
Abstract
High annual figures of sexually transmitted infections (STIs) are diagnosed in the Netherlands despite significant efforts to control them. Herein, we analyse trends and determinants of STI diagnoses, co-infections, and sexual risks among visitors of 26 STI clinics between 2007 and 2011. We recorded increased positivity rates of STIs (chlamydia, syphilis, gonorrhoea, and/or HIV) in women and heterosexual men up to 12.6% and 13.4%, respectively, in 2011, while rates in men having sex with men (MSM) were stable but high (18.8%) through the documented years. Younger age, origin from Surinam/Antilles, history of previous STI, multiple partners, or a previous notification are the identified risk factors for an STI in this population. Known HIV-infected men (MSM and heterosexuals) were at highest risk for co-infections (relative rate heterosexual men: 15.6; MSM: 11.6). STI positivity rates remained high (MSM) or increased over time (women and heterosexual men), a fact that highlights the importance of continuing STI prevention. Most importantly, the very high STI co-infection rates among HIV-positive men requires intensified STI reduction strategies to put an end to the vicious circle of re-infection and spread of HIV and other STIs.
Keywords
Introduction
Controlling sexually transmitted infections (STIs) among people with high-risk sexual behaviour is an important public health issue in the Netherlands, as well as globally. Undetected and untreated STI can increase a person’s risk for HIV 1 and can lead to serious conditions as pelvic inflammatory disease (PID), infertility, ectopic pregnancy, and perinatal death. 2
In the Netherlands, populations with high risk of STI acquisition include young people (<25 years old), 3 men having sex with men (MSM), 4 persons referred through partner notification (PN), 5 commercial sex workers (CSW) and their clients, 6 migrant populations, 7 swingers, 8 persons with a previous history of STI/HIV (diagnosis or symptoms), and persons with high-risk behaviour (defined as ≥ 3 partners in the past 6 months). For these groups, 26 STI clinics throughout the country provide low-threshold care (free of charge and, if preferred, anonymously). 9 Persons who do not fulfil these criteria are referred to the general practitioner (GP) for STI/HIV testing.
All STI clinic attendees are offered standard testing for chlamydia, gonorrhoea, syphilis, and HIV. Other STIs, such as hepatitis B and C, genital herpes, trichomoniasis, and lymphogranuloma venereum (LGV), are tested upon indication. The STI clinics routinely collect and submit diagnostic and key behavioural indicators anonymously for surveillance purposes to the National Institute for Public Health and the Environment (RIVM). The database contains demographics, STI/HIV testing results, and behavioural determinants.10,11
Our objective was to record and analyse trends in STIs and co-infection rates among STI clinic attendees, over the time indicated (2007
Materials and methods
At the STI clinics, STI/HIV surveillance data are reported to the RIVM facilitated by a web-based application (SOAP). 12 For all attendees, information on demographics and behavioural risks was initially collected. Each subsequent STI consultation involves laboratory testing and medical examination by a physician or specialised nurse. Attendees are routinely tested for chlamydia, gonorrhoea, syphilis, and HIV. Microbiological diagnostics are carried out locally at laboratories related to the STI centres in accordance with standard procedures established in an STI screening protocol, including quality control measures. For HIV testing, an antibody/antigen serology test with confirmation (Blot test and/or nucleic acid amplification test, NAAT) is the current method in most laboratories. For gonorrhoea, diagnostics were performed using NAAT, sometimes in combination with culture; for chlamydia only NAAT was used. Syphilis is determined using Treponema pallidum haemagglutination or T. pallidum particle agglutination (TPHA/TPPA) tests followed by a ‘venereal disease research laboratory’ (VDRL)-test and/or a fluorescent treponemal antibody (FTA) absorption test. 13 STI consultations between January 2007 and December 2011 were studied. We analysed the determinants of sexual risk behaviour, HIV testing, and STI/HIV diagnoses by univariable and multivariable Poisson regression analyses separately for MSM, heterosexual men, and women. To obtain robust standard errors for the parameter estimates and control for mild violation of the distribution assumption, we used criteria as described by Barros and Hirakata. 14
The Poisson models included (binary) behavioural outcomes such as (1) previously tested versus not previously tested for HIV, (2) having three or more sex partners in the past 6 months versus less than three (first key indicator for sexual risk), and (3) protected versus unprotected intercourse with a casual partner in the past 6 months (second key indicator for sexual risk).
Furthermore, models were constructed for STI diagnoses (4) the occurrence of a single STI diagnosis (chlamydia, gonorrhoea, syphilis, or new HIV infection) versus no STI diagnosis, and (5) the occurrence of a co-infection (at least two newly diagnosed STIs) versus no STI diagnosis. Known HIV-positive persons were classified as co-infected in case, next to HIV, two other STIs were diagnosed. Only individuals for whom the database contained results for all four lab tests were included in the analysis. The data collection does not allow for identification of repeat visits of the same individual due to lack of a personal identifier. The multivariable Poisson models (backwards selection) incorporated the independent variables from the univariable analysis that showed an association with the outcome parameters of p < 0.20. Variables included were year of consultation, age group, ethnicity, socioeconomic status (SES), swinger practices (heterosexual couples practicing partner swapping or having group sex 8 ), CSW and clients, number of sex partners in the past 6 months, condom use during last intercourse with steady partner, condom use during last intercourse with casual partner, STI-related symptoms, referral through PN, previous STI (chlamydia, gonorrhoea, or syphilis), and previous HIV test. Variables that produced p < 0.05 in the multivariable models were considered as statistically significant.
SES was deduced by postal code-associated data from the Netherlands Institute for Social Research 15 and is a composed measure of four variables: average income per household; percentage of households with low incomes; percentage of residents without a paid job; and percentage of households with an average-to-low education. Ethnicity is a combination of two definitions: self-defined ethnicity (compulsory question in SOAP until 2010, voluntary from 2011) and ethnicity based on country of birth of the clinic attendee and his/her parents (voluntary in 2010, compulsory from 2011). Analyses were carried out using SPSS statistics version 19 (IBM Corporation, Somers, New York, USA).
Results
Study population
Between 2007 and 2011, 478,024 STI consultations were registered. In total, 1799 consultations were excluded (0.4%) due to missing data on sexual preference in men, age, or individuals of 14 years or younger, leaving 476,225 consultations for analysis.
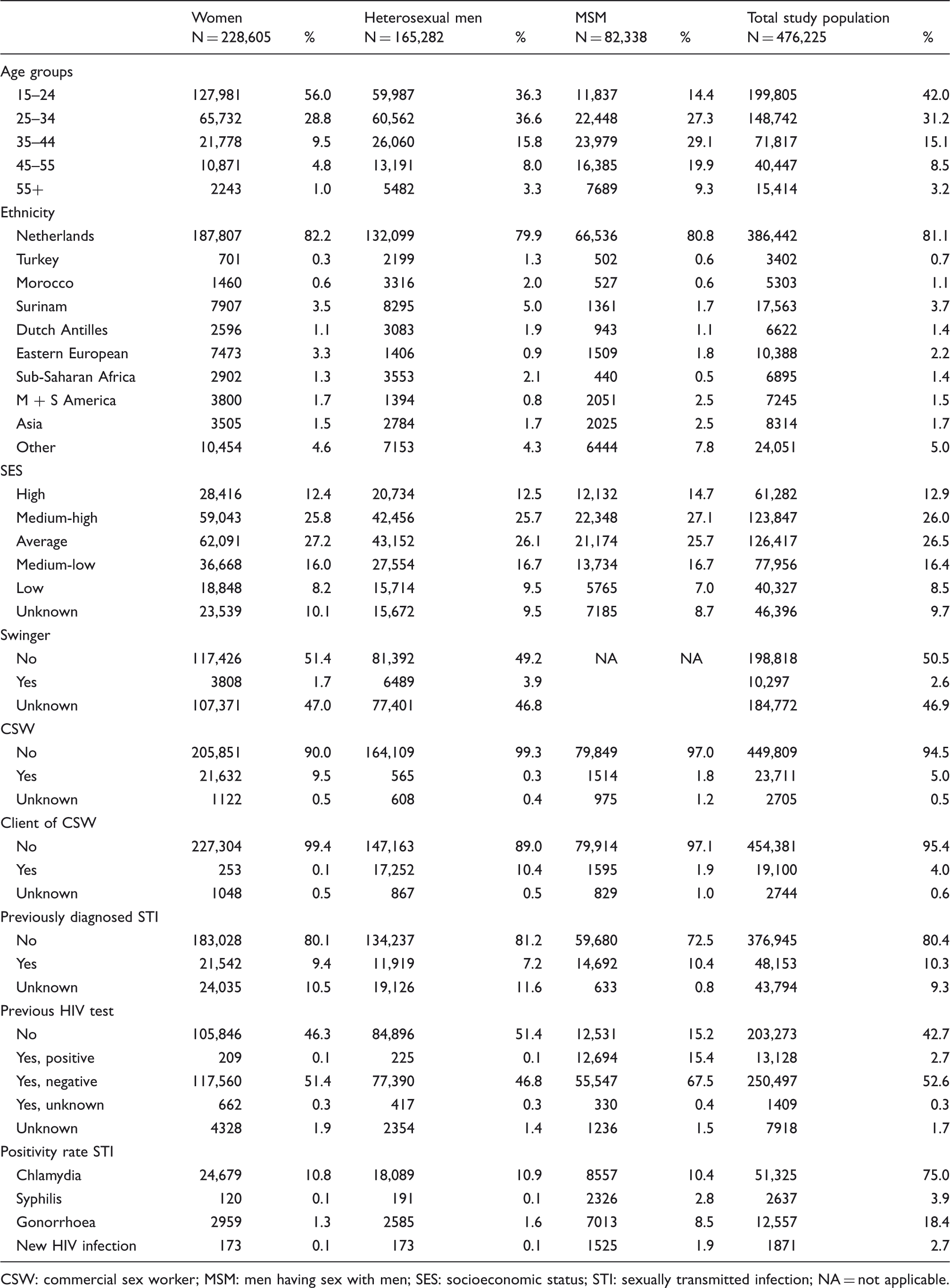
Over the past 5 years, the number of STI consultations increased by +45% from 78,062 in 2007 to 113,180 in 2011 (chi-square for trend, p < 0.001) (Figure 1). There was a proportional increase in consultations for MSM from 14.2% in 2007 to 19.3% in 2011. The exact numbers of MSM visits almost doubled over this observation period. Additionally for MSM, there were relatively more attendees from the older age groups (58.4% ≥ 35 years old) compared to women (15.3% ≥ 35 years old) and heterosexual men (27.1%, Table 1). Also, overall, 18.9% of attendees were of a non-Dutch ethnicity. Among heterosexuals, the largest groups of non-Dutch ethnicity were Surinamese, Eastern-Europeans, and sub-Saharan Africans, while among MSM relatively more people originated from Central or South America and Asia (Table 1).
Number of consultations and positivity rates for sexually transmitted infection (STI) in STI clinic attendees, by gender and sexual preference, 2007 Characteristics of STI clinic attendees in the Netherlands, 2007 CSW: commercial sex worker; MSM: men having sex with men; SES: socioeconomic status; STI: sexually transmitted infection; NA = not applicable.
HIV testing and sexual behaviour
Of all clinic attendees in 2007 Behavioural characteristics of sexually transmitted infection (STI) clinic attendees, 2007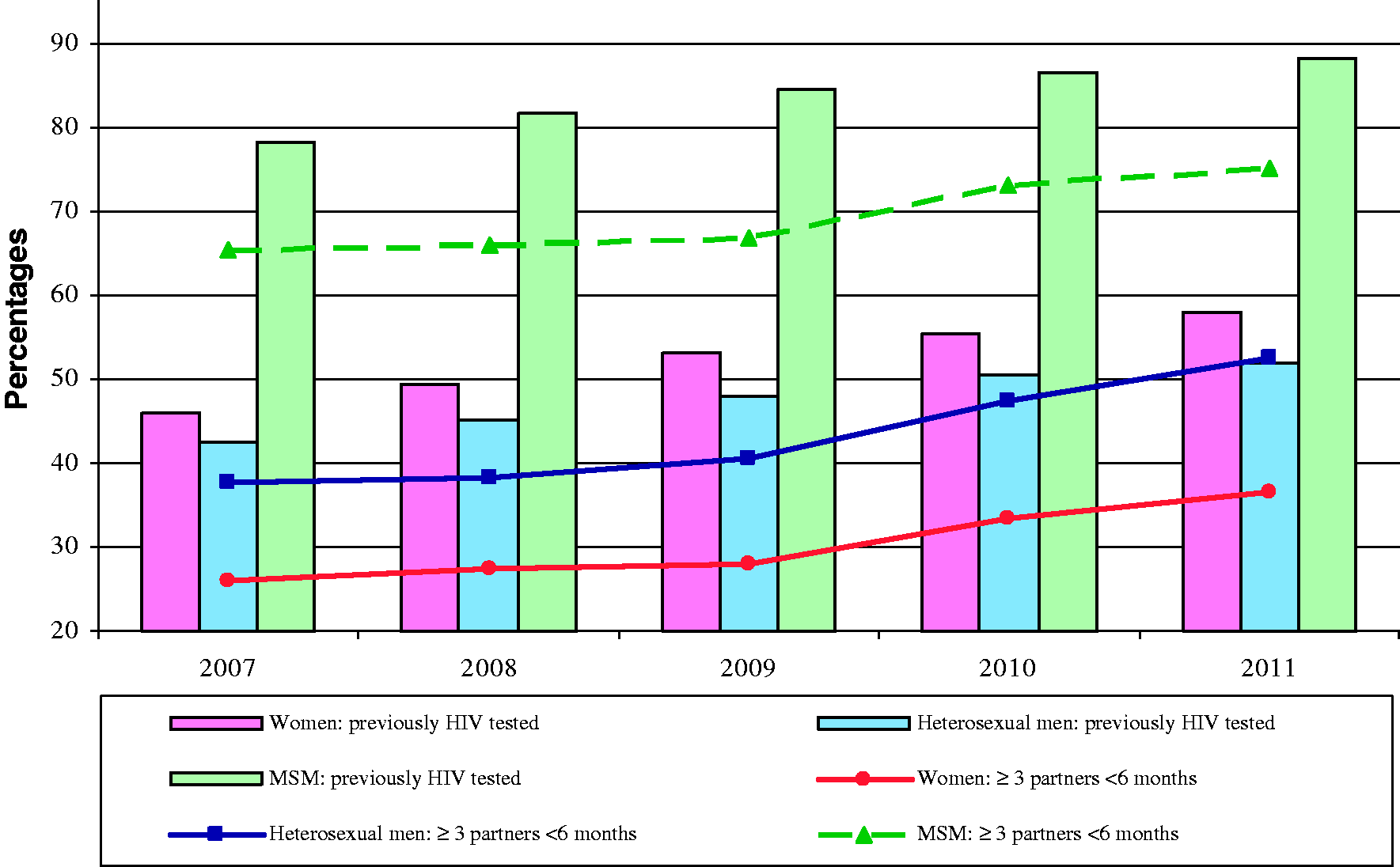
Multivariable Poisson regression for HIV testing and sexual risks among STI clinic attendees, 2007

NA: Not applicable or not tested (univariately not significant); NS: Multivariately not significant; RR: relative rate; CSW: commercial sex worker; MSM: men having sex with men; STI: sexually transmitted infection.
Variables not shown due to small or no significant effect in all subgroups: SES, condom use with steady/casual partner, being notified. Unknown categories were included in the model but not shown. The information about condom use with a casual or steady partner is only available since 2009.
In all groups (MSM, heterosexual men, and women), a significant increase in the category: “3 or more partners in the last 6 months” was observed (chi-square, p < 0.001) (Figure 2). In women and MSM, the 35+ age groups were more likely to fall in this category, while in heterosexual men this was the youngest group (<24 years old) (Table 2). Except for Eastern European women, non-Dutch women were less likely to report multiple partners compared to Dutch women (RRs between 0.6 and 0.8). Among heterosexual men and MSM, sub-Saharan African men reported less often multiple sexual partners (RR 0.8 [0.8–0.9]) and 0.9 [0.8–1.0]). Those who were previously tested for HIV were more likely to report multiple partners than those not tested before.
Although swingers, female CSW, and male clients of CSW more often reported ≥3 partners in the past 6 months, they were less likely to have had unprotected intercourse with a casual partner (RRs between 0.3 and 0.9). MSM subgroups reporting more often unprotected intercourse with a casual partner were MSM of non-Dutch origin (RR between 1.1 and 1.3), known HIV-positive MSM (RR: 1.2, 1.2
Determinants of STI
Out of all STI clinic attendees in 2007
In 1.2% (n = 4719) of all consultations, an STI co-infection was diagnosed, in which MSM accounted for 56.1%. Overall, 4.8% of MSM were newly diagnosed with two or more STIs. For women and heterosexual men, these percentages were 0.6 and 0.7%, respectively.
Multivariable Poisson regression for determinants of a single STI and co-infections among STI clinic attendees, 2007–2011.

NA = Not applicable or not tested (univariately not significant); NS = Multivariately not significant; RR: relative rate; CSW: commercial sex worker; MSM: men having sex with men; SES: socioeconomic status; STI: sexually transmitted infection.
Where individuals with a previously diagnosed HIV infection were less likely to have a single infection, they more often had co-infections, especially HIV-positive men (RR heterosexual men: 15.6 [7.0--35.0], MSM: 11.6 [10.0--13.6], and women: 4.5 [1.0--19.2]). The relative rate of having STI co-infections amongst HIV-positive heterosexual men remained stable after 2008 but slightly decreased for MSM (RR 0.7 in 2011 compared to 2007). Furthermore, Surinamese and Antilleans, female and MSM CSW, and previously notified persons were at higher risk for having a co-infection.
Discussion
Independent of sexual preference, STI clinic attendees who were young, had multiple partners, had previously been notified, were of Surinamese/Antillean origin, or had a previous STI were most likely to have an STI. Known HIV-positive men (MSM and heterosexual men) were at highest risk for STI co-infections. Previous studies described HIV-positive MSM being at particularly high risk for co-infections.12,16,17 They are more likely to report unprotected intercourse with casual partners compared to HIV-negative MSM, 18 which could refer to “serosorting” 19 : i.e. the behaviour of HIV-positive MSM to seek HIV-positive partners. 20 However, the high risk for young heterosexuals and HIV-positive heterosexual men for co-infections has not been elaborately described in the Netherlands. The risk in the last group was surprisingly high, although confidence intervals were broader compared to MSM. Determinants associated with high rates of STIs in these groups may also relate to the overall increase of the HIV-infected sexually-active population over the time studied, as well as the observed loss of the initial HIV-era fear for HIV transmission in later times, due to the vast availability of combination antiretroviral therapy (cART).21,22 Stolte et al. 23 reported an increase in MSM attending STI clinics and a rise in infection rates coinciding with the introduction of cART. We observed an increase in the proportion of individuals previously tested for HIV between 2007 and 2011, which could be a consequence of encouragement of high-risk populations, in particular MSM, to re-visit the clinic for testing. Unfortunately, it was not possible to control for repeated visits since attendees are registered anonymously. We cannot rule out the possibility that repeated visits, including those previously tested positive for HIV, may have resulted in an overestimation of infection risks. Therefore, the changes observed in STI positivity rates over time, as well as the increasing proportions of people with multiple partners or unprotected intercourse with casual partners, could be the result of increased STI risk or incidence or it could reflect changes in health care-seeking behaviour such as people being encouraged to visit the STI clinic more regularly because of high-risk behaviour.
Furthermore, HIV testing rates increased over the years, especially for women. This could be partly due to a shift in testing regulations at the STI clinics from opting in for HIV testing to opting out from it.23,24 Although HIV testing rates for women increased in general, Turkish and Moroccan women were slightly less likely to have been previously HIV tested, while they were more likely to test positive for an STI compared to Dutch women. Ethnic minority populations could be more specifically targeted for repeated visits, due to this higher risk for single and multiple STIs. CSW, their clients and swingers, were more likely to have been HIV tested before while they reported less often unprotected sex with casual partners. These groups seem to be more aware of their potential risk of infection.
A limitation of this study is that the number of STI clinic visits cannot be compared to the actual general population. This is because the particular STI clinics in our country are only testing high-risk group individuals, with GPs taking the burden of testing for a broader population. Recently, it has been described that an estimated 30% of the STI consultations are conducted at the STI clinics and the remaining at GPs. 25 It is also known that persons consulting a GP for STI testing are comparable to STI clinic attendees regarding age and ethnicity; however, high-risk groups such as MSM and CSW are less likely to attend the GP. Moreover, the GP testing may be considered far more selective, whereas the STI clinics routinely test all clients for the whole array of STIs. 26 Currently, the awareness of Dutch GPs of the importance of their role in STI/HIV testing and control is nationally highlighted in official professional education.
Discussion is currently evolving around the opportunistic screening for STIs in HIV treatment centres. A recent study including 659 HIV-positive MSM visiting outpatient clinics of academic hospitals showed that 16% had an asymptomatic STI. 27 Moreover, the use of drugs during sex was strongly associated with STI occurrence, a fact that may delineate an additional opportunity for testing in drug-using populations. The authors concluded that routine screening of HIV-infected MSM is appropriate and should not be limited to those who report high-risk sexual behaviours. It should be further examined whether STI testing of HIV-infected heterosexual men at HIV treatment clinics could be (cost) effective.
Our study has a few further limitations. Social desirability bias in the answers of the attendees cannot be excluded. In some cultures, having multiple partners is considered positive for men, but shameful for women, which may have influenced the numbers of sex partners reported by the clinic attendees, 28 although nowadays the shift towards a more healthy lifestyle is promoted across all SES and health education is wider than the previous years. In conclusion, the high STI positivity rates among young people and migrant populations, as well as the very high STI co-infection rates among HIV-positive men, require enhanced prevention efforts at various test locations to reduce further spread of HIV/STI. It may be wise to stretch from the questions asked currently to include other risk factor information such as substance use, 29 concurrent sexual partners, and partnership types to further control STI transmission.30,31 Lastly, the role of PN is highlighted as the rates in the particular groups are high for HIV and STI; and the monitoring and correct function of this system may result in further improvements of the effectiveness of Dutch PN services 5 and in the reduction of transmission of STI/HIV.
Footnotes
Acknowledgement
We thank all Public Health nurses and physicians of the STI clinics for their contribution in data collection; medical microbiology laboratories for STI diagnostics; Jantine Schuit, Marianne van der Sande and Birgit van Benthem for critically reviewing the manuscript, and Jan van de Kassteele for statistical advice.
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.