 854) or number and diversity of ambivalent ties (right panel, n = 300), adjusting for relevant covariates. Variables were standardized using the corresponding n for each model. Coefficients significantly differ in magnitude if their CIs do not contain the coefficient from the other (Greenland et al., 2016). *p < .05.
Ambivalent Ties and Functional Limitations
A parallel model contrasted the associations of number and diversity of ambivalent ties with functional limitations (see Table 2, bottom panel). Number of ambivalent ties exhibited a unique association with greater functional limitations [β = .22, t(291) = 2.77, p = .006]. Unexpectedly, diversity of ambivalent ties exhibited a unique association with fewer, rather than more, functional limitations [β = −.16, t(291) = −1.99, p = .047]. The CIs for each standardized regression coefficient did not contain the point estimate of the other, indicating that number of ambivalent ties was significantly more strongly related to functional limitations, compared to diversity of ambivalent ties (see Figure 1, right panel).
Number versus Diversity of Social Ties and Leisure Activities
Positive Ties and Leisure Activities
A multiple regression model adjusting for covariates examined the associations of number and diversity of positive ties with leisure activities (see Table 3, top panel). Number of positive ties exhibited a unique association with greater leisure activities [β= .23, t(834) = 5.27, p < .001]. Diversity of positive ties, in contrast, did not did not exhibit a unique association with leisure activities [β = .01, t(834) = .25, p = .80]. Moreover, the CIs for each standardized regression coefficient did not contain the point estimate of the other, indicating that number of positive ties was significantly more strongly related to leisure activities, compared to diversity of positive ties (see Figure 2, left panel). Comparing Confidence Intervals of Point Estimates for Leisure Activities Regressed on Number versus Diversity of Ties. Note. Each panel shows the standardized regression coefficients (β) and their 95% confidence intervals (CI) from separate multiple regression models in which leisure activities was regressed on number and diversity of positive ties (left panel, n = 854) or number and diversity of ambivalent ties (right panel, n = 300), adjusting for relevant covariates. Variables were standardized using the corresponding n for each model. Coefficients significantly differ in magnitude if their CIs do not contain the coefficient from the other (Greenland et al., 2016). *p < .05.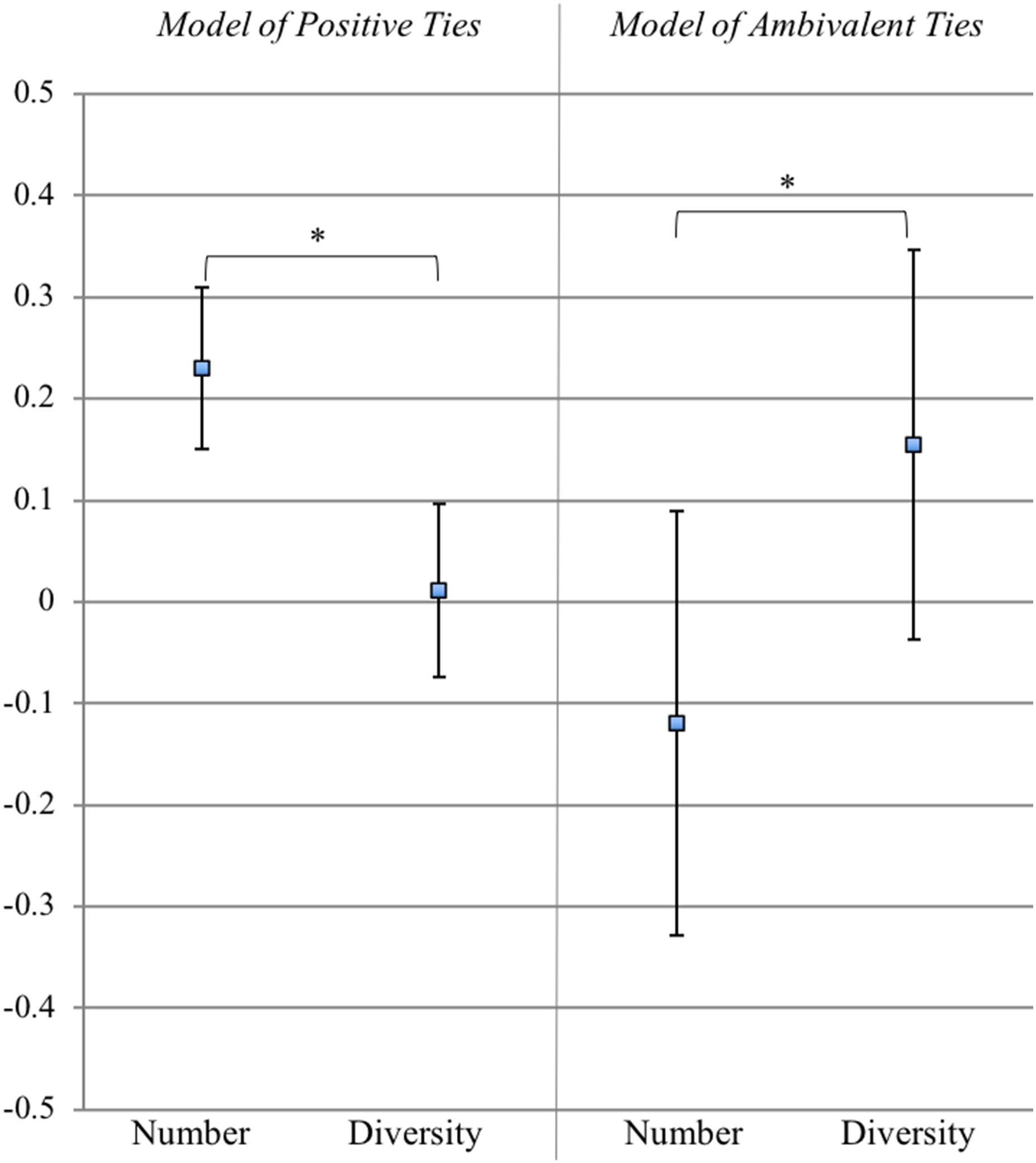
Ambivalent Ties and Leisure Activities
A parallel model contrasted the associations of number and diversity of ambivalent ties with leisure activities (see Table 3, bottom panel). Number of ambivalent ties did not exhibit a unique association [β = −.12, t(292) = −1.33, p = .19], and diversity of ambivalent ties exhibited a marginally significant unique association with greater leisure activities [β = .16, t(292) = 1.75, p = .08]. A comparison of CIs revealed that the unique (albeit non-significant) association between number of ambivalent ties and leisure activities was weaker in magnitude than was that of diversity of ambivalent ties (see Figure 2, right panel).
Supplemental Analyses
Given that our findings differed from those of previous research that has compared number and diversity of ties (e.g., Cohen et al., 1997), we undertook supplemental analyses to evaluate whether particular aspects of our analytic or assessment strategies may have contributed to these divergent findings. Because most studies implicitly assume that diverse networks are exclusively positive, we considered the possibility that analyses based on participants who had exclusively positive social ties would yield associations more similar to those reported in previous studies. Repeating our analyses with participants who had exclusively positive ties (n = 574) did not change the pattern of results. The sole exception was one CI comparison that revealed the unique association between number of positive ties and functional limitations (albeit non-significant) to be slightly stronger in magnitude compared to that of diversity of positive ties. Thus, these findings largely replicate the findings from our original models and modestly strengthen the evidence in favor of number of ties as particularly important for health. Results of these supplemental analyses are available upon request from the first author.
In addition, because some previous studies have emphasized role relationships with individuals contacted at least biweekly (e.g., Cohen et al., 1997; Ellwardt et al., 2015), we examined the frequency of contact with the 4,524 ties named as sources of positive exchanges in our study (1 = every day, 2 = several times a week, 3 = about once a week, 4 = several times a month, 5 = about once a month, and 6 = less than once a month). Interactions occurred with 75.4% of these ties at least once per week and with an additional 12.2% of these ties several times per month. Thus, our network elicitation method captured network members who were contacted frequently, which is consistent with previous studies.
Discussion
Prevailing views consider diversity of social ties to be more important than the sheer number of social ties as a determinant of health. Empirical tests of that claim are relatively scarce, however, and ambivalent ties are rarely considered. The present study critically evaluated this claim in a nationally representative sample of older adults by comparing the unique associations of number versus diversity of both positive and ambivalent ties with two key components of successful aging (Rowe & Kahn, 1997)—functional limitations and leisure activities. Contrary to prevailing views, we found that diversity of ties is not necessarily superior to number of ties. Rather, number was related to each outcome at a comparable or greater magnitude than was diversity in most of our models, with some nuances across the different outcomes and the positive or ambivalent nature of the ties.
Is Number or Diversity of Social Ties More Important for Functional Limitations?
When examining positive ties, our regression model revealed that number of positive ties was marginally related to fewer functional limitations, whereas diversity of positive ties was non-significant. Despite differences in significance, however, the magnitudes of their unique associations were comparable. Notably, given the goal of the current study, no analyses revealed diversity of positive ties to be more strongly related to functional limitations than was number of positive ties. These findings extend those of another study (Ellwardt et al., 2015) of older adults in which network size and diversity were each significantly related to mortality risk. By directly comparing their strengths in the current study, our findings provide evidence that number and diversity of positive ties are comparably important for functional limitations in later adulthood.
Examination of ambivalent ties revealed a somewhat different pattern. Our regression model revealed that number and diversity of ambivalent ties were uniquely related to functional limitations, albeit in different directions and with different strength. Having more ambivalent ties was related to more functional limitations, consistent with the existing literature. Having more diverse ambivalent ties, in contrast, was related to fewer functional limitations. Why having more diverse ambivalent ties might benefit functional health is unclear, although it is possible that having ambivalent ties distributed across multiple role relationships reduces their toxicity in some way or increases access to resources that bolster health. Alternatively, given that ambivalent ties are commonly family members (Fingerman et al., 2004), it is possible that more diverse ambivalent ties might reflect a more diverse family network. Interestingly, a recent study of older adults found that greater ambivalence in extended kin ties was related to longer telomeres (indicating less cellular aging; Lincoln et al., 2019), echoing our finding regarding functional health. Reverse causation may also underlie links between diverse ambivalent ties and health, if older adults who maintain more diverse ambivalent ties are able to do so because they are in better health. Importantly, in the current study, the link between number of ambivalent ties and functional limitations was significantly stronger than was the link between diversity of ambivalent ties and functional limitations, suggesting that the sheer number of ambivalent ties may be more consequential than their diversity for functional limitations in later adulthood.
Altogether, our findings diverge from those of Cohen et al. (1997), in which diversity of ties mattered more for cold susceptibility than did number of ties in a sample of young to middle-aged adults. The current study, in contrast, examined functional limitations as a key indicator of physical health in a large representative sample of older adults. The different dimensions of health examined and different sample characteristics in each study may account for the divergent findings. In addition, some evidence suggests older adults tend to have less diverse social networks than do younger adults (Weber et al., 2020; Zhaoyang et al., 2018). Recent evidence from an adult lifespan sample (Weber et al., 2020), however, revealed no age differences in the link between functional limitations and the diversity of social partners. Nonetheless, the generalizability of our findings to younger age groups remains to be evaluated.
Is Number or Diversity of Social Ties More Important for Leisure Activities?
Analyses of positive ties revealed that number was uniquely related to more leisure activities, and with greater strength, compared to diversity. Moreover, diversity of positive ties did not exhibit unique explanatory value. These findings challenge conventional wisdom that participation in a broad range of social roles is crucial to an active and healthy lifestyle in later life (Berkman et al., 2000). In fact, there may be potential “switching” costs of having multiple social roles (Cornwell, 2013), whereby needing to switch regularly between different roles and their respective activities or duties can be a source of stress. If such switching is taxing, it could help to explain why diversity of positive social ties did not appear to contribute to the older participants’ greater engagement in leisure activities beyond the sheer number of positive ties. Instead, our findings suggest that having more positive ties, rather than having more diverse positive ties, may be most important in supporting more frequent leisure activities.
Analyses of ambivalent ties and leisure activities were less conclusive. Number of ambivalent ties was not significantly related to leisure activities, whereas diversity of ambivalent ties was uniquely, albeit marginally, related to more frequent leisure activities. These results are puzzling, particularly in view of the earlier finding that diverse positive ties were unrelated to leisure activities. The link between diverse ambivalent ties and greater leisure activities might have reflected activity that was somewhat compulsory (e.g., family get-togethers, ceremonies, reunions), which would be consistent with some evidence (cf. Coleman & Iso-Ahola, 1993). Other research, however, suggests that ambivalent ties might deter leisure activities because older adults would attempt to limit exposure to these ties (Charles, 2010). Current findings reveal a trend that supports the former idea, but future research is needed to unpack the nuances.
The counterintuitive findings suggesting salutary links between diverse ambivalent ties and both leisure activities and functional limitations may actually be connected. It is possible that more diverse ambivalent ties contribute to more leisure activities (compulsory or otherwise) that in turn benefit functional health. It is also possible that functional health enables more leisure activities and also broadens social interactions in ways that include more diverse ambivalent ties. The cross-sectional nature of our analyses, however, precludes definitive tests of these ideas. Finally, these links may also be contingent on the closeness of ties, given that close (compared to peripheral) ties have been related to less activity engagement (Fingerman et al., 2020). Future studies assessing the perceived closeness of older adults’ activity partners could provide a more definitive explanation.
Implications for Interventions
The current findings call into question the often-repeated claim that the diversity of social ties matters more for health and well-being than does the sheer number of social ties. These findings thus help to extend knowledge of the social network characteristics that are most crucial for healthy and active aging. The findings also have implications for interventions, as they suggest that previous recommendations for interventions to emphasize the development of diverse social ties (e.g., Cohen & Janicki-Deverts, 2009; Rhee et al., 2021) may lack a strong empirical base and, as a result, might be premature. Diversifying social ties, moreover, is likely to require different, and potentially more numerous, strategies (e.g., making new friends, meeting a new neighbor, becoming a volunteer, joining a community organization, rekindling a dormant kin tie) than does increasing the number of social ties (e.g., making new friends). Encouraging older intervention participants to strive to diversify their social ties may lead them on a path that is difficult without clear evidence of superior benefits, compared to encouraging them simply to strive to increase their social ties.
Each of these strategies could be differentially preferable or accessible depending on the person, as well as the desired outcome. The current findings suggest that strategies to increase number of positive ties may be most important for leisure activity interventions, whereas increasing either number or diversity of positive ties, as well as decreasing number of ambivalent ties, may be equally useful for interventions aiming to improve functional health. Altogether, this study strengthens our understanding of when and why providing opportunities for older adults to develop ties, but not necessarily diversify ties, may be most crucial.
Limitations and Future Directions
Study limitations should be considered in evaluating the findings. First, the cross-sectional nature of the data makes it difficult to rule out reverse causation. Older adults in poor health may have fewer opportunities to maintain social ties (McQuoid, 2017), and caregiving responsibilities can be a source of ambivalence (Pillemer et al., 2019). Poor health would have to affect the number and diversity of social ties in distinctive ways, however, to account for the current findings. Additionally, our inclusion of chronic conditions as a covariate helps to rule out the influence of health status. Nonetheless, the possibility of reverse causation should be examined in future research. Second, the study sample was demographically similar to U.S. census data for older adults, but the 65+ population is becoming more racially and ethnically diverse. Future studies are needed, therefore, that examine racial, ethnic, and cultural variations in the links between health-related outcomes and the number versus diversity of social ties.
It also warrants noting that the diversity of social ties has been operationalized in a myriad of ways across the literature. The present study prioritized a detailed mapping of social network ties with whom participants had recently engaged in meaningful exchanges of support and companionship, rather than a complete record of daily interactions, as some previous studies have emphasized (e.g., Cohen & Lemay, 2007; Fingerman et al., 2020). A unique feature of the daily interaction approach is that it captures relatively brief or routine interactions with peripheral others or even strangers. Such interactions may benefit health and well-being by discouraging sedentary behavior or providing momentary boosts in positive affect (Fingerman et al., 2020). Diverse peripheral contacts may also provide stepping stones for building new ties or strengthening existing ties. On the other hand, diverse daily contacts may be more susceptible to switching costs discussed earlier (Cornwell, 2013), perhaps more so than the diverse enduring ties assessed in our study. These varied measurement approaches invite further attention to the different facets of social integration and their pathways to health.
A compelling direction for future research will be to examine connections between role diversity and functional specificity. Role diversity may contribute to well-being primarily when it reflects a mix of social partners who perform relatively specialized functions (e.g., instrumental support, emotional support, companionship) that are considered to be crucial for health and well-being. Having diverse social roles that lack this kind of mix might not contribute substantially to health and well-being. Although our findings challenge claims that diversity is better, we would also urge against a hasty conclusion that “more is better.” Number of ties decreases as people age, but people selectively engage with closer and more meaningful ties (Carstensen, 2006). This selective engagement may preserve older adults’ well-being if they retain key ties who perform functions defined as most crucial by theorists (e.g., Weiss, 1969). In this sense, having a good match between roles and functions, so that one’s key needs are met by the optimal providers, may be most important for health and well-being. Thus, the patterning of diverse social ties may matter as much, or more, than simply having diverse social ties.
Finally, data for this study were collected prior to the COVID-19 pandemic, and thus cannot speak to the impact of disasters that disrupt social lives and leisure opportunities. Much important work has been conducted to understand how older adults’ social networks operate during and after a widespread devastating event (Kwan & Walsh, 2017; Saltzman et al., 2020). More research is needed to learn whether current findings regarding the relative importance of number versus diversity of older adults’ social ties extend to such contexts and to relevant biological markers of health (e.g., respiratory illnesses, immune markers), which the current study lacked. It is possible, for example, that having more diverse social ties is particularly important in the context of a community-wide disaster, with a neighbor or friend stepping in to provide support that ordinarily would have been provided by a family member. Changing sociohistorical contexts, such as technological advancements, are also important to consider, as these changes may shape both the availability and costs of particular kinds of social interactions in later life (Fiori et al., 2020).
Despite these limitations, the study included notable strengths. It examined number versus diversity of social ties using data from a nationally representative sample of older adults, assessed a broad range of positive and negative functions performed by network members, assessed the role relationship with each network member, and extended previous research to consider ambivalent ties as well as positive ties. Future research might seek to join this strategy for examining social network ties with one that examines daily social interactions in order to deepen our understanding of the health-related significance of diversity in older adults’ interpersonal experiences.
Conclusion
Current study findings challenge prevailing views that diversity of social ties is more important than the sheer number of ties. Findings suggest that, among older adults, number of ties generally relates to health and leisure activity at a magnitude that is comparable to, or exceeds, that of diversity. This distinction is also nuanced depending on the outcome, as well as the positive or ambivalent nature of the ties. These findings suggest that scientific understanding, as well as intervention planning, may benefit from a critical consideration of the role of number versus diversity of social ties in older adults’ lives.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Institute on Aging (grant number AG14130).